SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Keblish’s
lateral
surgical
approach
enhances
patellar
tilt
in
valgus
knee
arthroplasty
夽
José
Roberto
Tonelli
Filho
∗,
Marcus
Ceregatti
Passarelli,
João
Alberto
Salles
Brito,
Gustavo
Constantino
Campos,
Alessandro
Rozim
Zorzi,
João
Batista
de
Miranda
UniversidadeEstadualdeCampinas(Unicamp),FaculdadedeCiênciasMédicas,DepartamentodeOrtopediaeTraumatologia,Campinas, SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30January2016 Accepted15February2016 Availableonline25October2016
Keywords:
Knee Osteoarthritis Arthroplasty Patella
a
b
s
t
r
a
c
t
Objective:Tocomparetheclinicalandradiologicaloutcomesofconventionalmedialand lateralapproachesfortotalkneereplacementinthevalgusosteoarthriticknee.
Methods:Inthisrandomizedcontrolledtrial,21patientswithvalguskneeosteoarthritiswere randomizedtototalkneereplacementthroughmedialorlateralapproach.Theprimary outcomewasradiographicpatellartilt.Secondaryoutcomeswerevisualanalogscaleof pain,postoperativelevelsofhemoglobin,andclinicalaspectoftheoperativewound.
Results:Therewerenodifferencesbetweenthegroupsregardingotherclinicalvariables. Meanlateraltiltofthepatellawas3.1degrees(SD±5.3)inthelateralapproachgroupand 18degrees(SD±10.2)inthemedialapproachgroup(p=0.02).Therewerenodifferences regardingthesecondaryoutcomes.
Conclusion:Lateralapproachprovidedbetterpatellartiltfollowingtotalkneereplacement invalgusosteoarthriticknee.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Acesso
lateral
de
Keblish
melhora
a
inclinac¸ão
da
patela
na
artroplastia
do
joelho
valgo
Palavras-chave:
Joelho Osteoartrite Artroplastia Patela
r
e
s
u
m
o
Objetivo:Compararosresultadosclínicoseradiológicosdaviadeacessoconvencionalcom artrotomiamedialedaviadeacessolateralnaprótesetotalprimáriaemjoelhovalgo.
Métodos:Nesteensaioclínicoprospectivo,21pacientescomosteoartriteedeformidadeem valgoforamdivididosaleatoriamenteemdoisgruposdeacordocomaviadeacessocirúrgico usada:medialoulateral.Odesfechoprincipalfoiamedidaradiográficadainclinac¸ãolateral
夽
StudyconductedatHospitaldeClínicas,UniversidadeEstadualdeCampinas(Unicamp),Campinas,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](J.R.TonelliFilho).
http://dx.doi.org/10.1016/j.rboe.2016.10.010
dapatela.Outrosdesfechosforamadorapósacirurgia(escalavisualdedor),osangramento (níveisséricosdehemoglobina)eoaspectoclínicodaferidaoperatória.
Resultados: Nãohouvediferenc¸aentreosgruposemrelac¸ãoaoutrasvariáveisclínicas.A inclinac¸ãolateralmédiadapatelanogrupolateralfoi3,1graus±5,3DPenogrupomedial foi18graus±10,2DP(p=0,02).Osoutrosdesfechosnãoapresentaramdiferenc¸asentreos grupos.
