REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brSCIENTIFIC
ARTICLE
A
comparison
of
two
different
doses
of
morphine
added
to
spinal
bupivacaine
for
inguinal
hernia
repair
夽
Basak
Ceyda
Meco
a,∗,
Onat
Bermede
a,
Cagil
Vural
a,
Atil
Cakmak
b,
Zekeriyya
Alanoglu
a,
Neslihan
Alkis
aaDepartmentofAnesthesiologyandIntensiveCare,AnkaraUniversityMedicalFaculty,Ankara,Turkey
bDepartmentofGeneralSurgery,AnkaraUniversityMedicalFaculty,Ankara,Turkey
Received11April2014;accepted6August2014 Availableonline21November2014
KEYWORDS
Spinalanesthesia; Morphine; Postoperative analgesia; Vomiting
Abstract
Backgroundandobjectives: Theaimofthisstudywastocomparetheeffectsoftwodifferent dosesofintrathecalmorphineonpostoperativeanalgesia,postoperativefirstmobilizationand urinationtimesandtheseverityofsideeffects.
Methods:After InstitutionalEthical Committeeapproval,48 ASA I-IIpatients were enrolled inthisrandomizeddouble-blindedstudy.Spinalanesthesiawasperformedwith0.1mg(Group I, n=22)or0.4mg (GroupII, n=26)ITM inadditionto7.5mg heavy bupivacaine.The first analgesic requirement, first mobilizationand voidingtimes, and postoperative sideeffects wererecorded.StatisticalanalyseswereperformedusingSPSS15.0andp<0.05wasconsidered asstatistically significant.The numeric data were analyzedby the t-testand presentedas mean±SD.Categoricaldatawereanalyzedwiththechi-squaretestandexpressedasnumber ofpatientsandpercentage.
Results:Demographicdataweresimilaramonggroups.Therewerenodifferencesrelatedto postoperativepain,firstanalgesicrequirements,andfirstmobilizationandfirstvoidingtimes. Theonlydifferencebetween twogroupswas thevomitingincidence.In GroupII23%(n=6) ofthepatients had vomitingduring thefirst postoperative 24h comparedto 0% inGroupI (p=0.025).
Conclusion:Foringuinalherniarepairs,thedoseof0.1mgofITMprovidescomparable post-operativeanalgesiawithadoseof0.4mg,withsignificantlylowervomitingincidencewhen combinedwithlowdoseheavybupivacaine.
©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
夽 Thisstudywaspresentedat44thNationalCongressofTurkishAnesthesiologyandReanimationAssociation,Antalya,Turkey.
∗Correspondingauthor.
E-mail:[email protected](B.C.Meco).
http://dx.doi.org/10.1016/j.bjane.2014.08.002
PALAVRAS-CHAVE
Raquianestesia; Morfina; Analgesia pós-operatória; Vômito
Comparac¸ãodeduasdosesdiferentesdemorfinaadicionadasàbupivacaína emraquianestesiaparaherniorrafiainguinal
Resumo
Justificativaeobjetivos: Oobjetivodesteestudofoicompararosefeitosdeduasdoses difer-entesdemorfinaintratecal(MIT)sobreaanalgesianopós-operatório,ostemposatéaprimeira mobilizac¸ãoemicc¸ãonopós-operatórioeagravidadedosefeitoscolaterais.
Métodos: Apósaaprovac¸ãodoComitêdeÉticaInstitucional,48pacientescomestadofísicoASA I-IIforamincluídosnesteestudorandômicoeduplo-cego.Araquianestesiafoirealizadacom 0,1mg(GrupoI,n=22)ou0,4mg(GrupoII,n=26)deMITadicionadosa7,5mgdebupivacaína hiperbárica.Ostemposatéaprimeiranecessidadedeanalgésico,mobilizac¸ãoemicc¸ãoeos efeitoscolateraisnopós-operatórioforamregistrados.Asanálisesestatísticasforamrealizadas usandooprogramaSPSS15.0ep<0,05foiconsideradoestatisticamentesignificativo.Osdados numéricos foramanalisadoscomoteste-te expressoscomo média±DP.Osdados categóri-cosforamanalisadoscomotestedoqui-quadradoeexpressos comonúmerodepacientese porcentagem.
