Alcohol Consumption and the Neoplastic Progression in
Barrett’s Esophagus: A Systematic Review and
Meta-Analysis
Zhifeng Lou1, Haibo Xing2, Da Li3*
1The department of stomatology, Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine, Hangzhou, Zhejiang, P. R. China,2The department of intensive care unit, Xiasha Hospital, Hangzhou, Zhejiang, P. R. China,3Department of Medical Oncology, Sir Run Run Shaw Hospital Affiliated to Zhejiang University School of Medicine, Hangzhou, Zhejiang, P. R. China
Abstract
Purpose:In the developed countries, the incidence of esophageal adenocarcinoma (EAC) is increasing over recent decades. The purpose of this meta-analysis was to arrive at quantitative conclusions about the contribution of alcohol intakes and the progression of Barrett’s esophagus.
Methods:A comprehensive, systematic bibliographic search of medical literature published up to Oct 2013 was conducted to identify relevant studies. A meta-analysis was conducted for alcohol consumption on the Barrett’s esophagus progression.
Results:A total of 882 cases in 6,867 individuals from 14 observational studies were indemnified in this meta-analysis. The result of this current meta-analysis, including 10 case-control and 4 cohort studies, indicated that alcohol consumption was not associated with the neoplastic progression in Barrett’s esophagus (RR, 1.17; 95% CI, 0.93–1.48). When stratified by the study designs, no significant association was detected in either high vs low group or ever vs never group.
Conclusions: Alcohol drinking is not associated with risk of neoplastic progression in Barrett’s esophagus. Further well designed studies are needed in this area.
Citation:Lou Z, Xing H, Li D (2014) Alcohol Consumption and the Neoplastic Progression in Barrett’s Esophagus: A Systematic Review and Meta-Analysis. PLoS ONE 9(10): e105612. doi:10.1371/journal.pone.0105612
Editor:Ken-ichi Mukaisho, Shiga University of Medical science, Japan
ReceivedNovember 23, 2013;AcceptedJuly 25, 2014;PublishedOctober 9, 2014
Copyright:ß2014 Lou et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding:The authors acknowledge the financial support from Chinese National Natural Science Foundation (Project NO. 81001034), Zhejiang Medicines Health Science and Technology Program (NO. 2009B087) and Sir Run Run Shaw Hospital Potential Doctor Foundation for Da Li. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests:The authors have declared that no competing interests exist. * Email: [email protected]
Introduction
The incidence rate of Barrett’s esophagus in the patients with gastroesophageal reflux disease (GERD) was 10% to 15% [1]. Endoscopic surveillance has been recommended for patients with Barrett’s esophagus because of its association with esophageal adenocarcinoma (EAC). In the developed countries, the incidence of EAC increased over recent decades [2,3]. Barrett’s esophagus, which is a condition of the distal esophagus in which the normal stratified squamous epithelium is replaced by specialised intestinal metaplasia, is a recognized precursor of EAC. The metaplasia in Barrett’s esophagus patients accumulates genetic alterations and can progress through dysplasia to EAC.
Factors that may be associated with an increased risk of Barrett’s esophagus or EAC were examined, including: age, gender, ethnicity, smoking, alcohol use, Barrett segment length, hiatal hernia presence and size,Helicobacter pyloristatus, presence and duration of GERD symptoms, and proton pump inhibitor (PPI) use and duration. However, the risk factors of the neoplastic progression in the Barrett’s esophagus remained unclear. Alcohol,
as a risk factor of several kinds of cancers [4], was reported to be associated with the incidence of both Barrett’s esophagus and EAC. However, the effect of alcohol intake on the neoplastic progression in Barrett’s esophagus was still unclear.
