http://dx.doi.org/10.1590/2317-6431-2015-1641 ISSN 2317-6431
Prevention in a school environment of hearing loss due
to leisure noise
Prevenção da perda auditiva no contexto escolar frente ao ruído
de lazer
Bruna Antonini Santana1, Kátia de Freitas Alvarenga2,Priscila Carvalho Cruz3, Isabela Alves de Quadros1, Lilian
Cássia Bornia Jacob-Corteletti2
ABSTRACT
Purpose: To verify the habits and attitudes of school-age youths re-garding the use of personal music players, and assess their knowledge level about the harmful effects to the hearing of exposure to amplified music before and after an educational lecture. Methods: A total of 58 elementary and middle school students aged 10 to 17 years participated in the study. We presented an educational lecture using an expository dialogue format with audiovisual resources. To evaluate the students, we applied two online questionnaires before and 15 days after the lec-ture. Descriptive analysis was also performed. Results: Most students reported using personal music players with earphones above the mean intensity of the equipment and for fewer than 3 hours a day. The most frequent complaint was tinnitus. After the educational lecture, there were differences in knowledge about the concept of hearing loss and the fact that high-intensity music in moments of leisure may cause hearing loss. There was also a difference in the intensity used to listen to music with earphones, which decreased. Conclusion: Most students had prior knowledge of the harmful effect of amplified music on hearing and even then, some indicated inadequate habits. The educational lecture showed significant changes in only some of the aspects investigated, reflecting a need to structure continuous actions towards hearing loss prevention in this population. The inclusion of the school and the family in educational actions and the continuity of these actions are fundamental to effective changes in habits and attitudes among children and adolescents.
Keywords: Hearing loss, Noise-induced; Child; Adolescent; Health education; Student health services
RESUMO
Objetivo: Verificar os hábitos e atitudes de jovens em idade escolar com relação ao uso de estéreos pessoais e avaliar o nível de conhecimento sobre os efeitos nocivos da exposição à música amplificada na audição, antes e após uma palestra educativa. Métodos: Participaram 58 estudan-tes do ensino fundamental e médio, entre 10 e 17 anos de idade. Foi rea-lizada palestra educativa, mediante aula expositiva dialogada, utilizando recursos audiovisuais. Para avaliação foram aplicados dois questionários no formato online, antes e após 15 dias da palestra. Realizou-se, também, análise descritiva. Resultados: A maioria dos escolares relatou fazer uso de estéreos pessoais com fone de ouvido, acima da intensidade média do equipamento e por período inferior a três horas diárias. A queixa mais frequente foi o zumbido. Após a palestra educativa, houve diferença no conhecimento sobre o conceito de perda auditiva e de que música em intensidade elevada, em momentos de lazer, pode causar perda auditiva. Também houve diferença na intensidade utilizada para ouvir música com fone de ouvido, que foi reduzida. Conclusão: Grande parte dos escolares possuía conhecimento prévio a respeito dos prejuízos da música amplificada, para a audição e, ainda assim, alguns referiram há-bitos inadequados. A palestra educativa revelou mudanças significativas em apenas alguns aspectos investigados, evidenciando a necessidade de estruturar ações contínuas na prevenção de perdas auditivas nessa população. A inclusão da escola e da família nas ações educativas e a continuidade dessas ações são fundamentais para mudanças efetivas de hábitos e atitudes das crianças e adolescentes.
Descritores: Perda auditiva provocada por ruído; Criança; Adolescente; Educação em saúde; Serviços de saúde para estudantes
Study conducted at the Department of Speech and Hearing Therapy, Bauru School of Dentistry, Universidade de São Paulo – USP – Bauru (SP), Brazil. (1) Postgraduate Masters Program in Communication Disorders, Department of Speech and Hearing Therapy, Bauru School of Dentistry, Universidade de São Paulo – USP – Bauru (SP), Brazil.
(2) Department of Speech and Hearing Therapy, Bauru School of Dentistry, Universidade de São Paulo – USP – Bauru (SP), Brazil.
(3) Professionalizing Practice in Adult Audiological Evaluation, Department of Speech and Hearing Therapy, Bauru School of Dentistry, Universidade de São Paulo – USP – Bauru (SP), Brazil.
Funding: Grant received from the Programa de Pré-Iniciação Científica da Pró-Reitoria de Pesquisa da Universidade de São Paulo (USP). Conflict of interests: No
Authors’ contribution:BAS main author, research project development, data collection and analysis, manuscript preparation; KFA research project development, data analysis, manuscript preparation; PCC data analysis, manuscript preparation; IAQ data collection, manuscript preparation; LCBJC mentor, research develop-ment, data collection and analysis, manuscript preparation and approval of its final version.
