.
Special Report
AIDS axnong Women in Latin America and
the Caribbean1
A
s the worldwide epidemic of AIDS continues, infection of women and their children with HIV virus is on the rise. The need to focus more strongly on this problem has drawn international at- tention (1). Among other things, in 1989 a global conference held in Paris on “Im- plications ofAIDS
for Mothers and Chil- dren” highlighted the special needs and concerns this problem poses; and World AIDS Day, 1 December 1990, was the- matically devoted to the problem of AIDS and HIV infection in women.The report presented here describes the epidemiologic character of the HIV epidemic among females in the Carib- bean and Latin America. However, the term “women” is generally used instead of the term “females” because cases oc- curring in young girls (less than 15 years old) are usually reported as pediatric AIDS cases without specification of gen-
‘This report will also be published in Spanish in the
Boletin de la Oficina Sanitaria Panamericana, Vol. 112, 1992. ’
2Regional Adviser on AIDS, PAHO.
3AIDS Information and Surveillance Officer, PAHO.
%enior Regional Adviser on AIDS and Sexually Transmitted Diseases, PAHO.
der. In addition, such cases represent a very small percentage of AIDS cases re- ported in the region.
DATA SOURCES AND ANALYSIS
Case reports received by the Pan American Health Organization (PAHO) between 1985 and 1990 were compiled and analyzed. These case reports had been procured through a system estab- lished in 1985 at the regional level that requires countries to submit quarterly re- ports on AIDS cases. Data in the quar- terly reports include the number of cases reported in the quarter; the cumulative number of cases and deaths; and a break- down of the cases reported in the quarter by age, sex, and attributed route of HIV infection. These data are compiled into a country-by-country quarterly report for the Americas that is distributed to all the countries for information-and for veri- fication of the data. (Verification has also been accomplished by phone or cable when inconsistencies between reporting periods appear.)
In addition to this case report data, cur- rent serologic information about HIV in- fection in the Americas was collected
from two other sources, the United States Census Bureau and country docu- ments forwarded to PAHO.
The U.S. Census Bureau has routinely collected published information on sero- surveillance worldwide as it has been published in scientific journals and pre- sented at international meetings. This in- formation is provided by the Census Bu- reau on a set of computer diskettes and is updated regularly.
PAHO also receives serologic informa- tion from country documents forwarded to it for other purposes-documents such as national AIDS program planning pa- pers and consultants’ reports. (Although PAHO has initiated quarterly reporting of HIV serosurveillance information, few reports have been received to date.)
RESULTS
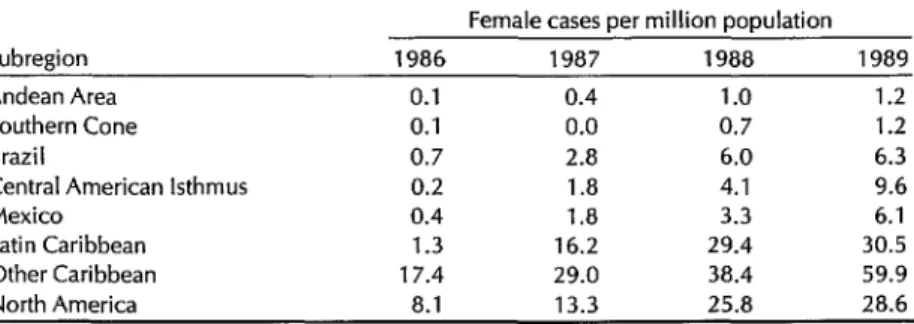
The total number of 1989 AIDS cases in women notified to PAHO by the coun- tries of Latin America was 891, indicating a rate of 5.84 AIDS cases per million women. An additional 579 cases were no- tified by the countries in the Caribbean, indicating a rate of 59.4 cases per million women there; and 5,279 cases were noti- fied in North America, indicating a rate of 28.6 cases per million women in that area (Table 1). Regarding high and low incidences among women in individual
countries for 1989, these ranged from a high of 607 cases per million women in Bahamas and 237 in Bermuda to a low of zero in Anguilla, Antigua, Bolivia, Cay- man Islands, French Guiana, Grenada, Guatemala, Montserrat, Nicaragua, Para- guay, and Virgin Islands (U.K.).
