RESUMEN
Objeivo: Construir un modelo teórico que
conigure la vivencia del apoyo de la red social por las personas en cuidado domici
-liario. Método: Estudio de abordaje cuali
-taiva, con la uilización del método Teoría Fundamentada en los Datos. La recopila
-ción y el análisis concomitante de los datos hizo viable la interpretación del signiicado
del fenómeno La vivencia del apoyo de la red social por las personas implicadas en el cuidado domiciliario. Resultados: Se desta
-có la postura pasiva de la población en la construcción de su bienestar. Reconocien
-do que debe exisir una responsabilidad comparida entre las partes implicadas, población y Estado. Conclusión: Se sugie
-re que los enfermeros sean esimulados a ampliar el cuidado que realizan en el do
-micilio para atender las demandas de los cuidadores; y que sean elaborados nuevos estudios con disintas poblaciones, con el in de validar o complementar el modelo teórico propuesto.
DESCRIPTORES
Personas impossibilitadas
Servicios de Atención de Salud a Domicilio Apoyo social
Cuidadores
Cuidados de enfermería en el hogar
RESUMO
Objeivo: Construir um modelo teórico que
conigure a vivência do apoio da rede social pelas pessoas envolvidas no cuidado domi
-ciliário. Método: Pesquisa de abordagem qualitaiva, com a uilização do método Te
-oria Fundamentada nos Dados. A coleta e análise concomitante dos dados viabilizou a interpretação do signiicado do fenôme -no A vivência do apoio da rede social pelas pessoas envolvidas no cuidado domicili-ário. Resultados: Destacou-se a postura passiva da população na construção de seu bem-estar. Reconhece-se que deve exisir uma responsabilização comparilhada en
-tre as partes envolvidas, população e Esta
-do. Conclusão: Sugere-se que os enfermei
-ros sejam esimulados a ampliar o cuidado que realizam no domicílio para atender demandas dos cuidadores; e que novos estudos sejam elaborados com populações diferentes, a im de validar ou complemen
-tar o modelo teórico proposto.
DESCRITORES
Pacientes domiciliares
Serviços de Cuidados Domiciliares Apoio social
Cuidadores
Enfermagem domiciliária
ABSTRACT
Objecive: To build a theoreical model to conigure the network social support ex
-perience of people involved in home care. Method: A quanitaive approach rese
-arch, uilizing the Grounded Theory me
-thod. The simultaneous data collecion and analysis allowed the interpretaion of the phenomenon meaning The network social support of people involved in home care. Results: The populaion passive posture in
building their well-being was highlighted. The need of a shared responsibility betwe
-en the involved parts, populaion and State is recognized. Conclusion: It is suggested for nurses to be simulated to amplify home care to atend the demands of care
-givers; and to elaborate new studies with diferent populaions, to validate or com
-plement the proposed theoreical model.
DESCRIPTORS
Homebound persons Home Care Services Social support Caregivers
Home health nursing
The network social support experience
of people involved in home care
*Ingrid Meireles Gomes1, Maria Ribeiro Lacerda2, Nen Nalú Alves das Mercês3 A VIVÊNCIA DO APOIO DA REDE SOCIAL PELAS PESSOAS ENVOLVIDAS NO CUIDADO DOMICILIÁRIO
LA VIVENCIA DEL APOYO DE LA RED SOCIAL POR LAS PERSONAS EN CUIDADO DOMICILIARIO
* Extracted from the dissertation “A vivência do apoio da rede social pelas pessoas envolvidas no cuidado domiciliar”, Nursing Graduate Program, Universidade Federal do Paraná, 2012. 1 Doctoral Student of the Nursing Graduate Program, Universidade Federal do Paraná, Curitiba, PR, Brazil. [email protected] 2 Doctor in Nursing. Professor of the Nursing Graduate Program, Universidade Federal do Paraná, Curitiba, PR, Brazil 3 Doctor in Nursing. Professor of the
DOI: 10.1590/S0080-623420140000300014
O
r
i
g
i
n
a
l
a
r
ti
c
INTRODUCTION
The health work has been developed to overcome the curaive care model, and for this reason, it has been di
-rected to the integrality of care and primary health care. Home care is a favorable pracice for this change when it ariculates prevenive, promoion, curaive, assistance and educaion acions(1). It is worthy to consider the home care
as a viable opion of health care considering the increase in longevity and chronic illness exising in the society and the inancial restricions in health, as it propiiate the fre
-quency reducion and the costs of hospitalizaions(2).
