www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Neonatal
hearing
screening
in
a
low-risk
maternity
hospital
in
São
Paulo
state
夽
,
夽夽
Adriana
Aparecida
Tahara
Kemp
a,∗,
Camila
Ribas
Delecrode
a,
Giovannna
César
da
Silva
a,
Fabiana
Martins
b,
Ana
Cláudia
Figueiredo
Frizzo
c,
Ana
Cláudia
Vieira
Cardoso
caHumanCommunicationDisorders,FaculdadedeFilosofiaeCiências(FFC),UniversidadeEstadualPaulista(UNESP),Marília,
SP,Brazil
bSecretariaMunicipaldeSaúdedeMarília,Marília,SP,Brazil
cSpeechTherapyDepartment,FaculdadedeFilosofiaeCiências(FFC),UniversidadeEstadualPaulista(UNESP),Marília,SP,Brazil
Received27March2014;accepted14October2014 Availableonline26July2015
KEYWORDS Audiology;
Neonatalscreening; Hearingtests
Abstract
Introduction:Theliteratureindicatesthatneonatalhearingscreeningshouldbeuniversal,so adescriptionofprogramsthatadoptthisrecommendationisrelevant.
Objective: Todescribetheresultsofnewbornhearingscreeningandtheprofileofmothersand newbornsattendedtoinalow-riskmaternitysetting,andtocorrelatethecharacteristicsof thispopulationwiththeresultsoftransientevokedotoacousticemissions.
Methods:Acontemporarycross-sectionalcohortstudy.Thesampleconsistedof670infantsand theprocedures performedwereaudiological history,transient-evoked otoacousticemissions (TEOAE),distortionproduct-evokedotoacousticemissions(DPEOAE),andautomated-brainstem auditoryevokedpotential(ABSAEP).
Results:Therateofsuccessinthisprogramwas98.5%,thefailureratewas0.62%,andthatof non-attendancetofinalizethediagnosticprocess,0.93%.Whencorrelatingthevariablesstudied with theresultsoftransientevoked otoacoustic emissions,therewasasignificant negative correlationonlyforageofinfant.
Conclusion: Theprogramofthismaternityhospitalwaseffectiveandcomplieswithnational and international recommendations. The population consisted of young mothers with few
夽 Pleasecitethisarticleas:KempAAT,DelecrodeCR,daSilvaGC,MartinsF,FrizzoACF,CardosoACV.Neonatalhearingscreeningina
low-riskmaternityhospitalinSãoPaulostate.BrazJOtorhinolaryngol.2015;81:505---13.
夽夽Institution:UniversidadeEstadualPaulista‘‘JúliodeMesquitaFilho’’,SchoolofPhilosophyandSciences,MaríliaCampus,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](A.A.T.Kemp).
http://dx.doi.org/10.1016/j.bjorl.2015.07.010
1808-8694/©2015Associac¸ãoBrasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.Published byElsevierEditoraLtda.Allrights
pregnancycomplicationsandhealthyinfants.Theonlyvariablethatinfluencedtransientevoked otoacousticemissionresults,afterhospitaldischarge,wastheageatwhichinfantswere eval-uated.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE Audiologia;
Triagemneonatal; Testesauditivos
Triagemauditivaneonatalemumamaternidadedebaixoriscodointeriorpaulista
Resumo
Introduc¸ão:Aliteraturarelataqueatriagemauditivaneonataldeveseruniversal,oquetorna relevanteadescric¸ãodeprogramasqueadotamestarecomendac¸ão.
Objetivo:Descreverosresultadosdatriagemauditivaneonataleoperfildasmãese recém-nascidosatendidosemumamaternidadedebaixoriscoecorrelacionarascaracterísticasdesta populac¸ãocomosresultadosdasemissõesotoacústicasevocadastransientes.
Método: Estudocoorte contemporâneo comcorte transversal. A amostra foi composta por 670bebêseosprocedimentosrealizadosforam:anamneseaudiológica,emissõesotoacústicas (EOA)transientes,EOAprodutodedistorc¸ão,epotencialevocadoauditivodetroncoencefálico automático.
Resultados: Oíndicedepassanesteprogramafoide98,5%;defalhade0,62%eodenão com-parecimentoparafinalizac¸ãodoprocessodiagnósticode0,93%.Aocorrelacionarasvariáveis estudadascomosresultados dasemissõesotoacústicastransientehouvecorrelac¸ãonegativa significanteapenasparaaidadedobebê.
