Correspondence address:
Lívia Rodrigues Santos
Av. Alfredo Balena, 190/275, Bairro Santa Eigênia, Belo Horizonte (MG), Brazil, CEP: 30130-100.
E-mail: [email protected]
Received: 18/1/2012
Accepted: 16/8/2012
Study carried out Speech Therapy Course, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brazil.
(1) Speech Therapy Course, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brazil. (2) Department of Pathology, Faculty of medicine, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brazil.
(3) Graduate Program (Ph.D.) in public health, Preventive and Social Medicine Department, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brazil.
(4) Department of Preventive and Social Medicine, Faculty of medicine, Universidade Federal de Minas Gerais – UFMG – Belo Horizonte (MG), Brazil.
Conlict of interests: nothing to declare.
Adesão das professoras disfônicas ao
tratamento fonoterápico
ABSTRACT
Purpose: To study the possible factors associated with adherence to the speech-language pathology treatment of dysphonia in female teachers of municipal schools of Belo Horizonte. Methods: This was a retrospective study that analyzed the medical records of 251 teachers treated at the Voice Ambulatory Speech Language Pathology Service, Hospital das Clínicas da Universidade Federal de Minas Gerais (AV-UFMG) from August 2007 to December 2009. The collected data included age, number of scheduled sessions, number of absences, number of children, type of dysphonia, degree of dysphonia, monthly family income, and education. We calculated the distance, in kilometers, of the residence to the place of treatment and the workplace to place of treatment. We also analyzed the social vulnerability index of the workplace. Results: The results of this research indicated that of the 135 records that were included in the study, 89 (65.93%) corresponded to the discharged group and 46 (34.07%) corresponded to the abandonment group. In comparison with all the variables studied, only the number of faults and the type of dysphonia were associated with poor adherence to voice therapy. Conclusion: Results showed that the number of absences in sessions, treatment-related factor, organofuncional dysphonia type, and clinical-related factor were all associated with the abandonment of voice therapy.
RESUMO
Objetivo: Estudar os possíveis fatores associados à adesão ao tratamento fonoaudiológico para a disfonia, em mulheres professoras da Rede Municipal de Ensino de Belo Horizonte. Métodos: Trata-se de um estudo retrospectivo, no qual foram analisados 251 prontuários de professores atendidos no Ambulatório de Voz do Serviço de Fonoaudiologia do Hospital das Clínicas da Universidade Federal de Minas Gerais (AV-UFMG) no período de 2007 a 2009. Foram coletados os seguintes dados: idade, número de sessões programadas, número de faltas, número de ilhos, tipo de disfonia, grau da disfonia, renda mensal familiar e escolaridade. Calculou-se a distância, em quilômetros, da residência ao local do tratamento e do local de trabalho ao local do tratamento fonoaudiológico. Analisou-se também o Índice de Vulnerabilidade Social do local de trabalho. Resultados: Dos 251 prontuários analisados, 135 preencheram os critérios de inclusão. Destes 89 (65,93%) correspondem ao grupo que recebeu alta e 46 (34,07%) ao grupo que abandonou o tratamento. Das variáveis estudadas, apenas o número de faltas e o tipo de disfonia apresentaram relação com a adesão à terapia de voz. Conclusão: O número de ausências às sessões, fator relacionado ao tratamento, e a disfonia do tipo organofuncional, aspecto referente ao quadro clínico, mostraram-se associados ao abandono da terapia de voz.
Artigo Original
Lívia Rodrigues Santos1
Letícia Almeida1
Letícia Caldas Teixeira2
Iara Bassi3
Ada Ávila Assunção4
Ana Cristina Côrtes Gama2
Keywords
Voice Faculty Speech therapy Patient compliance Dysphonia Speech, language hearing sciences
Descritores
group that is at risk for developing these symptoms of dyspho-nia, as shown by the data of medical licenses, clearances, and functional rehabilitation(2,3). The implications of dysphonia for the performance of professional practice are well documented(4). However, it is known that the impact of dysphonia in teachers is not restricted to the individual ield, because the labor reper-cussions cited manifest themselves in social, economic, and professional range, with a view to the activity of these teachers(5).