Conclusão:Avialateralproveumelhorinclinac¸ãolateraldapatelapós-operatórianas artro-plastiasdojoelhovalgo.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Approximately10%ofpatientsundergoingtotalknee arthro-plastyhaveavalgusdeformity,definedasavalgusalignment oftheanatomicalaxesofthefemurandtibiainthefrontal planegreaterthan tendegrees.1 Inthesecases,the results
areconsideredlesssatisfactorywhencomparedwithpatients whohavevarusknees.2–5
Thestandardaccessrouteintotalkneearthroplastiesis themedialparapatellararthrotomy.6,7 Thelateral
parapatel-larapproachdescribedbyKeblish2allowsforabetterexposure
ofthelateral and posterolateral structures,whichare con-tractedinvalgusdeformitiesandshouldbereleasedforproper ligamentbalance;italsohastheadvantageofincludingthe releaseoflateralpatellarretinaculum,whichisnecessaryin mostcaseswithvalgusdeformity.2,8
Althoughsome authors recommend the use ofthe lat-eralaccessrouteincasesoffixedvalgusdeformitiesofthe knee,8,9thereisnoconsensusintheliteratureregardingthe
bestapproachfortotalarthroplastiesinvalgusknees.8,10
Thisprospectivestudy aimed tocompare the resultsof medialparapatellar accessroute (classical) and the lateral parapatellarapproach(Keblish)inpatientswithvalgusknees, inordertodemonstratethebestcorrectionofpatellartilt.
Material
and
methods
Detailedexplanationsoftheprocedureandresearchprotocol were givento21 patients withadvanced knee osteoarthri-tis,referredfromthebasicnetworkoftheBrazilianUnified HealthSystem(SistemaÚnicodeSaúde[SUS])toauniversity hospitalfortotalarthroplastysurgery.Allpatientsagreedto participateandsignedaninformedconsentform.Thestudy protocolandtheinformedconsentformwereapprovedbythe localResearchEthicsCommittee(CEP;opinionNo.381113of August27,2013).
Inclusioncriteria
- Patients ofbothgenders,between50 and75 years, diag-nosedwithkneeosteoarthritisandvalgusdeformity. - Indicationoftotalkneearthroplastyduetofailureof
con-servativetreatment.
- Havingunderstood,accepted,andsignedtheconsentform.
Exclusioncriteria
- Arthroplastyrevisionsurgery.
- Extra-articulardeformitiesnotrelatedtoosteoarthritis. - Previousinfectionintheknee.
- Severecomorbiditywithanestheticcontraindication. - Inabilitytounderstandorsigntheconsentform.
The study was registered at ClinicalTrials.gov (NCT01965886).
Allocation
Two groups were created: lateral and medial. A computer program (www.randomization.com) generated a random sequence,dividedintoblocksofsixunits,withthree indica-tionsforeachgroupineachblocktoavoidtheaccumulation ofasinglegroupatthebeginningoratendofthestudy,as wellastheeffectofthesurgeons’learningcurve.
Blinding
Each of these indications was kept in a box with sealed envelopesinthepossessionofanoperatingroomnursewho didnotparticipateinthestudy.Intheoperatingroom,after skinincision,theenvelopewasopenedtoindicatethegroup towhichthepatienthadbeenallocated.
Interventions
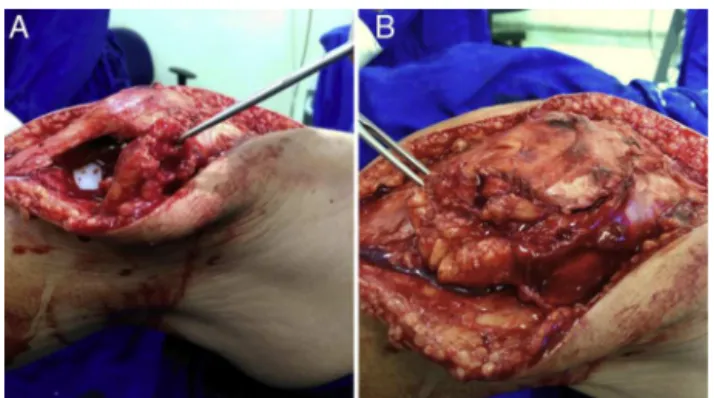
- Lateralgroup:lateralparapatellaraccessrouteandsoft tis-sueligamentbalanceasdescribedbyKeblish,2preservinga
flapoffat(Fig.1)forclosingtheunstressedjointcapsule. - Medial group: conventional medial parapatellar access
route and soft tissue ligament balance in the classic sequence.1
Surgicaltechnique
Fig.1–IllustrationofthesurgicaltechniqueusingKeblish’s
accessroute,demonstratingtheHoffafatflapneededfor
closurewithouttensionofthejointcapsule.A,thefatflap
isattachedtothelateralborderofthecapsule;B,fatisused
tocoverthedefectinthecapsule.
asingleintravenousdoseofcefazolin2g,30minbeforethe anestheticinduction. Apneumatictourniquet onthethigh (300mmHg)wasusedinallcases.