Conclusão:O programa desta maternidade mostrou-se efetivo e atende a recomendac¸ões nacionaiseinternacionais.Apopulac¸ãofoi compostapormãesjovenscompoucas intercor-rênciasgestacionais ebebês saudáveis. A única variávelque influenciounosresultados das emissõesotoacústicasportransiente,apósaaltahospitalar,foiàidadeemqueosbebêsforam avaliados.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
TheUniversalNewbornHearingScreening (UNHS)program seeksearlydetectionofhearingloss,withtheaimof eval-uating the hearing ability of neonates with and without risk factors for hearing loss (RFHL). This process consists ofperformingbehavioral,electroacoustic,and/or electro-physiologicalprocedurestoidentifyhearingloss.1
Discussions about the importance and implementation of newborn hearing screening programs were initiated in the 1990s.In 2000, the Brazilian Speech Therapy Council issuedan opinion indicating the need toimplement hear-ingscreeningproceduresinneonatesusingsomeobjective methodology already described in the literature, such as recordingevokedotoacousticemissionsandbrainstem audi-toryevokedpotential(BAEP).2
Several local and state laws have been passed in this country, making completion of the UNHS compulsory in maternity wards. Of note is National Law No. 12,303 of August 2,2010, which determinesthe obligation tocarry outevokedotoacoustic emission testsin all hospitalsand maternitywardsinchildrenbornontheirpremises.3 How-ever,itisknownthatfewpublicmaternityfacilitiesruna systematicuniversalnewbornhearingscreeningprogram.4
Theliteraturereportsthatthemostwidely used meth-ods in newborn hearing screening programs are probably
the transient-evoked otoacoustic emission (T-EOAE) test in a first stage, and the auditory brainstem response in a second stage, for those infants who failed the T-EOAE test. The combination of both tests was designed toreduce thenumberoffalse-negative results,especially in cases of auditory neuropathy/dyssynchrony, in addi-tion to improving the sensitivity and specificity of UNHS results.5---17
InreviewingthestudiespublishedintheBrazilian litera-turedescribingcharacteristicsofnewbornhearingscreening programs, it is observed that most of them specify test results,gender,age,birthweight,andriskindicators.There havebeennumerousreportsofscreeningresultsaccording toriskindicators.18---28
Unlikearticles publishedin the literature, thepresent studyaimedtodescribeanewbornhearingscreening pro-gram in which the majority of treated newborns had no risk indicators for hearingloss,which woulddecrease the incidenceofhearinglossinthispopulation.Inaddition,it wasintended toexpand the description ofthe character-isticscommonlyreportedintheliteratureformothersand newborns.
Test T-EOAE 645 (100%)
Retest T-EOAE DP-EOAE
A-ABEP 26 Passed
615
Passed 4 (0.66%)
Passed 16 (2.68%)
Failed 10 (1.66%)
Did not come to test 6 (1.0%) Diagnosis
Conductive hearing loss
4 (0.66%) Presence of RFHL
Monitoring 44 (7%)
Presence of RFHL Monitoring
0 (0%)
Presence of RFHL Monitoring
3 (0.50%) Absence of RFHL
Otrientation/discharge 571 (88%)
Absence of RFHL Orientation/discharge
4 (0,66%)
Absence of RFHL Orientation/discharge
13 (2,18%)
DP-EOAE 30 (5%)
Failed 30 (5%)
Failed 26 (4.34%)
Figure 1 Flowchart. RFHL, risk factors for hearing loss; TEOAE,transient-evoked otoacoustic emissions;DPEOAE, distortion product-evokedotoacousticemissions;A-ABEP,automated-auditorybrainstememissionpotential.
characteristics ofthis populationwiththe resultsof tran-sientevokedotoacousticemissions.
Methods
Thiswasacontemporarycohortcross-sectionalstudy, per-formed in a maternity hospital in São Paulo State and approved by the Institution’sResearch Ethics Committee, underNo.0703/2013.
ThismaternitywardispartoftheUnifiedHealthSystem (SUS)andcaresforlow-riskpregnantwomen,withan aver-ageof1500birthsperyear.TheinstitutionispartofRede
Cegonha, a program developed by the Ministry of Health
thatofferhumanizedcarewiththefollowingobjectives:(1) implementationofanewmodel ofhealthcarefor women andchildren, withafocusondelivery,birth, growth,and development;(2)Organizationofmaternalandchildhealth services;and(3)reductionofmaternal andinfant mortal-ityintheneonatalperiod.Inadditiontothisprogram,this maternitywardhaspartnershipwiththeHumanMilkBank of the city of Marília, São Paulo, Brazil in order to edu-catemothersontheimportanceofexclusivebreastfeeding and addressing any problem relatedto breastfeeding and collection,storage,anddonationofbreastmilk.
Astothecompositionofthissample,thefollowing inclu-sionandexclusioncriteriawereused:signingtheinformed consent,screenings conducted in the periodfrom May to
Novemberof2013,andresponseofthemothersto anamne-sisdata.
Thus,thisstudy wasbased ondata from670 newborns attendedbythisneonatalhearingscreeningprogram.
To achieve this goal, the following procedures were used:anamnesis, meatoscopy, and hearing tests(T-EOAE, distortionproduct-evokedotoacousticemission[DP-EOAE], and automated-auditory brainstem emission potential [A-ABEP]).
Initially,anaudiologicalhistorywasobtained,basedon a questionnaire (Annex) consisting of identification data, questionsabout gestationalhistory,delivery,andnewborn data, such as: gender, age, gestational time (preterm or term),mother’sage,typeofdelivery(normalorcesarean), pregnancycomplications,baby’sbirthweight,typeof feed-ing,bottlefeedingand/orpacifieruse,andotherriskfactors for hearing loss,1 including phototherapy for hyperbiliru-binemia. It was decided in favor of the addition of this indicator,becauseofthehigh incidenceofhearing lossin childrenundergoingphototherapyinclinicalpractice.