Meta-analysis is a useful statistical tool to pool the relevant studies together and gain a more powerful conclusion. The meta-analysis was also used in the search for potential causes of EAC. For instance, based on a combination of 4 cohorts and 31 case-control studies, Salehi M et al found that low levels of red and processed meat consumption and higher levels of fish intake might reduce esophageal cancer risk [5]. Although early studies made several attempts to summarize the epidemiologic evidence on alcohol drinking and the progression of Barrett’s esophagus, to our knowledge, no meta-analyses have ever been conducted in a standardized manner. To quantitatively assess the potential relationship, we conducted a comprehensive meta-analysis of case-control and cohort studies conducted between 1993 and 2013.
Methods
Search Strategy and Inclusion Criteria
As a analysis of observational studies, this current meta-analysis was conducted according to the PRISMA guidelines and MOOSE guidelines [6,7]. A systematic search of Pubmed and Embase databases was conducted for relevant literature published up to Oct. 2013 with the key words ‘‘esophag*’’, ‘‘adenocarcino-ma’’, ‘‘carcino‘‘adenocarcino-ma’’, ‘‘cancer’’ in combine with ‘‘Barrett’s esoph-agus’’ and ‘‘alcohol’’, ‘‘drink’’ or ‘‘wine’’ or ‘‘beer’’. No language or any other restrictions were set in the search strategy. In addition, we also manually searched the reference lists to detect additional eligible studies. When different articles from the same dataset were obtained, only the most recent study with available data was included in the meta-analysis. The contact with the corresponding author of certain article was conducted when more data was required.
Studies satisfying the following criteria were included in the observational meta-analysis: (1) the association between alcohol consumption and risk of Barrett’s esophagus progression; (2) a cohort or case-control study design was obtained; (3) the value of relative risk (RR), odds ratio (OR) with 95% confidence intervals (CI) or enough data to calculate them were reported.
Data Extraction and Assessment of Study Quality Two reviewers (ZL and HX) independently extracted the data and any discrepancy was checked again and resolved through discussion. The following data was extracted from each article: name of the first author, publishing year, study design, study site, age and gender of participants, type and amount of cases, adjustments of the confounding factors, and the OR/RR value with 95% CI.
Quality assessment that was performed by two reviewers back to back and any disagreement was discussed with the third reviewer. Considering the observational study design of the included studies, the Newcastle-Ottawa Scale (NOS) was obtained to assess the methodological quality of the included studies [8]. It assessed the selection, comparability and exposure of a case-control study, while the selection, comparability and outcome of a cohort study. A maximum of 9 stars was scored for a study and the study with over 6 stars would be regarded as relative high quality.
Statistical Methods for the Meta-analysis
Homogeneity of RR across studies was assessed by using the Cochrane Q statistic and I2statistic. WhenPfor the heterogeneity ,0.1 and I2
.50%, the interstudy heterogeneity would be considered statistically significant. Both OR and RR were reported in the included studies and the OR was obtained to approximate RR in this meta-analysis. When both crude and adjusted OR/RR values were offered in the article, only the adjusted ones were adopted for the meta-analysis. A random-effects model was obtained to estimate the pooled random-effects, thus it would provide a more conservative conclusion. The effects of alcohol drinking on the incidence of Barrett’s esophagus progres-sion were measured with the OR with 95% CI. The sensitivity analyses were conducted to detect the robustness of the conclusions by two independent methods. Firstly, we conducted a sensitivity analysis to investigate the influence of a single study on the overall risk estimate by omitting one study in each turn. Secondly, we excluded the studies with a relative lower method-ological quality and assess the effect of alcohol consumption and risk of progression of Barrett’s esophagus.
We constructed a funnel plot with logRR and their SEs of logRR by visual inspection to assess the potential publication bias.
Besides, potential publication bias was also assessed by both Begg’s rank correlation test [9] and Egger linear regression test [10] at the p,0.10 level of significance. All analysis was performed using STATA version 12.0 statistical software (Stata Corp LP, College Station). A p value,0.05 was considered as statistically significant.
