M Analysis of suicide rates and hospitalizations due to mental disorders.
11
0
0
Texto
(2) index Introduction 3 Data and Methods 3 Suicide Rates 4 Utilization of mental health services 7 References 9.
(3) “Evaluating and improving the access to mental health services of people affected by the economic crisis in Portugal based on a new understanding of the effects of the crisis on mental health of the population”. authors Paula Santana Adriana Loureiro Manuela Silva Graça Cardoso. NOVA medical school research team JM Caldas de Almeida (Coordinator) Graça Cardoso Ana Antunes Diana Frasquilho Manuela Silva Daniel Neto Benedetto Saraceno. partners Centre of Studies on Geography and Spatial Planning (CEGOT), University of Coimbra: Paula Santana and Adriana Loureiro Institute of Social Sciences, University of Lisbon: João Ferrão and Nádia Pereira Research Centre of Public Opinion (CESOP), Catholic University of Portugal: Jorge Cerol NOVA Information Management School, NOVA University of Lisbon: Jorge Mendes and Helena Baptista National School of Public Health, NOVA University of Lisbon: Julian Perelman Regional Health Administration of Lisbon and Tagus Valley (ARS-LVT): Luís Pisco Lisbon Hospital Psychiatric Centre (CHPL): José Salgado Magalhães Lemos Hospital: António Leuschner Faculty of Social Sciences, University of Oslo. international consultants Ron Kessler (Harvard Medical School, United States of America) Jordi Alonso and Gemma Vilagut (Institut Hospital del Mar d’Investigacions Mèdiques, Spain) Kristian Wahlbeck (Finnish Association for Mental Health, Finland) Arne Holte (Norwegian Institute of Public Health, Norway). acknowledgments Carla Abril Jorge Caixinhas Paula Broeiro Bruno Heleno Sofia Azeredo Teresa Santos Cláudia Costa Ricardo Almendra. funding This project was granted by the Public Health Initiatives Programme (PT06), financed by EEA Grants Financial Mechanism 2009-2014. mh crisis impact. www.crisisimpact.com.
(4) Introduction Mental health is a complex and multidimensional state, resulting from the interaction of philosophical, anthropological, psychological, biological and social factors (1–3). Vigo et al. (4) estimated that mental disorders are responsible for 32.4% of years lived with disability (YLDs) and 13.0% of disability-adjusted life-years (DALYs), considering the global burden of mental illness. Furthermore, suicide is one of the ten leading causes of death in the world, namely for those between 15 and 29 years of age (5). Research has shown an association between suicide and situations that usually accompany economic crisis, such as lower socio-economic status, unemployment, evictions, and indebtedness (6, 7). It is also well established that countries with a consolidated welfare state appear to be less exposed to suicide related to economic decline (6). Research on the use of psychiatric care in time of economic crises remains controversial, with some studies finding an increase in the use of the psychiatric services (8), and others documenting a lower demand for psychiatric care. The data suggest that the treatment gap among persons affected by psychiatric disorders increases in times of economic crisis, probably due to the lack of accessibility to services, the austerity measures, and the increased stigma towards people with mental illness (6). Portugal is one of the European countries with the highest prevalence rate of mental disorders (9). Suicide mortality increased between 1993-1999 and 2008-2012 in Portugal mainland (7). The results of the National Health Survey of 2014 indicated that 25.4% of the resident population, aged 15 years or older, have symptoms of depression. Between 2002 and 2012 the hospital admissions due to mental disorders increased in the metropolitan areas of Lisbon and Porto (8). It is estimated that the direct and indirect costs associated with mental disorders account for about 20% of all health costs of the public budget (1). The quantification of mental disorders and mortality are important for the academic community, the health professionals and the politicians, particularly in the evaluation of impacts, health outcomes and analysis of health determinants (10). The objective of this report is to analyse the suicide rates and the utilization of mental health services (hospitalizations due to mental disorders) between 2009 and 2014, in Portugal.. data and methods Mortality data by suicide and intentional self-harm (ICD-9: E950–E959) was collected in: i) The Portuguese National Statistics Institute, ii) Eurostat and iii) OECD.stat. Data was disaggregated by gender and age groups for the country and regions (NUT II and NUT III) for the years between 1960 and 2014. The analysis addresses the: i) mortality rate per 100,000 inhabitants, ii) standardized mortality rate per 100,000 inhabitants and iii) potential years of life lost per 100,000 inhabitants between 0 and 69 years of age. Hospitalizations due to mental disorders were gathered from the Diagnosis Related Groups (DRG) general database, made available by the Portuguese Health System Central Administration. Hospital admissions with main diagnosis of mental disorder were selected (ICD-9: 291, 303 – alcohol use-related mental disorders; 293 – transient mental disorders; 296, 311 – mood disorders; 295, 297, 298 – functional psychoses; 300 – anxiety, dissociative, somatoform disorders; 301 – personality disorders; 292, 304, 305 – drug use-related mental disorders; 306 – physiological malfunction arising from mental factors; 3071, 3075 – eating behaviour-related mental disorders; 3074 – non-organic sleep disorders; 3078 – psychogenic-related mental disorders; 308 – acute reaction to stress; 309 – adjustment reactions; 316 – specific factors associated with diseases classified elsewhere; E95 – suicide and intentionally self-inflicted injuries). The selection of these diagnostic categories was based on its importance and frequency (categories with higher number of admissions). The data was analysed by gender and age group between 2009 and 2014 for Portugal mainland and municipalities, using hospital admissions’ rate per 100,000 inhabitants. Population data was collected by gender and age group from 1960 to 2014 by the Portuguese National Statistics Institute.. mh crisis impact · report 2 · 3.
