jcoloproctol(rioj).2016;36(3):176–178
w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Case
Report
Inflammatory
cloacogenic
polyp:
a
rare
kind
of
benign
polyp
to
be
cured
with
endoscopic
and/or
surgical
removal
S¸
afak
Meric¸
Özgenel
∗,
Tuncer
Temel,
Evrim
Yılmaz,
Salih
Tokmak,
Ays¸egül
Özakyol
Eskis¸ehirOsmangaziUniversity,FacultyofMedicine,DepartmentofGastroenterology,Eskis¸ehir,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received11January2016 Accepted13April2016 Availableonline9May2016
Keywords: Inflammation Solitaryrectalulcer Cloacogenicpolyp
a
b
s
t
r
a
c
t
Background:Inflammatorycloacogenicpolypisaveryrarekindofbenignpolypwhichoccurs intheanaltransitionalzoneandlowerrectum.Thesepolypsariseinassociationwith var-iousconditions(e.g.,internalhemorrhoids,diverticulosis,colorectaltumors,andCrohn’s disease)inwhichmucosalinjuryistheunderlyingpathogenicmechanism.
Casereport:A24-year-oldmalepatientappliedtoemergencydepartmentwithbloody defe-cationforamonth.Apolypthatis1.5cminsizehadbeenobservedatrectumandanalverge junctionduringcolonoscopy,pathologicaldiagnosiswasinflammatorycloacogenicpolyp. Thereupon,colonoscopic polypectomywasperformedasthe malignanttransformation possibility.
Conclusion:Polypsoftheanorectaljunctionwithinflammatoryappearancemightbe inflam-matorycloacogenicpolypswithmalignanttransformationpotentialthatmustbetreated byendoscopicremovalorsurgeryandfolloweduproutinelywithcolonoscopicsurveillance. ©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Pólipo
cloacogênico
inflamatório:
um
raro
tipo
de
pólipo
benigno
a
ser
curado
por
remoc¸ão
endoscópica
e/ou
cirúrgica
Palavras-chave: Inflamac¸ão Úlceraretalsolitária Pólipocloacogênico
r
e
s
u
m
o
Experiência:Póliposcloacogênicosinflamatóriosconstituemumtipomuitorarodepólipo benigno,comocorrêncianazonadetransic¸ãoanaleretobaixo.Essespólipossurgemem associac¸ãocomdiversosdistúrbios(p.ex.,hemorroidasinternas,diverticulose,tumores colorretais,edoenc¸ade Crohn)nosquaisa lesãoàmucosaéomecanismopatogênico subjacente.
∗ Correspondingauthor.
E-mail:[email protected](S¸.M.Özgenel).
http://dx.doi.org/10.1016/j.jcol.2016.04.005
jcoloproctol(rioj).2016;36(3):176–178
177
Relatodecaso: Paciente,gêneromasculino,24anos,compareceuaoservic¸ode emergên-ciacomdefecac¸ãosanguinolentacomdurac¸ãodeummês.Duranteacolonoscopia,foi observadoumpólipomedindo1,5cmdediâmetronoretoenajunc¸ãodabordaanal;foi estabelecidoumdiagnósticopatológicodepólipocloacogênicoinflamatório. Subsequente-mente, foirealizada polipectomiacolonoscópica,diante dopotencialdetransformac¸ão maligna.
Conclusão: Pólipos da junc¸ão anorretal com aspecto inflamatório podem ser pólipos cloacogênicosinflamatórioscompotencialparatransformac¸ãomaligna,devendoser trata-dosporremoc¸ãoendoscópicaoucirúrgicaemonitoradosperiodicamentecomvigilância colonoscópica.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Inflammatorycloacogenicpolyp(ICP)isavery rarekind of benign polyp to be cured with endoscopic and/or surgical removal that was first described in 1981 by Lobert et al.1 Thesepolypsariseinassociationwithvariousconditions(e.g., internalhemorrhoids,diverticulosis,colorectaltumors,and Crohn’sdisease)inwhichmucosal injuryisthe underlying pathogenicmechanism.2 ICPsoccur intheanaltransitional zoneandlowerrectum.3AlthoughICPsaregenerallybenign, occasionalmalignanttransformationhasbeenreported.4
Werepresentacaseofcloacogenicpolyp,aninfrequently diagnosedtypeofpolyp,whichcauseslowergastrointestinal bleeding.
Case
report
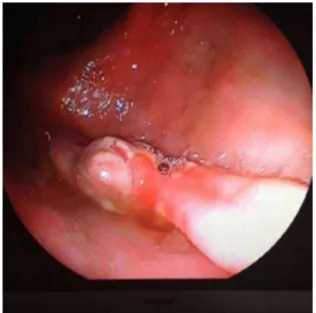
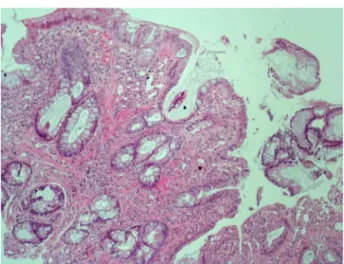
A 24-year-old male patient applied to emergency depart-ment with bloody defecation for a month. On laboratory analyzes, biochemistry panel, complete blood count, sedi-mentationand C-reactive protein was normal. Eitherfecal cultureorfecalanalysesforparasiteswerenegative.Apolyp thatis1.5cminsizehadbeenobservedatrectumandanal vergejunctionduringcolonoscopywhichwasperformedto determine the reason ofbloody defecation. (Fig. 1). In the pathologicalanalyzesofthepolyp,vesselswerestainedwith CD34andhistiocysteswerestainedwithCD68, fibromuscu-larfieldsinthelaminapropriawerestainedwithtrichrome, nofungal sporesor hyphaenutrientswere seenwith peri-odic acid schiff, there was no pathological feature with cyto-ceratin immuno-histochemical staining. The defining pathologicaldiagnosiswasICP;withulcers,minimal architec-turaldistortion,hyperplasticchangesandregenerativeatypia, fibromuscular hyperplasia in the lamina propria, and ves-selrichcolonicpolypoidtissues(Figs.2and 3).Thereupon, colonoscopicpolypectomywasperformedasthemalignant transformationpossibility.