Home care involve diferent categories, as care, hospi
-talizaion and home visit, each one with its own characteris
-ics(3). It requires knowledge of its peculiariies from health
professionals: home context, individual, family, caregiver, interdisciplinary team and network social support.
This way, the comprehension of involved people in health care (HC) is perceived as important for its concre
-ion either by its individual or collecive role. In this con
-text, it is believed to exist a real social network inluence in HC, considering it as a group of individuals interacing and allowing to build and rebuild an individual idenity constantly ime and space(4).
HC represents a situaion in which the social network is highlighted, being formal or informal, primary or sec
-ondary. With the arrival of an ill family member, life is of those involved in the context is modiied, causing physi
-cal, emoional, organizaional, personal and collecive adaptaions(5). Those adaptaions can be relieved or even
resolved when there is efecive network social support. The HC can be recognized as a potenial for greater ap
-proximaion of professionals with the community(5), allow
-ing beter use of available social resources and the com
-munity resolute potenial. Thus, the knowledge of social networks with a collaboraive role for health of individuals is believed to enable the health professional to promote a more comprehensive care, based in the needs and every
-day realiies, propiiaing autonomy to subjects(6-8).
The ideniied importance of the network social support for HC and the perceived lack of studies considering a joint vision of diferent involved people in HC about networks(9),
this invesigaion was proposed to search the answer for the quesion what is the meaning of the network social support experience of people involved in home care?. The objecive is to build a theoreical model that conigures the network social support experience of people involved in home care.
METHOD
This is a qualitaive approach research that uilized the Grounded Theory (GT), a method to elaborate theories and theoreical models based in data from social reality, systemaically collected and analyzed .
The study context was the territory limits of a Health Basic Unit with the Family Health Strategy teams (USESF) of a metropolitan region from Curiiba. The data collec
-ion was from January to June of 2012, through semi-structured interviews, scheduled with the paricipants in a convenient place and date during a home visit done with the USESF team. The study was presented to paricipants and it was the moment where they would give their con
-sent to paricipate voluntarily.
In agreement with the method, the subjects were listed from the necessity coming from the data; at the end, they composed three sample groups (SG). The irst was composed by four paients in home care (following the criteria of being over 6 months in HC, to have a familiar responsible caregiver, to be an adult or elderly and to be able to communicate ver
-bally), totalizing ive interviews, two were with the irst sub
-ject. The second SG was composed by three members of pri
-mary social networks, selected for being cited by the subjects or paients from the irst group as relevant in the HC, and the three interviews were conducted. At last, the third HC was composed by three members of secondary social networks, indicated by the irst and second SGs, ending in three more interviews. Thus, the involved subjects in HC in this study, in accordance with their own data, included paients, family members, friends/neighbors and health professionals.
The data analysis followed the glasserian model of codi
-icaion, composed by two phases – the substanive and the theoreical; being the irst subdivided in two moments – the open and selecive codiicaion. In the last phase was the theoreical codiicaion, the theoreical code opted in the present study was denominated interacive family(11).
This code proposes interacions within the data built by mutual efect relaionships, reciprocity, mutual trajectory, interdependency, efects interacion and covariance(11). Mu
-tual efect is when there is non-standardized relaionships within the variables; reciprocity deals with interacions with reciprocal exchanges; mutual trajectory happens when the alteraions happen concomitantly; efects interacion points the existence of a sequence relaionship; and the co
-variance presents a linear relaionship within the variables. This study followed the resoluion 196/96; it was ap
-proved by the Ethics in Research Commitee, under the registraion CEP/SD 1198.123.11.08. Ater verbally accept
-ing to voluntarily paricipate in the research, the subjects signed the Free and Informed Consent Term. The coni
-deniality and possibility to withdraw without jusiicaion was guaranteed, as well as the absence of material, physi
-cal or emoional onus.