Thelongitudinalincisionintheskinwasthesameinall cases.Atthatpoint,theenvelopesealwasbrokenandthetype ofinterventiontobeperformedwasrevealed,asdescribedin theprevioussection.Thesequenceofguidesandbonecuts wasthe same.Theprosthesis(Modular III,MDT, RioClaro, SãoPaulo,Brazil)andtheorthopediccement(Cemfix, Tekn-imed,France)werethesameinallcases.Insomecases,rodsor wedgesfromtheprosthesiswerenecessary.Nocaserequired constrainedorsemi-constrainedprosthesis.Whenever pos-sible,thepatellarcomponentwasused.Inallcases,24-hour suctiondrainandRobertJonesbandagewereusedonthefirst day.
Rehabilitation
Allpatientsreceivedprophylaxisforthromboembolicevents withmechanical(earlymobilityandelevationofthelimb)and pharmacologicalmethods(lowmolecularweightheparinby subcutaneousinjectioninaprophylacticdosesuitableforthe patient’sweight)for15days.
Allpatientswerehospitalizedforthreedaysaftersurgery, and received training for walking with a walker. Then, outpatientfollow-upwasperformedtwiceaweekinthe phys-iotherapyservice ofthe same hospitalinwhich theywere operated,withthesamerehabilitationprotocol.
Outcomes
- Visual pain scale (0–100) was appliedbya staff member blinded totheallocationofgroupsinthe firstthreedays aftersurgery,whilethepatientswereintheward, accord-ingtovalidatedtechnique.11Forthestatisticalanalysis,the
meanofthesethreemeasuresforeachcasewasused. - Serumhemoglobinlevelswerecollectedonthedaybefore
and onthedayafterthesurgery.Thedifferencebetween these two values was used to determine the reduction inserum hemoglobinand therebyestimate thebleeding.
Patientswhoreceivedtransfusionofredbloodcellsorother bloodproductswereexcluded.
- Appearanceofthesurgicalwoundoneweekafterthe pro-cedure.
- Functional scales were applied twice a year by examin-ersblinded tothe allocationofgroups: the KneeSociety Score(KSS),12theWesternOntarioandMcMaster
Universi-tiesArthritisIndex(WOMAC),13andtheKujalaScale14;were
appliedtwiceayearbyexaminersblindedtotheallocation ofgroups.
- Alignmentoftheoperatedlimbinthefrontalorthostatic panoramicradiography,bipedal,sixmonthsaftersurgery, throughthemethodofanatomicalaxesofthefemurand tibiainthefrontalplane.15
- Patellartiltintheaxialradiographysixmonthsaftersurgery, accordingtothetechniquepreviouslydescribed16(Fig.2).
Statisticalanalysis
Thispilotstudywasconductedtodeterminethesamplesize necessary to compare the results oftotal arthroplastiesin knees withvalgusdeformity vialateral and medialaccess, withstatisticalpowerof80%and5%significancelevel.
Thequantitativevariableswerepresentedasmeansand standarddeviations(SD).Thequalitativevariableswere pre-sented asabsolute frequencies. All significant values were presented as two-tailed. The significance level was set at
p<0.05.
Todeterminewhether thedatafollowedastandard nor-maldistribution,theKolmogorov-Smirnovtestwasused.The means ofthequantitativevariableswerecomparedby Stu-dent’st-testforindependentsamples,whentheparametric conditionsweremet,orbytheMann–Whitneytest,whenthe variabledidnotpresentnormaldistribution.Thefrequencies ofthequalitativevariableswerecomparedbyPearson’s chi-squaredtestorFisher’sexacttest.
