www.jped.com.br
ORIGINAL
ARTICLE
Febrile
seizures:
a
population-based
study
夽
Juliane
S.
Dalbem
a,b,∗,
Heloise
H.
Siqueira
b,
Mariano
M.
Espinosa
b,
Regina
P.
Alvarenga
aaPost-GraduatePrograminNeurology,UniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil bUniversidadeFederaldeMatoGrosso(UFMT),Cuiabá,MT,Brazil
Received22September2014;accepted23January2015 Availableonline26May2015
KEYWORDS
Prevalence; Febrileseizure; EpidemiologyAbstract
Objectives: Todeterminetheprevalenceofbenignfebrileseizuresofchildhoodanddescribe theclinicalandepidemiologicalprofileofthispopulation.
Methods: Thiswasapopulation-based,cross-sectionalstudy,carriedoutinthecityofBarra doBugres,MT,Brazil,fromAugust2012toAugust2013.Datawerecollectedintwophases. Inthefirstphase,aquestionnairethatwaspreviouslyvalidatedinanotherBrazilianstudywas usedtoidentifysuspectedcasesofseizures.Inthesecondphase,aneurologicalevaluationwas performedtoconfirmdiagnosis.
Results: Theprevalencewas6.4/1000inhabitants(95%CI:3.8---10.1).Therewasnodifference between genders.Simple febrileseizureswere foundin88.8% ofcases.A familyhistoryof febrileseizuresinfirst-degreerelativesandhistoryofepilepsywaspresentin33.3%and11.1% ofpatients,respectively.
Conclusions: TheprevalenceoffebrileseizuresinMidwesternBrazilwaslowerthanthatfound inotherBrazilian regions,probablyduetotheinclusiononlyoffebrileseizureswithmotor manifestationsanddifferencesinsocioeconomicfactorsamongtheevaluatedareas.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Prevalência; Crisefebril; EpidemiologiaConvulsãofebril:estudodebasepopulacional
Resumo
Objetivos: Estabeleceraprevalênciadascrisesfebrisedescreveroperfilclínicoe epidemi-ológicodessapopulac¸ão.
Métodos: EstudotransversaldebasepopulacionalrealizadonacidadedeBarradoBugres(MT), noperíododeagostode2012aagostode2013.Osdadosforamcoletadosemduasetapas.Na primeirafaseutilizamosumquestionáriovalidadopreviamenteemoutroestudobrasileiro,para identificac¸ãodecasossuspeitosdecrisesepilépticas.Nasegundaetaparealizamosaavaliac¸ão neuroclínicaparaconfirmac¸ãodiagnóstica.
夽 Pleasecitethisarticleas:DalbemJS,SiqueiraHH,EspinosaMM,AlvarengaRP.Febrileseizures:apopulation-basedstudy.JPediatr
(RioJ).2015;91:529---34.
∗Correspondingauthor.
E-mail:[email protected](J.S.Dalbem). http://dx.doi.org/10.1016/j.jped.2015.01.005
Resultados: A prevalência decrisefebril foide 6,4/1000habitantes (IC95%3,8;10,1).Não houvediferenc¸aentreossexos.Ascrisesfebrissimplesforamencontradasem88,8%doscasos. Ahistóriafamiliardecrisefebrileepilepsiaemparentesde1◦grauestevepresenteem33,3%
e11,1%dospacientes,respectivamente.
Conclusões: Aprevalênciadacrisefebrilnaregiãocentro-oestefoimenordoqueaencontrada emoutrasregiõesbrasileiras,provavelmenterelacionadoàinclusãoapenasdascrisesfebriscom manifestac¸õesmotoraseasdiferenc¸asdefatoressocioeconômicosentreasregiõespesquisadas. ©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Febrile seizures are the most common seizures in chil-drenyoungerthan5years,affecting2---5%ofthepediatric population1; they are considered to be benign and
self-limited,2 andareclassifiedassimpleandcomplex.1Upper
airway viral infections are the most common triggering factors.3,4 The risk of subsequently developing epilepsyis
6.9%5;althoughtheyhaveanexcellentprognosis,theybring
anxietytoparentsandfamilymembers.6
The clinical signs of febrile seizures are not different amongpopulations,buttheclinicalanddemographic char-acteristics are not identical in the different parts of the world,7 thus justifying the necessity ofthe present study.
