w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Indirect
and
direct
costs
of
treating
patients
with
ankylosing
spondylitis
in
the
Brazilian
public
health
system
Valderilio
Feijó
Azevedo
a,∗,
Chayanne
N.
Rossetto
a,
Pedro
G.
Lorencetti
a,
Mariana
Y.
Tramontin
a,
Bruna
Fornazari
a,
Denizar
V.
Araújo
baHospitaldeClínicas,UniversidadeFederaldoParaná,Paraná,PR,Brazil bUniversidadedoEstadodoRiodeJaneiro,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2March2015 Accepted1June2015
Availableonline9September2015
Keywords:
Ankylosingspondylitis Indirectcosts
Pharmacoeconomy Qualityoflife Directcosts
a
b
s
t
r
a
c
t
Introduction:Patientswithankylosingspondylitisrequireateamapproachfrommultiple professionals,varioustreatmentmodalitiesforcontinuousperiodsoftime,andcanleadto thelossoflabourcapacityinayoungpopulation.So,itisnecessarytomeasureits socio-economicimpact.
Objectives: TodescribetheuseofpublicresourcestotreatASinatertiaryhospitalafter theuseofbiologicalmedicationswasapprovedfortreatingspondyloarthritisintheHealth PublicSystem,establishingapproximatevaluesforthedirectandindirectcostsoftreating thisillnessinBrazil.
Materialandmethods:93patientsselectedfromtheambulatoryspondyloarthritisclinicat theHospitaldeClínicasoftheFederalUniversityofParanábetweenSeptember2011and September2012hadtheirdirectcostsindirecttreatmentcostsestimation.
Results:70patients(75.28%)weremaleand23(24.72%)female.Themeanagewas43.95 years.Thediseasedurationwascalculatedbasedontheageofdiagnosisandthemeanwas 8.92years(standarddeviation:7.32);63.44%wereusinganti-tumournecroticfactordrugs. ComparingmaleandfemalepatientsthemeanBathAnkylosingSpondylitisDiseaseActivity Indexwas4.64and5.49whilethemeanBathAnkylosingSpondylitisFunctionalIndexwas 5.03and6.35respectively.
Conclusions: TheBrazilianpublichealthsystem’sspendingrelatedtoankylosingspondylitis hasincreasedinrecentyears.Animportantpartofthesecostsisduetotheintroduction ofnew,moreexpensivehealthtechnologies,asinthecaseofnuclearmagneticresonance and,mainly,theincorporationofanti-tumournecroticfactortherapyintothetherapeutic arsenal.ThemeanannualdirectandindirectcosttotheBrazilianpublichealthsystemto treatapatientwithankylosingspondylitis,accordingtoourfindings,isUS$23,183.56.
©2015ElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](V.F.Azevedo).
http://dx.doi.org/10.1016/j.rbre.2015.08.009
Custos
diretos
e
indiretos
do
tratamento
de
pacientes
com
espondilite
anquilosante
pelo
sistema
público
de
saúde
brasileiro
Palavras-chave:
Espondiliteanquilosante Custosindiretos Farmacoeconomia Qualidadedevida Custosdiretos
r
e
s
u
m
o
Introduc¸ão: Ospacientescomespondilite anquilosante(EA)exigem umaabordagem de equipecomváriosprofissionaiseváriasmodalidadesdetratamento,continuamente;além disso,adoenc¸apodelevaràperdadacapacidadedetrabalhoemumapopulac¸ãojovem,de modoqueénecessáriomediroseuimpactosocioeconômico.
Objetivos: DescreverousoderecursospúblicosparaotratamentodaEAemum hospi-talterciárioapósousodosfármacosbiológicostersidoaprovadoparaotratamentodas espondiloartritespeloSistemaPúblicodeSaúdeeestabelecervaloresaproximadosparaos custosdiretoseindiretosdotratamentodessadoenc¸anoBrasil.
Materialemétodos: Foramestimadosos custosdetratamento diretoseindiretosde 93 pacientescomEAdoambulatóriodeespondiloartritedoHospitaldeClínicasda Univer-sidadeFederaldoParaná,entresetembrode2011esetembro2012.