The statistical analyses were performed with IBM SPSS Statistics(Version22.0.Armonk,NY:IBMCorp.).
Results
Allpatientsinvitedagreedtoparticipateandsignedthe con-sentform.Allpatientscompletedthefollow-up(Fig.3).
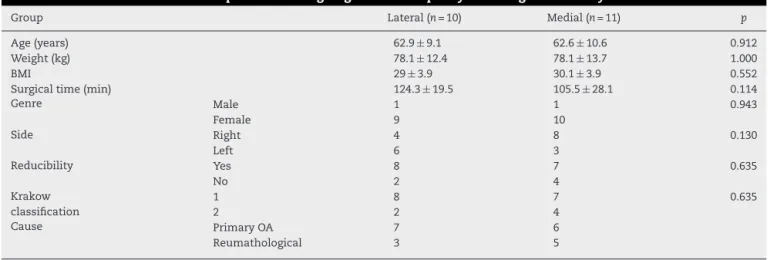
The analysis ofclinical data ofpatients in this sample (n=21)demonstratedthattherandomallocationprocesswas efficientinthecreationoftwohomogeneousgroups,withno differencesinothervariables,suchasage,weight,bodymass index (BMI), gender, operated side,cause ofthe deformity, magnitudeofthedeformity,passivereducibilityofthe defor-mitywithstressmaneuverinvarus,surgicaltime,andKrakow classificationforosteoarthritiswithvalgusdeformity(Table1). Themeanvalgusdeformitybeforesurgery,measuredbythe intersectionoftheanatomicalaxesofthefemurandtibiain thefrontalplane,was18.7degrees±7.2SDinthelateralgroup and25.7degrees±12.8SDinthemedialgroup(p=0.197).
Fig.2–Illustrationofthemethodusedtomeasurepatellartiltontheradiograph.A:normaltilt;B:increasedlateraltilt.
SDinthelateralgroupand,inthemedialgroup,34.4±15.3SD (p=0.605);themeanfunctionalKSSwas42.5±18.6SDinthe lateralgroupand49.6±19.2SDinthemedialgroup(p=0.468); themeanKujalascoreinthelateralgroupwas40.9±7.5SD andinthemedialgroup,39.1±9.7SD(p=0.557).
Asubjectiveevaluationofthesurgicalwoundoneweek aftersurgeryshowednodifferencebetweengroups.Inthe lat-eralgroup,sixpatientspresentedwoundsasexpected;three, betterthan expected;andone,worsethanexpected.Inthe medialgroup,sevenpatientspresentedwoundsasexpected; two, better than expected; and two, worse than expected (p=0.754).
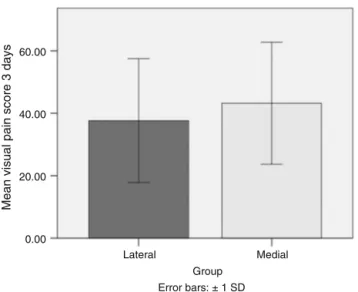
Postoperativepainwaslowerinthelateralgroup(Fig.4), butitwasnotpossibletodemonstrateastatistically signifi-cantdifference(p=0.705),asthesamplesizewasinsufficient (power=25%).Itwouldtake32subjectsineachgrouptofind adifferencebetweenthemeansof10points.
Bleeding,estimatedbythedecreaseinserumhemoglobin levels,wasverysimilarbetweengroups(Fig.5).
Themost important finding of this study was that the lateral patellar tilt in the lateral access group was lower (p=0.02;Fig.6).
Discussion
This study compared the medial and lateral access routes to total primary arthroplasty in valgus knees. The main resultwasthemoreefficientcorrectionoftheaxialpatellar tilt observedinthe groupwho underwent surgerythrough Keblish’s parapatellar lateral access route. This isthe first prospective,randomizedclinicaltrialcomparingthese tech-niques that includes the assessment of the postoperative correctionofthepatellartilt.