Hearing procedures were divided intotwo stages: test andretest.Forthetest,T-EOAEwascarriedout;incaseof failureinthistest,DP-EOAEwasadded.Forretest,T-EOAE, DP-EOAE,andA-ABEPwereperformed.
Inthisprogram,thenewbornwasdischargedfrom hos-pitalandreturnedafteraboutaweekforhearingscreening (test) andpuerperal consultation. Ifthe infant failedthe test, a retestwas scheduled tobe performed in approxi-mately15days.Intheeventofnoattendanceofthebaby forthetestorretest,themotherwascontactedinorderto scheduleanewdate.
It was considered that the baby passed the test when therewereresponsesin bothearsfortheprocedures per-formed.
It is noteworthy that in cases where newborns passed the hearing screening test and had no risk indicators for hearingloss,theirparentsreceivedguidanceaboutthe typ-icalof hearingandlanguagedevelopment,andonhowto proceedincaseof anychange inthisdevelopment(i.e.a newassessment); thenmotherandbabyweredischarged. Newbornswhopassedthehearingscreeningtestbutshowing riskindicatorsforhearinglosswerereferredforamonitoring program.Inthisprogram,thebabyattendedaconsultation everytwomonthsduringthefirstyear oflife, inorderto evaluateandmonitoritshearingandlanguagedevelopment. Infants who failed the hearing screening test were referredforafullhearingevaluation.
Evoked otoacoustic emission and automatic auditory brainstemevokedpotentialtestswerecarriedoutwiththe helpof a hand-heldAccuScreen® screener (Madsen),
suit-ableforuseinhearingscreeningprograms.Tocapturethe answers,anearprobewascoupledtotheexternalearofthe newborn,preferablyduringphysiologicalsleep,orwhenstill andquiet.Beforetheprocedures,anautomaticcalibration oftheequipmentwasperformed, whichdependedonthe newborn’sexternalauditorycanalvolume.
The transient evoked otoacoustic emissions were gen-erated from a click-type stimulus (frequency range, 1.5---4.5kHz) withintensity ranging between 45 and 60dB HL.Theminimumstabilityoftheprobeobtainedduringthe test was 70%. For the analysis of results, the equipment countsresponsesignal peaks;thepresence ofeightpeaks wasnecessarytoconsiderthattheneonatepassedthetest. The distortion product evoked otoacoustic emissions were generated from the presentation of a primary tone pairofdifferent frequencies(F1 andF2) ina relationship F2/F1=1.22, inwhich F1is the primarystimulusoflower frequencyandF2theprimarystimulusofgreaterfrequency; andthedistortionproductobtainedwilloccurinadifferent frequencyrange.Thestimuliwerepresentedontwolevels (L1/L2)of 60/50dBSPL.Forscreeningandanalysisofthe results,protocol1oftheequipmentwasused,which eval-uatesthefrequencies of 5,4, 3,and 2kHz,in this order. Thetestiscompletedwhenthenewbornpresentsresponse inthreefrequencies (passed)or whenit does notpresent responseintwofrequencies(failed).
Theautomaticbrainstemauditoryevokedpotentialtest was conducted with the electrodes applied to vertex (active), zygoma (ground), and C7 vertebra (reference). For this purpose, Ambu® Neuroline 720 disposable
elec-trodes were used. These deviceswere applied after skin cleaning with an abrasive paste (Nuprep®), ensuring 4
of maximum impedance for the electrodes. The stimula-tionparameterswere:clicksequencestimulusat35dBnHL, sampling rate 16Hz, click level of approximately 80Hz, incomingbandwidthfrom70Hzto4kHz,andgainof2000.
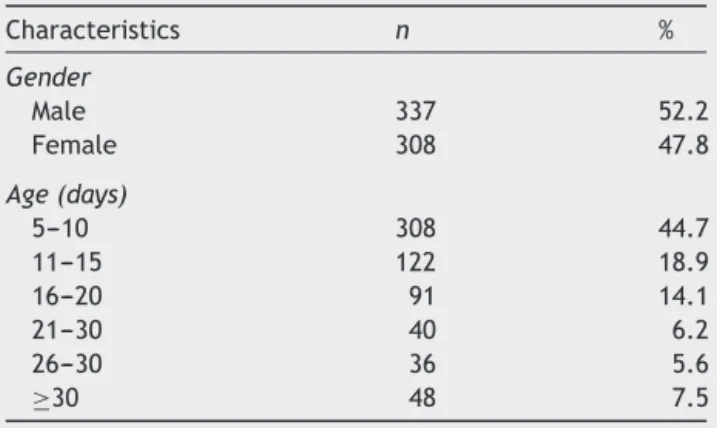
Table 1 Description of gender and age of infants who attendedscreening.
Characteristics n %
Gender
Male 337 52.2
Female 308 47.8
Age(days)
5---10 308 44.7
11---15 122 18.9
16---20 91 14.1
21---30 40 6.2
26---30 36 5.6
≥30 48 7.5
Forresponseanalysis,the‘‘passed’’resultwasestablished when a response to the stimulus was detected by the machine.
The results of this study were presented with the use ofdescriptiveandinferentialstatistics.Spearman’s correla-tionwasappliedtoverifytherelationshipamongvariables: birthweight,gender, age,gestationaltime,typeof deliv-ery, complicationsduring pregnancy,Apgar scoreat 1and 5minoflife,riskindicatorsforhearingloss,andresultsof transientotoacousticemissions.Thesignificancelevelwas setat5%(p≤0.05).