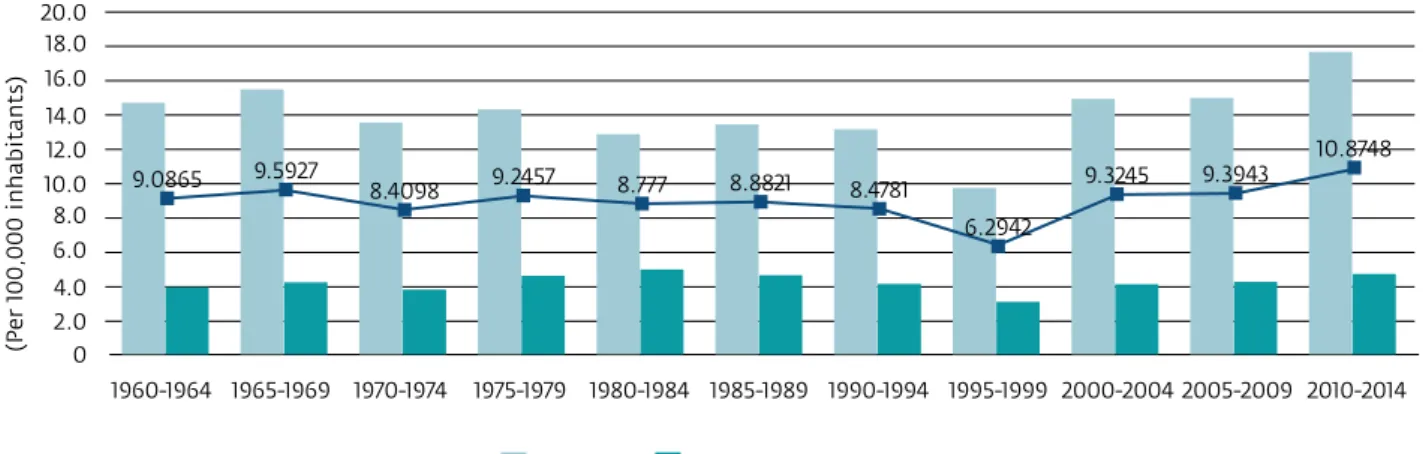
(5) suicide rates In the European context, the southern countries typically show lower standardized mortality rates by suicide, compared with the northern countries. However, considering the period 2011-2013, Portugal comprises regions (NUTS II) in the higher as well as lower class of suicide mortality rate (Fig.1). Alentejo region (21.4), Algarve region (14.4) and Açores islands (13.2) present values of deaths per 100,000 inhabitants by suicide above the European average (Fig.1).. Portugal in the European context Standardized Mortality Rate by suicide per 100,000 inhabitants, 2011-2013. 2.9. 6.4. 8.4. 10.7 12.3 14.0 17.6. 33.3. Classification Method: Quantile. EU28 11.7 per 100,00 inhab.. PORTUGAL. 9.8. Norte REGION. 5.8. Centro. 10.6. REGION. Lisboa METROPOLITAN. 9.5. AREA. Alentejo REGION. 21.4. Algarve REGION. 14.4. Açores REGION. 13.2. Madeira. 7.6. REGION. figure 1 standardized mortality rate by suicide per 100,000 inhabitants, 2011-2013 · source: data from eurostat (2016). In Portugal, between 1960-1964 and 1995-1994, the mortality by suicide decreased (1960-1964: 9.1 deaths per 100,000 inhabitants; 1995-1994: 6.3 deaths per 100,000 inhabitants) (Fig.2). Since 2000-2004 the suicide mortality has increased up to 10.9 deaths per 100,000 inhabitants (2010-2014), mainly between 2005-2009 and 2010-2014 (1.5 deaths per 100,000 inhabitants). Males have higher rates of death by suicide than females all over the period under analysis (Fig.2), with an average of 14.1 and 4.2 deaths per 100,000 inhabitants, respectively. Since 1995-1999, both genders show an increase of deaths per 100,000 inhabitants. The highest value of the period, 17.7 deaths per 100,000 inhabitants, was recorded in males in 2010-2014.. (Per 100,000 inhabitants). 20.0 18.0 16.0 14.0 12.0 10.0 8.0. 9.0865. 9.5927. 10.8748 8.4098. 9.2457. 8.777. 8.8821. 9.3245. 8.4781. 9.3943. 