Discussion
ICPsoftheanaltransitionalzonewerefirstdescribedin1981 byLobertPFandAppelmanHD.Rectalbleedingisthemost
Fig.1–Colonoscopicappearanceoftheinflammatory cloacogenicpolyp.
178
jcoloproctol(rioj).2016;36(3):176–178Fig.2–Elongated,irregularcryptstructures,hyperplastic changesinthelaminapropriafibromuscularhyperplasia andchronicinflammation(hematoxylineosine×100).
of116casesrevealedthatsolitaryrectalulcersmightalsobe foundcoexistingwithpolyps,ulcerativecolitis,hemorrhoids andcolonicmalignancy.6
ICPsaremorecommoninwomenusuallyoccurringfrom childhood to the fourth–the sixth decade of life.7,8 Lead-ing complaints are rectal bleeding, constipationand rectal tenesmus.8 Diagnosisisusuallyreachedbyendoscopyand biopsy.Itisdifficulttobedifferentiated from otherbenign andmalignantlesionsduringendoscopy.4 Thesepolypsare usually 1–5cm in the anorectal region and often sessile, and rarely occurs with pedincule. They may be single or multipleand canbefoundsimultaneous withhyperplastic oradenomatouspolyps.Anatomo-pathologicpropertiesare, erodedsurface,reactiveatypiaandhyperplasticchangeswith irregularbranchinginglandsandgranulationtissue.8,9
TransformationtosquamouscellcarcinomaforICP’sare mentioned.DysplasiawasdetectedincasesofParfittetal.4 andHansonandArmstrongfoundanalintraepithelial neo-plasia in his case.10 P53 and Ki67 immuno-histochemistry mustbeperformedtointerpretchallengingcasesby patholo-gists.Healsosimultaneouslydetectedthepresenceofhuman papillomavirus (HPV). Therefore,HPV screeningshould be consideredfortheICPbackground.
Fig.3–Increasedcollagenfibersandsmoothmusclefibers inthelaminapropriawithtrichrome(100×).
Ondifferentialdiagnosis,inflammatory,ischemicorother types ofpolyps,inflammatorybowel disease,Cowden syn-dromeandmalignanciesmustbeconsidered.8
Endoscopic removal orsurgical treatment isappliedfor treatment,2 patientsmusttakehigh fiberdietwith colono-scopic surveillance after polypectomyor surgical resection becauseoftherecurrencerisk.3
Inconclusion,itmustbebearinmindthatpolypsofthe anorectaljunction withinflammatoryappearancemightbe ICPs withmalignanttransformation potentialthatmustbe treatedbyendoscopicremovalorsurgeryandfollowedup rou-tinely withcolonoscopicsurveillance.CaseswithICPsmust beinvestigatedforunderlyingCrohn’sdisease,malabsorption syndromes,diverticulosis,hemorrhoids,adenocarcinomaand HPVinfection.Forpathologicaldiagnosisofchallengingcases immuno-histochemicalstainingcouldbebeneficial.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Thework conforms totheprovisions oftheDeclarationof Helsinki and the written consent ofthe subject has been acknowledged.
r
e
f
e
r
e
n
c
e
s
1.LobertPF,AppelmanHD.Inflammatorycloacogenicpolyp:a uniqueinflammatorylesionoftheanaltransitionalzone.Am JSurgPathol.1981;5:761–6.
2.TendlerDA,AboudolaS,ZacksJF,O’BrienMJ,KellyCP. Prolapsingmucosalpolyps:anunrecognizedformofcolonic polypsaclinicpathologicalstudyin15cases.AmJ
Gastroenterol.2002;97:370–6.
3.ZamanS,MistryP,HendrickseC,BowleyDM.Cloacogenic polypsinanadolescent:ararecauseofrectalbleeding.J PediatrSurg.2013;48:E5–7.
4.ParfittJR,ShepherdNA.Polypoidmucosalprolapsed complicatinglowrectaladenomas:bewaretheinflammatory cloacogenicpolyp!Histopathology.2008;53:91–6.
5.MadiganMR,MorsonBC.Solitaryulceroftherectum.Gut. 1969;10:871–81.
6.AbibS,KhawajaA,BhimaniSA,AhmadZ,HamidS,JafriW. Theclinical,endoscopicandhistologicalspectrumofthe solitaryrectalulcersyndrome:asingle-centerexperienceof 116cases.BMCGastroenterol.2012;12:72.
7.PoonK,MillsS,BoothL,MurphyS.Inflammatorycloacogenic polyp:anunrecognizedcauseofhematocheziaandtenesmus inchildhood.JPediatr.1997;130:327–9.
8.López-RamosCS,Rodríguez-GómezS,Bailador-AndrésC, Baizán-GarcíaMJ.Inflammatorycloacogenicpolyp:arare causeoflowergastrointestinalbleeding.RevEspEnfermDig. 2013;105:240–1.
9.MathialaganR,TurnerMJ,GorardDA.Inflammatory cloacogenicpolypmimickinganorectalmalignancy.EurJ GastroenterolHepatol.2000;12:247–50.
10.HansonIM,ArmstrongGR.Analintraepithelialneoplasiain aninflammatorycloacogenicpolyp.JClinPathol.