Resultados: Dospacientes,70(75,28%)eramdosexomasculinoe23(24,72%)dofeminino. Aidademédiafoide43,95anos.Adurac¸ãodadoenc¸afoicalculadacombasenaidade dodiagnóstico ea média foide 8,92anos(desviopadrão:7,32); 63,44%dos indivíduos usavamfármacosanti-TNF.Nacomparac¸ãodospacientesdossexosmasculinoefeminino, amédianoBathAnkylosingSpondylitisDiseaseActivityIndex(BASDAI)foide4,64e5,49, enquantoamédianoBathAnkylosingSpondylitisFunctionalIndex(BASFI)foide5,03e 6,35,respectivamente.
Conclusões: Osgastosdosistemapúblicodesaúdebrasileirorelacionadoscomaespondilite anquilosanteaumentaramnosúltimosanos.Umaparteimportantedessescustosdeve-seà introduc¸ãodasnovastecnologiasdesaúde,maisdispendiosas,comonocasoda ressonân-cianuclearmagnéticae,principalmente,daincorporac¸ãodaterapiaanti-TNFaoarsenal terapêutico.Ocustomédioanualdiretoeindiretodosistemapúblicodesaúdebrasileiro paratratardeumpacientecomespondiliteanquilosante,deacordocomosresultadosdeste estudo,édeUS$23.183,56.
©2015ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
AnkylosingSpondylitis (AS) is achronic inflammatory dis-ease,autoimmuneinorigin,whichgenerallyaffectsthespinal columnandcanevolveintostiffnessand progressive func-tionallimitationoftheaxialskeleton.1,2 Itismorefrequent
inyoung adultsaged between20 and 40 years.There is a greater prevalenceinmales (3:1),Caucasians,and HLA-B27 positiveindividuals.2,3TheHLA-B27antigenisstrongly
corre-latedwiththeappearanceofthedisease,andapositivetest forthismarkerisfoundin80–98%ofcases.4Itisaprogressive
diseasewhich,overtime,causesthepatient’squalityoflifeto deteriorate.Inadvancedstages,itmayleadtocompletespinal ankyloses,knownas“bamboospine”,andextremereduction ofmobility. Evenintheinitialstageofthe disease, inflam-matorylumbarpainmay causesignificantmorbidityinthe patient,complicatingdailyactivitiesandevenrequiring tem-poraryleavefromworkduties.Manypatientssufferfromthe progressivelossoftheircapacitytowork,whichmayresult inearlyretirement,generatingadditionalcoststothepublic welfaresystem.5,6
Theintroductionofanti-TNF(anti-tumournecroticfactor) pharmaceuticalstotreatASin2006guaranteedpatients bet-terqualityoflifethankstotheefficacyofthesemedications
inlessening symptomsand theprogressionofthe disease. Despite the efficacy and safety thesemedications provide, their highcostsgreatly impacthealthbudgets incountries wherethesedrugswereimplemented.Variousstudiesofcost effectivenesshavebeen conductedinanattempt toassess differencesbetweentheanti-TNFtherapies.7–9
Because this incapacitating disease requires a team approach from multiple professionals, various treatment modalitiesforcontinuousperiodsoftime,andcanleadtothe lossoflabourcapacityinayoungpopulation,itisnecessary tomeasureitssocio-economicimpact.Internationalstudies ofthedirectandindirectannualcostsofAShaveindicateda valueofapproximately10thousandeurosperpatient.10,11
ThelastBrazilianstudyintendedtodemonstratethedirect andindirectcostsinASpatientswaspublishedin2010,and demonstrated significant differencesbetween thedomestic andinternationalsituations.Thedomesticcostwasestimated atU$4597perpatient/year. Thisvaluewaslowin compari-sonwiththefindingsofinternationalstudiesthathadbeen published up to that point.12 However, the Brazilian study
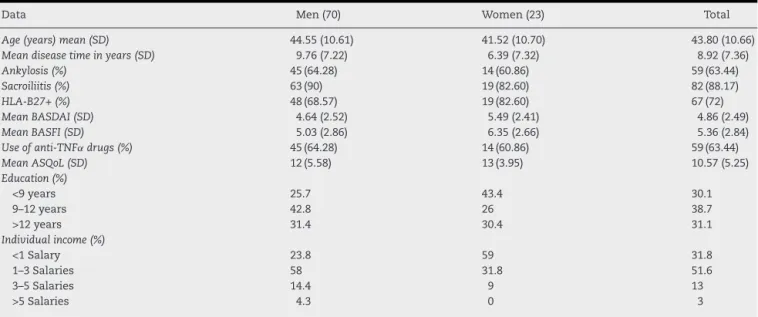
Table1–ClinicalanddemographicdataofankylosingspondylitispatientstreatedatHC-UFPRSpondyloarthritis outpatientclinic.