Resultados: Osdadosdemográficosforamsemelhantesentreosgrupos.Nãohouvediferenc¸as emrelac¸ãoàdor,temposatéaprimeiranecessidadedeanalgésicos,primeiramobilizac¸ãoe primeiramicc¸ão.Aúnicadiferenc¸aentreosdoisgruposfoiaincidênciavômito.NoGrupoII, 23%(n=6)daspacientesapresentaramvômitoduranteasprimeiras24horasdepós-operatório, emcomparac¸ãocom0%noGrupoI(p=0,025).
Conclusão:Paraherniorrafiainguinal,adosede0,1mgdeMITforneceanalgesiacomparável àdosede0,4mg,comumaincidênciadevômitosignificativamentemenorquandocombinada comumadosebaixadebupivacaínahiperbárica.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Pain afteringuinal herniarepair is described asmoderate to severe and may beassociated with prolonged hospital stay. Furthermore,in the literature thereare some clues that suggest that inadequatepostoperative pain manage-mentmaybeariskfactorforpersistentchronicpainafter inguinalherniarepair.1Itiswellknownthatthecombination
ofintrathecal lowdoselocalanesthetics withopioids
pro-duceasynergisticeffectwithoutprolongingmotorblockand
therefore delaying discharge.2 Intrathecal morphine (ITM)
maybeagoodalternativefor postoperativepain
manage-ment withits long durationof spinalanalgesia. However,
thesideeffectssuchasnausea,vomiting,pruritusandlate
respiratorydepressionmayberestrainingitsapplication.In
severalstudies,itissuggestedthatlowerdosesofITM
pro-ducegoodqualityandlongdurationpostoperativeanalgesia
whilereducingtheincidenceofsideeffects.3---5
Theprimaryaimofthisstudywastocomparetheeffects
oftwodifferentdosesofITMincombinationwithlowdose
heavy bupivacaine on postoperative pain management in
inguinal hernia repair surgery. The secondary aim was to
compare thefirstmobilization andvoiding timesand side
effectsbetweenthetwogroups.
Methods
AfterInstitutionalEthicalCommitteeapprovalandpatients’
written informed consent, 48 ASA physical status I-II
patients, aged 18---65 years, undergoing elective
unilat-eralopeninguinalherniarepairsurgerywereprospectively
enrolled in this randomized double-blinded study.
Exclu-sioncriteriaincludedcontraindicationstospinalanesthesia,
central or peripheral neuropathies, severe respiratory or
cardiacdiseases,chronicanalgesic useandhistoryof
sub-stanceabuseorallergytolocalanesthetics.
The study was recorded towww.clinicaltrials.gov with
theregistrationnumberofNCT02001948.
PatientswererandomlyassignedintotwoGroupsIand
II, according to a sealed envelope method. In Group I
(n=22), patients received 0.1mg morphine with 7.5mg
heavy bupivacaine intrathecally and in Group II (n=26),
patientsreceived0.4mgmorphinewith7.5mgheavy
bupi-vacaineintrathecally.
After standard monitoring (electrocardiography, heart
rate, pulseoximetry and noninvasive arterial blood
pres-sure)an18-gaugeintravenous(iv)cannulawasinsertedat
theforearmoppositetothesurgicalsideandroutineiv
pre-medication(midazolam0.03mg/kg)wasgiven.
Spinal anesthesia was performed using the midline
approach. Patients were placed in the lateral
decubi-tus position with the operational side down. After local
infiltrationwith2%lidocaine,a25gaugeQuinckespinal
nee-dle(Spinocan®, B BraunMelsungen Ag,D-Melsungen) was
insertedattheL2-3orL3-4interspace.Onaspirationofclear
cerebrospinalfluid, 7.5mgof 0.5%heavybupivacaine was
administered in combination with the assigned morphine
dose. The drugs were combined in saline, and a total of
patients’ group assignments performed spinal anesthesia.
Patientswereheldinthesamepositionfor15minandthen
theywereplacedinthesupinepositionforthesurgery.