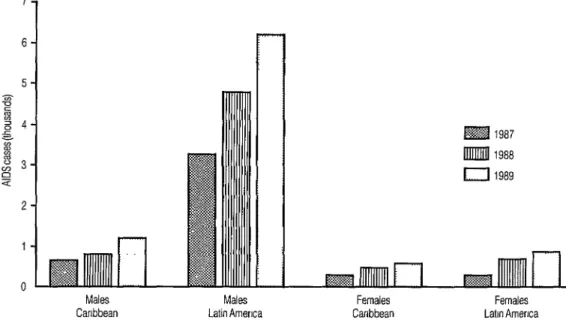
Overall, secular trends suggest that the AIDS incidence in women is increasing at about the same rate as in men within the Region of the Americas. Figure 1 shows the numbers of notified AIDS cases by sex in Latin America and the Caribbean for 1987,1988, and 1989. The evident pat- tern of steady increase is also visible, with respect to both case numbers and incidence, in all subregions where report- ing is complete. Indeed, as indicated in Table 1, the percentage increases in sub- regional case incidences from 1986 to 1989 has been dramatic, ranging from 244% in the non-Latin Caribbean (from 17.4 to 59.9 cases per million) to roughly 4,600% in Central America (from 0.2 to 9.6 cases per million). The percentage in- crease in North America during the same period was around 250%.
Part of this apparent increase could be due to improvements in case ascertain- ment and reporting as AIDS has become better known. However, countries where the epidemic is well established recorded similar increases over these years in the rate of AIDS cases among women. For
Table 1. AIDS cases among females in the Americas per million population, by
subregion, 1986-l 989.
Subregion Andean Area Southern Cone Brazil
Central American Isthmus Mexico
Latin Caribbean Other Caribbean North America
Female cases oer million oooulation 1986 1987 1988 1989
Figure 1. Reported cases of AIDS in the Caribbean (including the Latin Caribbean) and Latin America, 1987-l 989.
Males Males Females Females Canbbean Latin Amerrca Caribbean Latm America
example, in Brazil the number of AIDS cases reported among women rose from 72 in 1986 to 467 in 1989, and in the Do- minican Republic it rose from 24 to 186 in the same period. It is also noteworthy that the number of countries reporting no cases of AIDS among women declined from 16 in 1987 to 11 in 1989.
Heterosexual Transmission
In consonance with the increasing numbers of AIDS cases among women, available regional data point to a sharp apparent increase in the percentage of all AIDS cases attributable to heterosexual transmission. According to these data, the proportion of all annually reported AIDS cases attributed to heterosexual transmission rose from 19% in 1989 to 30% in 1990.
that although most AIDS cases among women in Mexico (66%) have been trans- fusion-related, nearly a third (31%) have been due to heterosexual transmission; only three cases or 0.5% were reported as being due to intravenous drug use (2). Also, available data from Brazil indicate that 34% of the AIDS cases in women in that country have been attributable to heterosexual transmission, 18% to blood transfusions, and 32% to intravenous drug use (3). Overall, it appears that while transfusion-related cases have long accounted for a considerable share of all cases among women, the recent increase could be related in some way to increas- ing heterosexual transmission. This mat- ter awaits further study and clarification.
4.F
Unfortunately, these regional data are In those countries reporting the age of not reported in such a
way
as to permit AIDS patients, the average age of female information on risk factors to be analyzed patients appears lower than the average by sex. However, Mexico has reported age of male patients. Specifically, it ap-Table 2. Cumulative numbers of AIDS cases, by age and sex, in five Latin Ameri- can and Caribbean countries where the age of AIDS patients has been reported consistently (Argentina, Bahamas, Barbados, Haiti, and Honduras). The figures shown do not include AIDS patients of unknown age.