Thereis noBrazilianstudy that hasdescribed theclinical andepidemiologicalcharacteristicsofpatientswithfebrile seizures.
This study aimed to determine the prevalence and describetheclinicalandepidemiologicalcharacteristicsof patientswithfebrileseizures.
Methods
Study
site
and
assessed
population
The study was conducted in the municipality of Barra do Bugres,state ofMato Grosso,Brazil,fromAugust 2012 to August2013.Theestimatedpopulationin2013was33,022 inhabitants,8 with 3445 inhabitants aged between 0 and
5 years and 11 months, of whom 1775 were males and 1670females.8 Approximately 60% of thepopulation is of
Africandescent.Inthemunicipality,77%ofthehouseholds have sewerage and 55% have water supply services. The HumanDevelopmentIndexofthemunicipalityis0.693and theper capitaincome, basedthe GrossDomestic Product (GDP)of2012 wasUS$6740.00.8 The municipality hassix
healthcare teams working for the Family Health Program (FHP)andforty-sixhealthcareworkersattendingto75%of thepopulation; thepopulation that isnot assisted bythe FHP receives health care in a Basic Health Unit located downtown.ThefactthatthemunicipalityhasgoodFHP cov-erageandthattheprogramworksregularlyfacilitatedthis study.
Study
phases
This was a cross-sectional, population-based study, per-formed in two phases. In the first phase, the healthcare workersperformedanactivesearchatthehouseholds, seek-ingsuspectedcasesofseizures.Aquestionnairewitheight questionswasused(Table1).Thequestionsweremodified fromthe guidelinesof theWorld HealthOrganization and aresimilarto thequestions usedin epidemiological stud-iesconductedinEcuador,9andwerepreviouslyvalidatedin
aBrazilianstudywithasensitivityof95.8%andspecificity of 97.8%.10 This screening questionnaire wasalso used in
aprevalencestudyofepilepsyinchildhoodinthestate of SãoPaulo.11Thehealthcareworkerswerepreviouslytrained
andreceivedexplanationsonseizures/epilepsyandhowto applythe questionnaire. The casesin which therewasat leastoneaffirmativeresponsetotheeightquestionswere referredtothesecond phaseoftheevaluation(diagnostic confirmation), whenthe clinical historywasobtained and theneurologicalexaminationwasperformed.
This study was approved by the Ethics Committee of Hospital Geral Universitário (Registered under n.128 CEP/UNIC---protocoln.2011-128).
Inclusion
and
exclusion
criteria
Children witha history of at least oneepisode of febrile seizureresidinginBarradoBugresandaged0---5yearswere includedinthestudy.Patientswhoseconditiondidnotfitthe definitionoffebrileseizureswereexcluded.Febrileseizures withoutmotorsymptomswerenotconsidered,duethe dif-ficulty in ascertaining whether theywere really epileptic seizuresaccordingtothedescriptionofthefamilymembers.
Definitions
Febrileseizuresweredefinedasseizuresoccurringin chil-drenolderthan1monthandyoungerthan5yearsassociated withfebrile illness. This definition excluded seizures that occurredinthepresenceofcentralnervoussysteminfection or caseswithahistory ofepileptic seizures inthe neona-tal period, unprovoked seizures, and acute symptomatic seizures.12 Febrile seizures can be classified as simple or
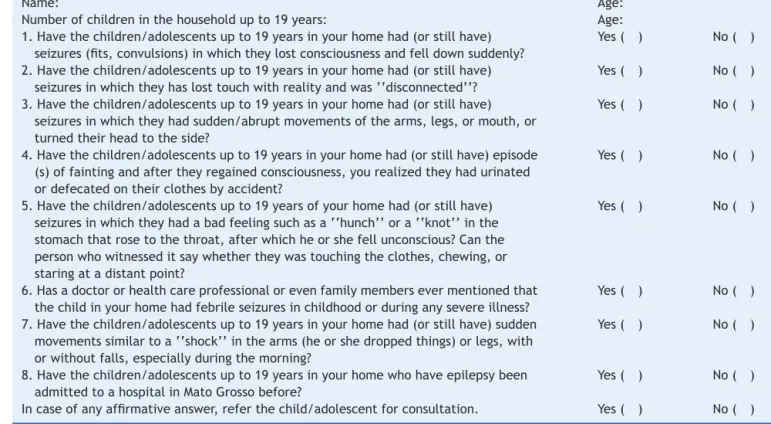
Table1 Screeningquestionnaire.10
Name: Age:
Numberofchildreninthehouseholdupto19years: Age:
1.Havethechildren/adolescentsupto19yearsinyourhomehad(orstillhave) seizures(fits,convulsions)inwhichtheylostconsciousnessandfelldownsuddenly?