Afterspinalinjection,ablindedobserverfollowedupthe
evolutionofspinalblock.Sensoryblockwasassessedusing
lossof pinpricksensation while motorblock wasassessed
usinga4-pointmodifiedBromagescore(0=nomotorblock,
1=hipblocked;2=hipandkneeblocked;3=hip,kneeand
ankleblocked).Theonsetofsurgicalanesthesiawasdefined
astheloss of pinpricksensation at ≥T10 witha Bromage
score≥2.TheinabilitytoreachasensoryblockatT10within
30min afterspinal injectionwasconsidered asblock
fail-ure.Hypotension(decreaseinsystolicbloodpressure≥30%
ofbaseline)wastreatedwith200mLofnormalsalineover
10minandifthiswasnotsufficient,5mgofephedrinewas
giveniv.Bradycardia(decreaseinheartratebelow45bpm)
wastreatedwith0.5mgivatropine.6
Thehemodynamicparametersduringtheprocedurewere
alsorecorded.Duringthepostoperativeperiodinthe
hospi-talpainwasassessedwithavisualanalogscale(VAS)score
of0---10andaVASscoreofhigherthan3weretreatedwith
rescueanalgesicIVtramadol25mg,repeatedasnecessary.
Thereafter,whenpatientswerereadyfordischargefromthe
hospital,theyweregivenaprescriptionofNSAIDandwere
asked tonote the use of analgesic drugs at home if
nec-essary.DuringthePACUstay,atwardandforthefirst24h
postoperativesideeffects(nausea,vomiting,pruritus,and
dizziness)werefollowedupandrecorded.Also,first
mobi-lizationand voidingtimes and firstanalgesic requirement
wererecorded.Thosewhocomplainedofurinaryretention
werecatheterizedwithasimplerubbercatheterandwere
recordedasurinaryretention.
Atelephonecallfollow-up wasperformed 3daysafter
surgerytoevaluatethepostoperativepainandtheincidence
ofsideeffectsincludingdizziness,nauseaandvomiting.
Statistics
Data were statistically analyzed using SPSS version 15.0
(SPSSInc.,Chicago,IL).Apilotstudywasconductedbefore
the initiation of the study and mean, and standard
devi-ationof firstanalgesic requirementtimewasfound tobe
5±2h with an ˛-error of 0.05 and a ˇ-error of 0.2. The
mainoutcomeofthestudywasdeterminedasanincrease
inthefirstanalgesicrequirementtimeby25%,andasample
sizeof44patientsintwogroups(GroupI,n=22;andGroup
II,n=22)wascalculated.The numericdatawereanalyzed
bythet-testandpresentedasmean±SD.Categoricaldata
were analyzed with the chi-squaretest and expressed as
numberofpatientsandpercentage.Ap-valueoflessthan
0.05wasconsideredtoindicatestatisticalsignificance.
Table1 Demographicdata.
Group I(n=22) II(n=26)
Age(year) 51±15 52±14 Gender(M/F) 20/0 24/2 Weight(kg) 76.9±12 74.8±6.8 Height(cm) 171.9±5.6 168.5±5.7
Allvaluesareshownasmean±SD.
Results
Demographicdataweresimilaramonggroups(Table1).
Sur-gical anesthesiawasachievedfor allthe patients,andno
spinalfailurewasobserved.Therewerenostatistically
sig-nificantdifferencesinhemodynamicparametersandpulse
oximetrymeasurements.Theclinicallyrelevanthypotension
or bradycardia requiring interventionwas notobserved in
bothgroups.
Table2showsthefirstmobilization,firstvoiding,urinary
retention incidence and first analgesic requirement times
for patientswhohadpain.Nosignificantdifferenceswere
observedbetweengroupsrelatedtotheseparameters.The
useofrescueanalgesic inthehospital(tramadol25mgiv)
wassimilaramonggroups.Nopatientsneededrescue
anal-gesic during their stay at PACU and only two patients in
GroupIandthreepatientsinGroupIIneededrescue
anal-gesicduringthefirstpostoperative24h.Nopatientusedany
analgesicathome.