Theparapatellarlateralarthrotomywasproposedin1991 by Keblish2 as an option to the classic medial
parapatel-lar arthrotomy in cases of osteoarthritis of the knee with valgus deformity. This approachallows for adirect access to the lateral knee structures, which are generally those thatarestrainedandrequirerelease.17However,thelateral
accessrouteisnotusedbymostsurgeons,probablydueto their unfamiliarity with the procedure, which can lead to technical difficulties and increased surgical time. Another concernisthedifficultyofexposureandsofttissuecoverageat closing.18
Table1–Clinicalcharacteristicsofpatientsundergoingkneearthroplastywithvalgusdeformity.
Group Lateral(n=10) Medial(n=11) p
Age(years) 62.9±9.1 62.6±10.6 0.912
Weight(kg) 78.1±12.4 78.1±13.7 1.000
BMI 29±3.9 30.1±3.9 0.552
Surgicaltime(min) 124.3±19.5 105.5±28.1 0.114
Genre Male 1 1 0.943
Female 9 10
Side Right 4 8 0.130
Left 6 3
Reducibility Yes 8 7 0.635
No 2 4
Krakow classification
1 8 7 0.635
2 2 4
Cause PrimaryOA 7 6
Reumathological 3 5
Recruitment
Elegibility (n=21)
Exclusion (n=0)
Allocation
Follow-up
Analysis
Analyzed (n=10) Excluded from analysis (n=0)
Analyzed (n=11) Excluded from analysis (n=0)
Loss to follow-up (n=0) Loss to follow-up (n=0)
Random distribution (n=21)
Medial group (n=11) Lateral group (n=10)
Underwent intervention as allocated (n=10)
Underwent intervention as allocated (n=11)
Fig.3–Flowdiagram–ConsolidatedStandardsof
ReportingTrials(Consort).
Toovercome thedifficulty ofexposure oreven toavoid acatastrophictearingofthepatellartendon,someauthors recommendtheroutineassociationofosteotomyofthe ante-rior tibial tuberosity (ATT) to the lateral approach.2,19 ATT
osteotomy,however,canbeafactorforincreased complica-tionsandriskofrevisionsurgery,10,20anditwasnotnecessary
inthecasesoperatedinthepresentstudy.
Theliteratureshowssimilarresultsbetweenthetwo tech-niques in relation to the post-operative alignment in the coronalplane.17,21,22Somestudiespointtoabetter
postopera-tiverangeofmotionusingthelateralapproach.21,23Another
advantageisthepossibilityofusingcommonimplants (non-constricted), while the knee valgus operated using medial
60.00
40.00
Mean visual pain score 3 days
20.00
0.00
Lateral Medial
Group Error bars: ± 1 SD
Fig.4–Bargraphcomparingthemeanvisualpainscore.
Lateralgroup=37.66±19.8SD;medialgroup=43.22±19.5
SD;p=0.705.
6.0
5.0
4.0
Mean Hb difference
3.0
2.0
1.0
.0
Lateral Medial
Group
Error bars: ± 1 SD
Fig.5–Bargraphcomparingthemeanbloodloss
estimatedbythedifferenceinhemoglobinserumlevels
beforeandaftersurgery.
Lateralgroup=4.29±0.88;medialgroup=4.13±1.87;
p=0.512.
accessroutetendstomoreoftenrequireimplantswithlarger constriction.22Furthermore,amajoradvantageofthelateral
approachover themedialistoavoidopeningboth retinac-ula ofthe patella,sincemanycasesofvalgusknee require releaseofthelateralretinaculumtocorrectthecourseofthe patella.Lateralreleaseafteramedialparapatellarapproachis notdesired,duetotheriskofdevascularizationofthepatella andpatellartendon.