It is noteworthy that the decision was made to corre-latethevariablesonlywiththeresultsoftransientevoked otoacousticemissions,sincedistortionproductevoked otoa-cousticemissionsandautomaticbrainstemauditoryevoked potentials werecarriedout onlyin infantsthat failedthe transient otoacoustic emission test. The low number of childrenundergoingtheseproceduresprecludedthe corre-lation.
Results
Throughoutthisstudy,645(96.3%)of670neonatesbornin thematernityattendedtoneonatalhearingscreeningtests. Itwasnotpossibletofindand/orreschedulethe25neonates whodidnotattendand,consequently,thereisno informa-tionastotheirhearingstatus.
The percentage of ‘‘passed’’ infants in this hearing screening program was 98.5% (635), of ‘‘failed’’ babies, 0.62%(four),andofnon-attendanceforcompletionofthe diagnostic process, 0.93% (six). Among those babies who passed, 92.6% (588) were discharged and 7.4% (47) were referred formonitoring, duetothepresence ofsome risk factor(Fig.1).
Infants whofailed were referred for diagnostic proce-dures,andtheiraudiologicalevaluationresultsshowedthe presenceofconductive-typehearinglossinallcases(three withbilateralandonewithunilateralloss).
When analyzing the variable ‘‘age’’, it was observed that 308 (47.75%) infants were submitted to our hearing screening programat 5---10daysofage;the meantimeof assessmentwas14days.As tothevariable‘‘gender,’’the attendanceforbothgenderswassimilar(Table1).
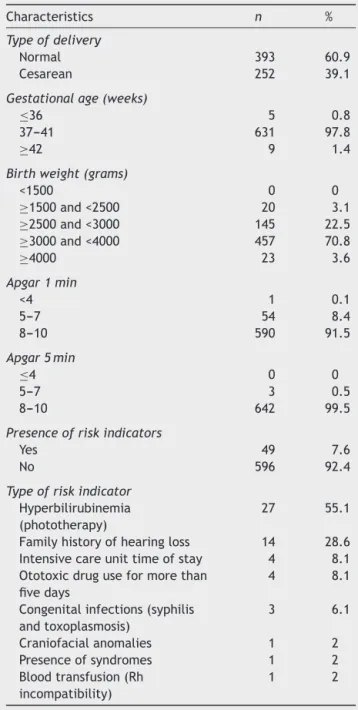
Table2 Perinatalcharacteristicsofbabiesscreenedinthe program.
Characteristics n %
Typeofdelivery
Normal 393 60.9
Cesarean 252 39.1
Gestationalage(weeks)
≤36 5 0.8
37---41 631 97.8
≥42 9 1.4
Birthweight(grams)
<1500 0 0
≥1500and<2500 20 3.1 ≥2500and<3000 145 22.5 ≥3000and<4000 457 70.8
≥4000 23 3.6
Apgar1min
<4 1 0.1
5---7 54 8.4
8---10 590 91.5
Apgar5min
≤4 0 0
5---7 3 0.5
8---10 642 99.5
Presenceofriskindicators
Yes 49 7.6
No 596 92.4
Typeofriskindicator
Hyperbilirubinemia (phototherapy)
27 55.1
Familyhistoryofhearingloss 14 28.6 Intensivecareunittimeofstay 4 8.1 Ototoxicdruguseformorethan
fivedays
4 8.1
Congenitalinfections(syphilis andtoxoplasmosis)
3 6.1
Craniofacialanomalies 1 2 Presenceofsyndromes 1 2 Bloodtransfusion(Rh
incompatibility)
1 2
childbirth,withmeanweightof3248gandwithappropriate one-andfive-minuteApgarscores(Table2).
As for risk indicators for hearingloss, such occurrence wasnotedina minorityofinfants (7.6%),withameanof riskindicators/babyof1.12;themostprevalentriskfactor washyperbilirubinemiatreatedwithphototherapy(Table2). In the mothers’ profile analysis,most were of theage group between 16 and 25 years (57.82%), did not smoke (89.5%), did not use alcohol or drugs (98.6%), and had nocomplications duringpregnancy(72.5%). The most fre-quentgestationalcomplicationwasurinarytractinfection (Table3).
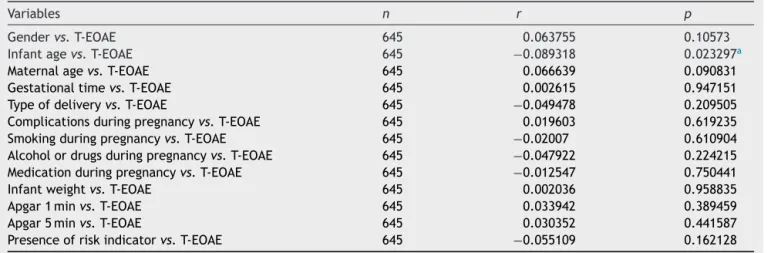
By correlating the variables studied with the results of transient otoacoustic emissions, we observed only a
Table3 Gestationalprofileofmothersofbabiesscreened intheprogram.