Data Men(70) Women(23) Total
Age(years)mean(SD) 44.55(10.61) 41.52(10.70) 43.80(10.66)
Meandiseasetimeinyears(SD) 9.76(7.22) 6.39(7.32) 8.92(7.36)
Ankylosis(%) 45(64.28) 14(60.86) 59(63.44)
Sacroiliitis(%) 63(90) 19(82.60) 82(88.17)
HLA-B27+(%) 48(68.57) 19(82.60) 67(72)
MeanBASDAI(SD) 4.64(2.52) 5.49(2.41) 4.86(2.49)
MeanBASFI(SD) 5.03(2.86) 6.35(2.66) 5.36(2.84)
Useofanti-TNF˛drugs(%) 45(64.28) 14(60.86) 59(63.44)
MeanASQoL(SD) 12(5.58) 13(3.95) 10.57(5.25)
Education(%)
<9years 25.7 43.4 30.1
9–12years 42.8 26 38.7
>12years 31.4 30.4 31.1
Individualincome(%)
<1Salary 23.8 59 31.8
1–3Salaries 58 31.8 51.6
3–5Salaries 14.4 9 13
>5Salaries 4.3 0 3
ASQoL,AnkylosingSpondylitisQualityofLife;BASDAI,BathAnkylosingSpondylitisDiseaseActivityIndex;BASFI,BathAnkylosingSpondylitis FunctionalIndex;TNF,tumournecroticfactor.
Datawithnormaldistributionwereexpressedinmeanandstandarddeviation.Nonnormaldatawereexpressedinmedianand25–75percentile. TheminimumwageusedasreferenceisU$306.40.
Theobjectiveofthisstudywastodescribetheuseof pub-licresourcestotreatASinatertiary hospitalaftertheuse ofbiologicalmedicationswasapprovedfortreating spondy-loarthritisintheSUS,establishingapproximatevaluesforthe directandindirectcostsoftreatingthisillnessinBrazil.
Materials
and
methods
Wedescribeatransversalstudy ofasampleof93patients selectedfrom the outpatientspondyloarthritisclinicatthe UniversidadeFederaldoParaná(UFPR)–HospitaldeClínicas between September 2011 and September 2012. The inclu-sion criteria were being diagnosed with AS for at least a yearaccordingtomodifiedNewYorkcriteria,fulfiltheASAS 2009classificationforaxialspondyloarthritisandbeingolder than18yearsold.Patientswhopresentmalignancies,acute infectionsandotherrheumatologicandautoimmunediseases wereexcludedfromthestudy.
Beforeanoutpatientclinicvisiteach patientanswered a questionnaireaboutits demographicaland economical sta-tus,clinicalstory,pensionsandwelfaresreceived,considering theprevioustwelvemonths.DiseaseindexessuchasBASFI (BathAnkylosingSpondylitisFunctionalIndex),BASDAI(Bath AnkylosingSpondylitis Disease Activity Index), and ASQoL (AnkylosingSpondylitisQualityofLife)werealsoassessedat thismoment.
Thedirectcosts aredefinedasthe sumofallresources spenttodirectlytreatandmanageASpatients.13TheNational
HealthSystemprovidesmostofthecarewithoutanypayment includingmedicalcare,medications,laboratoryandradiologic examsand physicaltherapy.Equipmentandhome adapta-tionswerealsoclassifiedindirectcostsregarditsimportance inthe management of the disease despite being aprivate spend. Indirect Costs are all the resources spent by the
Brazilian government with welfares, disease pensions and retirementdueincapacityresultedfromAS.
We performeda descriptive analysis ofthe direct costs obtainedaccordingtotheBrazilianhealthsystemcosttable whichappliedtotheperiodof2012.14Thecostfindingswere
convertedfrombrazilianrealintodollarusingtheexchange ratefromthelastdayofSeptember2012(U$1=R$2,03),when thestudyperiodended.