Yes( ) No( )
2.Havethechildren/adolescentsupto19yearsinyourhomehad(orstillhave) seizuresinwhichtheyhaslosttouchwithrealityandwas‘‘disconnected’’?
Yes( ) No( )
3.Havethechildren/adolescentsupto19yearsinyourhomehad(orstillhave) seizuresinwhichtheyhadsudden/abruptmovementsofthearms,legs,ormouth,or turnedtheirheadtotheside?
Yes( ) No( )
4.Havethechildren/adolescentsupto19yearsinyourhomehad(orstillhave)episode (s)offaintingandaftertheyregainedconsciousness,yourealizedtheyhadurinated ordefecatedontheirclothesbyaccident?
Yes( ) No( )
5.Havethechildren/adolescentsupto19yearsofyourhomehad(orstillhave) seizuresinwhichtheyhadabadfeelingsuchasa‘‘hunch’’ora‘‘knot’’inthe stomachthatrosetothethroat,afterwhichheorshefellunconscious?Canthe personwhowitnesseditsaywhethertheywastouchingtheclothes,chewing,or staringatadistantpoint?
Yes( ) No( )
6.Hasadoctororhealthcareprofessionalorevenfamilymembersevermentionedthat thechildinyourhomehadfebrileseizuresinchildhoodorduringanysevereillness?
Yes( ) No( )
7.Havethechildren/adolescentsupto19yearsinyourhomehad(orstillhave)sudden movementssimilartoa‘‘shock’’inthearms(heorshedroppedthings)orlegs,with orwithoutfalls,especiallyduringthemorning?
Yes( ) No( )
8.Havethechildren/adolescentsupto19yearsinyourhomewhohaveepilepsybeen admittedtoahospitalinMatoGrossobefore?
Yes( ) No( )
Incaseofanyaffirmativeanswer,referthechild/adolescentforconsultation. Yes( ) No( )
complex seizures are focal, last longer than 15min, and showrecurrencewithin24h.1
Data
processing
and
statistical
analysis
Thedatacollectedduringtheinterviewinpre-coded ques-tionnaireswereprocessedinapersonalcomputer,typedin duplicatetoreducetypos,inan electronicdatabaseusing Excel(Microsoft2003.MicrosoftExcel[computersoftware]. Redmond,Washington,USA).When inconsistentdatawere found,theywereverifiedintheoriginalquestionnaireand thenecessarycorrectionswereperformed.Datawere ana-lyzeddescriptively,and95%confidenceintervalswerebuilt for theirrespectiveprevalencein theinferentialanalysis. Thistechniquewasusedbecausethecomparison measure-mentscalewascategoricalornon-quantitative.
Results
ThemunicipalityofBarradoBugreshasapopulationof3445 inhabitantsattheagerangeof0---5yearsand11months;a totalof2811inhabitants(81.6%)werescreened.Thelosses inthefirstphaseofthestudyoccurredbecauseitwasnot possibletofindresidentsinthehouseholdsinmorethanone visitbythe healthcareworkers.The prevalenceoffebrile seizuresinthissample was6.40/1000inhabitants (95%CI: 3.8---10.10).Theageatthefirstseizurerangedfrom1month to60months(meanof19.38months).Clinicaland sociode-mographicvariablesareshowninTable2.
Discussion
The prevalence of febrile seizures in this sample was 6.4/1000 inhabitants; in the literature, it ranges from 3.5/100013to17/1000.14TwoBrazilianstudiesassessedthe
prevalenceoffebrileseizures,showingarateof13.9/1000 inSãoPaulo,SP,Braziland16/1000inPelotas,RS,Brazil.11,15
Intheassessed area,it wasobservedthat theprevalence was lower than that found in the South and Southeast regionsofBrazil.Thesedifferencesinprevalenceratesmay be justified by different methodologies used for patient recruitment,socioeconomic factors,andparticularities of the populationsfrom each region studied. In the present study, active search in households was used for patient recruitment,with18.4%oflossesinthisagegroup.