Patellofemoralinstabilityisamajorcauseofpainand func-tional limitation in the postoperative period of total knee prosthesisimplantation,and canevenleadtothe needfor
220
210
200
Patellar tilt 190
180
170
Lateral Medial
Group
Fig.6–Boxdiagramcomparingthemeanlateralpatellar
tiltafterarthroplasty.
Valuesabove180degreesindicatealateraltilt;below180
degrees,medialtilt.
Lateralgroup=183.1±5.3SD;medialgroup=198±10.2SD;
revisionsurgery.24,25 The lateralapproach hasbeen proven
tomoreeasilyfixpatellartiltinpatientswithosteoarthritis invalgus,whogenerallypresentretractionandevenlateral subluxationofthe patella. Thepresent study, evenwith a smallnumberofcases,demonstratedabettercorrectionof thepatellartiltinpatientswhounderwentsurgerythrough thelateralapproach.Theauthorswillcontinuethestudyto assesswhetherthisdifferenceinpatellartiltwillresultina clinicalbenefit,whichwillbeevaluatedbyKSS,WOMAC,and Kujalascores.
Althoughatrendwasobserved,therewasnodifference betweengroupsregardingbleedingandpainintheimmediate postoperativeperiod,aswellasinthecomparisonbetweenthe clinicalappearanceofthewoundinthefirstdaysafterthe pro-cedure.However,theauthorsbelievethatthereisatype2error duetothestillinsufficientnumberofpatientsfortheseother variables,whichwillbecorrectedasthestudyprogresses.In theory,anincisiononjustthelateralretinaculumshouldhurt andbleedless.Theeaseofexposureandlowerneedfortissue releasemayalsofavoralowertraumatothesofttissue,with betterwoundaspect.
Thepresentstudyhadsomelimitations.Firstly,thiswasa pilotstudywithasmallnumberofpatients.Nonetheless,very interestingresultsregardingthecorrectionofthepatellatilt wereobserved.Secondly,thereisnostandardnormalvalue forthe angle between the patella and the trochlea of the knee prosthesis. Theauthors believe that the components mustbeparallel.Thirdly,thisstudyusedradiographyto mea-surethepatellartilt.Despitebeingamethoddescribedinthe literature,11theauthorsconsidercomputedtomographytobe
theidealmethod,whichwillbeusedinthecontinuationof thestudy.
Conclusion
The lateral patellar tilt was lower in arthroplasties per-formed using Keblish’s lateral access route in knees with valgusdeformity. Thecontinuation of this controlled clin-ical trial, with increasing number of cases and increased follow-up time, will demonstrate whether this finding has anyimpactontheclinicalandfunctionaloutcomesofthese arthroplasties.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. RanawatAS,RanawatCS,ElkusM,RasquinhaVJ,RossiR, BabhulkarS.Totalkneearthroplastyforseverevalgus deformity.JBoneJointSurgAm.2005;87Suppl.1:271–84.
2. KeblishPA.Thelateralapproachtothevalgusknee.Surgical techniqueandanalysisof53caseswithovertwo-year follow-upevaluation.ClinOrthopRelatRes.1991;(271):52–62.
3. KrackowKA,JonesMM,TeenySM,HungerfordDS.Primary totalkneearthroplastyinpatientswithfixedvalgus deformity.ClinOrthopRelatRes.1991;(273):9–18.
4.SternSH,MoeckelBH,InsallJN.Totalkneearthroplastyin valgusknees.ClinOrthopRelatRes.1991;(273):5–8.
5.ElkusM,RanawatCS,RasquinhaVJ,BabhulkarS,RossiR, RanawatAS.Totalkneearthroplastyforseverevalgus deformity.Fivetofourteen-yearfollow-up.JBoneJointSurg Am.2004;86(12):2671–6.
6.WhitesideLA.Selectiveligamentreleaseintotalknee arthroplastyofthekneeinvalgus.ClinOrthopRelatRes. 1999;(367):130–40.
7.EnghGA.Thedifficultknee:severevarusandvalgus.Clin OrthopRelatRes.2003;(416):58–63.