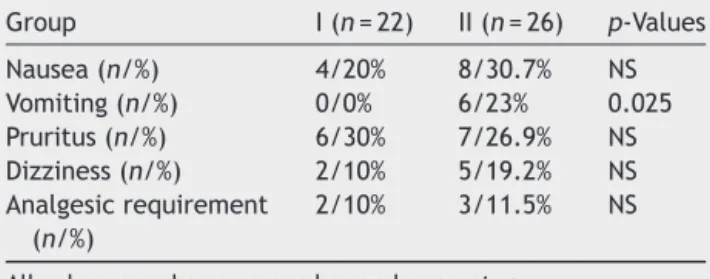
Morphine related postoperative side effects were also
assessed.Theonlydifferencebetweentwogroupswasthe
vomiting incidence.In GroupII 23% (n=6)of the patients
had an episode of vomiting during the first postoperative
24hcomparedto0%inGroupI(p=0.025)(Table3).
None ofthe patients in both groups developedclinical
evidenceofsevererespiratorydepressionatanytime.
Discussion
Resultsofthisrandomizedprospectivedouble-blindedstudy
demonstrated that 0.1mg ITM had similar anesthetic and
postoperative analgesic effects when comparedto 0.4mg
ofITM.However,theincidenceofvomitingwashigherwith
0.4mgofmorphine.
Thechoiceofanesthetictechniqueforopeninguinal
her-niarepairdependsonseveralfactorsincludingthepatient
and surgeon choices, postoperative pain management,
recoverytimeandpostoperativemorbidity.7However,spinal
anesthesia is mostly preferred and widely used for open
Table2 Postoperativeanestheticrecoveryandanalgesia.
Group I(n=22) II(n=26) p-Value
Firstmobilizationtime(h) 5.5±2 5.9±3 NS
Firsturinationtime(h) 7±2 7.6±4.6 NS
Urinaryretention(%) 15% 11.5% NS
Firstanalgesiatime(h) 5(4---12) 4(0.3---24) NS
h,hours.
Table3 Postoperativesideeffectsduringthefirst postop-erative24hrelatedtointrathecalmorphineuse.
Group I(n=22) II(n=26) p-Values
Nausea(n/%) 4/20% 8/30.7% NS Vomiting(n/%) 0/0% 6/23% 0.025 Pruritus(n/%) 6/30% 7/26.9% NS Dizziness(n/%) 2/10% 5/19.2% NS Analgesicrequirement
(n/%)
2/10% 3/11.5% NS
Allvaluesareshownasnumberandpercentage.
inguinalherniarepair,providingafastonsetandeffective sensoryandmotorblockade.8
Postoperativepainmanagement
Pain after inguinal hernia repair is defined as moderate
to severe and can be associated with prolonged hospital
stay.Inaddition,insufficienttreatmentofearly
postopera-tivepainmaycausepersistentchronicpain.1Earlierstudies
haveshownthattheadditionofintrathecalopioidstolocal
anestheticsinspinalanesthesiamayimprovepostoperative
painmanagementofambulatoryinguinalherniarepair.2,9,10
In their study Girgin et al. compared the combination of
intrathecal 25g fentanyl and low dose levobupivacaine
withahigherdoseoflevobupivacainealone.Theearly
post-operativepainscorewaslowerinthegroupwithintrathecal
fentanyl.Inthisstudy,theadditionoffentanylhasshortened
thereadinessfordischargetimeofthepatientsand
amelio-ratedthepostoperativepainmanagement.Inanotherstudy
Guptaetal.reportedthatthepostoperativepainincidence
atPACUwas20---25%,andtheearlypostoperativepain
inci-dence(first24h)was50%withintrathecalfentanyl25gand
bupivacainecombination.10 Similarly,in ourstudythetwo
differentdoses ofITM providedsatisfactory postoperative
analgesia.Additionally,inourstudyonly10.0---11.5%ofthe
patientsneededarescueanalgesicduringthefirst24h,and
noneofthemneededanyanalgesicatPACU.Thelonglasting
effectofITMmaybeagoodalternativeforthemanagement
ofpostoperativepainininguinalherniarepair.
Inguinalherniarepairisasurgicalprocedurewith
mod-eratetohighdegree postoperativepain.It shouldbewell
managedtopreventthedevelopmentofchronic
postopera-tivepain.Therefore,theuseofalongeractingintrathecal
opioidmightbeagoodalternative.Inourstudy,theaddition
oftwodifferentdosesofITMdidnotchangethe
postopera-tivepainincidenceor analgesicrequirement.Therefore,a
dose of 0.1mgof morphine canbea goodalternative for
postoperativepainmanagementforherniarepairs.