When comparingwith the study conducted in Pelotas, RS,Brazil,whichusedabirthcohort,thelossesconsistedof 26.2%individualsthatcouldnotbeassessed,thereby indi-catingalargerpopulationanalysisinthepresentstudy.The studyconductedinSãoPaulo,SP,Brazilusedaconvenience sampletoassessindividualstreatedatComplexoEinsteinin theParaisópoliscommunity,thuscreatingabiasthatcould justifyahigherprevalenceinthatstudy.
Table2 Observedfrequencydistribution,percentage,and95%CIof18patientswithfebrileseizuresaccordingtoclinicaland sociodemographicvariables.BarradoBugres,MT,Brazil,2014.
Variable Observedfrequency(n) Percentage(%) 95%CI
Gender
Male 9 50.00 (26.02---73.98)
Female 9 50.00 (26.02---73.98)
Ethnicity
White 7 38.89 (17.30---64.25)
Non-white 11 61.11 (35.74---82.70)
Numberofseizureepisodes
Singleepisode 16 88.89 (65.29---98.62)
Twoepisodes 1 5.56 (0.14---27.29)
Threeepisodes 1 5.56 (0.14---27.29)
Antiepilepticdrugused
Phenobarbital 2 11.11 (1.38---34.71)
Valproate 3 16.67 (3.58---41.42)
None 13 72.22 (46.52---90.30)
Typeofseizure
Generalized 16 88.89 (65.29---98.62)
Focal 2 11.11 (1.38---34.71)
Riskofmiscarriageinpregnancy
Yes 2 11.11 (1.38---34.71)
No 16 88.89 (65.29---98.62)
Receivedprenatalcare(>sixconsultations)
Yes 18 100
---Typeofdelivery
Vaginal 9 50.00 (26.02---73.98)
Cesariansection 9 50.00 (26.02---73.98)
Gestationalage
Full-term 17 94.44 (72.71---99.86)
Preterm 1 5.56
Birthweight
2000g≤weight<2500g 2 11.11 (1.38---34.71)
2500g≤weight≤3000g 5 27.78 (9.70---53.48)
Weight>3000g 11 61.11 (35.74---82.70)
Apgar>7
Yes 18 100
---Neonatalcomplication(infection)
Yes 2 11.11 (1.38---34.71)
No 16 88.89 (65.29---98.62)
Neuropsychomotordevelopment
Normal 18 100
---Familyhistoryofepilepsy
Yes 2 11.11 (1.38---34.71)
No 16 88.89 (65.29---98.62)
Familyhistoryoffebrileseizure
Yes 6 33.33 (13.34---59.01)
No 12 66.67
Consanguinity
---Table2 (Continued)
Variable Observedfrequency(n) Percentage(%) 95%CI
Paternallevelofschooling
IncompleteElementarySchool 9 50.00 (26.02---73.98)
CompleteElementarySchool 3 16.67 (3.58---41.42)
IncompleteHighSchool 1 5.56 (0.14---27.29)
CompleteHighSchool 4 22.22 (6.41---47.64)
College/University 1 5.56 (0.14---27.29)
Maternallevelofschooling
IncompleteElementarySchool 8 44.44
CompleteElementarySchool 2 11.11 (1.38---34.71)
IncompleteHighSchool 2 11.11 (1.38---34.71)
CompleteHighSchool 5 27.78 (9.69---53.48)
College/University 1 5.56 (0.14---27.29)
Familyincome
1MW 7 38.89 (17.30---64.25)
Between1and2MWs 1 5.56 (0.14---27.29)
2MW 6 33.33 (13.34---59.01)
>3MW 4 22.22 (6.41---47.64)
MW,Brazilianminimumwage;95%CI,95%confidenceinterval.
veryparticular,reflectingthemiscegenationobservedinthis country.ThisisdifferentfromotherBrazilianregions,where thepopulationismorehomogeneous,indicatingthatBarra doBugresbearsmoreresemblancetothegeneralBrazilian populationprofile. Inthisstudy,onlyfebrile seizureswith motormanifestationswereincluded.This,togetherwiththe abovementionedfactors,mayexplainthelowerprevalence foundinthepresentstudy.
