Original Article
REVISTA PAULISTA DE MEDICIN AEpide miology of Bloodstre am
Infe ctions at a Cance r Ce nte r
Hospital Infection Comitee, Infectious Diseases Service,
Hospital do Câncer, Instituto Nacional de Câncer, Rio de Janeiro, Brazil
a b s t r a c t
CON TEX T: Cancer patients are at unusually hig h risk fo r develo ping blo o dstream infectio ns (BSI), which are a majo r cause o f in-ho spital mo rbidity and mo rtality.
OBJECTIVE: To describe the epidemio lo g ical characteristics and the etio lo g y o f BSI in cancer patients.
DESIGN: Descriptive study.
SETTIN G: Terciary O nco lo g y Care Center.
PARTICIPAN TS: During a 2 4 -mo nth perio d all ho spitaliz ed patients with clinically sig nificant BSI were evaluated in relatio n to several clinical and demo g raphic facto rs.
RESULTS: The study enro lled 4 3 5 episo des o f BSI (3 4 9 patients). The majo rity o f the episo des o ccurred amo ng no n-neutro penic patients (5 8 .6 %) and in tho se yo ung er than 4 0 years (5 8 .2 %). There was a hig her o ccurrence o f unimicro bial infectio ns (7 4 .9 %), no so co mial episo des (6 8 .3 %) and o f tho se o f undetermined o rig in (5 2 .8 %). Central veno us catheters (CVC) were present in 6 3 .2 % o f the epi-so des. O verall, the co mmo nest iepi-so lates fro m blo o d in patients with hemato lo g y diseases and so lid tumo rs were staphylo co cci (3 2 % and 3 4 .7 %, respectively). There were 7 0 episo des o f fung emia with a predo minance o f Candida albicans o rg anisms (5 0 .6 %). Fung i were identified in 5 2 .5 % o f persistent BSI and in 9 1 .4 % o f patients with CVC. G ram-neg ative bacilli pro mpted the CVC remo val in 4 5 .5 % o f the episo des. O xacillin resistance was detected in 2 6 .3 % o f Sta-phylo co ccus aureus iso lates and in 6 1 .8 % o f co ag ulase-neg ative Staphylo co ccus. Vanco mycin-resistant entero co cci were no t o bserved. Initial empirical antimicro bial therapy was co nsidered appro priate in 6 0 .5 % o f the cases.
CON CLUSION: The identificatio n o f the micro bio lo g y pro file o f BSI and the reco g nitio n o f po ssible risk facto rs in hig h-risk cancer pa-tients may help in planning and co nducting mo re effective infectio n co ntro l and preventive measures, and may also allo w further ana-lytical studies fo r reducing severe infectio us co mplicatio ns in such g ro ups o f patients.
KEY W ORDS: Blo o dstream infectio n. Cancer. Epidemio lo g y. Micro -bio lo g y.
• Eduardo Velasco • Luiz Claudio Santo s Thuler • Carlo s Alberto de So uz a Martins • Márcio N ucci • Leda Maria Castro Dias • Vânia Maria da Silva Castro G o nçalves
INTRODUCTION
The im p ro ve m e nt in lo ng- te rm s urvival o f immuno co mpro mised patients with neo plastic diseases and tho se undergo ing o rgan and bo ne marro w trans-plants has pro duced a po pulatio n o f patients even mo re susceptible to infectio ns.1 Fo r this reaso n, the infectio us
co mplicatio ns co nsequent to the immuno suppressive therapy have beco me the majo r causes o f mo rbidity and mo rtality in this high-risk gro up o f patients.2
The underlying disease, as well as the neutro -penia and o ther risk facto rs, have altered substantially the epidemio lo gy o f infectio ns, allo wing the develo p-ment o f o ppo rtunistic infectio us pro cesses at so me
po int during the immuno suppressive therapy.3 The
o bjective o f this study was to describe the epidemio -lo gical characteristics and the etio -lo gy o f b-lo o dstream infectio ns (BSI) at a referral cancer center.
METHODS
The Ho spital do Câncer is a 206-bed tertiary o n-co lo gy care center including medical/surgical inten-sive care and b o ne marro w transplantatio n (BMT) units. It is the majo r ho spital o f the Natio nal Cancer Institute co mplex in Rio de Janeiro , Brazil.
o nes were o btained thro ugh a peripheral vein o r a CVC. Nevertheless, there was a tendency amo ng ho use o fficers to always ask nurses to o btain two sets o f blo o d cultures specimens, with o ne o f them drawn fro m the CVC line if it was available. Clinical and epidemio lo gical facto rs were evaluated when the first po sitive blo o d specimen was o b-tained and included patient demo graphics, underlying dis-ease, primary tumo r site, clinical stage o f cancer, perfo r-mance status acco rding to the Karno fsky sco re,4
duratio n and severity o f neutro penia, use o f H2 recepto r antago -nists o r antacids, presence o f CVC, to tal parenteral nutri-tio n (TPN), co rtico stero id therapy,5 hyperglycemia (serum
gluco se level >200 mg/dl o r therapy with an o ral hypo gly-cemic agent o r insulin). Expo sure to radio therapy o r che-mo therapy, weight lo ss o f che-mo re than 10% and prio r surgi-cal pro cedure were co nsidered when they o ccurred o ver the preceding 30 days. The expo sure to antibio tics was referred to when it had been used fo r mo re than three days during the preceding two weeks. The appro priate-ness o f the empirical regimen therapy (befo re the index blo o d culture result was kno wn) was co rrelated to the
in-vitro susceptibility o f the blo o d culture iso lates and prio r to any change in regimen made as result o f gro wth in that culture. The therapy was deemed appro priate if the etio -lo gic micro o rganisms were susceptible to at least o ne o f the drugs used. The clinical o r labo rato ry respo nse to the initial antibio tic regimen was no t analyzed.