Characteristics n %
Age(years)
13---20 201 32.8
21---25 180 27.9
26---30 141 21.9
31---35 81 12.5
≥36 32 4.9
Complicationsduringpregnancy
Yes 177 27.5
No 468 72.5
Typeofcomplication
Urinaryinfection 138 78 Placentalabruption 17 9.6
Hypertension 5 2.9
Diabetes 2 1.1
Thyroid 3 1.7
Depression 2 1.1
Anemia 4 2.2
Other 6 3.4
Alcoholordrugsduringpregnancy
Yes 9 1.4
No 636 98.6
Smokingduringpregnancy
Yes 68 10.5
Not 577 89.5
Medicationduringpregnancy
Yes 159 24.6
No 486 75.4
significantnegativecorrelationforinfant’sage:thehigher theinfant’sage,thelowerthe‘‘failed’’rate(Table4).
Discussion
Theimplementationofuniversalnewbornhearingscreening programs intends to minimize and/or prevent hearing impairmentrelateddeficitsinlanguage,social,emotional, and cognitive development of children, regardless of the presenceofriskindicators.
In the literature reports it can be seen that, for a screeningprogramtobeconsidereduniversal,atleast95%of neonatesmustbeevaluated.1Basedonthisindex,itcanbe saidthatthisprogramwasuniversal,sinceitcovered96.3% ofnewbornsinthismaternity.Thus,theimportanceof uni-versalscreeninginthismaternityisreinforcedbythefact thatthemajorityofthepopulationcaredforisconsidered asatlowriskforhearingloss.
Table4 Correlationamongvariablesstudiedwiththeresultsoftransientevokedotoacousticemissions.
Variables n r p
Gendervs.T-EOAE 645 0.063755 0.10573
Infantagevs.T-EOAE 645 −0.089318 0.023297a
Maternalagevs.T-EOAE 645 0.066639 0.090831
Gestationaltimevs.T-EOAE 645 0.002615 0.947151
Typeofdeliveryvs.T-EOAE 645 −0.049478 0.209505
Complicationsduringpregnancyvs.T-EOAE 645 0.019603 0.619235 Smokingduringpregnancyvs.T-EOAE 645 −0.02007 0.610904
Alcoholordrugsduringpregnancyvs.T-EOAE 645 −0.047922 0.224215
Medicationduringpregnancyvs.T-EOAE 645 −0.012547 0.750441
Infantweightvs.T-EOAE 645 0.002036 0.958835
Apgar1minvs.T-EOAE 645 0.033942 0.389459
Apgar5minvs.T-EOAE 645 0.030352 0.441587
Presenceofriskindicatorvs.T-EOAE 645 −0.055109 0.162128
T-EOAE,transient-evokedotoacousticemissions;p,significancelevel;r,correlationcoefficient.
aStatisticallysignificantrelationship.
Anotherfactobservedinthisstudy,relatedtoitsscope, is the low dropout rate, which corroborates the findings describedintheliterature.18,34However,otherstudieshave reportedahighdropoutrateasamajorchallengefor new-bornhearingscreeningprograms.35,36
Thefactthatthehearingscreeningtestswereperformed onthebabiesonthedayscheduledforpuerperal consulta-tionandtheactivesearchsystemconductedbythehealth workers of theBasic HealthUnits of themunicipality are possibleexplanationsforthislowdropoutrate.
The implementationof newbornhearingscreening pro-gramsinthis country,especiallyin maternities thatserve people with a lower socioeconomic status, is confronted withmany difficultiesthat hinderitsefficiency, sincethe dropoutrateof thispopulationduringtheprocessof new-born hearing screening is very high. Included among the reasonsfornotattendingtotherecommendedreturnsare a lack of information of parents about the causes and symptoms, and the impactof hearing loss on the overall developmentofthechild,aprevalentideaamongmothers thattheirchildrenhavenoriskofsufferingahearingloss, andanxietytriggeredbytheknowingthattheirchildrenare beingtested.36
By analyzing another indicator of effectiveness of the program, it was observed that the age group with high-estconcentrationofscreeningtestsperformedwasthatof infantsbetweenthefifthandtenthdayoflife(mean,12); thisfindingisconsistentwiththeliterature,whichcallsfor screeningtestsinthefirstmonthoflife.1
The percentageofhearinglossfound inourpopulation was0.62%. Intheliterature,lowerandsimilarrateswere found,rangingbetween0.1%and0.5%;18,22,36---38buthigher rateswerealsofound,rangingbetween1.8%and3.44%.39---41 Thisvariationmaybeduetothedifferenceamong popula-tionsstudiedandalsoamongmethodologiesemployed.
The percentage of children who failed and thus were referredfordiagnosiswas1.7%---lessthanthose4%reported intheliterature.1,42Byanalyzingtheuseoftransient otoa-coustic emissionsasan initial test, it wasfoundthat 95% of infants passed the exam. In the Brazilian literature, thispercentagerangedfrom85%to96.78%;someofthese
studiescorroboratethisfinding,whileothersdonotconfirm it.19,40,43,44
Thefindingsofthisstudy,includingtheeffectivenessof theprogramandlackofsensorineuralhearingloss,are jus-tifiedbythefactthatmostoftheevaluatedbabiesshowed noriskindicatorsforhearingloss,bythenumberofbabies evaluatedintheperiodand,finally,becausethescreening test washeld in the same day of puerperal consultation, allowingtherealizationofseveralproceduresonthesame dayandplace.