Dysphonia can be treated through speech therapy focused on behavioral changes and therefore depends on the active partici-pation of patients in the process. Thus, it is crucial that a patient understands that he should be part of the therapeutic plan(6,7).
Even with the vocal symptoms and their negative conse-quences on the quality of life(8), it is acknowledged that though membership of the speech therapy is not immediate(7), it is not uncommon to abandon the treatment. As seen in cases of chronic diseases, poor adherence to long-term treatments is a world-wide phenomenon(9). Several factors are superimposed to such behavior and thus relate to the characteristics of the profession, to the type and severity of the symptoms, to the complexity of the treatment, and to the cultural and socio-psychological aspects of patients(10,11).
Treatment adherence is a dynamic process, inluenced by a number of factors that predisposes the continuity of the treat-ment, which urges the ongoing monitoring strategy(12). Studies on joining the voice therapy, point out that most of the patients did not complete the speech therapy, in spite of the recognized effectiveness of the current therapeutic resources(13,14).
From this perspective, we consider relevant investigative projects that seek to identify and understand the mediations that compete for adherence to speech-language treatment for dysphonia. Understanding the factors associated with adherence to speech therapy by teachers can help in adoption of strate-gies that enable to optimize the treatment, and consequently reduces the labor losses arising due to dysphonia. Thus, the present research aims to study the possible factors associated with treatment adherence for dysphonia, in teachers of the Rede Municipal de Ensino de Belo Horizonte (RME-BH).
METHODS
This is a retrospective, observational, and an analytical research study. We analyzed the medical records of 251 dys-phonic teachers of RME-BH, who underwent language therapy in the Outpatient Speech Services Speech Therapy, Hospital das Clínicas of the Universidade Federal de Minas Gerais
dysphonia; receiving delivery of GSPM of Belo Horizonte; and having completed clinical documentation, including speech therapy evaluation and ear, nose, and throat evaluation. The following exclusion criteria were adopted: to complain for non-speech voice; and to appear only to non-speech therapy evaluation or vocal guidance workshops (three meetings whose purpose was to address issues associated to vocal production and pro-vide guidance on vocal behavior in professional practice). We decided to exclude male teachers because of less number of men in the teaching profession.
The response variable, i.e., the variable of greatest interest in this research, was considered as the status of “discharged” or “abandonment” of language therapy. Discharged criteria, used in voice and speech of the institution, are as follows: absence of complaint from vocal fatigue, vocal quality adapted to the ana-tomical and functional conditions of the larynx (perception and hearing assessed through otorhinolaryngological examinations), and/or itness vocal resistance to social and professional patient demand. It is considered as abandonment of treatment has three consecutive unexcused absences, the impossibility of informed attendance, or declared option by stopping the treatment.
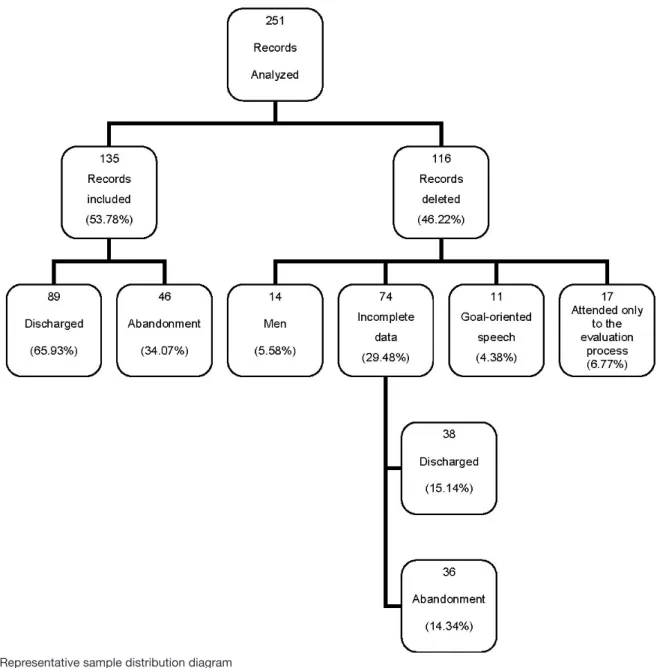
Of the 251 records, which were set previously and selected for the study, 135 (53.78%) records were included and 116 (46.22%) records were excluded (Figure 1). The excluded records repre-sented the following: 14 (5.58%) were men; 74 (29.48%) were the cases caused due to the incompleteness of the data records, of which 38 (15.14%) cases belonged to the group that were discharged from the treatment and 36 (14.34%) cases belonged to the group that abandoned the treatment; 11 (4.38%) teachers who participated only in the workshops of vocal guidance, without indication of speech treatment; and 17 (6.77%) teachers who did not attend the session following the evaluation.