8.SatishBR,GanesanJC,ChandranP,BasanagoudarPL, BalachandarD.Efficacyandmidtermresultsoflateral parapatellarapproachwithouttibialtubercleosteotomyfor primarytotalkneearthroplastyinfixedvalgusknees.J Arthroplasty.2013;28(10):1751–6.
9.KeblishPA.Alternatesurgicalapproachesinmobile-bearing totalkneearthroplasty.Orthopedics.2002;252Suppl.:s257–64.
10.HirschmannMT,HoffmannM,KrauseR,JenabzadehRA, ArnoldMP,FriederichNF.Anterolateralapproachwithtibial tubercleosteotomyversusstandardmedialapproachfor primarytotalkneearthroplasty:doesitmatter?BMC MusculoskeletDisord.2010;11:167.
11.CarlssonAM.Assessmentofchronicpain.I.Aspectsofthe reliabilityandvalidityofthevisualanaloguescale.Pain. 1983;16(1):87–101.
12.InsallJN,DorrLD,ScottRD,ScottWN.RationaleoftheKnee Societyclinicalratingsystem.ClinOrthopRelatRes. 1989;(248):13–4.
13.FernandesMI[Dissertac¸ão]Traduc¸ãoevalidac¸ãodo questionáriodequalidadedevidaespecíficopara
osteoartroseWomac(WesternOntarioMcMasterUniversities) paraalínguaportuguesa.SãoPaulo:EscolaPaulistade Medicina,UniversidadeFederaldeSãoPaulo;2003.
14.KujalaUM,JaakkolaLH,KoskinenSK,TaimelaS,HurmeM, NelimarkkaO.Scoringofpatellofemoraldisorders. Arthroscopy.1993;9(2):159–63.
15.SpecognaAV,BirminghamTB,HuntMA,JonesIC,JenkynTR, FowlerPJ,etal.Radiographicmeasuresofkneealignmentin patientswithvarusgonarthrosis:effectofweightbearing statusandassociationswithdynamicjointload.AmJSports Med.2007;35(1):65–70.
16.GomesLS,BechtoldJE,GustiloRB.Patellarprosthesis positioningintotalkneearthroplasty.Aroentgenographic study.ClinOrthopRelatRes.1988;(236):72–81.
17.GunstS,VillaV,MagnussenR,ServienE,LustigS,NeyretP. Equivalentresultsofmedialandlateralparapatellar approachfortotalkneearthroplastyinmildvalgus deformities.IntOrthop.2016;40(5):945–51.
18.FiddianNJ,BlakewayC,KumarA.Replacementarthroplasty ofthevalgusknee.Amodifiedlateralcapsularapproachwith repositioningofvastuslateralis.JBoneJointSurgBr. 1998;80(5):859–61.
19.BuechelFF.Asequentialthree-steplateralreleasefor correctingfixedvalguskneedeformitiesduringtotalknee arthroplasty.ClinOrthopRelatRes.1990;(260):170–5.
20.PiedadeSR,PinaroliA,ServienE,NeyretP.Tibialtubercle osteotomyinprimarytotalkneearthroplasty:asafe procedureornot?Knee.2008;15(6):439–46.
21.SekiyaH,TakatokuK,TakadaH,SugimotoN,HoshinoY. Lateralapproachisadvantageousintotalkneearthroplasty forvalgusdeformedknee.EurJOrthopSurgTraumatol. 2014;24(1):111–5.
22.RawalJ,DevanyAJ,JefferyJA.Arthroplastyinthevalgusknee: comparisonanddiscussionoflateralvs.medialparapatellar approachesandimplantselection.OpenOrthopJ.2015;9:94–7.
treatmentofnon-correctablevalguskneeosteoarthritis:a retrospectiveclinicalstudy.Knee.2014;21(1):204–8.
24.MaloM,VinceKG.Theunstablepatellaaftertotalknee arthroplasty:etiology,prevention,andmanagement.JAm AcadOrthopSurg.2003;11(5):364–71.