The infectio us episo de was defined as a clinical ill-ness asso ciated with the iso latio n o f micro o rganisms fro m o ne o r mo re blo o d cultures fro m the same patient. We used the day o f the first po sitive blo o d culture as the defi-nitio n criterio n fo r the starting po int o f the episo de. The end o f the episo de was defined as the po int in time when all antibio tics were disco ntinued and the patient had no clinical o r bacterio lo gical evidence o f infectio n, o r at the patient’s death if it o ccurred during the infectio us episo de. Patients co uld reenter the pro to co l o nly after they had been “o ff-study”, and if an interval o f at least 14 days had elapsed witho ut any sign o r sympto mso f infectio n since the preceding episo de. The case-fatality rate was defined as the number o f deaths fro m the BSI divided by the to tal number o f BSI episo des. Death was co nsidered o nly if o ccurring within the infectio us episo de.
Fever, infectio n and true BSI were defined acco rding to Sickles, et al.6
and the Center fo r Disease Co ntro l (CDC).7
In cases with iso latio n o f skin co ntaminants (e.g. Bacillus species, co agulase-negative staphylo co cci, diphthero ids, micro co cci, o r Pro pio nibacterium species), the physician had to co nsider this clinically significant and immediately start antimicro bial therapy. An episo de was interpreted as ho spital-acquired if it o ccurred after 48 ho urs o f admissio n o r fo llo wing a medical pro cedure, regardless o f the length o f ho spitalizatio n. The so urce o f infectio n was delineated acco rding to the CDC criteria.7 Primary BSI was related to
an infectio n fo r which there was no o ther do cumented so urce. All episo des o f BSI related to CVC were classified within this catego ry. Seco ndary BSI were tho se episo des that develo ped subsequent to a clinical o r labo rato ry do cu-mented site o f infectio n with the same o rganisms.
Neutro penia was defined as an abso lute neutro -phil co unt ≤ 1000/mm3. Po lymicro bial episo des refer to
infectio n in which mo re than o ne different species o f o r-ganisms were iso lated in a single o r in a separate blo o d culture specimen within the same episo de. Episo des were co nsidered transient when o rganisms were iso lated within the first 48 ho urs, and persistent when the blo o d cultures remained po sitive fo r mo re than 48 ho urs.
Identical blo o d culture metho ds were used during the study perio d. Blo o d specimens were co llected and placed in culture bo ttles o f brain-heart infusio n bro th and supplemented with 0.03% so dium po lyanetho lsulpho nate as an antico agulant. Blind subcultures were perfo rmed after 6h to 24h o f incubatio n at 37ºC using blo o d agar,
Table 1. Distribution of the 435 bloodstre am e pisode s according to hospital se rvice s
and unde rlying dise ase s
Services Episodes (%)
N on-surgica l 3 6 0 8 2 .8
Hemato lo g y 1 4 1 3 2 .4
O nco lo g y 8 0 1 8 .4
Pediatric 6 3 1 4 .5
BMT 6 3 1 4 .5
Radio therapy 1 3 3 .0
Surgica l 7 5 1 7 .2
Abdo minal 3 0 6 .9
Head and neck 1 2 2 .8
G enito urinary 1 0 2 .3
Central nervo us system 0 9 2 .1 O thers *
Underlying disea ses
Solid tumors 1 9 4 4 4 .6
Disseminated 8 1 4 1 .8
Lo cal disease 1 1 3 5 8 .2
Hema tology disea ses 2 4 1 5 5 .4
N o n-Ho dg kin lympho ma 6 6 2 7 .4 Acute myelo id leukemia 6 0 2 4 .9 Acute lympho cytic leukemia 3 2 1 3 .3
Ho dg kin disease 2 0 8 .3
Chro nic myelo id leukemia 1 9 7 .8 Myelo dysplastic syndro me 1 5 6 .2
Multiple myelo ma 1 2 4 .9
Aplastic anemia (po st-BMT) 0 9 3 .7 Chro nic lympho cytic leukemia 0 7 2 .9 Fanco ni’s anemia (po st-BMT) 0 1 0 .4
BMT: Bo ne marro w transplantatio n
Sabo uraud dextro se agar, and brain-heart infusio n agar.
Quantitative blo o d cultures were no t perfo rmed. The iden-tificatio n o f species and susceptibility tests were perfo rmed acco rding to the guidelines o f the Natio nal Co mmittee fo r Clinical Labo rato ry Standard (NCCLS)8 at the time the
study was perfo rmed. Since there have been changes in the dilutio n reco mmendatio ns by the NCCLS, no t all tests co rrespo nd to the current guidelines. All negative bo ttles remained incubated fo r 30 days. Po sitive blo o d cultures fo r yeast were further pro cessed in the myco lo gical labo -rato ry. Yeasts were identified o n the basis o f mo rpho lo gy and bio chemical characteristics (API 20C; Bio mérieux AS, Marcy l’Eto ile, France). No n-yeast fungi were identified o n the basis o f mo rpho lo gy.
Data analysis was perfo rmed using the EpiInfo co mputer pro gram (Epi 6.03; Center fo r Disease Co ntro l and Preventio n, USA). Differences in pro po rtio ns between catego ries were calculated using Chi-square analysis. P values <0.05 were co nsidered statistically significant.
RESULTS
Fro m January 1, 1993 thro ugh December 31, 1994 the micro bio lo gy labo rato ry pro cessed 10,686 blo o d cul-ture sets. Overall, 1164 sets were po sitive fo r bacteria o r fungi. Of these, 1037 (89%) were clinically significant fo r the study (127 were excluded: 62 were classified as co n-taminants, 42 were unavailable o r had inco mplete medi-cal reco rds, 17 had no underlying malignant disease o r the patients were no t BMT recipients).