RESULTS
provides support in home care; and Perceiving changes coming from health care. From the exising interacions between those categories, through the theoreical code denominated as interacive family, a central category was built, described as the following statement: Experiencing the social network support from people involved in home care that presents the studied phenomenon, ideniied as The experience of the social network support from people involved in the home care.
In the category Idenifying the social support in home care the composiion of perceived support sources in the experience of HC was apprehended, including primary so
-cial networks, mainly composed by the family, neighbors and friends; the secondary social networks were specially ideniied as USESF, but also by physiotherapy clinic linked to the Uniied Health System (SUS) and the Church; and the use of electronic resources as source of social sup
-port and as a tool to obtain sup-port. In this category the exising support sources, underuilized or known by the community also emerge, as those coming from the Social Acion Secretary and the Health Secretary. Sill, the per
-ceived reasons for the diiculty in obtaining social assis
-tance, speciied by jusiicaions for support restricion by primary networks and by experienced problems in the search for formal support.
Characterizing the social networks that provide sup-port in home care, is the category in which the charac
-terization of such networks by social support functions is comprehended, identified as material and services help, social company, emotional support, cognitive guidance and advices and access to new contacts. Oth
-er network aspects that integrate the size and multi
-dimensionality of social networks are the frequency of contacts, the connection and compromise within mem
-bers, at last, the main necessity and the perceived ab
-sence of social support.
The role of people as part of the social network is presented in the category Understanding it as part of the social network that provides support in home care
con-taining the meanings of being a paricipant in the HC so
-cial network, as the feelings and moivaions from those subjects in this context of care; the paient posiion of needing support in his condiion of being cared as social support of third paries or as searching for an available support; and the importance of the social network sup
-port for the caregivers, for the paients and family and also to the own network.
The category Perceiving changes coming from health care exposes the peculiariies coming with the need for care or for being cared at home; changes for the paient, as the emoional and operaional changes and in the so
-cial relaionships; and also changes for those who act as the source of social support for the paient, involving per
-sonal modiicaions and variaions in the support given over ime in the HC.
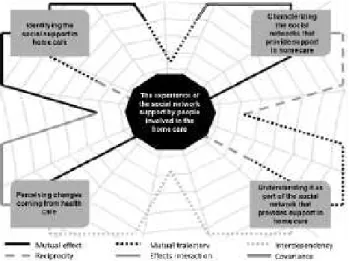
Those four categories describing the phenomenon have a straight relaionship with the central category, as the relaionships are not formed by themselves; they are connected parts from a central concept described as Expe-riencing the social network support from people involved in home care, which can be perceived in the theoreical model proposal explaining the phenomenon The experi-ence of the social network support by people involved in the home care (Figure 1).
Figure 1- Theoretical model of the phenomenon The experience of the social network support of people involved in the home care.
The given amplitude of interacions within the data should be considered, not being possible to draw them in a theoreical model by uni and bidirecional lines exclu
-sively. Thus, behind the model drawing a net was inserted, symbolizing the exising muliple interacions in the stud
-ied phenomenon. Besides that, the existence of diferent types of lines connecing the categories can be observed, demonstraing the possibility of more than one type of interacion within the same data, simultaneously or not.
As perceived in the theoreical model, the proposed cat
-egories Idenifying the social support in home care and Char-acterizing the social networks that provide support in home care establish three diferent types of relaionships; of mu
-tual trajectory, mu-tual efect and covariance. Simultaneously, recognizing the composiion of the social network of the sub
-ject in HC, the descripion of this network characterisics are disinguished, exposing the mutual trajectory relaionship.