Corresponding author: Lilian Cássia Bornia Jacob-Corteletti. E-mail: [email protected]
INTRODUCTION
Hearing loss caused by leisure activities with loud noise has been growing substantially in young populations(1,2,3),
causing concern among researchers(3,4,5,6,7,8). Exposure to high
sound pressure levels in leisure activities has been placing at risk the hearing of young individuals throughout the world. Approximately half of all adolescents and young adults (12 to 35 years of age) in countries of medium and high income use personal sound devices, and 40% of them are exposed to potentially harmful sound levels in clubs, discos, and bars(9).
In these places, abuses with exposure to amplified music are common. Sound pressure levels are known to have exceeded 104–112 dB(A)(10), and dosimetric evaluations of disc jockeys
(DJs) have shown exposures of 93.2 to 109.7 dB(A)(11).
Personal music players currently enable playback and recording of digital sounds that may reach strong intensities without distortion. When delivered through earbuds, the sounds may reach levels of 85 to 115 dB(A) and, in extreme cases, up to 120 dB(A)(1). In addition to the sound intensity level,
other hearing risk factors are the duration of the exposure to the noise and the environment in which music players are used, since the tendency is to increase the volume with higher competitive noise(1).
A document published by the European Commission - Health & Consumer Protection DG/2008 (regulation of noise at work in the European Community - Directive 2003/10/EC, implemented in 2006) referred to a limit to leisure noise ex-posure, which may be considered equal to noise exposure in the work environment (equivalent to 80 dB[A] for an 8-hour working day and 5 days or 40 working hours per week).
This comparison between the limit of noise exposure dur-ing work and leisure aims at preventdur-ing heardur-ing loss related to entertainment activities since there is no regulation in this regard. From this perspective, when we consider an average use of personal music players of 7 hours a week (1 hour/day), this average would exceed that recommended by the Regulation of Noise at Work when sound levels exceed 89 dB(A)(1).
The sound pressure level of personal portable music players at a maximum volume and measured with the KEMAR system varies from around 80 to 115 dB(A) in different devices(1).
Previous studies reported a direct correlation between long periods (both daily and yearly) of exposure to high-intensity noise with the occurrence of auditory symptoms(5,7,12), of which
tinnitus was the most prevalent (5,7).
Excessive noise may increase the risk of hearing loss, which may be temporary or permanent, and the occurrence of tinni-tus. Exposure to excessive noise may cause severe damage to inner hair cells, although the most affected cells are the outer hair cells(1,13). Tinnitus is one of the main symptoms reported
by the young population after excessive exposure to noise(5,7,8).
In recent studies, researchers showed that temporary hearing losses may cause immediate and irreversible damage to auditory
nerve fibers. These damages may not affect the detection of sounds, i.e., hearing may be normal in terms of audiometric thresholds, but may hinder the ability to process more complex signals. According to a study(13), this condition is called hidden
hearing loss, since the auditory thresholds are normal. The damage to the auditory nerve is, therefore, concealed. Hidden hearing loss may also cause other auditory complaints, such as tinnitus and hyperacusis, suggesting auditory nerve damage(13).
Youths have been showing inadequate behavior regarding the duration of use and volume of portable music players, exceeding 1 hour/day at a strong intensity, thus leading to hearing risks(3,7,14,15). Most individuals in this population are
unaware of the damage that excessive noise exposure may cause to hearing(2,4). The consequences that this exposure can cause
vary from a temporary disorder to future permanent hearing impairment(1,13).
Hearing loss induced by noise is still considered an im-portant health and social problem(1,16), which justifies the
de-velopment and implementation of strategies for its prevention and intervention. Researchers worried about the exposure of youths to noises harmful to the hearing have developed different educational programs for implementation in school classrooms aiming at increasing knowledge about the damages caused by excessive exposure to noise and need of use of hearing protec-tors. The effectiveness of these programs has been demonstrated in questionnaires applied before and after the interventions, showing changes in the behavior and attitudes of adolescents regarding hearing habits(3,4,5,6,7).
In this context, the earlier the child becomes aware of hea-ring risks caused by loud noise through educational campaigns and programs implemented in primary schools, more effective their knowledge, attitudes, and intentions will be regarding the prevention of hearing loss once they become adolescents, thus avoiding common risk behaviors(5,14,15).
The involvement of health professionals and teachers is fundamental to this process to promote reflection on the sub-ject, modify the behavior of the students, and encourage the effective involvement of the parents, who are an essential part of the success of programs for hearing loss prevention(15,17).