Theindirect costs estimation tookinconsideration sick leavesand retirementsresultedfrom thedisease.Thetotal amountwascalculatedbasedonthenationalminimumwage forthatperiod,whichwasU$306.40.15
Thepatientswereinformedabouttheobjectiveofthestudy andsignedtheFreeandInformedConsentAgreement.The studywasapprovedbytheEthicsCommitteeofthe Universi-dadeFederaldoParaná–HospitaldeClínicas.
Results
Ofthe93patientswithankylosingspondylitis70(75.28%)were maleand23(24.72%)female.Themeanagewas43.95years, andincludedindividualsbetween21and69yearsofage.The duration ofthe diseasewascalculated basedontheageof diagnosis,andthemeanwas8.92years(standarddeviation: 7.32);63.44%wereusinganti-TNFdrugs.Comparingmaleand female patientsthe mean BASDAI was4.64 and 5.49while themeanBASFIwas5.03and6.35respectively;83.4%ofthe samplereceivedlessthanthreesalariesasindividualincome. OtherdemographicandclinicaldataareexposedinTable1.
Table2–Complementaryexaminationsconductedinthelast12monthsonpatientswithASwhoweremonitoredbythe HC-UFPRspondyloarthritisoutpatientclinic.
Complementaryexaminations N◦ofexamsconducted Unitcost Totalcost Costperpatient
Hemogram 372 3.36 1253.43 13.477
ESR(sedimentationrate) 372 1.34 500.27 5.37
CRP(C-reactiveprotein) 372 4.55 1695.07 18.22
Bilirubins 197 0.99 195.05 2.09
Livertransaminases 197 1.98 390.11 4.19
Tuberculin(PPD) 27 0 0 0
anti-HBs 27 9.13 246.72 2.65
HbsAg(HepatitisBSurfaceAntigen) 27 9.13 246.72 2.65
anti-HCV 27 9.13 246.72 2.65
X-rays 165 4.92 812.80 8.73
ComputerTomography 24 49.80 1195.27 12.85
Magneticresonanceimageofsacroiliacjoint 16 132.38 2118.22 22.77
Shoulderultrasound 4 11.92 47.68 0.51
HLA-B27test 34 – – –
Echocardiogram 1 19.67 19.67 0.21
Analysisofsynovialfluid 1 1.82 1.82 0.01
Total 1863 8969.62 96.44
Averagepricecalculatedfromthemostcommonlyrequestedimages.Valuesareshownindollar.
representing97.96%(1.887,131,43),NSAIDs0.58% (11.249,84) andDMARDs1.09%(21.131,2)ofthisamount.
ThedirectcostsarereportedinTable4andindirectcosts inTable5.
ThetotalcostforthesamplewasU$2,156,070.83/year, rep-resentingU$23,183.56perpatient/year.
Discussion
InBrazil,thereisascarcityofstudiesthatevaluatetheimpact ofthecostsoftreatingpatientswithankylosingspondylitis. Furthermore,althoughthiswasnotourobjective,wenoted thatstudiesofcosteffectivenessrelatedtoASarealmost non-existentcomparedtotheproportionofstudiesinEuropean countriesandtheUnitedStates.Thisisthefirststudy con-ductedinBrazilthat assessesthecostsofASafterthe full
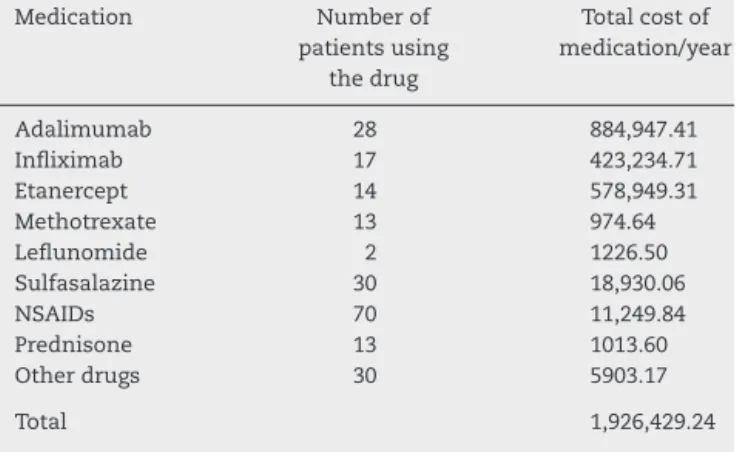
Table3–Alldrugsprescribedfortreatmentof ankylosingspondylitisduringanoneyearperiod.