Results
Identification and Selection of Studies
A total of 433 articles (198 from Pubmed and 235 from EMBASE) were identified from the electronic database searching. Besides, 131 more records were identified through consulting the reference lists of the relevant reviews and articles. After excluding 382 articles with unrelated topics, a total of 182 records were detailed evaluated. Among the 182 articles, 31 full-texts were assessed for eligibility after removing 151 articles (reviews, case reports and overlapped articles). Subsequently 2 articles were duplicated reports from previous data and 15 ones in which the data not in usable format were excluding from the inclusion and in final, a total of 14 studies were included for the quantitative synthesis [11–24]. Figure 1 demonstrated the selection of studies.
Study Characteristics and Quality
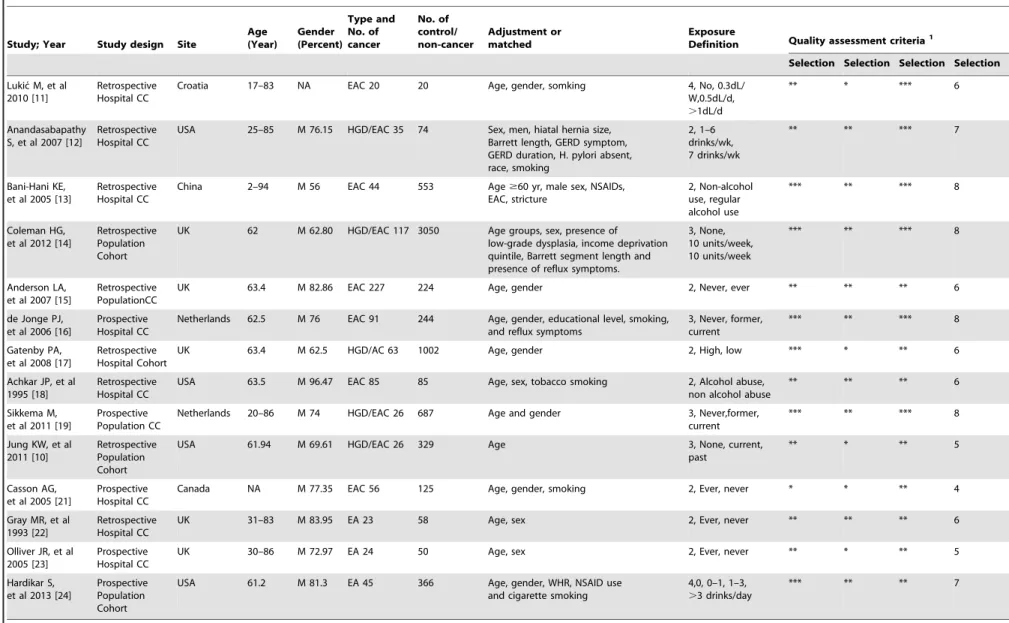
A total of 882 cases and 6,867 individuals in 14 observational studies were indemnified in this current meta-analysis. All the detailed characteristics of each included study were presented in Table 1. The included studies were published between 1993 and 2013. A total of 4 cohort studies and 11 case-control studies were identified in this current meta-analysis. Among all the included studies, 8 studies were in European, 5 in Americas and 1 in Asia. The age, gender distribution, categories of alcohol consumption, and adjustments of confounding factors were demonstrated in Table 1.
The NOS were obtained to assess the selection, comparability and exposure of the case-control study, while the selection, comparability and outcome of the cohort study. All the scores of each part in the evaluation of all the studies were displayed in Table 1. Eleven in nine studies were in relative high quality (over 6 stars) and the mean NOS score was 6.43 stars (standard deviation: 1.28).
Alcohol Consumption and Neoplastic Progression in Barrett’s Esophagus
CI, 0.85–1.18) nor ever vs never group. All the results of the subgroup analysis were presented in Table 2.
Heterogeneity, Sensitivity analysis and Publication bias The heterogeneity was significant when all the 14 studies were pooled in the meta-analysis (I2, 41.3%; P= 0.063). We tried to explore the source by excluding the included studies one by one and re-count the heterogeneity. When one study [18] was removed from the meta-analysis and the heterogeneity became non-significant (I2, 9.2%; P= 0.769). The result of this current meta-analysis didn’t change when that study was excluded (RR, 0.99; 95% CI, 0.85–1.16).