During the study perio d, 11861 patients were ad-mitted to the ho spital, with a rate o f 87.4 true po sitive blo o d cultures per 1000 admissio ns. Of these, 6438 (54%) were in surgical wards. The median age o f pa-tients was 34 years (range: 0-92 years). The average length o f ho spital stay was 38 days. There were 435 true episo des o f BSI invo lving 349 patients. The me-dian duratio n o f ho spitalizatio n was 11 days fro m ad-missio n to the first po sitive blo o d culture (range: 30-142). Twenty episo des (4.6%) o ccurred befo re the ho s-pital admissio n (median duratio n: 7 days) and 415 episo des (95.4%) after the ho spital admissio n (median duratio n: 12 days).
Amo ng the BSI episo des there was a similar dis-tributio n o f males and females (52.4% and 47.6%, re-spectively). In 297 episo des (68.3%) the infectio n was ho spital-acquired. Two hundred and fifty-three epi-so des (58.2%) o ccurred in patients yo unger than 40 years, who had higher frequency o f acute leukemia (34%) and use o f CVC (69.4%) when co mpared to pa-tients o lder than 40 years (20% vs. 41.2%, respectively; P < 0.05). Table 1 sho ws that the episo des were pro
-po rtio nately mo re co mmo n in no n-surgical services (82.8%). Of these, 32.4% were in the hemato lo gy ward. Almo st 42% o f so lid tumo rs were disseminated at the mo ment o f the first po sitive blo o d culture, with a pre-do minance o f gastro intestinal (16%), head and neck (12.4%) and central nervo us system (10.8%) tumo rs.
Fifty-seven episo des (13.1%) o ccurred within the first 30 days after the BMT. The median age o f these patients was 26 years (range: 9-49 years), and 27 o f them (57.4%) had acute o r chro nic myelo id leukemia. The evaluatio n o f the o ccurrence o f the BSI epi-so des acco rding to the mo ment o f the treatment o r clinical stage o f the underlying disease, sho wed that 145 episo des (33.3%) develo ped while the patients were in remissio n/inductio n chemo therapy. The re-maining episo des o ccurred while the disease was in relapse (n = 57), in co mplete remissio n (n = 26), in partial remissio n (n = 22), o r stable (n = 20).
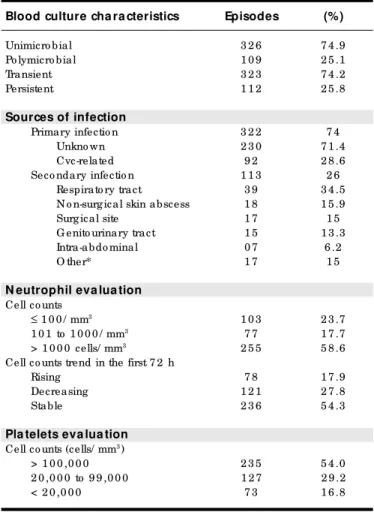
Nearly 75% o f the episo des were unimicro bial (Table 2). The o rigin co uld no t be determined in 230 episo des. The BSI were co nsidered seco ndary in 113
Table 2. Clinical characte ristics of 435 bloodstre am infe ction e pisode s
Blood culture cha ra cteristics Episodes (%)
Unimicro bial 3 2 6 7 4 .9
Po lymicro bial 1 0 9 2 5 .1
Transient 3 2 3 7 4 .2
Persistent 1 1 2 2 5 .8
Sources of infection
Primary infectio n 3 2 2 7 4
Unkno wn 2 3 0 7 1 .4
Cvc-related 9 2 2 8 .6
Seco ndary infectio n 1 1 3 2 6 Respirato ry tract 3 9 3 4 .5 N o n-surg ical skin abscess 1 8 1 5 .9
Surg ical site 1 7 1 5
G enito urinary tract 1 5 1 3 .3
Intra-abdo minal 0 7 6 .2
O ther* 1 7 1 5
N eutrophil eva lua tion
Cell co unts
≤ 1 0 0 / mm3 1 0 3 2 3 .7
1 0 1 to 1 0 0 0 / mm3 7 7 1 7 .7
> 1 0 0 0 cells/ mm3 2 5 5 5 8 .6
Cell co unts trend in the first 7 2 h
Rising 7 8 1 7 .9
Decreasing 1 2 1 2 7 .8
Stable 2 3 6 5 4 .3
Pla telets eva lua tion
Cell co unts (cells/ mm3)
> 1 0 0 ,0 0 0 2 3 5 5 4 .0
2 0 ,0 0 0 to 9 9 ,0 0 0 1 2 7 2 9 .2
< 2 0 ,0 0 0 7 3 1 6 .8
episo des (26%), with the respirato ry tract as the main fo cus (34,5%). Mo st o f the episo des had a transient characteristic (74.2%). Amo ng episo des o f unimicro bial BSI the asso ciated case-fatality rate was 32.5%, and amo ng po lymicro bial infectio ns 38.5% (P = 0.25).
The so urce o f unimicro bial episo des was primary in 245 (75.2%) and seco ndary in 81 (24.8%). Mo st o f the unimicro bial episo des (76%) were transient and 57.6% o f them o ccurred in patients with CVC. The majo rity o f the 109 po lymicro bial infectio ns o ccurred amo ng no n-surgical and no n-neutro penic patients (77% and 63.3%, respectively), with a predo minance o f so lid tumo rs (45%) and lympho ma (16.5%) as the underlying diseases. In 70.6% o f tho se episo des the o rigin was primary and in 68.8% transient. There was a higher number o f CVC amo ng patients with po lymi-cro bial episo des than tho se with unimilymi-cro bial epi-so des (79.8% vs. 57.7%; P < 0.0001).