The aim of this study was to verify the habits and attitudes of school-age youths regarding the use of personal music players, and assess their knowledge level about the harmful effects on hearing caused by exposure to amplified music before and after an educational lecture.
METHODS
youth in the study and publication of its findings. The form guaranteed anonymity and freedom to withdraw the consent at any moment. The research participants also received expla-nations about the procedures and were invited to fill out an online consent form, in which they selected the item “agree to participate” if they were interested in participating.
Sample
The invitation to participate in the research was delivered to two elementary classrooms (6th and 7th grades) and three middle school classrooms (2nd grade) along with 119 FICF. The classrooms were selected at random. Only 66 students participated in all research stages (educational lecture, and pre- and post-lecture questionnaires), including 53.03% elementary students and 46.97% middle school students. However, only 58 were selected for the analysis (60.35% elementary and 39.65% middle school students), since the FICF signed by the parent or guardian was not returned by all participants, and one student was unable to participate after the authorization was declined by the guardian or parent.
Thus, the participants included 58 students of both genders (56.9% male and 43.1% female), children and adolescents, aged between 10 and 17 years (mean 13.1 years; standard deviation [SD] ± 2.2), users or nonusers of personal music players, and elementary and middle school students. The students were selected based on their availability and interest in participating in the study.
Inclusion criteria
- Student regularly enrolled in primary or secondary school; - Delivery of the FICF signed by the parent or guardian; - Agreement with the consent form;
- Participation at all stages of the research.
Procedures
The students were invited to answer a questionnaire (Appendix 1) before and 15 days after the educational lecture, comprising closed-ended questions investigating their know-ledge, habits, and attitudes regarding exposure to high-intensity music. The questionnaire was developed by the authors on Google Docs®, an entirely free online tool, which generated a form (http://goo.gl/forms/ll5S2BcHgy). The form was compo-sed of the following: 1) Consent form approved by the Research Ethics Committee; 2) Identification form; 3) Questionnaire. The school provided a room equipped with computers for application of the online questionnaire.
The educational lecture used an expository dialogue for-mat. It lasted for 1-hour and was held in a classroom provided by the school administration. We used audiovisual resources such as written information, images, and videos addressing
hearing elements and possible damage caused by exposure to amplified music, emphasizing the use of personal music players. The lecture occurred at two moments: it was initially presented to elementary students, and subsequently to middle school students.
Descriptive statistics determined the mean, SD, and frequency of occurrence of the responses. We applied the Wilcoxon test to compare the results obtained before and after the lecture related to the volume level used to listen to music with the earphones, and the McNemar test to verify the sig-nificance of the students’ changes in answers from the pre- to the post-lecture questionnaires. We considered as significant the results with a p-value ≤0.05.
There was reduced participation of middle school students at all stages of the research. Therefore, the cohort comprised mostly (60.3%) of elementary students.
RESULTS
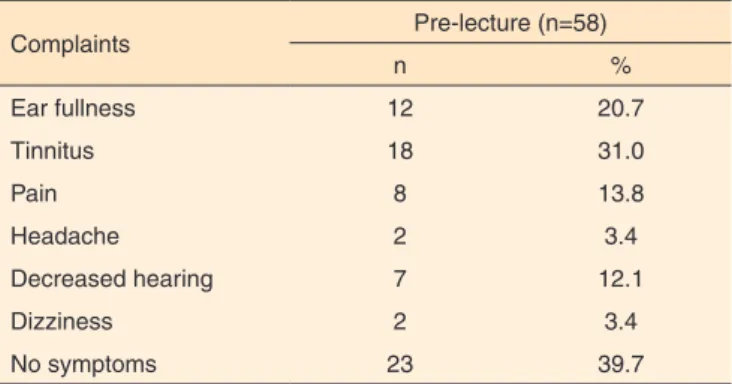
The students were asked about complaints that could be related to exposure to high-intensity music, with the option to include more than one complaint. Most participants (60.3%) reported at least one complaint, of which tinnitus was the most frequent (31%) (Table 1).