A one-way sensitivity analysis was conducted and there was little change in the quantitative summary measure of RR or 95% CI. Although one studies [15] seemed to slightly influence the results, there was no change to the direction of effect, when anyone study was excluded. Besides, we just included the articles with a relative high quality (over 6 stars NOS score in the meta-analysis); however, no significant association was detected neither (n = 11; RR, 1.21; 95% CI, 0.93–1.58). A significant heterogeneity should be noted as well (I2= 50.1%,P= 0.029).
Evidence of publication bias for studies in this current meta-analysis wasn’t noted in symmetrical funnel plot on visual inspection (Figure S1). Both Begg’s graph and Egger’s test were obtained to detect the potential publishing bias. No significant publication bias was found in this current meta-analysis (Begg’s test,P= 0.381; Egger’s test,P= 0.645).
Discussion
A total of 882 EAC cases in 6,867 individuals from 14 observational studies were identified in this meta-analysis. The result of this meta-analysis, including 10 case-control and 4 cohort studies, indicated that alcohol consumption was not associated with the neoplastic progression in Barrett’s esophagus. Meanwhile,
this result was demonstrated in the most subgroup analyses by study design, study sites, end points. However, the studies conducted in the Americas showed that alcohol drinking increased the neoplastic risk. When stratified by the study designs, no significant association was detected in either high vs low group or ever vs never group. The heterogeneity was not significant when all the 14 studies were pooled in the meta-analysis. Publication bias was not detected in the meta-analysis. The results of the sensitivity analysis suggest that the conclusions of this study were quite robust.
EAC is now a more and more serious problem in the entire world [25]. It affects the life quality of the patients with EAC. While risk factors for the development of EAC in the general population have been well investigated, it is largely unclear which kinds of patients with Barrett’s esophagus have an increased risk for malignant progression. It is important to detect the harmful or protective factors for the EAC in the Barrett’s esophagus patient and it might help in the primary prevention. The realization of the relationship between the modifiable epidemiological factors and neoplastic progression in Barrett’s esophagus would provide a more effective strategy for the cancer prevention in the future. Alcohol consumption, which was related with the incidence of both the Barrett’s esophagus and EAC, was considered to play a role in the progression from Barrett’s esophagus to the EAC. However, inconsistent evidence exists regarding the effect of alcohol consumption on the neoplastic progression in Barrett’s esophagus.
In this meta-analysis, we found that alcohol consumption is not associated with progression of Barrett’s esophagus. This result supports the conclusions of several previous studies. In 2003–2004, a prospective, multicenter cohort study including 713 patients with Barrett’s esophagus was conducted. After 4 years of follow-up, duration of Barrett’s esophagus of$10 years, length of Barrett’s esophagus, esophagitis, and LGD were significant predictors of progression to HGD or EAC; however, alcohol intake was not Figure 1. Flow chart of the literature search.A totaol of 14 observational studies (10 case-control and 4 cohort studies) were indemnified in this meta-analysis.
doi:10.1371/journal.pone.0105612.g001
Alcohol and Progression of Barrett’s Esophagus
Table 1.Characteristics of eligible studies.
Study; Year Study design Site
Age (Year) Gender (Percent) Type and No. of cancer No. of control/ non-cancer Adjustment or matched Exposure
Definition Quality assessment criteria1
Selection Selection Selection Selection
Lukic´ M, et al 2010 [11]
Retrospective Hospital CC
Croatia 17–83 NA EAC 20 20 Age, gender, somking 4, No, 0.3dL/
W,0.5dL/d, .1dL/d
** * *** 6
Anandasabapathy S, et al 2007 [12]
Retrospective Hospital CC
USA 25–85 M 76.15 HGD/EAC 35 74 Sex, men, hiatal hernia size, Barrett length, GERD symptom, GERD duration, H. pylori absent, race, smoking
2, 1–6 drinks/wk, 7 drinks/wk
** ** *** 7
Bani-Hani KE, et al 2005 [13]
Retrospective Hospital CC
China 2–94 M 56 EAC 44 553 Age$60 yr, male sex, NSAIDs,
EAC, stricture
2, Non-alcohol use, regular alcohol use
*** ** *** 8
Coleman HG, et al 2012 [14]
Retrospective Population Cohort
UK 62 M 62.80 HGD/EAC 117 3050 Age groups, sex, presence of low-grade dysplasia, income deprivation quintile, Barrett segment length and presence of reflux symptoms.