Studieshaveshownavariationinsimplefebrileseizure prevalencerangingfrom55.2%to85.6%16,17;inthepresent
study,this proportionwas88.8%, similartothat reported in Tunisia, Turkey, Cameroon, India, China, Iran, and
England.16---23Statusepilepticussecondarytofebrileseizure
wasnotobservedinthepresentstudy,unliketheone con-ductedinCameroon,whichidentifieditin10%ofcases.24
Whenanalyzingthefrequencyoffebrileseizuresin rela-tiontogender, nodifferencewasobserved,similartothe research by Pavlovic et al.25 differing from some studies
in which theauthors described a higher frequency in the malegender,7,16,19,26 whereasonly Sillanpääetal.found a
predominanceinthefemalegender.27
The family history of febrile seizures and epilepsy in first-degreerelatives wasfound respectively in 33.3%and 11.1%ofcases.Studieshaveshownavariationfrom14.7%
Table3 Characteristicsassessedinthemainstudiesonfebrileseizures.
Author/year Country Patient recruitment
Meanageat firstseizure (months)
Prevalence/ 1000
Male gender
Familyhistory offebrile
seizure
Family historyof
epilepsy
Simple febrile seizure
Sampaio,201011 Brazil Cross-sectional
(activesearch)
13.9
Nunes,201115 Brazil Cohort 16
AlRajeh,200113 SaudiArabia Cross-sectional
(activesearch)
3.55
Sfaihi,201216 Tunisia Hospitalfiles 58.7% 14.7% 5.6% 55.2%
Nguefack,201018 Cameroon Hospitalfiles 24.6 36.4% 58.7%
Yakinci,200017 Turkey Cross-sectional 23.0 3.24 37.28% 12.71% 85.6%
Banerjee,200919 India Cross-sectional
(activesearch)
1.11 84.7%
Chung,200620 China Hospitalfiles 25 17.5%
Fallah,201021 Iran Hospitalfiles 24 67%
Verity,198522 England Cohort 24 16.2% 7.5% 76.9%
Sillanpää,200827 Finland Cohort
Aydin,200828 Turkey
Cross-sectional, schoolchildren
to39.3%16,17,19,20,22---24,28inrelationtofamilyhistoryoffebrile
seizuresandfrom2.7%to12.71%16,17,20,24regardingepilepsy.
Familyincomewasuptotwominimumwagesin77.7% ofcases.Studieshaveshownthattheprevalenceoffebrile seizuresisnotassociatedwithsocialclassandparentallevel ofschooling.22,23Table3showsasummaryofthemain
varia-blesin articles publishedtodate, demonstratingthe lack of data regarding the pre- and perinatal periods and the heterogeneityofthestudiedvariables,whichhindersdata comparisonandthedevelopmentofmeta-analysesrelated tothesubject.
It can be concluded that the prevalence of febrile seizuresin the Midwestregionwaslower thanthat found in other Brazilian regions, probably due to the inclusion only of febrile seizures withmotor manifestations and to thesocioeconomicdifferencesamongtheassessedregions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorswouldliketothanktheHealthSecretariatofthe municipalityofBarradoBugres,theFamilyHealthProgram, andthetechnical-administrativeteamofCentro deSaúde doMaracanãwhosparednoeffortstoconductthisresearch.
References
1.SubcommitteeonFebrileSeizures;AmericanAcademyof Pedi-atrics. Neurodiagnosticevaluationofthechildwithasimple febrileseizure.Pediatrics.2011;127:389---94.
2.PattersonJL,Carapetian SA,HagemanJR,KelleyKR. Febrile seizures.PediatrAnn.2013;42:249---54.
3.Kaputu KalalaMalu C,Mafuta Musalu E,Dubru JM,Leroy P, TomatAM,MissonJP.Epidemiologyandcharacteristicsoffebrile seizuresinchildren.RevMedLiege.2013;68:180---5.
4.Abuekteish F, Daoud AS, Al-Sheyyab M, Nou’man M. Demo-graphiccharacteristicsandriskfactorsoffirstfebrileseizures: aJordanianexperience.TropDoct.2000;30:25---7.
5.LeungAK,RobsonWL.Febrileseizures.JPediatrHealthCare. 2007;21:250---5.
6.VestergaardM,PedersenCB,SideniusP,OlsenJ,ChristensenJ. Thelong-termriskofepilepsyafterfebrileseizuresin suscep-tiblesubgroups.AmJEpidemiol.2007;165:911---8.
7.ShimonyA,AfawiZ,AsherT,MahajnahM,ShorerZ. Epidemio-logicalcharacteristicsoffebrileseizures---comparingbetween Bedouin and Jews in the southern part of Israel. Seizure. 2009;18:26---9.