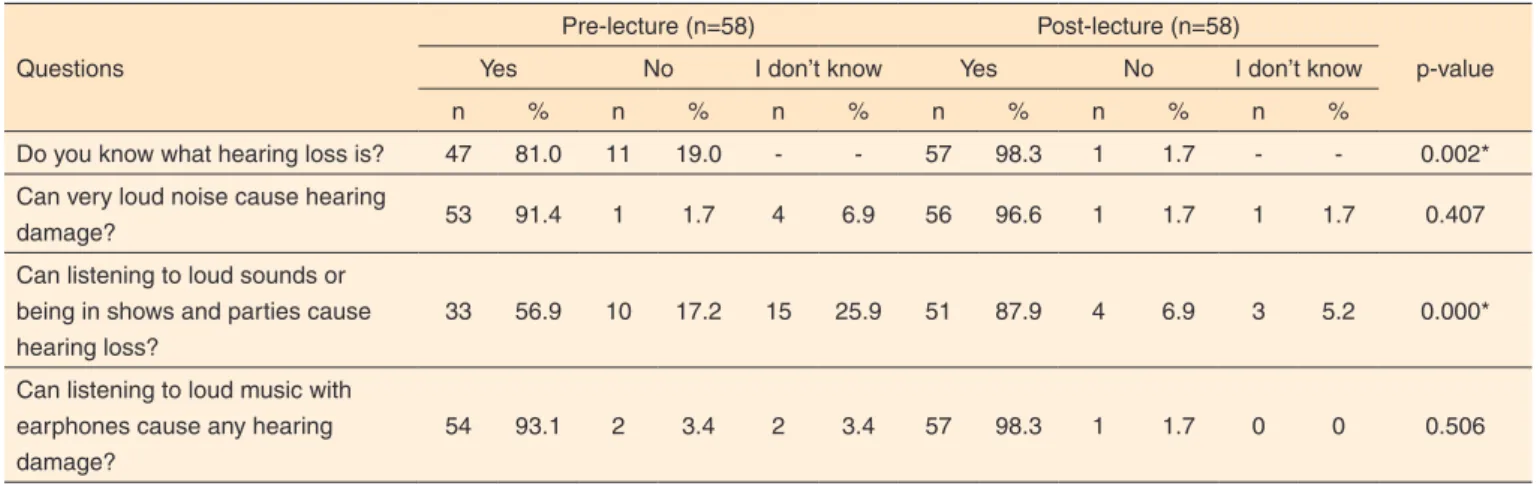
After the educational lecture, there were differences in knowledge about the concept of hearing loss and the fact that high-intensity music in moments of leisure, such as in con-certs and nightclubs, may cause hearing loss. Regarding other questions, we observed that some students acquired knowledge about the subject. However, there was no difference when the questionnaires obtained before and after the lecture were compared (Table 2).
We observed that in both pre- and post-lecture questionnai-res most participants reported the use of personal music players above the average intensity of the equipment and for fewer than 3 hours a day (Table 3). There was a difference (p≤0.05) between the pre- and post-lecture questionnaires regarding the intensity used to listen to music with the earphones. Among most participants who used it above the mean intensity, 31%
Table 1. Characterization of the complaints reported by the school students after use of personal music players
Complaints Pre-lecture (n=58)
n %
Ear fullness 12 20.7
Tinnitus 18 31.0
Pain 8 13.8
Headache 2 3.4
Decreased hearing 7 12.1
Dizziness 2 3.4
and 29.3% (pre- and post-lecture, respectively) reported using the equipment at maximum intensity.
After the lecture, there was a reduction in the number of daily hours in which the participants used music players with earphones, but the difference was not significant.
The students reported a preference for earbuds (72.4% pre-lecture and 70.07% post-lecture). We also observed that in both questionnaires, 1.7% of the cohort mentioned not using earphones to listen to music on personal music players.
DISCUSSION
The results of this study showed that if school-aged youths continue with certain inappropriate behaviors regarding ex-posure to amplified music they may develop some degree of hearing damage.
Previous studies have pointed out tinnitus as the most fre-quent complaint reported by children and adolescents, which may be an indicator of risk related to noise exposure(5,8). Such
finding is similar to that reported in this study, in which most
adolescents had one or more complaints, of which tinnitus was the most frequently reported (Table 1). Tinnitus may occur alo-ne and does not require the occurrence of hearing loss(18). Such
fact may contribute to carelessness among youths since only tinnitus alone may erroneously not appear to be a considerable risk to hearing health.
Most adolescents had previous knowledge about the har-mful effects of high-intensity music on hearing. However, this knowledge did not lead to changes in these youths’ attitudes with regard to exposure to amplified music, since they remained with inadequate habits and attitudes (Table 2), a finding similar to previous studies(8,12,14,15). In another study(19), most students
reported knowing that high-intensity noise may lead to hea-ring loss. However, only some of the participants reported not knowing how to protect their hearing, or not being concerned about preventing the effects of exposure to high-intensity music. Confirming findings from the literature(3,5,8,14,15),most
you-ths in our cohort reported using earphones to listen to music (Table 3), with the exception of one student who reported not using them. Since personal music players are portable devices,
Table 2. Comparison between prior knowledge and knowledge acquired after the educational lecture about hearing and exposure to amplified music
Questions
Pre-lecture (n=58) Post-lecture (n=58)
p-value
Yes No I don’t know Yes No I don’t know
n % n % n % n % n % n %
Do you know what hearing loss is? 47 81.0 11 19.0 - - 57 98.3 1 1.7 - - 0.002*
Can very loud noise cause hearing
damage? 53 91.4 1 1.7 4 6.9 56 96.6 1 1.7 1 1.7 0.407
Can listening to loud sounds or being in shows and parties cause hearing loss?