3, None, 10 units/week, 10 units/week
*** ** *** 8
Anderson LA, et al 2007 [15]
Retrospective PopulationCC
UK 63.4 M 82.86 EAC 227 224 Age, gender 2, Never, ever ** ** ** 6
de Jonge PJ, et al 2006 [16]
Prospective Hospital CC
Netherlands 62.5 M 76 EAC 91 244 Age, gender, educational level, smoking, and reflux symptoms
3, Never, former, current
*** ** *** 8
Gatenby PA, et al 2008 [17]
Retrospective Hospital Cohort
UK 63.4 M 62.5 HGD/AC 63 1002 Age, gender 2, High, low *** * ** 6
Achkar JP, et al 1995 [18]
Retrospective Hospital CC
USA 63.5 M 96.47 EAC 85 85 Age, sex, tobacco smoking 2, Alcohol abuse,
non alcohol abuse
** ** ** 6
Sikkema M, et al 2011 [19]
Prospective Population CC
Netherlands 20–86 M 74 HGD/EAC 26 687 Age and gender 3, Never,former,
current
*** ** *** 8
Jung KW, et al 2011 [10]
Retrospective Population Cohort
USA 61.94 M 69.61 HGD/EAC 26 329 Age 3, None, current,
past
** * ** 5
Casson AG, et al 2005 [21]
Prospective Hospital CC
Canada NA M 77.35 EAC 56 125 Age, gender, smoking 2, Ever, never * * ** 4
Gray MR, et al 1993 [22]
Retrospective Hospital CC
UK 31–83 M 83.95 EA 23 58 Age, sex 2, Ever, never ** ** ** 6
Olliver JR, et al 2005 [23]
Prospective Hospital CC
UK 30–86 M 72.97 EA 24 50 Age, sex 2, Ever, never ** * ** 5
Hardikar S, et al 2013 [24]
Prospective Population Cohort
USA 61.2 M 81.3 EA 45 366 Age, gender, WHR, NSAID use
and cigarette smoking
4,0, 0–1, 1–3, .3 drinks/day
*** ** ** 7
NA: not available; CC: case-control study; LGD: low-grade dysplasia; EAC: esophageal adenocarcinoma; NASID: non-steroids antiinflammatory drugs; GERD: gastroesophageal reflux disease; WHR: waist-to-hip ratio; BMI: bady mass index; BE: Barrett esophagus; M: male.
1The study quality was assessed by Newcastle-Ottawa Scale.
associated with the progression of Barrett’s esophagus (RR, 1.5; 95% CI, 0.3–6.7). In a hospital-based case-control study in which 91 cases with EAC and 244 controls with histologically confirmed Barrett’s esophagus (.2 cm) with no dysplasia or low-grade dysplasia were included, current alcohol use was not associated the incidence of EAC (RR, 1.6; 95% CI, 0.6–4.3) [16]. The data from patients with Barrett’s esophagus identified from the population-based Northern Ireland Barrett’s esophagus register, diagnosed between 1993 and 2005 with specialized intestinal metaplasia (n = 167) was analyzed and the result showed alcohol intake was not associated with increased risk of HGD or EAC after adjusting for several confounding factors (RR, 0.82; 95% CI, 0.41–1.62). When the subgroup analyses stratified by the study designs was conducted, the associations between alcohol consumption and Barrett’s esophagus progression wasn’t detected in neither case-control nor cohort studies. As we know, the cohort study design could avoid the potential recall bias and would provide more credible conclusions. A consistent result is obtained in both the case-control and cohort studies and it suggests that the result of this meta-analysis is quite credible.