The consequence of the alteraions in the network characterisics generated in the ideniicaion of its mem
-bers indicates the existence of mutual efect. This situa
-ion can be exempliied as follows: when there is an in
-crease of commitment within the members of a speciic social network with the person needing HC, an alteraion can happen in the type of network that this member will represent, a neighbor can become a friend or even start to develop new supporing funcions. The same can hap
-pen with members of any ideniied networks. As it is per
More were the people who appeared after, that ended up getting closer to me and becoming my friends (Interview 3).
Waw, the neighbor woman now is a mother; she does ev-erything (Interview 2).
The opposite can also happen, that is, members of a network that had afecive connecions before can restrain the contact or even be excluded of the social relaionship circle, decreasing the subject’ network. This way, the exis
-tence of a covariance relaionship is perceived within the two categories menioned above, as the alteraion in one of them interfere linearly on the other.
The following speeches presents this situaion, the irst when talking about the longer ime in the partner’ trips, who is a truck driver, and started to come less home ater the HC was iniiated; and the second by the distance of the brother.
Now he travelled on the irst of on December 31th and hasn’t
come until now (more than two months after) (Interview 1).
There is one (brother) who came twice to see me and hasn’t anymore. If he calls, it is for one of my sisters and does not ask about me (Interview 2).
The relaionship between the categories Characterizing the social networks that provide support in home care and Understanding it as part of the social network that provides support in home care is a mutual trajectory. In the measure, which the network characterisics are known, the role for those involved in the HC can be understood.
Another relaionship linking those categories is the reciprocity. The subject percepion about his role in the social network is modiied by the network characterisics, and this new percepion can alter diverse types of char
-acterisics. For example, the existence of higher support availability with access funcion to new contacts or cogni
-ive and advice guidance, in a way to transmit informaion about the available social networks, including by the elec
-tronic resources, the higher search for available support or even the importance ampliicaion of having a wide and afecive social network as consequence. Consequently, this can increase the connecion size, or the frequency of the social network contacts of the subject in HC.
(…) Then the health agent goes there, sees the patient’s condition and comes. (…) when the agent is really active,
the patients are beneited, because we move with the
team to make something to help (Interview 11).
In the popular pharmacy has, because we buy there. I hear here on the radio them talking about this government program (Interview 5).
Within the categories Understanding it as part of the social network that provides support in home care and Per-ceiving changes coming from health care there is an inter
-dependence relaionship. Because only when one is aware of your role as a social network in HC is when he perceives
which changes this fact will result for diferent people in
-volved and for the HC itself. Similarly, to comprehend one
-self in this process, necessarily one has to perceive how his change his life, the social relaionships and the support.
The neighbors say: - Neighbor lady, I haven’t seen you lately. Then I say: - But I’m dealing there, the woman is in bed, but I did not abandon you (Interview 7).
Idenifying the social support in home care and Perceiv-ing changes comPerceiv-ing from health care are categories that establish sequenial relaionship, that is, efects interacion; as the paient perceive changes in his life as consequence of the HC, with the dependence increase, consequently the lack of support from the social network is perceived. An
-other sequence is established when there is percepion by the social network members of the paient’ autonomy and, consequently, less need of support from this network.
What she used to do now I do, almost everything in the be-ginning. When it is only us at home, is hard. (Interview 8).
Now I stopped a little because she is better and her kids gained more practice in the job. So now I’ve stopped a little. But when she was bad, I saw that she was really not good, I ran, left everything here (Interview 7).
Those categories also have a mutual efect relaion
-ship, as the alteraion of one category by the other will not always be unidirecional. There are situaions where there are no standards within them. Although the inlu
-ence of one category on the other is perceived, it is not possible to measure how this inluence will happen. For example, in a HC situaion the paient can perceive to receive more support from the closer people. Thus, the creaion of expectaions that the same will happen with other social networks in which this individual is part of can happen, but the no intensiicaion of pre-exising situa
-ions ends up generaing unhappiness or disappointment, leading the paient to have negaive feelings.
