Arq. Gastroenterol. vol.51 número2
Texto
Imagem
Documentos relacionados
Several reports showed the association of single nucleotide polymorphisms (SNPs) of the preproghrelin gene with type 2 diabetes, obesity, insulin resistance, metabolic
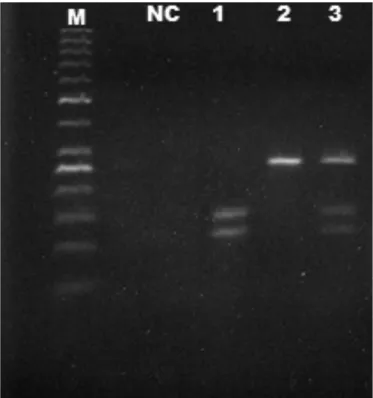
In view of this finding, we genotyped the rs2891230 single-nucleotide polymorphism (TaqManH SNP genotyp- ing assay, Applied Biosystems Inc, Foster City, CA, USA) of the HMCN1 gene
The biologic effect of the studied single nucleotide polymorphism (SNP) and odds ratios (OR) for polymorphisms which have been shown to be associated with risk of Crohn's disease
Genome structure variations including single nucleotide polymorphism (SNP) have been identified for genes coding Wnt and its related signaling pathway and are likely to
We examined the association of seven single nucleotide polymorphisms (SNPs) across the LTA gene, and their related haplotypes, with risk of myocardial infarction (MI) in
Results: There was evidence of association between the single nucleotide polymorphism rs17368528 in exon five of the H6PD gene, which encodes an amino-acid change from proline
The genetic diversity of a single nucleotide polymorphism (SNP) at the exon 20 (T945M) of the leptin receptor gene (LEPR) and of three short tandem repeats (STRs BM7225, BMS694,
It has been suggested that single nucleotide polymorphisms (SNPs) in the MDR1 gene may have an impact on the expression and function of Pgp, therefore influencing susceptibility