33 56.9 10 17.2 15 25.9 51 87.9 4 6.9 3 5.2 0.000*
Can listening to loud music with earphones cause any hearing damage?
54 93.1 2 3.4 2 3.4 57 98.3 1 1.7 0 0 0.506
*Significant values (p≤0.05) - McNemar test
Table 3. Comparison between the results obtained before and after the lecture on the use of personal music players with earphones, level of sound intensity, and duration of use
Variables Pre-lecture (n=58) Post-lecture (n=58) p-value
n % n %
Earphone use
Yes 57 98.3 57 98.3 ___
No 1 1.7 1 1.7
Volume
Up to the average intensity 8 13.8 16 27.5 0.047*
Above the average intensity 49 84.8 41 70.6
Duration (daily)
Longer than 3 hours 20 34.5 14 24.1 0.109
Fewer than three hours 37 63.8 43 74.1
*Significant value (p≤0.05) - Wilcoxon test
they are convenient for daily use(12), and since music is
conside-red a pleasant sound, it is regarded as unable of causing damage to the individual(20). However, the habit of listening to
high--intensity music for long durations(1) jeopardizes the hearing
health and may cause irreversible hearing damage. When we consider all 58 students (of whom only one reported not having the habit of using earphones), we conclude that interventions are recommended to prevent hearing loss caused by exposure to music at high sound pressure levels.
It is often possible to hear the music playing on a personal music player of an individual using earphones because it is increasingly common among youths to use the maximum vo-lume of the equipment. The results of this study showed that most patients listened to music at a higher intensity than the equipment’s average (Table 3), a finding aligned with other studies(7,14,15). However, after the educational lecture, it was
possible to observe a significant habit change among a few adolescents (Table 3) who began to set the average intensity of the equipment as the limit. Inadequate attitudes related to auditory health and consequences of noise may be caused by lack of information and absence of interesting educational activities targeting this population, among other reasons(21).
The findings showed that most adolescents remained ex-posed to high-intensity music, using earphones for fewer than 3 hours a day (Table 3), a fact that was also found in other stu-dies(3,7). However, due to the increased intensity, these students
may develop hearing loss.
Another important element to be considered is the type of earphone, since depending on the model, it may boost the potential of the equipment, adding 7 to 9 dB to the intensity level(1). However, a study(22) has reported that the type of
ear-phone does not affect the output levels, a finding attributed to the measurement method. In the present study, as in previous ones, we observed that most adolescents used earphones(1,7,12,22).
These findings show the importance of educational/ preventive actions to help improve the awareness of adoles-cents to exposure to high-intensity music, as suggested in the literature(2,8,14,15,19,21,23).
Some initiatives have already been developed for the pur-pose of promoting and protecting the auditory health of school students. In Brazil, educational actions promoting knowledge in schools are limited(21,23,24,25,26). The “Young Doctor Project”
stands out among them. This project focuses on the auditory health(24) and develops a training program via interactive
distan-ce learning. The program comprises in-person activities using audiovisual resources and 3D iconographic animations from the CD-ROM/Virtual Man: Hearing(27), online tutorial (Cybertutor),
and practical activities, such as workshops, group dynamics, and knowledge multiplication, creating an opportunity for the adolescent to transmit the knowledge to others.
In the United States, researchers(4) have investigated the
effectiveness of a government-sponsored prevention cam-paign for adolescents. The camcam-paign was based on the theory
of planned behavior for guidance and change in habits. The authors believe that the repetition of prevention campaigns for adolescents will establish appropriate attitudes regarding noise exposure. Another study(6) developed a pilot program -
Cheers for Ears – which was able to improve the knowledge of pre-adolescents about the impact of noise on hearing and the habits of primary school students. The program included multimodal educational and interactive activities appropriate for the students’ age, as well as a long-term questionnaire eva-luation in which it was observed that the changes related to the knowledge of hearing and the habit of the students regarding noise exposure were stable and sustained for up to 3 months after the intervention.
