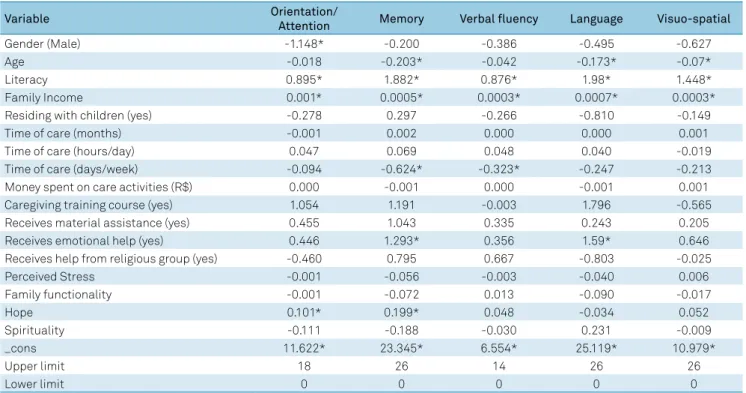
Factors associated with cognitive performance in elderly caregivers
Texto
Imagem

Documentos relacionados
This study provided information on the profile of caregivers and elderly care recipients, as well as on the health complaints of caregivers and the care they took of themselves,
Given the above-mentioned scenario, the objective of this study was to assess the preva- lence of the factors associated with self-reported diabetes in elderly population and verify
he objective of the present study was to describe the performance of a group of healthy elderly, a patient group with Mild Cognitive Impairment (MCI), and another with
Purpose: The aim of this study was to determine the factors associated with temporomandibular disorders (TMD) in the non-institutionalized and institutionalized elderly population
The present study aimed to investigate the relationships between the perceptions of quality of life of elderly caregivers of elderly people with neurological diseases (dementia
This cross-sectional study analyzes the association between cognitive performance and functional capacity in an elderly population sample in Natal, Brazil.. A total of 213
Em compensação, outras peças, feitas de bula timpânica de baleia, tem uma forma semelhante aos zoólitos, algumas delas até apresentam uma cavidade (aquela que existe
Nesse contexto, marcado pela aparente contradição entre individualismo e uma era de possibilidades globais, intenta-se abordar, de modo crítico, os conceitos trazidos