They (sisters) help inancially, in the tasks, in everything.
(…) He (brother) used to come always, for me to cook
for them. As my son says: - The uncle is selish, mom; if you are ine he will come back. Then I’ll say: - Now it’s not
needed, right?! (Interview 2).
The mutual trajectory and reciprocity are the relaion
-ships developed by the categories Idenifying the social support in home care and Understanding it as part of the social network that provides support in home care. The ideniicaion of networks that are part of a social network of a subject in HC allows the comprehension of oneself as part of it; at the same ime that recognizing one’s role inside this network allows a criical vision, therefore per
-ceiving reciprocity.
The mutual trajectory is related with the search for new available sources. As the search for new contacts for social support broadens the exising sources of assistance that are underused, starts to be uilized. This sill happens when perceiving that the comprehension of the support importance for the involved people in the NC is in accor
-dance to the recognized support.
The social networks are certainly important in all aspects. I think there are people surviving through this. (…) They (other social networks) are work collaborators, right? If someone does a service and collaborate with what I do, ends up helping me too (Interview 10).
There are sill, the relaionship between the catego
-ries Characterizing the social networks that provide
sup-port in home care and Perceiving changes coming from health care with a mutual efect. This relaionship can be perceived by the alteraions that the network and support characterisics provoke in the paient as well as in other people involved in the HC. Alternaively, in opposiion, by the way those changes from the HC interfere in the sup
-port characterisic.
From the type of funcion from the received support, the paient will perceive higher or lower signiicant altera
-ions in relaion to be in HC; the same happens with the variaion on the size of the network and its funcionality. In counterpart, the changes passed by the subjects in HC alter those characterisics in an unpredictable manner. People who perceive their social relaionships as reduced can develop strict social networks, but intense and high density, causing posiive emoional changes and facility to adapt. However, this may not happen and this size reduc
-ion in the network can result in a support with litle types of funcion and consequently negaive changes.
I even started to think one day that I was depressed, with fear. Because I think this is not possible! I wanted to talk to someone, right? Never, it is hard to have. It is that I have been always active (Interview 5).
Other people involved in HC are also afected by the described mutual efect relaionship. One chance in the of
-fered support over HC ime alters diferent characterisics, as the size, the connecion or simply the type of support funcion. On the other hand, the characterisics of social as
-sistance cause personal changes in caregivers, for example, reducing or amplifying their personal social network.
DISCUSSION
Regarding the category Idenifying the social support in home care the naional literature corroborate(12-14) the pres
-ent study indings, that the social network composiion is mainly formed by family members and neighbors in the pri
-mary networks and by USESF professionals in the second
-ary networks. Studies that invesigated(12-14) diferent con
-texts and health care subjects pointed to the importance of
the social networks for health; this way, it is believed those subjects as well as the paients should be part of the acion plan of health professionals. It is necessary to think about it, in special when dealing with HC, an environment where those subjects, more than an opion in care, should be seen as subjects, who also need assistance by being modiied by the reality that they help to change.
In opposiion, internaional studies points to friends as the most signiicant social network, even more than family member, propiiaing improve in the social isolaion and de
-crease of the possibility to develop depression, even when the family role is highlighted in the social network(15-16).
The recogniion of the USESF as social network that supports subjects in HC allow the possibility to create bounds of trust between users and professionals, besides the establishment of favorable relaionships within the so
-cial network support and the families, contribuing to the subjects’ health(17).
Diferent authors(14;17-19) approach the use of electron -ic resources (radio, television and telephone) as source of support, but as an incipient way. Those resources are weighted as valid as social support for subjects if uilized in an adequate way(17); and this use can represent signii
-cant assistance, especially for the paient’s families(18).
Regarding the types of support funcion menioned in the present study in the category Characterizing the so-cial networks that provide support in home care, there is no consensus in the literature about the main types. One possible reason can be the subject’s variability in each study about social networks that provides support. How
-ever, this might not be the only reason, considering that in diferent studies(12,20) with elderly as subjects, it was also possible to note the disparity in the types of funcion of the cited support.