6.2942. 6.0 4.0 2.0 0 1960-1964 1965-1969. 1970-1974. 1975-1979. 1980-1984 1985-1989 1990-1994 1995-1999 2000-2004 2005-2009 2010-2014. 2008. 2015. Total. figure 2 deaths by suicide per 100,000 inhabitants between 1960 and 2014 by gender in portugal source: data from oecd stat (2017) and ine (2017). mh crisis impact · report 2 · 4.
(6) The potential years of life lost by suicide had a decreasing trend between 1960 and 1999 (Fig.3). Since 2000, the values are rising, presenting a value of 142 years lost per 100,000 inhabitants in the last period (2010-2014). Total. 200. Per 100,000 inhabitants between 0 and 69 years old. 180 160 140 120 100 80 60 40 20. 2010-2014. 2005-2009. 2000-2004. 1995-1999. 1990-1994. 1985-1989. 1980-1984. 1975-1979. 1970-1974. 1965-1969. 1960-1964. 0. figure 3 potential years of life lost by suicide between 1960 and 2014 in portugal (rate per 100,000 inhabitants 0-69 years old) source: data from oecd stat (2017). Considering the suicide mortality by age group (Fig.4), the older classes have higher mortality rates. The rates of the age group above 75 years of age increased between 1994 and 2014 (Fig.5). With the exception of the age group 15-29 years old, the suicide rate increased between 2001 and 2014. Nevertheless, the highest increase in suicide mortality during this period was registered in the age group of 45-59 years, mainly since 2006 (Fig.4 and 5). Between 2001 and 2014, the age group 15-29 years was the only one where the mortality rates decreased (Fig.5).. 45.0. (Per 100,000 inhabitants). 40.0 35.0 30.0 25.0 20.0 15.0 10.0 5.0. 1994. 2001. 2006. 2010. >85. 80 a 84. 75 a 79. 70 a 74. 65 a 69. 60 a 64. 55 a 59. 50 a 54. 45 a 49. 40 a 44. 35 a 39. 30 a 34. 25 a 29. 20 a 24. 15 a 19. 10 a 14. 6a9. <5. 0.0. 2014. figure 4 suicide mortality rate by age group between 1994 and 2014 in portugal source: data from eurostat (2016). mh crisis impact · report 2 · 5.
