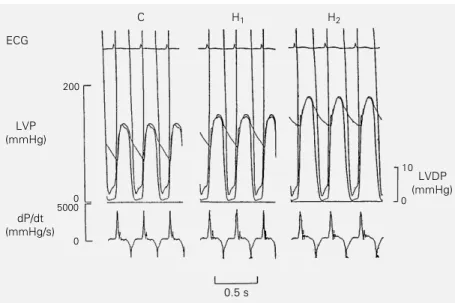
The rate of force generation by the myocardium is not influenced by afterload
Texto
Imagem
Documentos relacionados
Ao Dr Oliver Duenisch pelos contatos feitos e orientação de língua estrangeira Ao Dr Agenor Maccari pela ajuda na viabilização da área do experimento de campo Ao Dr Rudi Arno
Neste trabalho o objetivo central foi a ampliação e adequação do procedimento e programa computacional baseado no programa comercial MSC.PATRAN, para a geração automática de modelos
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
Para tanto foi realizada uma pesquisa descritiva, utilizando-se da pesquisa documental, na Secretaria Nacional de Esporte de Alto Rendimento do Ministério do Esporte
Este relatório relata as vivências experimentadas durante o estágio curricular, realizado na Farmácia S.Miguel, bem como todas as atividades/formações realizadas
Nesse sentido, este estudo realizou a caracterização da flora das Restingas da Zona de Expansão de Aracaju, analisando sua similaridade florística e distinção taxonômica com
Extinction with social support is blocked by the protein synthesis inhibitors anisomycin and rapamycin and by the inhibitor of gene expression 5,6-dichloro-1- β-
Having introduced a generic method to build propositional many-valued dy- namic logics, parameterised by an action lattice (intended to capture the nature of computations), we plan