Thus, cultural, economic, geographical, educaional, within other factors can inluence this characterizaion(15).
However, in the present study, the analysis of those fac
-tors was not conducted; a reason to suggest new similar studies, but with populaions with diferent characteris
-ics, to verify the presented phenomenon and recify or complement the proposed theoreical model.
The moivaions to be social support in HC presented in the category Understanding it as part of the social net-work that provides support in home care are frequently discussed in the literature(20-25). The obligaion can be per
-ceived as a moivaion, people give support because of an obedience condiion to norms and social values(20-25).There
are also posiive moivaions, as love, afecion, devoion or acknowledgement(21-23). Independently of the moivaion,
especially for that person who assume more caring load at home, the generaion of overload is recognized(21,26).
to note an ambiguity of involved feelings; pleasure and sat
-isfacion happen simultaneously to impotence, impaience and insecurity(25,27). In this study, this ambiguity is perceived beyond the members of the informal social networks, af
-licing specially members of secondary networks, as the health professionals. This happen because those subjects, besides acing in the HC, they sufer interference by the car
-ing they provide.
The small search for social support demonstrated a pas
-sivity of the populaion in the search for ways to promote wellbeing. The paricipaion of people in the search for available social resources is believed to inluence directly the reach of supports(28). Similarly to this study, authors(29)
observed the populaion deicit in searching for assistance, idenifying within the reasons for it, the illness sigma, prob
-lems with alcoholism and tobacco, but ended recognizing the diiculty to understand the reason for the small search.
About the category Perceiving changes coming from health care it is important to consider the changes from the need of HC afects the enire social network. Howev
-er, the primary inluence is highlighted more speciically, the responsible caregiver(21,23,30). This inluence is related to diverse factors and reaches varied dimensions of the caregiver life, which gives exposure to physical, emo
-ional, personal and social risks(21,23,26-27). Thus, the care -giver can have the sensaion of lacking autonomy upon his life and prioriize the care for the other in detriment
of himself(21,23,30).
In this context, it becomes imperious that nurses di
-rect their sight to caregivers, understanding them as sub
-jects that specially in HC, need support(26). Those profes
-sionals need to recognize the home complexity as caring environment and the inluences brought to the lives of all involved people.
Social networks are believed to be able to minimize the diiculies of those caregivers and even stop the phys
-ical and mental illness of being support in HC(26), besides
the representaion of those as a factor of inluence for the saisfacion of needs from the home cared paients(16).
Thus, nurses are expected to recognize the inluence and possibiliies that social networks support can ofer to per
-form HC and for the reach and maintenance of paients health and from other involved people.
CONCLUSION
The presented indings reinforce the understanding of social networks as potenial for HC, as atending the neces
-sity of support for subjects involved in this context. With the theoreical model construcion, it was possible to recognize how the relaionships happen within the social network that gives support to HC and consequently, it is expected to give instruments for nurses to act in this care environment, using the social network support as facilitator.
More research is suggested in the same topic, with similar methodology, in regions with diverse populaion characterisics, to complement or recify the proposed theoreical model. It is also considered that with the pro
-posal it would be viable to verify the direct inluence of factors that characterize the populaion, as geographical, economic, educaional, within others, in the experience of social network support of those involved in HC.
The relecion about how the ciizen conscience is be
-ing built is needed. In most diverse situaions, people seek too litle the opions of available support in the society, presening a passive posture in front of found barriers. It is perceived that populaions wait for soluion of their health and social problems to be solved by formal bodies, without commiing to solve them.
The responsibility for the populaion needs should be shared. The government and formal bodies cannot be re
-lieved from their responsibility of exising social needs. However, each one, individually and collecively should have a ciizen conscience and adequate aitudes to reach their rights.