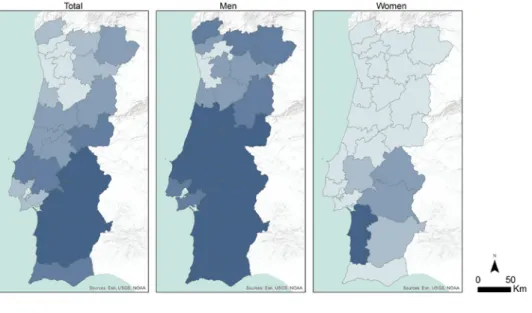
(7) 180. 140. 100. 60. 20 1994. 2001 15-29. 30-44. 2006 45-59. 2010 60-74. 2014 >=75. figure 5 suicide mortality rate by age group in portugal (1994 = 100) source: data from eurostat (2016). In the period 2009-2014, 6,133 suicides were registered in Portugal mainland (10.2 deaths per 100,000 inhabitants). Suicide mortality had a significantly diverse geographical distribution in Portugal mainland (Fig.6). The northern regions presented lower rates while the southern regions showed higher rates. The Alentejo region had the highest rates (37.8 suicides per 100,000 inhabitants in Alentejo Litoral sub-region). The lowest rates were observed in the northern coastal region, namely Ave sub-region with 4.7 suicides per 100,000 inhabitants. The two metropolitan areas of Portugal, Porto and Lisbon, presented lower suicide mortality (less than 9.7 suicide per 100,000 inhabitants). The pattern shown for total mortality differs when analysed by gender (Fig.6). The number of regions with high rates of mortality by suicide is more evident for men than for women. For men, the highest values were observed in the Centre and South of the country (more than 18.8 suicides per 100,000 inhabitants), with exception of the metropolitan area of Lisbon. For women, the Alentejo region presented the highest values of the country (namely Alentejo Litoral sub-region).. Crude death rate due to suicide (deaths/100.000 inhab.) <= 7.9. 8.0 - 9.7. 9.8 - 13.7. 13.8 - 18.7. >= 18.8. figure 6 mortality rate by suicide per 100,000 inhabitants between 2009 and 2014 in portugal by region (nut iii) source: data from ine (2017). mh crisis impact · report 2 · 6.
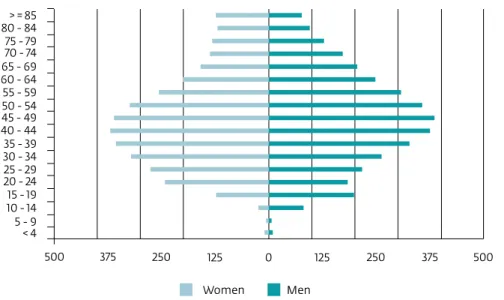
(8) utilization of mental health services In Portugal mainland, 134,335 episodes of hospitalization due to mental disorders were identified, in the period 2009-2014. The average hospitalization rate, in this period, was 224 per 100,000 inhabitants. The number of hospitalizations presented small variations all over the period, indicating a slight decrease (Fig.7). There were more hospitalizations in women than in men, corresponding to a rate of 227 and 221 hospital admissions per 100,000 inhabitants, respectively.. 25000. 20000. 15000. 10000. 5000. 0 2009. 2010. 2011. 2012. 2013. 2014. figure 7 hospital admissions due to mental disorders between 2009 and 2014 in portugal mainland source: data from health system central administration (general database of diagnoses related groups 2009-2014). For men and women, hospitalization rates tended to increase with age and the age groups of 40-44 and 45-49 years, respectively, showed the highest values (Fig.8), with 370 hospitalizations per 100,000 inhabitants for men and 386 for women. In the higher age groups, a progressive decrease in the rate of hospitalizations for both genders was observed (Fig.8). However, males presented a higher rate in the age group >=85 compared to the immediately lower age group (Fig.8). Males had higher rates than females in the ages < to 4 years old, between 20 and 39 years and above 75 years (Fig.8).. > = 85 80 - 84 75 - 79 70 - 74 65 - 69 60 - 64 55 - 59 50 - 54 45 - 49 40 - 44 35 - 39 30 - 34 25 - 29 20 - 24 15 - 19 10 - 14 5-9 <4 500. 375. 250. 125 Women. 0. 125. 250. 375. 500. Men. figure 8 hospital admissions by mental disorders by sex and age group in portugal mainland source: data from health system central administration (general database of diagnoses related groups 2009-2014) and ine (2017). mh crisis impact · report 2 · 7.
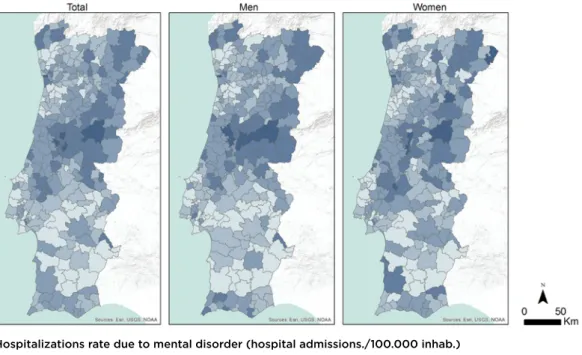
(9) The hospitalization rates due to mental disorders showed a geographical pattern marked by large disparities (Fig.9). In the period 2009-2014, the higher values were registered in some municipalities of the Centro region, that presented between 390 and 578 hospital admissions per 100,000 inhabitants, and of the Norte region (especially in Trás-os-Montes and Alto Minho sub-regions). Lower rates were observed in municipalities of the Alentejo region and in some municipalities of the Oeste, Cávado and Aveiro sub-regions, registering between 54 and 156 hospital admissions per 100,000 inhabitants. The geographical pattern was similar in men and women (Fig.9).. Hospitalizations rate due to mental disorder (hospital admissions./100.000 inhab.) 54.1 - 155.9. 156.0 - 211.9. 212.0 - 277.6. 277.7 - 390.2. 390.3 - 578.2. figure 9 hospitalization rates due to mental disorders between 2009 and 2014 by municipality in portugal mainland source: data from health system central administration (general database of diagnoses related groups 2009-2014) and ine (2017). mh crisis impact · report 2 · 8.