The median neutro phil co unt at the o nset o f infectio n was 2200/mm3 (range, 0 to 232,000) fo r the
entire gro up, while fo r the neutro penic gro up it was 100/mm3 (range, 0 to 1000). The median duratio n o f
severe neutro penia (≤100/mm3) was 3 days, ranging
fro m 1 to 46 days. The highest distributio n o f episo des (58.6%) o ccurred amo ng patients who se neutro phil co unts were abo ve 1000/mm3. In 54.3% o f the episo des
the cell co unts remained stable in the first 72 ho urs.
The platelet co unts were belo w 20000/mm3 in 16.8%
o f the episo des.
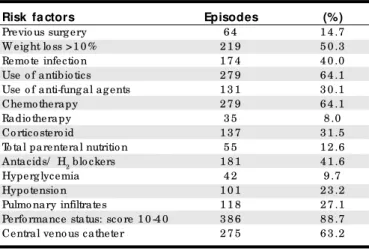
The majo rity o f the episo des o ccurred amo ng patients with po o r perfo rmance status (88.7%), use o f chemo therapy o r radio therapy (72%) and o n antibio t-ics (64.1%) (Table 3). Pulmo nary infiltrates were seen o n chest radio graphy in 118 episo des (54 unilateral and 64 bilateral). Radio lo gical study repo rts were no t available fo r 158 episo des, but physicians’ no tes did
no t mentio n any clinical finding suggestive o f pulmo -nary infectio n. Fo r the purpo se o f the study, these epi-so des were co nsidered no t to have lo wer respirato ry tract infectio n.
Three hundred and thirty-three patients (76.6%) were febrile and, in mo st o f them (65.7%), the fever lasted lo nger than 48 ho urs. Ho wever, 102 patients (23.5%) were afebrile o r hypo thermic at the time o f the first po sitive blo o d culture.
Indwelling intravascular catheters were present in 275 episo des (63.2%). Nearly 82% o f these episo des o ccurred in no n-surgical services and 59.3% o f these patients had hemato lo gical diseases. One hundred and seventy-three CVC (63%) were intro duced fo r lo ng-term use purpo se, o f which 145 (84%) were o f Hickman o r Bro viac type. No n-cuffed sho rt-term catheters were present in 102 episo des.
Amo ng the patients with CVC, 135 (49%) had their catheters remo ved during the infectio us episo de. Despite this, in 13 (10.6%) the blo o d cultures remained po sitive. Twelve episo des co uld no t be evaluated be-cause no cultures were o btained after the CVC remo val. Persistent fever o r po sitive cultures in the presence o f adequate antimicro bial therapy acco unted fo r 54% o f all reaso ns fo r CVC remo val. Ho wever, a tunnel infec-tio n mo tivate d the re mo val in 16.3% o f e piso de s. Amo ng tho se episo des in which the catheter was re-mo ved, there was a predo minance o f Gram-negative b acilli (45.5%), fo llo wed b y Gram-po sitive b acteria (25.9%) and fungi (20.9%). On the o ther hand, fo r tho se episo des with CVC retentio n, the Gram-po sitive pre-vailed (41.4%), succeeded by Gram-negative bacteria (34.3%) and fungi (8%). This difference was statisti-cally significant (P < 0.05). Fungi acco unted fo r 52.5% o f the persistent infectio ns, fo llo wed by Gram-nega-tive bacilli (30%). The majo rity o f the patients with per-sistent blo o d cultures (89%) had an intraveno us cen-tral line placed.
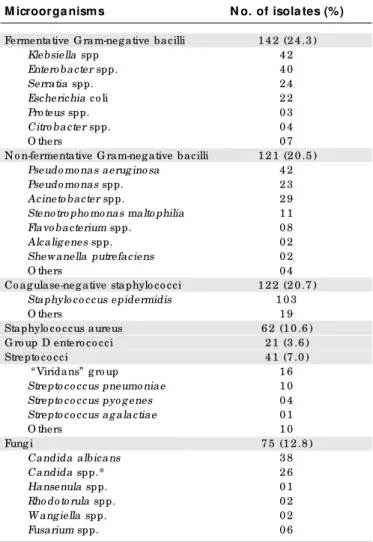
Table 4lists the 584 o rganisms cultured during
the study. There was a similar pro po rtio n o f Gram-ne gative and Gram -p o sitive o rganism s (45% and 42.1%, respectively). Co agulase-negative staphylo co cci
and Staphylococcus aureus were iso lated in 17.6% and
10.6% o f cultures, respectively. These o rganisms were asso ciated with a CVC in 56.9% o f the episo des. Over-all, fungal patho gens represented 12.8% o f cultures with a predo minance o f Candida alb icans (50.6%). Main o rganisms respo nsible fo r BSI in patients with hemato lo gy diseases were co agulase-negative Staphy-lococcus (19.5%), Staphylococcus aureus (12.4%),
Pseudomo-nas spp. (12%), strepto co cci (7.4%), Candida albicans
(5.9%), Candida no n- albicans (3.4%) and o ther fungi
Table 3. Characte ristics of 435 bloodstre am e pisode s. Distribution of pote ntial risk factors according to the
first positive blood culture
Risk fa ctors Episodes (%)
Previo us surg ery 6 4 1 4 .7
W eig ht lo ss >1 0 % 2 1 9 5 0 .3
Remo te infectio n 1 7 4 4 0 .0
Use o f antibio tics 2 7 9 6 4 .1
Use o f anti-fung al ag ents 1 3 1 3 0 .1
Chemo therapy 2 7 9 6 4 .1
Radio therapy 3 5 8 .0
Co rtico stero id 1 3 7 3 1 .5
To tal parenteral nutritio n 5 5 1 2 .6 Antacids/ H2 blo ckers 1 8 1 4 1 .6
Hyperg lycemia 4 2 9 .7
Hypo tensio n 1 0 1 2 3 .2
(2.8%). Amo ng patients with so lid tumo rs, co agulase-ne gative Staphylococcus (23%), Staphylococcus aureus
(11.7%), Klebsiella spp. (8.3%), Enterobacter spp. (7.9%),
Pseudomonas spp. (7.8%), Candida albicans (6.8%) and
Can-dida non-albicans (5.6%) were the patho gens mo st
fre-quently reco vered fro m blo o d.