However, the studies conducted in the Americas showed that alcohol drinking was a risk factor of the progression of Barrett’s esophagus. The geographical differences, the diet diversity and ethnic and genetic disparity are the possible reasons. Alcohol consumption, which was classified as beer, liquor and wine intake, might demonstrate different effect in the development of Barrett’s
esophagus. The difference of the drinking habits in each region might cause the results. Besides, the relatively small number of studies included in the subgroup analyses (5 in the Americas and 1 in the Africa) might lead to the instability of the conclusions. When stratified by the end points, no significant association was detected in either HGD or EAC or just EAC. It suggests that alcohol might be not associated in any stage of the Barrett’s esophagus progression.
To our best knowledge, this is the first meta-analysis involving the relationship between alcohol consumption and risk of development of Barrett’s esophagus. There are some strengths of this work. In the literature search, a large number of subjects were evaluated for the detection of the effect of the neoplastic risk in Barrett’s esophagus associated with alcohol drinking. Besides, through two independent methods, the publication bias wasn’t significant. The results of the sensitivity analysis suggest that the conclusions of this study were quite robust. These above results demonstrated that the conclusions of this meta-analysis were quite persuasive.
Despite these advantages mentioned above, some limitations of the current meta-analysis should be acknowledged. First, the definitions of the case groups were not uniformly defined. Both the patients without higher alcohol intake or ever alcohol intake were obtained as the controls in the included studies. This would produce potential misclassification bias. While the subgroup analyses showed that no different results were detected and thus Figure 2. Forest plot of the association between alcohol drinking and risk of Barrett’s esophagus progressiom.
doi:10.1371/journal.pone.0105612.g002
Alcohol and Progression of Barrett’s Esophagus
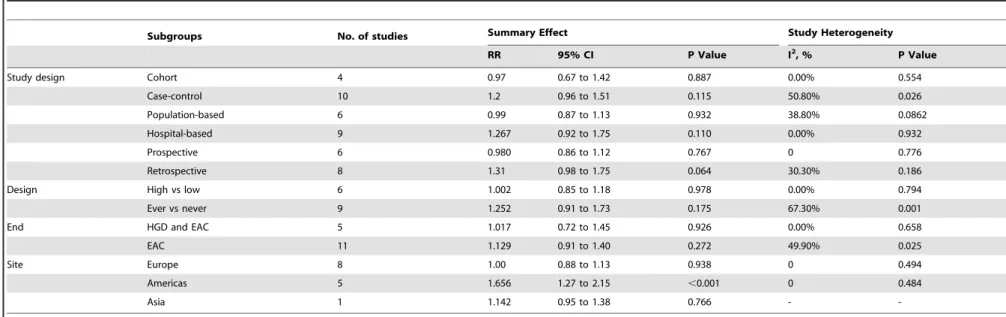
Table 2.Subgroup analysis of alcohol consumption and BE progression with combined RR.