Medication Numberof
patientsusing thedrug
Totalcostof medication/year
Adalimumab 28 884,947.41
Infliximab 17 423,234.71
Etanercept 14 578,949.31
Methotrexate 13 974.64
Leflunomide 2 1226.50
Sulfasalazine 30 18,930.06
NSAIDs 70 11,249.84
Prednisone 13 1013.60
Otherdrugs 30 5903.17
Total 1,926,429.24
Valuesareshownindollar.OtherdrugsincludeOmeprazole,Folic Acid,Codeine,CyclobenzaprineandAmitriptyline.
introduction ofbiologicalmedications bythe SUSfor treat-mentofthisaffliction.
Thestudysamplewasmainlycomposedofmenandthe mean age was 44 years. The mean disease duration was approximately 9 years,differing from the results foundby Torres,whichwas16years.12
ThemeanBASFIfunctionalscorewas5.36,andtheBASDAI was 4.86,similarvaluestothose foundbyTorres (BASFI=5 andBASDAI=4),suggestingasimilarsamplewithrelationto functionalstateanddiseaseactivity.Asforqualityoflife,the meanASQoLscorewas10.57,alsohigherthanthefindingsby Torres(ASQoL=8);nevertheless,asthisindexhasnotyetbeen validatedinaBrazilianPortugueseversion,comparisonsmay becontroversial.
The total number of complementary examinations
requested for the group was 1863. The most commonly requested tests were laboratory evaluations, principally hemograms, ESR, CRP, liver enzymepanels and bilirubins, usedtoassessdiseaseactivityandtomonitorthesideeffects ofimmunosuppressanttherapy.Thecostsspentonimaging accounted for 46.8% of total examination costs, compared withthe56%obtainedbyTorres.Althoughthisauthordidnot conductmoreexpensivetestssuchascomputertomography (CT) and nuclear magnetic resonance (NMR), that study describedgreaterutilisationofexaminationssuchasX-rays andbonedensityscans.12
Only16NMRswere ordered,despitethegrowing impor-tance of this test to the early diagnosis of the disease, principallyfordiagnosingaxialspondyloarthritisaccordingto ASASclassificationwhennoalterationsare evidentin con-ventional radiography imagingofthespinalcolumnor the sacroiliacjoint.16However,thepatientsselectedhadhadtheir
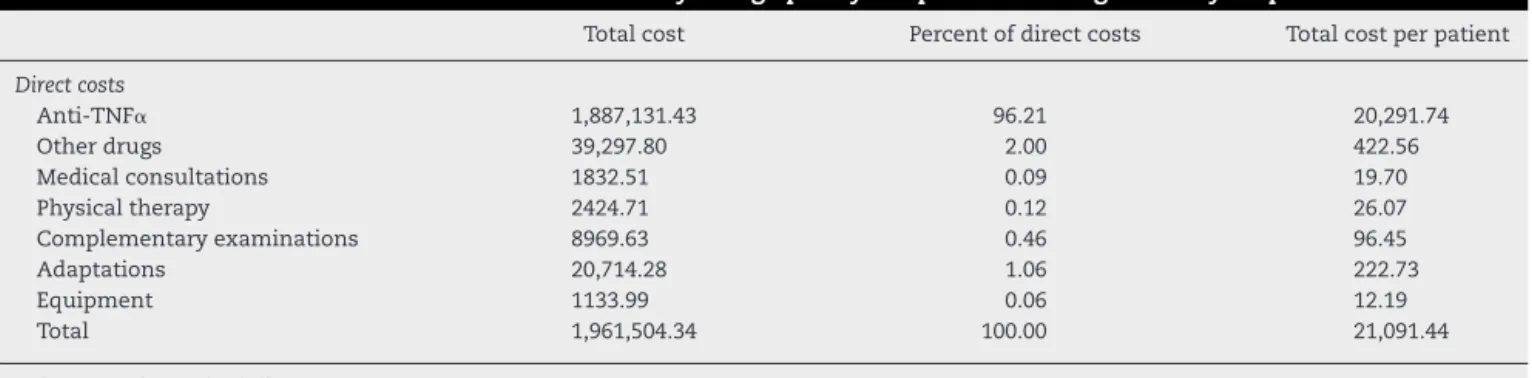
Table4–Totaldirectcostsrelatedtotreatmentofankylosingspondylitispatientsduringanoneyearperiod.