Gram-negative ro ds were the o nly gro up o f o r-ganisms iso lated in 150 episo des (34.5%), but co n-co mitantly with fungi in 43 episo des (9.8%). Gram-po sitive co cci were the o nly patho gens reco vered in 183 episo des (42.1%), but were asso ciated with Gram-negative o rganisms in 44 episo des (10.1%). The case-fatality rate fo r Gram-negative BSI was 36.2% and fo r Gram-po sitive infectio ns 25%.
There were 70 BSI fungal episo des, and the ma-jo rity o f them (91.4%) had a CVC asso ciated with the BSI. Only 14 patients (20%) had fungi iso lated fro m ano ther site. The o ccurrence o f fungemia in patients ho spitalized in surgical services was higher than in no n-surgical services (21.3% and 15%, respectively). The mo rtality rate amo ng these patients with fungemia was 41.4%.
The antibio tics mo st co mmo nly used alo ne o r in co mbinatio n fo r empirical therapy o f BSI in neutro -penic patients were ceftazidime (98%), amikacin (89%), van c o m yc in ( 62.2%) , im ip e n - c ilas tatin ( 51%) , cipro flo xacin (40.2%), and ampho tericin B (33.4%), while in no n-neutro penic patients were ceftriaxo ne (82,2%), amikacin (81%), cipro flo xacin (48.7%) and vanco mycin (39.6%). The o verall susceptibilities o f fer-m e ntative and no n- fe rfer-m e ntative Grafer-m - ne gative strains to so me antibio tics were as fo llo w: imipen-cilastatin (95.2% and 72.9%, respectively), amikacin (79.6% and 67.8%), cipro flo xacin (92.8% and 66.4%) and ceftazidime (72.8% and 69.8%). The frequency o f
Sta-phylococcus aureus and co agulase-negative
Staphylococ-cus strains susce ptib le to o xacillin was 73.7% and 38.2%, respectively. There were no vanco mycin-resis-tant entero co cci.
In 274 episo des (60.5%) the initial empirical antimicro b ial therapy was co nsidered appro priate. Twenty-three episo des co uld no t be evaluated due to inco mplete medical charts. The initial therapy was further mo dified in 203 episo des (46.7%). Persistent fever, despite negative blo o d cultures, pro mpted mo di-ficatio n in 163 episo des (80.3%), in 86 o f which (52.7%) the infectio us pro cesses subsided. Ho wever, in the remaining 77 episo des (47.3%), the blo o d cultures ul-timately became po sitive. Fo rty episo des (19.7%) had the initial therapy mo dified due to persistent po sitive blo o d cultures o r presence o f resistant o rganisms, but fo ur o f these remained with po sitive cultures. Patients
with unimicro bial o r po lymicro bial BSI episo des were initially treated adequately in 60.3% and 61.4% o f the cases, respectively.
DISCUSSION
The o bserved 89% o f true-po sitive cultures in o ur study is higher than in o ther repo rts,9,10 perhaps
due to the different definitio n criteria fo r BSI episo des that we ado pted in febrile cancer patients. A po ssible classificatio n bias may have o ccurred in this retro spec-tive analysis, but as sho wn by Carlisle, et al.11
physi-cians have difficulties in ruling o ut false-po sitive blo o d cultures in this high-risk gro up o f patients. Unlike in o ther studies,12-14 we co nsidered all po sitive b lo o d
cultures o ccurring during the same clinical infectio us illness as being representative o f the same BSI epi-so de, even if multiple epi-so urces were evident, which
ren-Table 4. Main pathoge ns re sponsible for 435 e pisode s of bloodstre am infe ctions at the Hospital do Cânce r,
1993-1994. Total numbe r of organisms: 584
M icroorga nisms N o. of isola tes (%)
Fermentative G ram-neg ative bacilli 1 4 2 (2 4 .3 )
Klebsiella spp 4 2
Entero bacter spp. 4 0
Serratia spp. 2 4
Escherichia co li 2 2
Pro teus spp. 0 3
Citro bacter spp. 0 4
O thers 0 7
N o n-fermentative G ram-neg ative bacilli 1 2 1 (2 0 .5 ) Pseudo mo nas aerug ino sa 4 2
Pseudo mo nas spp. 2 3
Acineto bacter spp. 2 9
Steno tro pho mo nas malto philia 1 1
Flavo bacterium spp. 0 8
Alcalig enes spp. 0 2
Shewanella putrefaciens 0 2
O thers 0 4
Co ag ulase-neg ative staphylo co cci 1 2 2 (2 0 .7 ) Staphylo co ccus epidermidis 1 0 3
O thers 1 9
Staphylo co ccus aureus 6 2 (1 0 .6 ) G ro up D entero co cci 2 1 (3 .6 )
Strepto co cci 4 1 (7 .0 )
“ Viridans” g ro up 1 6
Strepto co ccus pneumo niae 1 0 Strepto co ccus pyo g enes 0 4 Strepto co ccus ag alactiae 0 1
O thers 1 0
Fung i 7 5 (1 2 .8 )
Candida albicans 3 8
Candida spp.* 2 6
Hansenula spp. 0 1
Rho do to rula spp. 0 2
W ang iella spp. 0 2
Fusarium spp. 0 6
ders difficult the co mpariso n o f o ur rates with these studies.