The following data were collected from the medical records: age, number of sessions, number of absences (categorized by median), number of children, type of dysphonia(15), grade of dysphonia(16) (indicated by the parameter G of the GRBASI scale), monthly family income, and education.
We calculated the distance, in kilometers, from the residence of the professor to the treatment site and from the workplace to the speech treatment site. We also examined the social vul-nerability index (SVI) of the school teacher, to understand the elements of context. On the whole, these data were considered as explanatory variables in the analysis.
associated with discharged and abandonment groups, binary logistic regression was used. The magnitude of each factor with the therapy’s abandonment was measured by the odds ratio (OR) and statistical signiicance at a conidence interval of 95% (95%CI). All associated factors at the signiicance level of p≤0.20 in univariate analysis were included in the multivariate model through sequential deletion of variables. The final multivariate model included variables associated with signiicance level of p≤0.05.
We consider the signiicance level of p<0.20, because this step of univariate analysis serves as a criterion for selection of the variables that enter into a inal model of the survey. Because this is an initial step and not deinitive data analysis, we can be less stringent and adopt levels of signiicance larger than the usual (for example, 0.15 or 0.20), and there will be no risk of discarding important variables. We used the Hosmer-Lemeshow test for the veriication of the inal it of the model.
Data collection was performed at the AV-UFMG. The research was approved by the Research Ethics Committee of
Figure 1. Representative sample distribution diagram
the same institution, under the ETIC 48208 opinion. All the participants signed an informed consent form.
RESULTS
In univariate analysis, the association of the variables de-scribed above for the discharged-abandonment groups was not signiicant at p<0.20 level, namely: age (p=0.302), number of children (p=0.610), number of scheduled sessions (p=0.250), residence distance therapy (p=0.228), and distance work therapy (p=0.405).
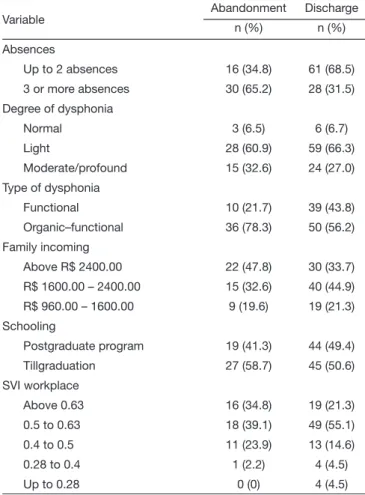
The proportions of the categorical variables (Table 2) were also obtained. The abandonment group was characterized by
sessions Discharge 15.03 7.59
Residence-therapy distance (km)
Abandonment 13.54 7.01
Discharge 15.63 10.57
Work-therapy distance (km) Abandonment 16.29 6.19 Discharge 15.33 6.46
Legends: SD = standard deviation
Table 2. Description of the categorical variables studied in patients who were discharged and those who abandoned the treatment
Variable Abandonment Discharge
n (%) n (%)
Absences
Up to 2 absences 16 (34.8) 61 (68.5)
3 or more absences 30 (65.2) 28 (31.5) Degree of dysphonia
Normal 3 (6.5) 6 (6.7)
Light 28 (60.9) 59 (66.3)
Moderate/profound 15 (32.6) 24 (27.0)
Type of dysphonia
Functional 10 (21.7) 39 (43.8)
Organic–functional 36 (78.3) 50 (56.2) Family incoming
Above R$ 2400.00 22 (47.8) 30 (33.7)
R$ 1600.00 – 2400.00 15 (32.6) 40 (44.9) R$ 960.00 – 1600.00 9 (19.6) 19 (21.3) Schooling
Postgraduate program 19 (41.3) 44 (49.4)
Tillgraduation 27 (58.7) 45 (50.6)
SVI workplace
Above 0.63 16 (34.8) 19 (21.3)
0.5 to 0.63 18 (39.1) 49 (55.1)
0.4 to 0.5 11 (23.9) 13 (14.6)
0.28 to 0.4 1 (2.2) 4 (4.5)