Sideeffects
Thesideeffectsofintrathecalopioidsarediscussedin
sev-eralstudies.Intheirstudy,Girginetal.compareddifferent
dosesofITMforcesareandeliveryandreportedthathigher
dosesofITMresultedinahigherincidenceofpruritus(15.5%
vs.39.5%).11InanotherstudyGuptaetal.useda
combina-tionofintrathecal fentanylwithbupivacaineandreported
an incidence of pruritus of 50---60%.10 In our study, the
incidenceofprurituswassimilarwiththepreviousstudies.
However,therewasnodifferencebetweenthetwodifferent
dosesofITM.Moreover,inourstudythefrequencyofnausea
and vomiting were higher than the previously reported
studiesintheliterature(20---30%and0---23%,respectively).
Also,theincidenceofvomitingwassignificantlyhigherwith
higherdoseofITM(0.4mgvs.0.1mg).Thissideeffectmay
limittheuseofhigherdosesofITMininguinalherniarepair.
Postoperativerecovery
Inourstudy,allpatientswereabletostandandwalk
with-outhelpafterapproximately340minandvoidafter440min.
Theseresultsarelongerthanthefindingofstudieswith
fen-tanyl.This delayinpostoperativerecoverymayretardthe
homedischargeofpatients.Thisdelayindischargemaybea
seriousproblemandmaydecreasethepatientsatisfaction.
A limitation of this study is that intraoperative fluid
management and the urinary retention assessed with a
bladderscanwerenotfollowedup.Also,thepatients’
satis-factionanddischargetimesareimportantdata,whichwere
notassessedinthisstudy.Thesedatamaybecrucialforthe
selectionofanesthesiatechniqueforinguinalherniarepair
procedures.
In conclusion, the addition of 0.1mg ITM to 7.5mg of
heavybupivacaineforspinalanesthesiaproduces
compara-blepostoperativeanalgesiatothatproducedwith0.4mgof
ITM,butwithalowerincidenceofnausea.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.JoshiGP,RawalN,KehletH,onbehalfofthePROSPECT col-laboration.Evidence-basedmanagementofpostoperativepain inadultsundergoingopen inguinalherniasurgery.Br JSurg. 2012;99:168---85.
2.Girgin NK, Gurbet A, Turker G, et al. The combination of low-dose levobupivacaine and fentanyl for spinal anaesthe-sia in ambulatory inguinal herniorrhaphy. J Int Med Res. 2008;36:1287---92.
3.MilnerAR,BogodDG,HarwoodRJ.Intrathecaladministrationof morphineforelectivecaesareansection.Acomparisonbetween 0.1mgand0.2mg.Anaesthesia.1996;51:871---3.
4.Terajima K, Onodera H, Kobayashi M, et al. Efficacy of intrathecalmorphineforanalgesiafollowingelectivecesarean section:comparisonwithpreviousdelivery.JNipponMedSch. 2003;70:327---33.
5.PalmerCM,EmersonS,VolgoropolousD,etal.Dose-response relationshipofintrathecalmorphineforpostcesarean analge-sia.Anesthesiology.1999;90:437---44.
6.CasatiA,FanelliG,DanelliG,etal.Spinalanesthesiawith lido-caineorpreservativefree2chlorprocaineforoutpatientknee arthroscopy:aprospective,randomized,double-blind compari-son.AnesthAnalg.2007;104:959---64.
7.KehletH,DahlJB.Spinalanaesthesiaforinguinalherniarepair? ActaAnaesthesiolScand.2003;47:1---2.
9.Salinas FV, Liu SS. Spinal anaesthesia: local anaesthet-ics and adjuncts in the ambulatory setting. Clin Anesth. 2001;16:195---210.
10.Gupta A, AxelssonK,Thörn SE,etal. Lowdose bupivacaine plusfentanylforspinalanesthesiaduringambulatoryinguinal herniorrhaphy:acomparisonbetween6mgand7.5mgof bupi-vacaine.ActaAnaesthesiolScand.2003;47:13---9.