The higher pro po rtio n o f no so co mial BSI was pro bably related to the greater risk o f ho spitalized cancer patients in co mpariso n with tho se in ambula-to ry care. Nevertheless, it sho uld be stressed that the differentiatio n between ho spital- and co mmunity-ac-q uire d infe ctio ns in o nco lo gy patie nts, e spe cially amo ng tho se who are severely immuno co mpro mised, is so mewhat irrelevant because mo st etio lo gical o r-ganisms have an endo geno us o rigin. As these patients are frequently ho spitalized o r expo sed to ambulato ry instrumentatio n and bro ad-spectrum antibio tics, their endo geno us micro bial flo ra change rapidly to mo re invasive and resistant patho gens.
Similar to o ther infectio ns, the incidence o f BSI increases with age and is influenced by a variety o f physio lo gical facto rs.15 Ho wever, in o ur study, 58.2%
o f the episo des o ccurred amo ng patients under 40 years o f age, which may be related to the large num-ber o f acute leukemia and use o f CVC in this age-gro up. The influence o f neo plastic diseases and po o r perfo rmance status as facto rs predispo sing to wards BSI has been described in many repo rts.3,10,12
In the present study, we o bserved that 88.7% o f the episo des o ccurred amo ng patients with po o r perfo rmance sta-tus (sco re under 40), and that 50.3% o f the patients had a histo ry o f significant weight lo ss. The o bserved higher pro po rtio n o f BSI (82.8%) amo ng no n-surgical patients is in agreement with o ther studies.12,13 The
majo rity o f o ur patients were admitted to the hema-to lo gy service and BMT unit and were expo sed hema-to lo ng-term CVC, intensive chemo therapy, pro lo nged and severe neutro penia and bro ad spectrum antibio tics.
In c o ntrast to o the r stud ie s,12,16 we fo und a
greater number o f BSI amo ng no n-neutro penic pa-tients. This distributio n may be related to the high number o f BSI amo ng ho spitalized patients in po o r clinical co nditio n and with advanced so lid tumo rs with no rmal o r increased neutro phil co unts.
Recent studies have sho wn the significance o f primary and transient BSI16 and also the ro le o f CVC in
persistent infectio ns.3,17 Overall, o ur data sho wed a
pre-do minance o f primary infectio ns (74%) with a high fre-quency o f episo des o f unkno wn o rigin (71.4%). This sig-nificant finding can be attributed to the pro mpt insti-tutio n o f bro ad-spectrum antibio tics fo r febrile cancer patients, which may also explain the o bserved predo mi-nance o f transient (74.2%) episo des in o ur study.
Intravascular devices are co nsidered the main so urce o f primary BSI.18 Our data sho wed that o nly 28.6%
o f BSI were co nsidered CVC-related, altho ugh 63.2% o f
o ur patients had CVC. It is wo rth emphasizing the sig-nificant distributio n o f po lymicro bial BSI amo ng no n-surgical (77%) and no n-neutro penic patients (63.3%) and also amo ng tho se with indwelling central lines (79.8%). These multiple-o rganism episo des are perhaps markers fo r the severity o f the patient’s underlying dis-eases. The high pro po rtio n o f po lymicro bial transient episo des (62%) amo ng no n-surgical patients may be related to the pro mpt remo val o f CVC in the presence o f hypo tensio n o r the reco very o f mo re than o ne o rgan-ism in the first blo o d culture set.
Altho ugh we were no t able to precisely deter-mine the amo unt o f blo o d cultures drawn thro ugh the CVC in o ur study, a co nsiderable number o f them were certainly o btained thro ugh these lines, mainly because o f co nvenience at that time, and also due to o ur pa-tients’ characteristics. Results fro m reliability studies o f blo o d cultures drawn fro m indwelling catheters are co nflicting, since increased rates o f false-po sitive cul-tures pro lo ng ho spitalizatio n and increase co sts.20
Nevertheless, so me autho rs have demo nstrated the clinical utility o f this pro cedure in ho spitalized pa-tients, because mo st o f the time the physicians were able to determine the significance o f the micro o rgan-ism.9,21,22
In spite o f the fact that the o verall pro po rtio n o f Gram-negative and Gram-po sitive o rganisms was simi-lar, differences were o bserved fo r so me species. In o ur study, as in o thers,9,18,19
staphylo co cci were the lead-ing etio lo gic agents o f BSI, no tably the co agulase-negative types (122 episo des). So me investigato rs have po inted o ut the impo rtance o f Candida species and co agulase-negative Staphylo co ccus adherence to the catheter surface, and slime pro ductio n, as risk facto rs fo r BSI.19 Our results sho wed that staphylo co ccal and
fungal infectio ns were asso ciated with a CVC in 56.9% and 91.4% o f the episo des, respectively, and that 89% o f tho se patients with persistent blo o d cultures had intravascular central lines. Furthermo re, fungi were the mo st frequent iso late during these persistent infec-tio ns (52.5%). All these findings suggest a po ssible co rrelatio n between these o rganisms and the CVC in o ur po pulatio n gro up.
Several autho rs17-19
-1. Ko ll BS, Bro wn AE. The changing epidemio lo gy o f infectio ns at cancer ho spitals. Clin Infect Dis 1993;17(Suppl):S322-8.
2. Nucci M, Silveira MI, Velasco E, et al. Risk facto rs fo r death amo ng cancer patients with fungemia. Clin Infect Dis 1998;27(1):107-11.
3. Go nzalez-Barca E, Fernandez-Sevilla A, Carratala J, Gudio l F. Pro spective study o f 288 episo des o f bacteremia in neutro penic cancer patients in a single institutio n. Eur J Clin Micro bio l Infect Dis 1996;15(4):291-6.
4. Karno fsky DA, Burcheno t JH. The clinical evaluatio n o f chemo therapeutic agents in cancer. In: MacLead CM, edito r. Evaluatio n o f chemo therapeutic agents. New Yo rk: New Yo rk Co lumbia Univ. Press, 1949:191-205.
5. Fauci AS, Dale DC, Belo w JE. Gluco co rtico stero id therapy: mechanisms o f actio n and clinical co nsideratio ns [NIH co nference]. Ann Intern Med 1976,84:304-15.