Up to 0.28 0 (0) 4 (4.5)
Legends: SVI = social vulnerability index
Table 3. Result of multivariate binary logistic regression, “speech therapy discharge” as reference category
Factors Abandonment
p-value OR (95% IC) Absences
Up to 2 absences 1.0
3 or more absences <0.000* 3.67 (1.71–7.92) Type of Dysphonia
Functional 1.0
Organic–functional 0.043* 2.34 (1.0–5.49)
* Signiicant values (p≤0.05) Legends: OR = odds ratio
p<0.20 level, namely: education (p=0.370), degree of dysphonia (p=0.775), grade of moderate-profound dysphonia (p=0.493), family income of R$ 1,600–2,400 (p=0.375), family income of R$ 960–1,600 (p=0.644), SVI of 0.5–0.63 (p=0.999), SVI of 0.4–0.5 (p=0.999), SVI of 0.28–0.4 (p=0.999), and SVI up to 0.28 (p=0.999). However, the associations of the variables “absences” and “type of dysphonia” with the discharged-aban-donment group were found to be signiicant at p<0.20 level, namely: absences (p<0.000) and type of dysphonia (p=0.013).
Final multivariate model was presented with the vari-ables that were statistically associated with the discharged- abandonment groups to a signiicance level of p<0.05 (Table 3). The OR statistics or the probability of the occurrence of events was demonstrated. The variables concerning the number of absences and the type of dysphonia were associated with the abandonment of the therapy. Patients with three or more absences had 3.67 more chances to abandon the treatment. The type of dysphonia was also positively associated with the abandonment of the therapy, and the patients with organic and functional dysphonia had 2.34 more chances, likely to abandon the treatment. The model showed good quality of it as evalu-ated by the Hosmer-Lemeshow’s test (p=0.399).
DISCUSSION
Low adherence to treatments is a problem worldwide. In developed countries, in comparison with developing countries, adherence to long-term treatment in the general population is around 50%(9).
that the lowest proportion of abandonment is related to the pro-ile of the patients observed in this research study, because they depended on their voice to perform their professional activities. It is thus known that dysphonia can lead to career damage(2,4), leading to believe that the largest accession of teachers to be treated is related to the risks of losses.
The age group was found to be compatible with 42 years of average (DP8) described in a previous article, in which there was an association between age and adherence to speech treatment(2). A number of children interfered in various health situations and events in women’s group(17), but we did not ind an association with adherence to speech treatment. In the investigated literature, studies which compared these effects were not identiied.
Concerning the number of scheduled sessions, an aver-age of 15 sessions for both groups (Table 1) differs from a study(13) that described a mean duration of 5–5.6 voice therapy sessions. In relation to a teaching hospital, with periods of disruption in outpatient, follow-up is possible to prolong the treatment, including a higher number of sessions. Besides, speech treatment differs from one service to another, and it may involve different procedures and number of sessions. However, as mentioned in the literature, it is worth men-tioning the absence of association between the number of sessions of speech therapy and adherence to treatment for future studies(13).
