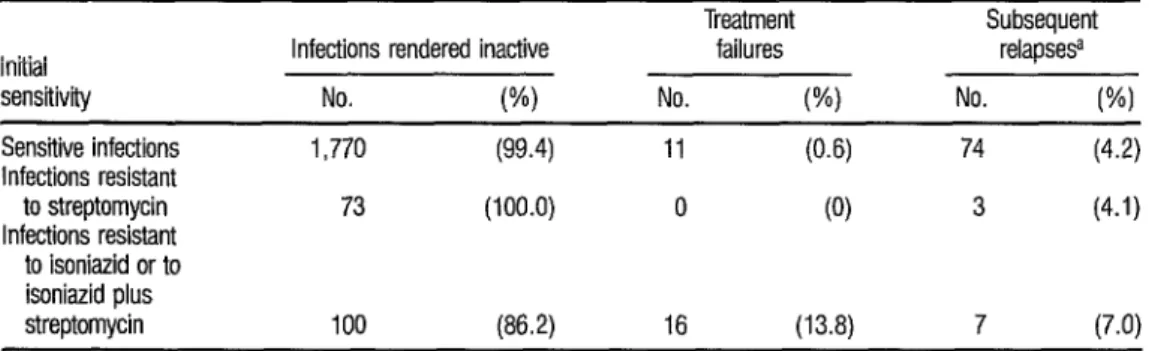
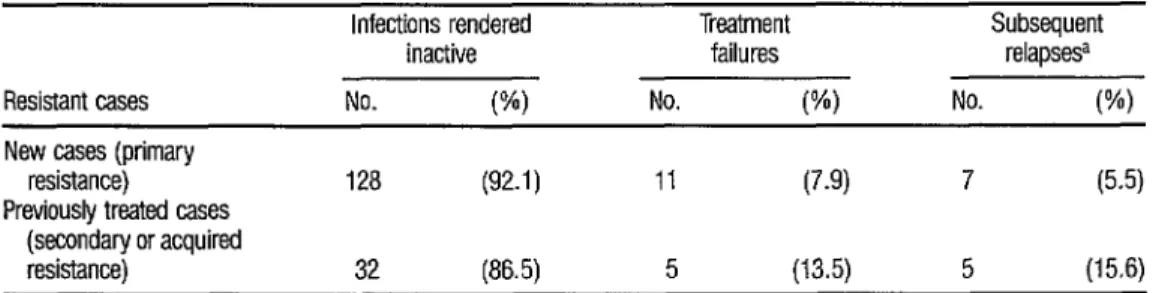
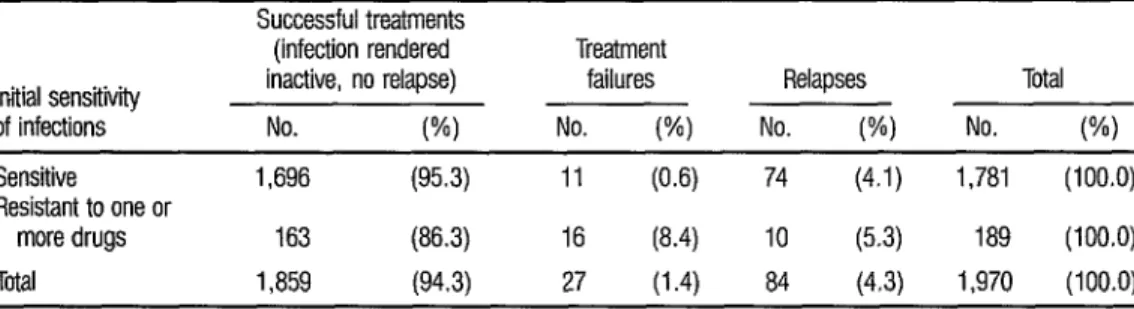
Response to short-course chemotherapy of patients with initial resistance to antituberculosis drugs
Texto
Imagem

Documentos relacionados
[...] resistência do aprendiz em tomar responsabilidade sobre sua própria aprendizagem; a ideia de que o professor dever ser o responsável pelas decisões sobre todos
To turn the Lyapunov exponent decay global our main ingredients will be a Kakutani tower scheme, the use of special flows isomorphic to our original dynamics, recurrence results to
However, the hospitalization of a child in a Pediatric Intensive Care Unit (PICU) because the family moments of anguish, suffering and despair 7 and experience a break
Desta forma, diante da importância do tema para a saúde pública, delineou-se como objetivos do es- tudo identificar, entre pessoas com hipertensão arterial, os
Regarding the type of response to previous treatment, patients for whom drugs were discontinued during treatment because of a lack of a response and individuals who had detectable
Patients with a prescription of three to four daily doses were 53% less likely to adhere (odds ratio of adherence to treatment (OR) = 0.47, 95% confidence interval (CI) 0.22-1.01)
(1996) found significantly higher numbers of globule leucocytes/mucosal mast cells in the intestinal mucosa in resistant than in susceptible lambs that were naturally infected
gloeosporioides in hypocotyls and green and ripe berries used by Orozco Miranda (2003) were different in some aspects in relation to field evaluations done in this