At last, it is important to note especially in HC, the caregiver should be understood and atended as sub
-ject of nursing acions, considering this environment presening more than one work object for nurses, due to alteraions coming from HC, which afect diferent involved people in the home context. This way, it is rec
-ommended for this professional to be simulated to am
-plify the care given at home, trying to understand the nuances of this environment, guiding the ones involved to acivate their social network, to paricipate in sup
-port groups and to ind material resources and social company to support them.
REFERENCES
1. Kerber NPC, Kirchhof ALC, Cezar-Vaz MR. Considerações sobre a atenção domiciliária e suas aproximações com o mundo do trabalho na saúde. Cad Saúde Pública [Internet]. 2008 [citado
2011 jun. 03];24(3):485-93. Disponível em: htp://www.sci
-elo.br/pdf/csp/v24n3/02.pdf
2. Cook RJ, Berg K, Lee KA, Poss JW, Hirdes JP, Stolee P. Reha
-bilitaion in home care is associated with funcional im
3. Lacerda MR, Oliniski SR, Giacomizzi CM, Venturi KK, Truppel TC.
The kinds of home health care and the pracice of health profes
-sionals: exploratory and descripive research. Online Braz J Nurs [Internet]. 2007 [cited 2011 July 14];6(0). Available from: htp:// www.objnursing.uf.br/index.php/nursing/aricle/view/557
4. Sluzki CE. Personal social networks and health: conceptual and clinical implicaions of their reciprocal impact. Fam Syst Health. 2010;28(1):1-18.
5. Sawyer MG, Barnes J, Frost L, Jefs D, Bowering K, Lynch J.
Nurse percepions of family home-visiing programmes in Aus
-tralia and England. J Paediatr Child Health. 2013;49(5):369-74.
6. Hayakawa LY, Marcon SS, Higarashi IH, Waidman MA. Rede social de apoio à família de crianças internadas em uma unidade de terapia intensiva pediátrica. Rev Bras Enferm. 2010;63(3):440-5.
7. Bitencourt ZZLC, Françozo MFC, Monteiro CR, Francisco DD.
Surdez, redes sociais e proteção social. Ciênc Saúde Coleiva [In
-ternet]. 2011 [citado 2012 jan. 23];16 Supl. 1:769-76. Disponível em: htp://www.redalyc.org/pdf/630/63018473007.pdf
8. Brusamarello T, Guimarães AN. Labronici LM, Mazza VA, Maf
-tum MA. Redes sociais de apoio de pessoas com transtornos mentais e familiares. Texto Contexto Enferm. 2011;20(1):33-40.
9. Gomes IM, Kalinowski LC, Lacerda MR, Ferreira RM. The dom
-iciliary health care and its state of art: a bibliographic study. Online Braz J Nurs [Internet]. 2008 [cited 2012 Sept 10];7(3). Available from: htp://www.objnursing.uf.br/index.php/ nursing/aricle/view/j.1676-4285.2008.1781
10. Dantas CC. Grounded theory - conceptual and operaional
aspects: a method possible to be applied in nursing re -search. Rev Laino Am Enferm [Internet]. 2009 [cited 2012 Jan 15];17(4):573-9. Available from: htp://www.scielo.br/ pdf/rlae/v17n4/21.pdf
11. Glaser BG. Advances in the methodology of Grounded Theory: theoreical sensiivity. California: The Sociology Press; 1978.
12. Mesquita RB, Morano MTAP, Landim FLP, Collares PMC, Pin
-to JMS. Rede de apoio social e saúde de idosos pneumopa
-tas crônicos. Ciênc Saúde Coleiva. 2012; 17(5):1125-33.
13. Muramoto MT, Mângia EF. A sustentabilidade da vida co
-idiana: um estudo das redes sociais de usuários de serviço de saúde mental no município de Santo André (SP, Brasil). Ciênc Saúde Coleiva [Internet]. 2011 [citado 2011 nov. 23];16(4):2165-77. Disponível em: htp://www.scielo.br/ pdf/csc/v16n4/v16n4a16.pdf
14. Pedro ICS, Galvão CM, Rocha SMM, Nascimento LC. Social support and families of children with cancer: an integraive review. Rev Laino Am Enferm [Internet]. 2008 [cited 2012 Nov 20];16(3):477:83. Available from: htp://www.scielo.br/ pdf/rlae/v16n3/pt_23.pdf
15. Wilby F. Depression and social networks in community dwelling elders: a descripive study. J Gerontol Soc Work. 2011;54(3):246-59.