The Dangerous Decibels® program, developed in the late
1990s in the United States, is a public health campaign direc-ted to children and adolescents with the aim of substantially reducing the prevalence of hearing loss and tinnitus caused by exposure to intense sounds. It uses interactive strategies ela-borated for children and adolescents about the effects of high--intensity sounds on hearing. In 2015, the Brazilian Academy of Audiology (Academia Brasileira de Audiologia, ABA) joined the program’s partnership network(28). The authors of a
study(26) have verified the effectiveness of a Brazilian version of
the Dangerous Decibels® program in grades 3 to 5 elementary school children and concluded that programs aimed at hearing conservation, such as Dangerous Decibels®, are effective in improving knowledge, attitudes, and behaviors related to ex-posure to potentially dangerous sounds.
The World Health Organization(9) haspublished an
informa-tive catalog, developed with the participation of researchers, focusing on all aspects related to hearing loss due to excessive noise exposure in situations of leisure. This catalog is useful for individuals to acquire knowledge about hearing loss and learn how to protect their hearing from strong intensity sounds during recreational activities.
It is important to elaborate carefully the materials and proce-dures to be used in educational actions, so that the information necessary to promoting hearing health and preventing related problems are provided by resources covering the preferences of the respective age ranges, triggering interest in the subject and leading the individuals to participate actively in the proposed action. The active participation of the adolescents is believed to help the action achieve success, collaborating for the deve-lopment of a critical conscience and, consequently, change in habits and inadequate attitudes regarding high-intensity music. A study(29) has suggested that playful educational actions
The educational actions focused on hearing preservation are recommended to be implemented by health professionals, the school, and by the students’ parents(15,17). Health
professio-nals should take the role of mediators, promoting knowledge about auditory health to the students, as well as to the parents and the school, since they may contribute to the effectiveness of the action.
School participation is fundamental in this process(12,15).
Schools can offer different intervention measures during a student’s formation since they are the second largest influence on a person’s development after the family(19). However, schools
contribute little to build knowledge about the damage caused by noise(12,19). The implementation of educational programs would
enable the use of some disciplines so that teachers could develop strategies to promote hearing health in order to give continuity to the educational actions during the academic year(29).
The continuity of the intervention in the family environment with parental support is relevant to maintain healthier habits regarding exposure to high-intensity music. Results of a study(17)
have shown that many parents do not believe that their children are at risk of developing hearing loss, so they demand little from their children in terms of hearing protection. In addition, most parents have little knowledge of the danger that noise exposure can cause to adolescents, and it is necessary to improve the un-derstanding of the subject in order to create effective programs for auditory conservation. Thus, the participation of the parents in behavioral interventions may be a fundamental part in the success of the programs(14,15,17).
We observed in the present study a greater interest of youn-ger (elementary) students in participating at all research stages when compared with older (middle school) students. Among the different behaviors we observed that some middle school students left the lecture before it ended, and failed to return the FICF signed by a parent or guardian. We should mention that more middle school than elementary students were invited to participate in the study. However, since not all middle school students met the inclusion criteria, they comprised the smallest subcohort in the study.
Based on these findings, we should emphasize an important aspect of the child’s cognitive-affective development that de-termines his or her behavior at different development phases: changes in interpersonal relationships such as affective depen-dence (search for acceptance, approval and affection, usually from the parents), and greater independence and autonomy, observed as part of the development in the passage from chil-dhood to adolescence. With these changes, parents no longer have a large influence on the child’s decisions as in younger ages(30). Based on that, it is believed that educative actions
should start in early elementary school since this is a period in which children with a typical development do not oppose to social, educational, and/or familiar rules, which makes the awareness of health risks and maintenance of healthy habits a successful action.
The low adherence of the parents to signing the FICF (CNS Resolution 466/12) was a limitation of this study. Of all forms delivered to the parents, we observed that only half returned signed. We were unable to verify if the documents were deli-vered to the parents, who were not interested in signing them, or if they were not even delivered to them by the students. It is extremely important to consider this observation in the design of future research projects, in which actions should be taken to clarify and raise awareness of students and parents or guardians about the purpose of the FICF.
The fact that we performed only a single intervention was another limitation of the study, since systematic and continuous actions are reported as fundamental to the success of programs for hearing loss prevention.
CONCLUSION
Despite most students having prior knowledge about hearing damages caused by high-intensity music, some still reported inadequate habits.
The educational lecture only led to significant changes in some of the elements investigated, reflecting a need to structure continuous actions for the target population, aiming at the prevention of hearing loss, mainly when considering adolescent school students. The inclusion of the school and the family in educative actions and the continuity of these actions are fundamental to effective changes in habits and attitudes in children and adolescents.
ACKNOWLEDGMENTS
To the students of the Pré-Iniciação Científica program at Universidade de São Paulo (USP), Layla Beatriz de Souza Silva and Fellipe Augusto Narcizo, and to the administration staff and teachers at Escola Estadual Ernesto Monte de Bauru, who contributed to the study’s implementation.