(10) References 1. Direção-Geral da Saúde. Portugal – Saúde Mental em números – 2013. Lisboa: Direção-Geral da Saúde; 2013. 2. Patel V, Lund C, Hatherill S, Plagerson S, Corrigall J, Funk M, et al. Mental disorders: equity and social determinants. In: Blas E, Kurup AS, editors. Equity, social determinants and public health programmes. Geneva: World Health Organization, 2010. 3. World Health Organization. Mental health: a state of well-being [Internet]. Geneva: World Health Organization; 2014 August [cited 2015 Oct 6]. Available from: http://www.who.int/features/factfiles/mental_health/en/ 4. Vigo D, Thornicroft G, Atun R. Estimating the true global burden of mental illness. Lancet Psychiatry. 2016; 3(2):171–178. 5. World Health Organization. Preventing Suicide: a global imperative. Geneva: World Health Organization; 2014. 6. Martin-Carrasco M, Evans-Lacko S, Dom G, Christodoulou NG, Samochowiec J, González-Fraile E, et al. EPA guidance on mental health and economic crises in Europe. Eur Arch Psychiatry Clin Neurosci. 2016; 266(2):89–124. 7. Santana P, Costa C, Cardoso G, Loureiro A, Ferrão J. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place. 2015; 35:85–94. 8. Cardoso G, Loureiro A, Mateus P, Silva M, Santana P, Caldas de Almeida J. Utilização de Serviços de Saúde Mental em Portugal em tempos de crise económica. In: Santana P, editor. Território e Saúde Mental em Tempos de Crise. Coimbra: Imprensa da Universidade de Coimbra; 2015. 9. Caldas-de-Almeida J, Xavier M. Estudo Epidemiológico Nacional de Saúde Mental - 1.o Relatório [National Mental Health Epidemiological Study - 1st Report]. Lisboa: Faculdade de Ciências Médicas, Universidade Nova de Lisboa; 2013. 10. Moriarty DG, Zack MM, Holt JB, Chapman DP, Safran MA. Geographic Patterns of Frequent Mental Distress. U.S. Adults, 1993-2001 and 2003-2006. American Journal of Preventive Medicine. 2009; 36(6):497–505.. mh crisis impact · report 2 · 9.
(11) www.crisisimpact.com.
(12)
Imagem

+2
Documentos relacionados
Existe uma colisão entre o interesse na realização da justiça consagrado no artigo 205º da CRP e o direito de reserva de vida privada, consagrado no n.º 1 do artigo 26º da CRP, e
Face à necessidade de implementar e avaliar a eficácia de intervenções psicológicas de apoio à tomada de decisão e adaptabilidade de carreira, esta investigação tem como
Devido à falta de informação concreta acerca do fator solar do vidro aplicado no vão envidraçado, optou-se por adotar o valor tabelado para este a partir da Tabela 12 do
Saccharomyces cerevisiae. Inositol phosphorylceramide, a novel substance and the chief member of a major group of yeast sphingolipids containing a single inositol phosphate. The
As formas intraeritrocíticas foram evidenciadas a partir do décimo dia da inoculação do sangue, não tendo sido observado alta parasitemia durante o experi- mento.. Entretanto,
Sources: Authorization for outpatient procedures (APAC); National Database on Health Units (CNES)... b) F11: Mental and behavioural disorders due to use of opioids. c) F12: Mental
Results: Teenagers value the indissociability between body and mind, recognize lack of attention to the psychological dimension in the health network, and point to mental
Objective: To estimate the 12-month prevalence of mental health services utilization (overall and by type of service sector), the adequacy of treatment provided, and