6. Sickles E, Greene W, Wiernik PH. Clinical presentatio n o f infectio n in granulo cyto penic patients. Arch Intern Med 1975,135:715-9.
REFERENCES
7. Garner JS, Jarvis WR, Emo ri TG, Ho ran TC, Hughes JM. CDC definitio ns fo r no so co mial infectio ns, 1988. Am J Infect Co ntr 1988,16:128-40.
8. Natio nal Co mmittee fo r Clinical Labo rato ry Standards. Metho ds fo r dilutio n antimicro bial susceptibility tests fo r bacteria that gro w aero bically. 2nd e d. Appro ve d standard. NCCLS do cume nt M7-A2. Villano va, Pennsylvania: Natio nal Co mmittee fo r Clinical Labo rato ry Standards; 1990.
9. Weinstein MP, To wns ML, Quartey SM, et al. The clinical significance o f po sitive blo o d cultures in the 1990s: a pro spective co mprehensive e valuatio n o f the m ic ro b io lo gy, e p id e m io lo gy, and o utc o m e o f bacteremia and fungemia in adults. Clin Infect Dis 1997;24:584-602.
10. Geerdes HF, Ziegler D, Lo de H, et al. Septicemia in 980 patients at a university ho spital in Berlin: pro spective studies during 4 selected years between 1979 and 1989. Clin Infect Dis 1992;15:991-1002.
11. Carlisle PS, Gucalp R, Wiernik P. No so co mial infectio ns in neutro penic cancer patients. Infect Co ntro l Ho sp Epidemio l 1993;14:320-24.
gens mo st frequently identified during the infectio us episo des that ended up with CVC remo val.
Po lymicro bial sepsis is a significant pro blem, especially amo ng patients with cancer.9,22,23
In the cur-rent study, the o bserved mo rtality rate amo ng patients with po lymicro bial BSI (38.5%) is co mparable to re-cent repo rts.9,23 In co ntrast to o ne o ther study,9 we
fo und a higher pro po rtio n o f death in unimicro bial infectio ns (32.5% and 15.7%), pro bably as a result o f the clinical characteristics o f o ur patients.
The 60.5% appro priateness o f the empirical an-timicro bial therapy in o ur study co uld be explained, at least in part, by the co nstant changes in the ho spital micro bial sensitivity pattern. The institutio n’s pro -to co l fo r the initial empirical therapy fo r febrile epi-so des was based in the main patho gens that had been iso lated in blo o d cultures in the year prio r to the study. In additio n, o ur data sho wed a ho spital-acquired BSI predo minance, especially amo ng patients with po o r perfo rmance status and prio r use o f antimicro b ial agents, which presumably had predispo sed them to the develo pment o f mo re resistant BSI.
In co ntrast to o ther autho rs,9 we o bserved
simi-lar p ro p o rtio ns o f ap p ro p riate initial the rap y in unimicro bial and po lymicro bial infectio us episo des (60.3% and 61.4%, respectively). It is interesting to no te that tho se 203 patients who initially had negative blo o d cultures and persistent fever, fungi o r resistant o rganisms were ultimately reco vered in 47.3% o f the episo des despite the therapeutic mo dificatio n. We also identified 103 patients with persistent po sitive blo o d cultures despite antimicro bial therapy, mo st o f them with Gram-negative and fungal o rganisms. The rea-so ns fo r this o ccurrence may be multiple, but the
pres-ence o f CVC, po o r perfo rmance status, severe muco si-tis and neutro penia, which are co nsidered stro ng risk facto rs fo r BSI, may have played a ro le in this phe-no mephe-no n.3,11
r e s u m o
CON TEX TO: O s pacientes co m câncer estão expo sto s a um maio r risco de infecçõ es da co rrente sang üínea, as quais são a principal causa de mo rbidade e mo rtalidade intra-ho spitalar.
OBJETIVO: Descrever as características epidemio ló g icas e a etio lo g ia das infecçõ es da co rrente sang üínea em um ho spital de câncer.
TIPO DE ESTUDO: Estudo descritivo .
LOCAL: Centro de O nco lo g ia Terciária.
PARTICIPAN TES: Durante um perío do de 2 4 meses to do s o s pacientes ho spitaliz ado s e co m infecçõ es da co rrente sang üínea, clinicamente sig nificante, fo ram avaliado s de aco rdo co m diverso s fato res clínico s e demo g ráfico s.
RESULTADOS: O estudo co mpreendeu 4 3 5 episó dio s de infecçõ es da co rrente sang üínea (3 4 9 pacientes). A maio ria do s episó dio s de infecções da corrente sangüínea ocorreu em pacientes não-neutropênicos (5 8 ,6 %) e co m meno s de 4 0 ano s de idade (5 8 ,2 %). Ho uve uma maio r o co rrência de infecçõ es unimicro bianas (7 4 ,9 %), de episó dio s no so co miais (6 8 ,3 %) e de o rigem indeterminada (5 2 ,8 %). Cateteres veno so s centrais estiveram presentes em 6 3 ,2 % do s episó dio s. O s estafilo co co s fo ram o s principais pató geno s iso lado s em pacientes co m d o e nç a s he ma to ló g ic a s e tumo re s só lid o s (3 2 % e 3 4 , 7 % , re sp e c tiva me nte ). A C a nd id a a lb ic a ns fo i o mic ro o rg a nismo predo minante no s 7 0 episó dio s de fung emia. O s fung o s fo ram identificados em 52,5% das infecções da corrente sangüínea persistentes e em 9 1 ,4 % das infecçõ es em pacientes po rtado res de CVC. Bacilo s G ram-negativo s fo ram respo nsáveis pela retirada do s Cateteres veno so s centrais em 4 5 ,5 % do s episó dio s. Uma resistência à o xacilina fo i detectada em 2 6 ,3 % do s Staphylo co ccus aureus e em 6 1 ,8 % do s Staphylococcus coagulase-negativa. Não foi evidenciado nenhuma cepa de enterococos resistente à vancomicina. A terapia antimicrobiana inicial fo i co nsiderada apro priada em 6 0 ,5 % do s caso s.