REFERENCES
1. European Comission, Scientific Committee on Emerging and Newly Identified Health Risks - SCENIHR. Potential health risks of exposure to noise from personal music players and mobile phones including a music playing function: preliminary report. Brussels: European Commisson; 2008 [citado 5 nov 2015]. Disponível em: http://ec.europa.eu/health/archive/ph_risk/committees/04_scenihr/ docs/scenihr_o_017.pdf
2. Biassoni EC, Serra MR, Hinalaf M, Abraham M, Pavlik M, Villalobo JP et al. Hearing and loud music exposure in a group of adolescentes at the ages 14-15 and retested at 17-18. Noise Health. 2014;16(72):331-41. http://dx.doi.org/10.4103/1463-1741.140515 3. Lee GJC, Lim MY, Kuan AYW, Teo JHW, Tan HG, Low WK. The
2014;55(2):72-7. http://dx.doi.org/10.11622/smedj.2014018 4. Gilles A, Van de Heyning P. Effectiveness of a preventive campaign
for noise-induced hearing damage in adolescents. Int J Pediatr Otorhinolaryngol. 2014;78(4):604-9. http://dx.doi.org/10.1016/j. ijporl.2014.01.009
5. Martin WH, Griest SE, Sobel JL, Howarth LC. Randomized trial of four noise-induced hearing loss tinnitus prevention interventions for children. Int J Audiol. 2013;52 Suppl 1:S41-9. http://dx.doi.org/10. 3109/14992027.2012.743048
6. Taljaard DS, Leishman NF, Eikelboom RH. Personal listening devices and the prevention of noise induced hearing loss in children: the Cheers for Ears Pilot Program. Noise Health. 2013;15(65):261-8. http://dx.doi.org/10.4103/1463-1741.113523
7. McNeill K, Keith SE, Feder K, Konkle AT, Michaud DS. MP3 player listening habits of 17 to 23 year old university students. J Acoust Soc Am. 2010;128(2):646-53. http://dx.doi.org/10.1121/1.3458853 8. Zocoli AMF, Morata T, Marques J, Corteletti LJ. Brazilian young
adults and noise: attitudes, habits, and audiological characteristics. Int J Audiol. 2009;48(10):692-9.
9. World Health Organization – WHO. Hearing loss due to recreational exposure to loud sounds: a review. Geneva: World Health Organization; 2015 [citado 5 nov 2015]. Disponível em: http:// apps.who.int/iris/bitstream/10665/154589/1/9789241508513_eng. pdf?ua=1/
10. Serra MR, Biassoni EC, Richter U, Minoldo G, Franco G, Abraham S et al. Recreational noise exposure and its effects on the hearing of adolescents. Part I: An interdisciplinary long-term study Exposición a ruido recreativo y sus efectos en la audición de los adolescentes. Parte I: un estudio interdisciplinario a largo plazo. Int J Audiol. 2005;44(2):65-73. http://dx.doi.org/10.1080/14992020400030010 11. Santos S, Morata TC, Jacob LC, Albizu E, Marques JM, Paini
M. Music exposure and audiological findings in Brazilian disc jockeys (DJs). Int J Audiol. 2007;46(5):223-31. http://dx.doi. org/10.1080/14992020601188575
12. Luz TS, Borja ALVF. Sintomas auditivos em usuários de estéreos pessoais. Int Arch Otorhinolaryngol. 2012;16(2):163-9. http://dx.doi. org/10.7162/S1809-97772012000200003
13. Liberman MC. Hidden Hearing Loss: Jackhammers, concerts and other common noisemakers may cause irreparable damage to our ears in unexpected ways. Scientific American. 2015;313(2):49-53. 14. Vogel I, Brug J, Ploeg CP, Raat H. Adolescents risky
MP3-player listening and its psychosocial correlates. Health Educ Res. 2011;26(2):254-64. http://dx.doi.org/10.1093/her/cyq091
15. Vogel I, Verschuure H, Ploeg CP, Brug J, Raat H. Adolescents and MP3 players: too many risks, too few precautions. Pediatrics. 2009;123:e953-8. http://dx.doi.org/10.1542/peds.2008-3179 16. Sliwinska-Kowalska M, Davis A. Noise-induced hearing loss. Noise
Health. 2012;14(61):274-80.