8.InstitutoBrasileirodeGeografiaeEstatística(IBGE)[cited15 out2013].Availablefrom:http://www.cidades.ibge.gov.br 9.Placencia M, Sander JW, Shorvon SD, Ellison RH, Cascante
SM. Validation of a screening questionnaire for the detec-tion of epileptic seizures in epidemiological studies. Brain. 1992;115:783---94.
10.BorgesMA,Min LL, Guerreiro CA,Yacubian EM,Cordeiro JA, TognolaWA,etal.Urbanprevalenceofepilepsy:populational studyinSãoJosédoRioPreto,amedium-sizedcityinBrazil. ArqNeuropsiquiatr.2004;62:199---204.
11.SampaioLP,CabocloLO, KuramotoK,RecheA,Yacubian EM, ManrezaML.PrevalenceofepilepsyinchildrenfromaBrazilian areaofhighdeprivation.PediatrNeurol.2010;42:111---7. 12.Guidelinesforepidemiologicstudiesonepilepsy.Commission
onEpidemiology and Prognosis,International League Against Epilepsy.Epilepsia.1993;34:592---6.
13.AlRajehS,AwadaA,BademosiO,OgunniyiA.Theprevalence ofepilepsyandotherseizuredisordersinanArabpopulation:a community-basedstudy.Seizure.2001;10:410---4.
14.BaumannRJ,MarxMB,LeonidakisMG.Epilepsyinrural Ken-tucky: prevalence in a population of school age children. Epilepsia.1978;19:75---80.
15.Nunes ML,Geib LT, Grupo Apego. Incidence ofepilepsy and seizuredisordersinchildhoodandassociationwithsocial deter-minants:abirthcohortstudy.JPediatr(RioJ).2011;87:50---6. 16.SfaihiL,MaaloulI,KmihaS,AloulouH,ChabchoubI,KamounT, etal.Febrileseizures:anepidemiologicalandoutcomestudy of482cases.ChildsNervSyst.2012;28:1779---84.
17.YakinciC,KutluNO,DurmazY,KarabiberH,E˘griM.Prevalence offebrileconvulsionin3637childrenofprimaryschoolagein theprovinceofMalatya,Turkey.JTropPediatr.2000;46:249---50. 18.NguefackS,NgoKanaCA,MahE,KuateTegueuC,ChiabiA,Fru F,etal.Clinical,etiological,andtherapeuticaspectsoffebrile convulsions.Areviewof325cases inYaoundé.Arch Pediatr. 2010;17:480---5.
19.BanerjeeTK,HazraA,BiswasA,RayJ,RoyT,RautDK,etal. Neurological disordersin children and adolescents. Indian J Pediatr.2009;76:139---46.
20.ChungB, Wat LC,WongV. Febrileseizures in southern Chi-nese children: incidence and recurrence. Pediatr Neurol. 2006;34:121---6.
21.FallahR,KarbasiSA.RecurrenceoffebrileseizureinYazd,Iran. TurkJPediatr.2010;52:618---22.
22.VerityCM,ButlerNR,GoldingJ.Febrileconvulsionsinanational cohort followed up from birth. I --- Prevalence and recur-rence inthe firstfive yearsof life. Br MedJ (ClinRes Ed). 1985;290:1307---10.
23.VerityCM,ButlerNR,GoldingJ.Febrileconvulsionsinanational cohortfollowedupfrombirth.II---Medicalhistoryand intel-lectual ability at 5 years of age. Br Med J (Clin Res Ed). 1985;290:1311---5.
24.GururajAK,BenerA, Al-SuweidiEK,Al-TatariHM,KhadirAE. Predictorsoffebrileseizure:amatchedcase---controlstudy.J TropPediatr.2001;47:361---2.
25.Pavlovic MV, Jarebinski MS, Pekmezovic TD, Marjanovic BD, LevicZM. Febrileconvulsions in a Serbianregion: a 10-year epidemiologicalstudy.EurJNeurol.1999;6:39---42.
26.FarwellJR,BlacknerG, SulzbacherS,Adelman L,Voeller M. Firstfebrileseizures.Characteristicsofthechild,theseizure, andtheillness.ClinPediatr(Phila).1994;33:263---7.
27.Sillanpää M, Camfield P, Camfield C, Haataja L, Aromaa M, Helenius H, et al. Incidence of febrile seizures in Fin-land: prospective population-based study. Pediatr Neurol. 2008;38:391---4.