The distance between the residence and the workplace and between the residence and the place of treatment was not as-sociated with the abandonment group (p=0.228 and p=0.405, respectively). Despite the dificulty of access being mentioned among the barriers to continue speech-language therapy(10), other studies have not been found that focus such an issue.
Regarding the number of absences on sessions, the results indicated that patients with three or more absences had 3.67 more chances, likely to abandon the treatment (p<0.000) ( Table 3). The published literature does not conirm the direct relationship between the number of absences and the speech-language therapy adherence. However, it points out that the number of sessions is the strongest predictor for the completion of voice therapy(13) for each new session conducted (after evaluation).
Each new session conducted (after evaluation) resulted in a 1.6 times greater probability to complete the vocal treatment. When it is considered that non-attendance in the sessions can be associated with individual factors, such as the level of motiva-tion of the patient for therapy, it becomes reasonable to infer about their role in the adherence. A study shows that individu-als who claim to be motivated for treatment, have 3.06 times more chance of adherence to the pharmacological treatment for diabetes mellitus(18).
Regarding the degree of dysphonia, obtained through perceptual-hearing evaluation, the results were found to be consistent with the published literature. An association among the grade of dysphonia and vocal therapy adherence was not observed(14). Therefore, the degree of vocal devia-tion does not seem to inluence the patient’s motivadevia-tion to continue therapy and, consequently, complete the speech-language treatment.
The type of dysphonia was also positively associated to the abandonment of therapy (Table 3), and patients with organo-functional dysphonia had 2.34 more chances, likely to abandon the treatment. Considering that organofunctional dysphonia corresponds to the clinical evolution of functional dysphonia(15), it can be assumed that the teachers with this type of dysphonia took more time to search for professional help. Published litera-ture points out that the self- assessment of a vocal teacher shows the satisfaction of most of them to own voice, which alludes to the dificulty of these professionals in to self-evaluate and understand vocal changes(19). It is the consensus that focused on the disease itself, such as the patient’s perception about his health problems and strategies to deal with the disease and its symptoms and impact on quality of life are able to inluence not only the demand for care, but also the process of adherence to the proposed treatment(12,20). In this way, such a result may be associated with dificulty in vocal problem’s perception and the resistant behavior to admit the dysphonia or search for an expert help.
The result that indicates no association with family in-come, given the reports of patients under the inluence of the inancial terms on the abandonment of language therapy, was unexpected(21). This result differs from a study(18) in which the patients with diabetes mellitus were analyzed. Future research to clarify the relationship between income and adherence would be useful.
Schooling also was not associated with the abandonment to voice therapy (p=0.370). The literature points to conlicting results regarding to schooling. In a previous study, the college level was associated with adherence to healthy eating diets(22). On the other hand, in another study there was no association between the level of education and adherence to treatment with anti-retroviral therapy(23).
The SVI aimed to understand the population access to ive “Dimensions of Citizenship”, observed as essential factor to reach the following: environmental, cultural, economic, legal, and survival security(24). The “Dimensions of Citizenship” con-sist of variables, which in turn concon-sist of indicators, namely, numerical data from which the IVS is calculated. The calcula-tion is carried out by means of successive aggregacalcula-tions made by means of weighted arithmetic means and its inal value varies between zero and one. As the IVS expresses a negative attribute, the social vulnerability of a population will be greater than the higher value, that is, the higher the value of the IVS, a population is subjected to more vulnerable social exclusion(24). In summary, the IVS combines different variables on a gauge whose purpose is to synthesize relevant information that relects the cited inequalities and social risk areas(18).
dynamic process that characterizes the speech-language treat-ment adherence. It is expected to have added knowledge to the design of future studies and contributed to better approach of patients during their treatment.
CONCLUSION
The analysis of medical records of 135 teachers treated in AV-UFMG from August 2007 to December 2009 showed that most of them joined speech-language treatment for dyspho-nia. The variables concerning the number of absences and the organofunctional type of dysphonia were associated with the abandonment of voice therapy.
ACKNOWLEDGEMENTS
We thank Fundação de Amparo à Pesquisa do estado de Minas Gerais-FAPEMIG (01474-10) for inancing this study.