17. Sekhar DL, Clark SJ, Davis MM, Singer DC, Paul IM. Parental perspectives on adolescent hearing loss risk and prevention. JAMA Otolaryngol Head Neck Surg. 2014;140(1):22-8. http://dx.doi. org/10.1001/jamaoto.2013.5760
18. Weisz N, Hartmann T, Dohrmann K, Schlee W, Norena A. High-frequency tinnitus without hearing loss does not mean absence of deafferentation. Hear Res. 2006;222(1-2):108-14. http://dx.doi. org/10.1016/j.heares.2006.09.003
19. Borja ALV, Souza BF, Ramos MM, Araújo RPC. O que os jovens adolescentes sabem sobre as perdas auditivas induzidas excesso de ruído? Rev Ciênc Méd Biol. 2002;1(1):86-98.
20. Barcelos DD, Dazzi NS. Efeitos do mp3 player na audição. Rev CEFAC. 2014;16(3):779-91. http://dx.doi.org/10.1590/1982-0216201422112
21. Lacerda ABM, Soares VMN, Gonçalves CGO, Lopes FC, Testoni R. Oficinas educativas como estratégia de promoção da saúde auditiva do adolescente: estudo exploratório. Audiol Commun Res. 2013;18(2):85-92. http://dx.doi.org/10.1590/S2317-64312013000200006
22. Kim J. Analysis of factors affecting output levels and frequencies of MP3 players. Korean J Audiol. 2013;17(2):59-64. http://dx.doi. org/10.7874/kja.2013.17.2.59
23. França AG, Lacerda ABM. Promoção da saúde auditiva: estratégias educativas desenvolvidas por estudantes do ensino médio. Disturb Comun. 2014;26(2):365-72.
24. Blasca WQ, Picolini MM, Silva ASC, Campos K, Pinto GFR, Brasolotto AG et al. Projeto Jovem Doutor Bauru: capacitação de estudantes do ensino médio em saúde auditiva. Rev CEFAC. 2013;15(6):1407-17.
25. Blasca WQ, Correa CC, Picolini MM, Campos K, Silva ASC, Berretin-Félix G et al. Uma estrategia de teleducación sobre la salud auditiva y vocal en Brasil. Rev Logoped Foniatr Audiol. 2015;35(1):2-7. http://dx.doi.org/10.1016/j.rlfa.2014.05.002 26. Knobel KA, Lima MC. Effectiveness of the Brazilian version of the
Dangerous Decibels® educational program. Int J Audiol. 2014;53 Suppl 2:S35-42. http://dx.doi.org/10.3109/14992027.2013.857794 27. Böhm GM, Cruz OLM, Zanoni A, Zorzetto NL, Oliveira JAC, Sady
S et al. Homem virtual: audição [2 CD-ROM]. São Paulo: Faculdade de Medicina da Universidade de São Paulo; 2005.
28. Academia Brasileira de Audiologia – ABA. Portal Dangerous Decibels Brasil. [citado 5 nov 2015]. Disponível em: http://www. audiologiabrasil.org.br/ddbrasil/
29. Lacerda ABM. Audição no contexto da educação: práticas voltadas à promoção e à prevenção. In: Bevilacqua MC, Martinez MAN, Balen AS, Pupo AC, Reis ACMB, Frota S, organizadores. Tratado de audiologia. São Paulo: Santos; 2013. p. 549-70.
Appendix 1. Questionnaire: knowledge, habits, and attitudes of school students regarding exposure to amplified music
Identification form
Full name:
Age:
Grade: ( ) 6th ( ) 7th ( ) 2nd middle school
1. Do you use personal music players (MP3, MP4, cell phone) with earphones to listen to music?
( ) Yes ( ) No
2. In the scale below, mark the intensity with which you normally listen to music on your personal music player, 1 being a very low volume (soft)
and 10 being a very high volume (loud):
Very low volume (soft) 1__________________________________10 Very high volume (loud)
3. How many hours a day do you listen to music on your device?
( ) Fewer than 3 hours ( ) More than 3 hours
4. What type of earphones do you use more?
( ) Placed inside the ear (earbud) ( ) Placed outside the ear (supra-aural headphone)
5. After listening to music with earphones, have you ever noticed any of these symptoms?
( ) Tinnitus (noise inside the ear) ( ) Pain ( ) Dizziness ( ) Decreased hearing
( ) Sensation of a blocked ear ( ) No symptom ( ) Other:
6. Do you know what hearing loss is?
( ) Yes ( ) No
7. Do you believe that noises or very high sounds (loud) may damage hearing?
( ) Yes ( ) No
8. Do you think that listening to high sounds (loud) or being in environments with a lot of noise, such as concerts and parties, can cause hearing loss?
( ) Yes ( ) No ( ) I don’t know
9. Do you think that listening to loud/high music with earphones in a cell phone, MP3, or MP4 can cause any injury to the hearing?