Totalcost Percentofdirectcosts Totalcostperpatient
Directcosts
Anti-TNF␣ 1,887,131.43 96.21 20,291.74
Otherdrugs 39,297.80 2.00 422.56
Medicalconsultations 1832.51 0.09 19.70
Physicaltherapy 2424.71 0.12 26.07
Complementaryexaminations 8969.63 0.46 96.45
Adaptations 20,714.28 1.06 222.73
Equipment 1133.99 0.06 12.19
Total 1,961,504.34 100.00 21,091.44
Valuesareshownindollar.
contributingtotheincreaseinthedirectcostsofdiagnosing andtreatingthedisease.
Non-steroidalanti-inflammatories werethe mostwidely usedmedications inthis study;however, the costofthese medicationscorrespondstoapproximately0.6%ofthetotal spendingonmedications.Thesecondmostwidelyusedclass ofmedicationswasthebiologicals,corresponding63.44%of thesample.Thecostofthesedrugscorrespondedto97.96% ofthespendingonmedicationsand87.53%ofthetotalcost oftreatment.Thelargerproportionofspendingonbiological medicationshadalreadybeenobservedinBrazil;inthat sam-ple,only13.33%ofthesampleusedbiologicalmedicationsbut thesewereresponsiblefor80%ofdrugspendingand74%of thetotalcost.12Ourobjectivewasnottocomparethecostsof
differentbiologicaltherapies,asthisisthesubjectofastudy currentlyunderwayatthesamefacility.
Physicaltherapywasresponsibleforasmall increasein costs, US$ 26.00 per person, which demonstrates a small degreetowhichthistherapeuticresourceisused.
Only14patientsreportedcostsrelatedtoadaptingtheir residences,representingonly1%ofdirectcostsofthedisease. Nevertheless,thisnumbermaynotcorrespondtoreality,asit dependsonthesubjects’ memories.Costsrelatedto trans-portationwere notobtainedduetothe degreeofdifficulty associatedwiththesamplesubjectsprovidingthis informa-tioninretrospect;however,Torresreportedinhisstudythat thesecostscouldrepresentaround2%ofdirectcostsand1% oftotalcosts.12
Indirectcostsassociatedwith retirementand sickleave constitute8.9%oftotalcosts.Asthediseaseprimarilyaffects youngpeopleintheproductiveageranges,inabilitytowork isoneofthefactorsthatcontributestotheincreaseintotal costs.Nearly59%ofthesamplewasretiredoronleavefrom workasaresultofthedisease,whichissimilartothefindings byTorres(56%).
Inthecurrentstudy,totalannualcoststotreat93patients withASreachedatotalofUS$2,156,070.83dollars/yearand a mean value ofUS$ 23,183.56/patient/year, while Torres’s studyfoundatotalof4597.00/patient/year.Anincreaseinthe costoftreatingASpatientsinBraziloverthelastthreeyears wasfound,particularlyasaresultoftheadditionofanti-TNF agentstothetherapeuticarsenalintreating spondyloarthri-tis.
ThedirectcostswereUS$1,961,504.34,correspondingto 90.9%oftotalcosts,whileindirectcostswereUS$194,566.49, correspondingtoonly9.1%oftotalcosts.Thisdataindicates adivergencefromthedatageneratedbyTorres’sstudy,which founddirectcostsof45%andindirectcostsof55%,despite thefactthatthetotalnumberofretiredpatientsandpatients onleaveweresimilarinbothstudies.Theresultweobtained was principally due to the higher costs oftreatment with anti-TNF agents, which are now used on a larger scale in Brazil.
Theintroduction of newmedications based onthe rec-ommendationsoftheASASgroupandtheBrazilianSociety of Rheumatology since2006 haverevolutionised the treat-ment of people with axial spondyloarthritis.16–19 Patients
withASare prescribedanti-TNF medicationsafterthe fail-ureofatleasttwonon-steroidalanti-inflammatories(NSAIDs) over a period of three months, without the need to use disease-modifying antirheumatic drugs (DMARDs) before-hand,accordingtotheBrazilianpublichealthsystem(SUS) protocol.20Consequently,thereisanearlieruseofthese
bio-pharmaceuticals inAS comparedwithother diseases such asrheumatoidarthritis(RA)andpsoriaticarthritis(PsA)with peripheralmanifestations,forexample,inwhichitis neces-saryto demonstratethe therapeuticfailure ofatleasttwo DMARDs.