Anotheraspectaddressedbytheauthorswasthe charac-terizationofmothersandbabiesthatattendedthisprogram. Itmustbeborneinmindthat32.8%ofmothersinthisstudy wereaged13---19 years,thusbeing classifiedasteenagers accordingtotheWorldHealthOrganization.45
Onestudyreportedthatoccurrenceofpregnancyinthis periodisaconsistentpublichealthproblem,becauseofthe greaterriskforthemotherandherinfant,inadditiontoits strongbiological,psychological,andsocialimpact.Therisk ofmaternaldeathforwomenaged15---19yearsistwicethe riskfor womenaged20---24years.46 However,inthisstudy therewerefewcomplicationsinthispopulation.
Finally,bycorrelatingthesevariableswiththeresultsof transientotoacousticemissions,asignificantnegative cor-relationwasnotedonlyfortheinfant’sage:thehigherthe age,thelowerthefailurerate.However,therewasno cor-relationamongothervariablesstudied,includingpresence ofriskindicators,withtheresultsoftheexamination.
Onestudyindicatesthatfailureratescanvaryfrom5%to 20%whenthescreeningprocedureisperformedwith otoa-cousticemissionsduringthefirst24h,fallingto3%whenthe testisheldbetween24and48hafterbirth.42
InBrazil,most servicesperformtheir neonatalhearing screeningbeforedischargingtheinfant;however,thereisno ruleindicatingwhetherthetestshouldbeconductedduring thefirst24hoflifeoratalatertime,duringthefirst48hof life.Thus,itremainsuncleariftheinfant’slifespanaffects theoutcomeofneonatalhearingscreeningtests.47
neonatalhearingscreening procedures;26 however,itmust besaidthatotherstudiesfoundcorrelationbetweenthese variables.37 The most common risk factor in this popula-tionwashyperbilirubinemiatreatedwithphototherapy;this findingagreeswithdataintheliterature.27 Thisfactorcan compromisethenewbornhearingability,withinnerearand centralauditorypathwayinjury.48
Conclusion
The universal newborn hearing screening program imple-mented in this maternity ward was effective and meets nationalandinternationalrecommendations.Asforthe par-ticipants’profile,thepopulationconsistedofyoungmothers
with few alterations in their pre-, peri-, and post-natal periods, and withhealthy infants. The only variable that influenced the results of transient otoacoustic emissions afterhospital dischargewas theage at which the infants wereevaluated.
Funding
source
ThisstudywasfundedbyFundac¸ãodeAmparoàPesquisado EstadodeSãoPaulo---FAPESP.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Annex.
Newborn hearing screening program
Mother name: ____________________________________________Age
Baby’s name: ______________________________________ BD: ____ / ____ / _____ Gender ( ) F ( ) M Weight: __________ Apgar: ____ / _____
Prenatal care: ( ) yes ( ) no.
Received information on hearing characteristics in prenatal care: ( ) yes ( ) no. Complaints about hearing: ( ) yes ( ) no. Which? _____________________________ Do you think it is important to evaluate your child’s hearing? ( ) yes ( ) no.
Have you ever heard about neonatal auditory screening (teste da orelhinha)? ( ) yes ( ) no.
Complications during pregnancy: ( ) yes ( ) no. Which?
______________________________________________________________________ Smoking during pregnancy ( ) yes ( ) no. How many cigarettes? __________
Alcohol use during pregnancy: ( ) yes ( ) no. How much: _______________ Drugs during pregnancy: ( ) yes ( ) no. What: _____________
Gestational time: _________________ Delivery type: ( ) normal ( ) cesarean ( ) forceps Breastfeeding: ( ) exclusive ( ) mixed ( ) artificial Bottle feeding: ( ) yes ( ) no.
Pacifier use: ( ) yes ( ) no.
Risk indicators for hearing change
( ) Hearing loss family history. Who? _________________ ( ) Inbreeding.
( ) Congenital infections (rubella, syphilis, CMV, herpes, toxoplasmosis, HIV). In which month? ________
( ) ICU stay
( ) Craniofacial anomalies. What? _________________________ ( ) Hyperbilirubinemia ( ) sunbathing ( ) phototherapy ( ) transfusion
( ) Presence of syndromes. What? _________________________________________ ( ) Viral or bacterial meningitis
( ) Ototoxins for more than five days (antibiotics, aminoglycosides, diuretics, chemotherapeutic agents)
( ) Encephalopathy, hydrocephalus, peri-ventricular hemorrhage, head trauma ( ) Seizures
( ) Bronchopulmonary dysplasia, persistent pulmonary hypertension, or diaphragmatic
hernia
( ) Mechanical ventilation for a minimum of five days
References
1.Joint Committee on Infant Hearing. Executive Summary of
JointCommitteeonInfantHearingYear2007.Position
State-ment:principlesandguidelinesforearlyhearingdetectionand
interventionprograms Internet.Available from:http://www.
jcih.org/ExecSummFINAL.pdf
2.ConselhoRegionaldeFonoaudiologia---2a
.Região SãoPaulo.
Parecer do CFFa. n. 05/00, de 10 de junho de 2000.