* LRS, LA, LCT, IB, AAA and ACCG participated in preparing this study. All helped to build and develop the research, since the revision literature, analysis of results, discussion and conclusions. LRS and LA collaborated with data collection.
REFERENCES
1. Roy N, Weinrich B, Gray SD, Tanner K, Stemple JC, Sapienza CM. Three treatment for teachers with voice disorders: a randomized clinical trial. J Speech Lang Hear Res. 2003;46(3):670-88.
2. de Medeiros AM, Barreto SM, Assunção AA. Voice disorder (dysphonia) in public school female teachers working in Belo Horizonte: prevalence and associated factors. J Voice. 2008;22(6):676-87.
3. Unterbrink T, Zimmermann L, Pfeifer R, Wirsching M, Brähler E, Bauer J. Parameters inluencing health variables in a sample of 949 German teachers. Int Arch Occup Environ Health. 2008;82(1):117-23.
8. Jardim R, Barreto SM, Assunção AA. Condições de trabalho, qualidade de vida e disfonia entre docentes. Cad Saúde Pública. 2007;23(10):2439-61. 9. World Health Organization (WHO). Adherence to long-therm therapies
evidence for action. WHO Library Cataloguing-in-Publication Data. 2003. 10. Portone C, Johns MM, Hapner ER. A review of patient adherence to the
recommendation for voice therapy. J Voice. 2008;22(2):192-6. 11. van Leer E, Connor NP. Patient perceptions of voice therapy adherence.
J Voice. 2010;24(4):458-69.
12. Silveira LMC, Ribeiro VMB. Grupo de adesão ao tratamento: espaço de “ensinagem” para proissionais de saúde e pacientes. Interface – Comunic., Saúde, Educ. 2005;9(16):91-104.
13. Portone-Maira C, Wise JC, Johns MM, Hapner EE. Differences in temporal variables between voice therapy completers and dropouts. J Voice. 2011;25(1):62-6.
14. Hapner E, Portone-Maira C, Johns MM. A study of voice therapy dropout. J Voice. 2009;23(3):337-40.
15. Behlau M, Azevedo R, Pontes P. Conceito de voz normal e classiicação das disfonias. In: Behlau M. Voz: O livro do especialista. Rio de Janeiro: Revinter; 2001.p. 53-79.
16. Hirano M. Clinical examination of voice. New York: Springer Verlag. 1981. 17. Rocha LE, Debert-Ribeiro M. Trabalho, saúde e gênero: estudo
comparativo sobre analistas de sistemas. Rev Saúde Pública. 2001;35(6):539-47.
18. Assunção TS, Ursine PGS. Estudo de fatores associados à adesão ao tratamento não farmacológico em portadores de diabetes mellitus assistidos pelo Programa Saúde da Família, Ventosa, Belo Horizonte. Ciênc Saúde Coletiva. 2008;13(2):2189-97.
19. Penteado RZ, Pereira IM. Qualidade de vida e saúdevocal de professores. Rev Saúde Pública. 2007;41(2):236-43.
20. Leite SN, Vasconcellos MPC. Adesão à terapêutica medicamentosa: elementos para a discussão de conceitos e pressupostos adotados na literatura. Ciênc saúde colet. 2003;8(3):775-82.
21. Esteves D, Silva MR. Estudo de adesão e abandono dos respiradores orais encaminhados para fonoterapia. São Paulo: CEFAC, 2005. Disponível em: http://www.cefac.br/publicar/arquivos/SP_adesao_e_abandono_de_ RO_na_fonoterapia.pdf
22. Martin KA, Bowen DJ, Dunbar-Jacob J, Perri MG. Who will adhere? Key issues in the study and prediction of adherence in randomized controlled trials. Control Clin Trials. 2000;21(5):195-9.
23. Colombrini MR, Coleta MF, Lopes MH. Fatores de risco para a não adesão ao tratamento com terapia antiretroviral altamente eicaz. Rev Esc Enferm USP. 2008;42(3):490-5.