InBrazil,threeanti-TNFmedicationsareavailablefor treat-ingASpatientsinthepublichealthsystem. Inoursample,
Table5–Totalindirectcostsrelatedtotreatmentofankylosingspondylitispatientsduringanoneyearperiodbasedon humancapitalapproach.
Numberofpatients(%oftotalnumber) Totalcost Costperpatient
RetirementduetoAS 51(54.83%) 184,761.57 3622.78
SickleaveduetoAS 4(4.30%) 9804.92 2451.23
Unemployed 8(8.6%)a
noneofthe patientshad thefinancialresources topayfor theirtreatmentthemselves,consideringthemeanindividual andhouseholdincomeofeach,aswellasthefactthatthey alsodidnothaveaccesstoprivatehealthplans.Furthermore, duringtheperiodthisdatawasbeingcollected,itwasrareto findcasesofASpatientsbeingtreatedbytheprivatehealth caresystem.
Duetotheincreaseintheincoherentcostsoftreatment withanti-TNF agents,cost effectivenessstudies havebeen conducted.StudiesbyKobeltetal.8,9indicatethatinfliximab
iscost-effectiveanditsuseisjustifiedbytheincreasein qual-ityoflifeandthereductionofthecostsofthedisease;atthe sametime,Boonenetal.10proposetheneedtoidentifythe
patientsinwhichtreatmentwithinfliximabandetanercept willbeeffectiveandcost-effectivebecauseofthehighcosts associatedwithtreatment withbiologicals. Atthis present time,therehavebeennostudiesofcost-effectivenessinBrazil. Brazilhasfewstudiesaboutthesocio-economicand finan-cial impact of rheumatologic diseases. Due to the large expanseofthecountryandespeciallyinequalitiesin acces-singdiagnosticproceduresandtherapies,thecostprojections shouldnotbegeneralised.
Wealsobelievethat,withregardtotheincreaseindirect costsassociatedwithAS, the overallscene encountered in SouthAmericashouldnotdifferfromthefindingsinBrazil,as themajorityofcountriesonthecontinenthaveincorporated anti-TNFtherapyintothetreatmentofASpatients.
Itisimportanttostressthatstudiesoftheimpactonquality oflifehavereinforcedtheneedformoreeffectiveparticipation byotherhealthprofessionalsinthemonitoringandtreatment ofpatientswithAS,andthisalsocouldberesponsiblefora partialincreaseincosts.21,22
Anadditionallimitationofourstudyisthatalthoughthe authorsbelievethattheclinicalandepidemiological charac-teristicsofthepatientsamplearerepresentativeoftheother patientsservedbytheSUS,ourstudytrackedasampleserved atauniversityhospitallocatedinalargestatecapitalinBrazil, acity whereaccesstomoreexpensivehealthtechnologies suchasnuclearmagneticresonanceimaginghasbeen eas-ierinrelationtothechallengesfacedbypatientsinotherSUS hospitalsinmoreremotelocationsthroughoutBrazil.
Conclusions
TheBrazilianpublichealthsystem’sspendingrelatedto anky-losingspondylitishasincreasedinrecentyears.Animportant partofthesecostsisdue tothe introductionofnew,more expensivehealthtechnologies,asinthecaseofnuclear mag-neticresonanceand,principally,thecostsresultingfromthe incorporationofanti-TNF biologicaltherapyintothe thera-peuticarsenal.Themeanannualdirectandindirectcostto theBrazilianpublichealthsystemtotreatapatientwith anky-losingspondylitis,accordingtoourfindings,isUS$23,183.56.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Sampaio-BarrosPercivalD,AzevedoVF,BonfiglioliR,Campos WR,CarneiroSCS,CarvalhoMAP,etal.ConsensoBrasileirode Espondiloartropatias:EspondiliteAnquilosanteeArtrite Psoriásica.DiagnósticoeTratamento–PrimeiraRevisão.Rev BrasReumatol.2007;47:233–42.
2.DougadosM.Diagnosticfeaturesofankylosingspondylitis.Br JRheumatol.1995;34:301–5.
3.VanDerLindenS,VanDerHeijdeD.Ankylosingspondylitis: clinicalfeatures.RheumDisClinNAm.1998;24:
663–76.