AspectospertinentesàTriagem AuditivaNeonatal(TAN).São
Paulo:ConselhoRegionalde Fonoaudiologia---2a
. RegiãoSão
Paulo. Available from: http://www.fonosp.org.br/legislacao/
pareceres-do-cffa/parecer-do-cffa-n%C2%BA-0500/ [accessed 09.03.2012].
3.Brasil. Lei12.303, de02de agostode 2010. Dispõesobre a
obrigatoriedade de realizac¸ão do exame denominado
Emis-sões Otoacústicas Evocadas. Brasília; 2010. Available from:
http://www.planalto.gov.br/ccivil03/Ato2007-2010/2010/ Lei/L12303.htm
4.TochettoTM,VieiraEP.Legislac¸ãobrasileirasobretriagem audi-tivaneonatal.1sted.SãoPaulo:Pró-fono;2006.
5.SilvaDPC,MartinsRHG.Análisedasemissõesotoacústicas tran-sientesedospotenciaisevocadosauditivosdotroncoencefálico emneonatoscomhiperbilirrubinemia.BrazJOtorhinolaryngol. 2009;75:381.
6.Azevedo MF. Emissões otoacústicas. In: Figueiredo MS, edi-tor. Conhecimentos essenciais para entenderbem: emissões otoacústicas eBERA. São José dos Campos: Pulso Editorial; 2003.p.35---83.
7.BorgesCAB,MoreiraLMO,PenaGM,FernandesFR,BorgesBCB, OtaniBH.Triagemauditivaneonataluniversal.ArqInt Otorrin-olaringol.2006;10:28---34.
8.KunstLR,DidonéDD,MoraesSC,EscobarGB,VaucherAV, Biag-gioEPV,etal.Sociodemographicprofileofmothersadmitted toa serviceofnewbornhearingsccreening. DistúrbComum. 2013;25:328---35.
9.MatasCG.Medidaseletrofisiológicasdaaudic¸ão-audiometria de tronco cerebral. In: Carvalho RMM, editor. Fonoaudiolo-gia:informac¸ãoparaaformac¸ão. Riode Janeiro:Guanabara Koogan;2003.p.43---57.
10.Ito-Orejas JI, Ramirez B, Morais D, Almaraz A, Fernandez-CalvoJL.Comparisonoftwo-steptransientevokedotoacoustic emissions(TEOAE)andautomatedauditorybrainstemresponse (AABR)oruniversalnewbornhearingscreeningprograms. Pedi-atrOtorhinolayngol.2008;72:1193---201.
11.SimonekMCS,AzevedoMF.Respostasfalso-positivasnatriagem auditiva neonatal universal: Possíveis causas. Rev CEFAC. 2011;13:292---8.
12.Bubbico L, Bartolucci MA, Broglio D. The newborn hearing screeninginItaly.ItJPediatr.2005;31:290---2.
13.De Capua B, Costantini D, Martufi C, Latini G, Gentile M, DeFeliceC.Universalneonatalhearingscreening:TheSiena (Italy)experienceon19.700newborns.EarlyHumDev.2007;83: 601---6.
14.Lewis DR,Marone SAM,MendesBCA, Cruz OLM, NóbregaM. Comitê multiprofissional em saúde auditiva COMUSA. Braz J Otorhinolaryngol.2010;76:121---8.
15.PatelH,FeldmanM,CanadianPaediatricSociety,Community Paediatricscommittee.Universal newbornhearingscreening. PaediatrChildHealth.2011;16:301---5.
16.GilbeyP,KrausnC,GhanayimR,Sharabi-NovA,BretlerS. Uni-versalnewbornhearingscreeninginZefat,Israel:Thefirsttwo years.IntJPediatrOtorhinolaryngol.2013;77:97---100.
17.GhirriP,LiumbrunoA,LunardiS,Forli F,BoldriniA, Baggiani A, et al. Universal neonatal audiological screening: experi-enceoftheUniversityHospitalofPisa.RevItalPediatr.2011; 37:16.
18.Barreira-Nielsen C, Neto HAF, Gattaz G. Processo de implantac¸ãodePrograma deSaúdeAuditivaem duas mater-nidadespúblicas.RevSocBrasFonoaudiol.2007;12:99---105.
19.LimaGM,MarbaST,SantosMF.Hearingscreeninginaneonatal intensivecareunit.JPediatr.2006;82:110---4.
20.Amado BCT, Almeida EOC, BerniOS. Prevalence ofdeafness riskindicatorsinnewbornsinaSãoPauloupcountrymaterninty hospital.RevCEFAC.2009;11:18---23.
21.VieiraEP,MirandaEC,AzevedoMF,GarciaMV.Occurenceofrisk indicatorsforhearinglossoverfouryearsinaneonatalhearing screeningprogramofapublichospital.RevSocBrasFonoaudiol. 2007;12:214---20.
22.Mattos WM, Cardoso LF, Bissani C, Pinheiro MMC, Viveiros CM,FilhoWC.Newbornhearingscreeningprogram implanta-tionanalysisataUniversityHospital.BrazJOtorhinolaryngol. 2009;75:237---44.
23.BarbozaACS,ResendeLM,FerreiraDBC,LapertosaCZ,Carvalho SAS.Correlationbetweenhearinglossandriskindicatorsina neonatalhearingscreeningreferenceservice.AudiolCommun Res.2013;18:285---92.