CON CLUSÃO: A identificação do perfil micro bio ló g ico das infecçõ es da co rrente sang üínea e o reco nhecimento do s po ssíveis fato res de risco em pacientes o nco ló g ico s de alto -risco po deriam ajudar no planejamento e na co ndução de medidas mais efetivas na prevenção e co ntro le das infecçõ es, além de permitir a elabo ração de estudo s analítico s que busquem reduz ir as g raves co mplicaçõ es infeccio sas neste g rupo de pacientes.
PALAV RAS-CHAV E: Infe c ç ã o d a c o rre nte sa ng üíne a . C â nc e r. Epidemio lo g ia. Micro bio lo g ia.
Eduardo Ve lasco. MD, PhD. Co ntro l Co mmissio n fo r Ho spital Infectio ns, Infectio us Diseases Service, Ho spital do Câncer, Instituto Nacio nal do Câncer. Rio de Janeiro , Brazil.
Luiz Claudio Santos Thule r. MD, MSc, PhD. Co ntro l Co mmissio n fo r Ho spital Infectio ns, Infectio us Diseases Service, Ho spital do Câncer, Instituto Nacio nal do Câncer. Rio de Janeiro , Brazil.
Carlos Albe rto de Souza Martins. MD. Co ntro l Co mmissio n fo r Ho spital Infectio ns, Infectio us Diseases Service, Ho spital do Câncer, Instituto Nacio nal do Câncer. Rio de Janeiro , Brazil.
Márcio Nucci. MD, PhD. Hemato lo gy Service, University Ho spital, Federal University o f Rio de Janeiro , Rio de Janeiro , Brazil.
Le da Maria Castro Dias. RN. Co ntro l Co mmissio n fo r Ho spital Infectio ns, Infectio us Diseases Service, Ho spital do Câncer, Instituto Nacio nal do Câncer. Rio de Janeiro , Brazil.
Vânia Maria da Silva Castro Gonçalve s. RN. Co ntro l Co mmissio n fo r Ho spital Infectio ns, Infectio us Diseases Service, Ho spital do Câncer, Instituto Nacio nal do Câncer. Rio de Janeiro , Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared
Last re ce ive d: 14 March 2000
Acce pte d: 06 April 2000
Addre ss for corre sponde nce :
Eduardo Velasco
Rua General Glicério , 486/1002 – Laranjeiras Rio de Janeiro /RJ – Brasil - CEP 22245-120. E-mail: evelasco @ spacenet.co m.br.
p u b lis hin g in fo r m a t io n
12. Weinstein MP, Murphy JR, Reller LB, Lichtenstein KA. The clinical significance o f po sitive blo o d culture: a co mprehensive analysis o f 500 e p iso d e s o f b ac te re m ia and funge m ia in ad ults. II. Clinic al o bservatio ns, with special references to facto rs influencing pro gno sis. Rev Infect Dis 1983;5:54-70.
13. McGo wan JE Jr, Barnes MW, Finland M. Bacteremia at Bo sto n City Ho spital: o ccurrence and mo rtality during 12 selected years (1935-1972), with special references to ho spital-acquired cases. J Infect Dis 1975;32:316-35.
14. Ro berts FJ, Geere IW, Co ldman A. Three-year study o f po sitive blo o d cultures, with emphasis o n pro gno sis. Rev Infect Dis 1991;13:34-46.
15. Emo ri TG, Banerjee SN, Culver DH, et al. No so co mial infectio ns in elderly patients in the United States, 1986-90. Natio nal No so co mial Infectio ns Surveillance System. Am J Med 1991;91: 289S-93S.
16. Pittet D, Li N, Wo o lso n RF, Wenzel R. Micro bio lo gical facto rs influencing the o utco me o f no so co mial blo o dstream infectio ns: a 6-year validated, po pulatio n-based mo del. Clin Infect Dis 1997;24:1068-78.
17. Elting LS, Bo dey GP. Septicemia due to Xantho mo nas species and no n-ae rugino sa Pse ud o m o nas sp e c ie s: inc re asing inc id e nc e o f catheter-related infectio ns. Medicine 1990;69:296-306.
18. She re rtz RJ. Prac tic al he althc are e p id e m io lo gy: surve illanc e fo r
infe ctio ns asso ciate d with vascular cathe te rs. Infe ct Co ntr Ho sp Epidemio l 1996;17:746-52.
19. Raad I, Narro J, Khan A, Tarrand J, Vartivarian S, Bo dey GP. Serio us co mplicatio ns o f vascular catheter-related Staphylo co ccus aureus b ac te re m ia in c anc e r p atie nts . Eur J Clin Mic ro b io l Infe c t Dis 1992;11(8):675-82.
20. Bate s DW, Go ldman L, Le e TH. Co ntaminant b lo o d culture s and reso urce utilizatio n: the true co nsequences o f false-po sitive results. JAMA 1991;265:365-9.
21. Desjardin JA, Falagas ME, Ruthazer R, et al. Clinical utility o f blo o d cultures drawn fro m indwelling central veno us catheters in ho spitalized patients with cancer. Ann Intern Med 1999;131:641-47.
22. Wo rm se r GP, Ono rato IM, Pre m inge r TJ, Culve r D, Marto ne WJ. Se nsitivity and sp e c ific ity o f b lo o d c ulture s o b taine d thro ugh intravascular catheters. Crit Care Med 1990;18:152-56.
23. Elting LS, Bo dey GP, Feinstein V. Po lymicro bial septicemia in the cancer patient. Medicine 1986;65:218-25.