16. Canga A, Vivar CG, Naval C. Dependencia y familia cuidadora: relexiones para un abordaje familiar. Anales Sis San Navarra [Internet]. 2011 [citado 2013 dic. 14]; 34(3). Disponible en: htp://scielo.isciii.es/pdf/asisna/v34n3/revision3.pdf
17. Alexandre AMC, Labronici LM, Matum MA et al. Map of
the family social support network for the promoion of child development. Rev Esc Enferm USP [Internet]. 2012 [cited 2012 Nov 20];46(2):272-9. Available from: htp:// www.scielo.br/scielo.php?script=sci_artext&pid=S0080-62342012000200003&lng=pt&nrm=iso&tlng=en
18. Nascimento JD, Lacerda MR, Kalinowski LC, Favero L. Sup
-porive social networks to homecare: descripive explorato
-ry research. Online Braz J Nurs [Internet]. 2011 [cited 2012 June 24];10(3). Available from: htp://www.objnursing.uf. br/index.php/nursing/aricle/view/3431
19. Domingues MARC, Santos CF, Quintans JR.Doença de Al
-zheimer: o peril dos cuidadores que uilizam o serviço de
apoio telefônico da ABRAz – Associação Brasileira de Al
-zheimer. Mundo Saúde. 2009;33(2):161-9.
20. Nardi EFR, Oliveira MLF. Conhecendo o apoio social ao cui
-dador familiar do idoso dependente. Rev Gaúcha Enferm. 2008;29(1):47-53.
21. Bapista BO, Beuter M, Girardon-Perlini NMO, Brondani CM,
Budó MLD, Santos NO. A sobrecarga do familiar cuidador no
âmbito domiciliar: uma revisão integraiva da literatura. Rev Gaúcha Enferm. 2012;33(1):147-56.
22. Canesqui AM, Barsaglini RA. Apoio social e saúde: pontos de vista das ciências sociais e humanas. Ciênc Saúde Coleiva. 2012;17(5):1103-14.
23. Marques AKMC, Landim FLP, Collares PM, Mesquita RB. Apoio social na experiência do familiar cuidador. Ciênc
Saúde Coleiva [Internet]. 2011 [citado 2012 mar. 11];16 Su
-pl. 1:945-55. Disponível em: htp://www.scielo.br/pdf/csc/ v16s1/a26v16s1.pdf
24. Bicalho CS, Lacerda MR, Catafesta F. Releindo sobre quem é o cuidador familiar. Cogitare Enferm. 2008;13(1):118-23.
25. Machado ALG, Jorge MSB, Freitas CHA. A vivência do cuidador
familiar de víima de acidente vascular encefálico: uma aborda
-gem interacionista. Rev Bras Enferm. 2008;62(2):246-51.
26. Miranda-Casillo C, Woods B, Galboda K, Oomman S, Olojug
-ba C, Orrell M. Unmet needs, quality of life and support net
27. Gomes WD, Resck ZMR. A percepção dos cuidadores domi
-ciliares no cuidado a clientes com sequelas neurológicas. Rev Enferm UERJ. 2009;17(4):496-501.
28. Paula ES, Nascimento LC, Rocha SMM. The inluence of social support on strengthening families of children with chronic renal failure. Rev Laino Am Enferm. 2008;16(4):692-9.
29. Santana JJRA, Zanin CR, Maniglia JV. Pacientes com câncer:
enfrentamento, rede social e apoio social. Paidéia [Inter
-net]. 2008 [citado 2011 dez. 10];18(40):371-84. Disponível em: htp://www.scielo.br/pdf/paideia/v18n40/13.pdf