24.Oliveira JS,Rodrigues LB, Aurélio FS, Silva VB. Risk factors and prevalence of newborn hearing lossin a private health caresystemofPortoVelho,NorthernBrazil.RevPaulPediatr. 2013;31:299---305.
25.PereiraPKS,MartinsAS,VieiraMR,AzevedoMF.Programade triagemauditivaneonatal: associac¸ãoentreperdaauditivae fatoresderisco.Pró-Fono.2007;3:267---78.
26.DidonéDD,GarciaMV,KunstLR,VieiraEP,SilveiraAF.Correlac¸ão dosindicadoresderiscoparadeficiênciaauditivacomafalhana triagemauditivaneonatal.Saúde(SantaMaria).2013;1:113---20.
27.DantasMBS,AnjosCAL,CamboimED,PimentelMCR.Resultados deumprogramadetriagemauditivaneonatalemMaceió.Braz JOtorhinolaryngol.2009;75:58---63.
28.GrizSMS,AlmeidaeSilvaAR,BarbosaCP,MenezesDC,Curado NRPV,SilveiraAK,etal.Indicadoresderiscoparaperdaauditiva emneonatoselactentesatendidosemumprogramadetriagem auditivaneonatal.RevCEFAC.2011;13:281---91.
29.SwanepoelD,EbrahimS,JosephA,FriedlandPL.Newborn hear-ingscreeninginaSouthAfricanprivatehealthcarehospital.Int JPediatrOtorhinolaryngol.2007;71:881---7.
30.GuimarãesVC, Barbosa MA. Prevalence of auditory changes innewbornsinateachinghospital.IntArchOtorhinolaryngol. 2012;16:179---85.
31.BevilacquaMC,AlvarengaKF,CostaOA,MoretAL.The univer-salnewbornhearingscreeninginBrazil:fromidentificationto intervention.IntJPediatrOtorhinolaryngol.2010;74:510---5.
32.NationalInfantHearing.Earlyidentificationofhearing impair-mentininfantsand youngchildren. NIHConsensStatement. 1993;11:1---24.
33.Durante AS, Carvalho RMM, Costa MTZ, Cianciarullo MA, VoegelsRL, TakahashiGM,etal. Programa deTriagem Audi-tivaNeonatal:modelodeimplementac¸ão.ArqOtorrinolaringol. 2004;8:56---62.
34.KorresSG,BalatsourasDG,NikolopoulosT,KorresGS,Ferekidis E.Makinguniversalnewbornhearingscreeningasuccess.IntJ PediatrOtorhinolaryngol.2006;70:241---6.
35.MachadoMS,OliveiraTMT,CóserPL.Triagemauditiva neona-taluniversal:projetopilotonoHospitalUniversitáriodeSanta Maria(RS)-Brasil.Pró-fono.2002;14:199---204.
36.Onoda RM, Azevedo MF, Santos AMN. Neonatal Hearing Screening: failures, hearing loss and risk indicators. Braz J Otorhinolaryngol.2011;77:775---83.
37.VohrB,CartyL,MooreP,LetourneauQ.TheRhodeIsland hear-ing assessment program: experience with statewide hearing screening.WPediatr.1998;133:353---440.
39.TiensoliLO,GoulartLMHF,ResendeLM,ColosimoEA.Hearing screeninginapublichospitalinBeloHorizonte,MinasGerais State,Brazil:hearingimpairmentandriskfactorsinneonates andinfants.CadSaúdePública.2007;23:1431---41.
40.BoscattoSD,MachadoMS.HearingscreeningofSãoVicentede PauloHospital:surveydata.RevCEFAC.2013;15:1118---24.
41.GaffneyM,Green DR,GaffneyC.Newbornhearingscreening andfollow-up:arechildrenreceivingrecommendedservices. PublicHealthRep.2010;125:199---207.
42.ComitêBrasileiroSobrePerdasAuditivasnaInfância.Período Neonatal.Recomendac¸ão01/99.JornaldoCFFa.2000;5:3---7.
43.Franc¸ozoMFC,FernandesJC,LimaMCMP,RossiTRF. Improve-mentofreturnratesinaneonatalhearingscreeningprogram: the contribution of social work. Soc Work Health Care. 2007;3:179---90.
44.RodriguesPAL,CarvalhoTSF,LaurisJRP,SchochatE.Resultsofa newbornhearingscreeningprograminCuiabá---MatoGrosso. BrazilRevSocBrasFonoaudiol.2011;16:454---8.
45.World Health Organization. Young people’s health: a chal-lenge for society. Geneva: World Health Organization; 1986.
46.OliveiraFC,SuritaFG,PintoeSilvaJL,CecattiJG,ParpinelliMA, HaddadSM,etal.Severematernalmorbidityandmaternalnear missintheextremesofreproductiveage:resultsfromanational cross-sectional multicenter study.BMC Pregnancy Childbirth. 2014;14:77.
47.RibasA,CabralJ,Gonc¸alvesV,Gonc¸alvesCGO.Newborn hear-ingscreeningprogram:theinfluenceofthelifespanofnewborns intheresearchoftransientotoacousticemissions.RevCEFAC. 2013;15:773---7.