4.ReveilleJD,BallEJ,KhanMA.HLA-B27andgenetic predisposingfactorsinspondyloarthropathies.CurrOpin Rheumatol.2001;13:265–72.
5.HuscherD,MerkesdalS,ThieleK,ZeidlerH,SchneiderM, ZinkA.Costofillnessinrheumatoidarthritis,ankylosing spondylitis,psoriaticarthritisandsystemiclupus erythematosusinGermany.AnnRheumDis.2006;65: 1175–83.
6.FrauendorfR,PinheiroMdeM,CiconelliRM.Variablesrelated toworkproductivitylossinpatientswithankylosing spondylitis.RevBrasReumatol.2013;53:303–9.
7.GordeevVS,MaksymowychWP,SchachnaL,BoonenA. Understandingpresenteeisminpatientswithankylosing spondylitis:contributingfactorsandassociationwithsick leave.ArthritisCareRes(Hoboken).2014;66(6):916–24.
8.KobeltG,Andlin-SobockiP,MaksymowychWP.The cost-effectivenessofinfliximab(Remicade)inthetreatment ofankylosingspondylitisinCanada.JRheumatol.
2006;33:732–40.
9.KobeltG,Andlin-SobockiP,BrophyS,JonssonL,CalinA, BraunJ.Theburdenofankylosingspondylitisandthe cost-effectivenessoftreatmentwithinfliximab(Remicade).J Rheumatol.2004;43:1158–66.
10.BoonenA,vanderHeijdeD,SeverensJL,BoendermakerA, LandewéR,BraunJ,etal.Markovmodelintothecost-utility overfiveyearsofetanerceptandinfliximabcomparedwith usualcareinpatientswithactiveankylosingspondylitis.Ann RheumDis.2006;65:201–8.
11.BoonenA,vanderHeijdeD,LandewéR,GuilleminF, Rutten-vanMölkenM,DougadosM,etal.Directcostsof ankylosingspondylitisanditsdeterminants:ananalysis amongthreeEuropeancountries.AnnRheumDis. 2003;62:732–40.
12.TorresTM,FerrazMB,CiconelliRM.Resourceutilisationand costofankylosingspondylitisinBrazil.ClinExpRheumatol. 2010;28:490–7.
13.MerkesdalS,RuofJ,HuelsemannJL,SchoeffskiO,MaetzelA, MauW,etal.Developmentofamatrixofcostdomainsin economicevaluationofrheumatoidarthritis.JRheumatol. 2001;28:657–61.
14.AgenciaNacionaldeVigilanciaSanitária.Prec¸omáximode medicamentosporprincipioativoparacompraspúblicas. Availablefrom:http://s.anvisa.gov.br/wps/s/r/f6[accessed 19.07.13].
15.Brazilianminimumwage.Availablefrom:
http://www.guiatrabalhista.com.br/guia/salariominimo.htm
[accessed15.05.14].
16.vanderHeijdeD,SieperJ,MaksymowychWP,DougadosM, Burgos-VargasR,LandewéR,etal.Assessmentof
SpondyloArthritisInternationalSociety.2010Updateofthe internationalASASrecommendationsfortheuseofanti-TNF agentsinpatientswithaxialspondyloarthritis.AnnRheum Dis.2011;70:905–8.
17.RudwaleitM,BraunJ,SieperJ.Assessmentof
criteriaforaxialspondyloarthritis.ZRheumatol. 2009;68(7):591–3.
18.BraunJ,vandenBergR,BaraliakosX,BoehmH,
Burgos-VargasR,Collantes-EstevezE,etal.2010updateofthe ASAS/EULARrecommendationsforthemanagementof ankylosingspondylitis.AnnRheumDis.2011;70: 896–904.
19.Sampaio-BarrosPD,KeisermanM,MeirellesEdeS,Pinheiro MdeM,XimenesAC,AzevedoVF,etal.Recommendationsfor themanagementandtreatmentofankylosingspondylitis. RevBrasReumatol.2013;53:242–57.
20.MinistériodaSaúde.Availablein:
http://200.214.130.94/consultapublica/index.php?modulo=display&sub=dsp
[accessed25.10.12].
21.LeeTJ,ParkBH,KimJW,ShinK,LeeEB,SongYW.
Cost-of-illnessandqualityoflifeinpatientswithankylosing spondylitisatatertiaryhospitalinKorea.JKoreanMedSci. 2014;29:190–7.