Subgroups No. of studies Summary Effect Study Heterogeneity
RR 95% CI P Value I2, % P Value
Study design Cohort 4 0.97 0.67 to 1.42 0.887 0.00% 0.554
Case-control 10 1.2 0.96 to 1.51 0.115 50.80% 0.026
Population-based 6 0.99 0.87 to 1.13 0.932 38.80% 0.0862
Hospital-based 9 1.267 0.92 to 1.75 0.110 0.00% 0.932
Prospective 6 0.980 0.86 to 1.12 0.767 0 0.776
Retrospective 8 1.31 0.98 to 1.75 0.064 30.30% 0.186
Design High vs low 6 1.002 0.85 to 1.18 0.978 0.00% 0.794
Ever vs never 9 1.252 0.91 to 1.73 0.175 67.30% 0.001
End HGD and EAC 5 1.017 0.72 to 1.45 0.926 0.00% 0.658
EAC 11 1.129 0.91 to 1.40 0.272 49.90% 0.025
Site Europe 8 1.00 0.88 to 1.13 0.938 0 0.494
Americas 5 1.656 1.27 to 2.15 ,0.001 0 0.484
Asia 1 1.142 0.95 to 1.38 0.766 -
-HGD: high-grade dysplasia; EAC: esophageal adenocarcinoma; RR, relative risk; CI, confidence interval. doi:10.1371/journal.pone.0105612.t002
Alcohol
and
Progres
sion
of
Barrett’s
Esophagu
s
PLOS
ONE
|
www.ploson
e.org
6
October
2014
|
Volume
9
|
Issue
10
|
this might produce no serious problem. Secondly, even the categories of alcohol consumption are reported in some studies; however, the data were varied and broad. Thus, we were unable to determine the dose-response association between alcohol con-sumption and progression of Barrett’s esophagus. Third, it has been argued that because meta-analyses of observational studies may produce very precise, but spurious, results, a statistical combination of these data should not be the prominent component. However, considering that as an etiology exploring nature of this study, the pooled results of the observational studies would also provide certain improvement of the knowledge of the neoplastic development. The end, a combination of prognostic factors has been suggested to be required to define subgroups of patients at an increased risk of progression. However, the data of the included studies reported no sufficient data for an advanced research, which demonstrated the potential breakthrough. The forth, the understanding of the Barrett’s esophagus has developed in the recent years. The old conception says that although several different kinds of columnar epithelium can be found in the lower esophagus, it is only specialized intestinal metaplasia (SIM), distinguished by the presence of goblet cells, which increased the cancer risk. However, nowadays recent studies revealed that cardiac-type mucosa, columnar lined esophagus without goblet cells, also have the posibility of cancer development. With the development of understanding of Barrett’s esophagus, the older papers might provide results based on inaccurate definitions and
thus the bias could not be ignored. Advanced well-designed studies based on both endoscopic results and histocytology are wanted in the future.
In conclusion, on the basis of epidemiologic evidence, we found that alcohol consumption was not a neoplastic risk in Barrett’s esophagus. To get a more definitive conclusion, further pooled analyses with more complete raw data or prospective cohort studies with larger sample size, well controlled confounding factors and longer duration of follow-up are needed in this area.
Supporting Information
Figure S1 The funnel plot of all the included studies.
Evidence of publication bias for studies in this current meta-analysis wasn’t noted in symmetrical funnel plot on visual inspection.
(TIF)
Checklist S1 PRISMA checklist.
(DOC)
Author Contributions
Conceived and designed the experiments: ZL HX DL. Performed the experiments: ZL HX DL. Analyzed the data: ZL HX DL. Contributed reagents/materials/analysis tools: ZL HX DL. Wrote the paper: ZL HX DL.
References
1. Bresalier R (2005) Barrett’s Metaplasia: defining the problem. Semin Oncol 32: 21–24.
2. Hansson LE, Sparen P, Nyren O (1993) Increasing incidence of both major histological types of esophageal carcinomas among men in Sweden. Int J Cancer 54: 402–407.
3. Francis AM, Sepesi B, Correa AM, Blum MA, Erasmus JJ, et al. (2013) The Influence of Histopathologic Tumor Viability on Long-term Survival and Recurrence Rates Following Neoadjuvant Therapy for Esophageal Adenocar-cinoma. Ann Surg 258: 500–507.
4. La Vecchia C, Bosetti C, Bertuccio P, Castro C, Pelucchi C, et al. (2013) Trends in alcohol consumption in Europe and their impact on major alcohol-related cancers. Eur J Cancer Prev.
5. Salehi M, Moradi-Lakeh M, Salehi MH, Nojomi M, Kolahdooz F (2013) Meat, fish, and esophageal cancer risk: a systematic review and dose-response meta-analysis. Nutr Rev 71: 257–267.
6. Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339: b2535. 7. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, et al. (2000) analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283: 2008–2012.
8. Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25: 603–605.
9. Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50: 1088–1101.
10. Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315: 629–634.
11. Lukic M, Segec A, Segeca I, Pinotic L, Pinotic K, et al. (2010) The role of the nutrition in the pathogenesis of gastroesophageal reflux disease, Barrett’s oesophagus and oesophageal adenocarcinoma. Coll Antropol 34: 905–909. 12. Anandasabapathy S, Jhamb J, Davila M, Wei C, Morris J, et al. (2007) Clinical
and endoscopic factors predict higher pathologic grades of Barrett dysplasia. Cancer 109: 668–674.
13. Bani-Hani KE, Bani-Hani BK, Martin IG (2005) Characteristics of patients with columnar-lined Barrett’s esophagus and risk factors for progression to esophageal adenocarcinoma. World J Gastroenterol 11: 6807–6814.
14. Coleman HG, Bhat S, Johnston BT, McManus D, Gavin AT, et al. (2012) Tobacco smoking increases the risk of high-grade dysplasia and cancer among patients with Barrett’s esophagus. Gastroenterology 142: 233–240.
15. Anderson LA, Watson RG, Murphy SJ, Johnston BT, Comber H, et al. (2007) Risk factors for Barrett’s oesophagus and oesophageal adenocarcinoma: results from the FINBAR study. World J Gastroenterol 13: 1585–1594.
16. de Jonge PJ, Steyerberg EW, Kuipers EJ, Honkoop P, Wolters LM, et al. (2006) Risk factors for the development of esophageal adenocarcinoma in Barrett’s esophagus. Am J Gastroenterol 101: 1421–1429.
17. Gatenby PA, Caygill CP, Ramus JR, Charlett A, Watson A (2008) Barrett’s columnar-lined oesophagus: demographic and lifestyle associations and adenocarcinoma risk. Dig Dis Sci 53: 1175–1185.
18. Achkar JP, Post AB, Achkar E, Carey WD (1995) Risk of extraesophageal malignancy in patients with adenocarcinoma arising in Barrett’s esophagus. Am J Gastroenterol 90: 39–43.
19. Sikkema M, Looman CW, Steyerberg EW, Kerkhof M, Kastelein F, et al. (2011) Predictors for neoplastic progression in patients with Barrett’s Esophagus: a prospective cohort study. Am J Gastroenterol 106: 1231–1238.
20. Jung KW, Talley NJ, Romero Y, Katzka DA, Schleck CD, et al. (2011) Epidemiology and natural history of intestinal metaplasia of the gastroesoph-ageal junction and Barrett’s esophagus: a population-based study. Am J Gastroenterol 106: 1447–1455; quiz 1456.
21. Casson AG, Zheng Z, Evans SC, Veugelers PJ, Porter GA, et al. (2005) Polymorphisms in DNA repair genes in the molecular pathogenesis of esophageal (Barrett) adenocarcinoma. Carcinogenesis 26: 1536–1541. 22. Gray MR, Donnelly RJ, Kingsnorth AN (1993) The role of smoking and alcohol
in metaplasia and cancer risk in Barrett’s columnar lined oesophagus. Gut 34: 727–731.
23. Olliver JR, Hardie LJ, Gong Y, Dexter S, Chalmers D, et al. (2005) Risk factors, DNA damage, and disease progression in Barrett’s esophagus. Cancer Epidemiol Biomarkers Prev 14: 620–625.
24. Hardikar S, Onstad L, Blount PL, Odze RD, Reid BJ, et al. (2013) The role of tobacco, alcohol, and obesity in neoplastic progression to esophageal adenocarcinoma: a prospective study of Barrett’s esophagus. PLoS One 8: e52192.
25. Li WQ, Park Y, Wu JW, Ren JS, Goldstein AM, et al. (2013) Index-based Dietary Patterns and Risk of Esophageal and Gastric Cancer in a Large Cohort Study. Clin Gastroenterol Hepatol 11: 1130–1136 e1132.
Alcohol and Progression of Barrett’s Esophagus