Age
Wears)
O-14 15-24 25-34 35-44 45-54 55+
Total
No. 111
381 1,326 767 259 133 2,977
Males
Cumulative % %
3.7 3.7 12.8 16.5 44.5 61.0 25.8 86.8 8.7 95.5 4.5 100.0 100.0
No. 89
284 352 334 72 38 1,169
Females
Cumulative % %
7.6 7.6 24.3 31.9 30.1 62.0 28.6 90.6 6.2 96.7 3.3 100.0 100.0
pears that 27.5% of the females afflicted with AIDS are less than 25 years old, as compared to only 17.5% of the afflicted males. Table 2, which shows different fig- ures but the same trend, only includes data from countries where age has been reported consistently over time.
Pediatric Cases
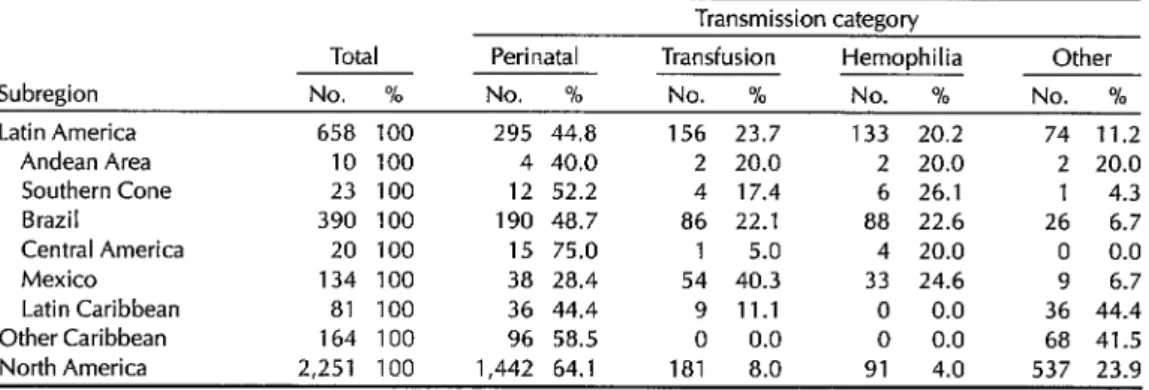
Increasing numbers of pediatric AIDS cases are also being reported in the Americas, of which a substantial share are attributed to perinatal transmission (Table 3). In Latin America, 295 (44.8%) of the 658 AIDS cases reported through 1989 in subjects under 15 years old were
attributed to perinatal transmission. In the Caribbean, 96 (58.5%) of 164 reported cases were attributed to perinatal trans- mission; and in North America, 1,442 (64.1%) of 2,251 reported cases were at- tributed to perinatal transmission. It is also noteworthy that 4.9% of all reported AIDS cases in the Caribbean (96 of 1,972 cases) have been attributed to perinatal transmission, as compared to lesser per-
centages in Latin America (1.4%) and North America (1.1%).
HIV Infection
Serologic information about HIV infec- tion is only now becoming the object of
Table 3. The number and percentage distribution of pediatric AIDS cases in various subregions of the Americas, by transmission category, through 1989.
Transmission category
Subregion Latin America
Andean Area Southern Cone Brazil Central America Mexico Latin Caribbean Other Caribbean North America
Total No. %
658 100 295 44.8 156 23.7 133 20.2 74 11.2 10 100 4 40.0 2 20.0 2 20.0 2 20.0 23 100 12 52.2 4 17.4 6 26.1 1 4.3 390 100 190 48.7 86 22.1 88 22.6 26 6.7 20 100 15 75.0 1 5.0 4 20.0 0 0.0 134 100 38 28.4 54 40.3 33 24.6 9 6.7 81 100 36 44.4 9 11.1 0 0.0 36 44.4 164 100 96 58.5 0 0.0 0 0.0 68 41.5 2,251 100 1,442 64.1 181 8.0 91 4.0 537 23.9
Perinatal
No. % No. %
Hemophilia
systematic surveillance throughout much of the Region (4). In parts of the Carib- bean and Central America, high sero- prevalence rates (as high as 35% in San Pedro Sula, Honduras, and 72% in Port au Prince, Haiti) have been found among women with high-risk behaviors, while much lower rates (O-1.2%) have been found among groups of low-risk women such as blood donors. Nonetheless, throughout most of the Region a majority of the women in high-risk groups (such as prostitutes) have remained uninfect- ed, and reports of seroprevalences over 10% among women practicing high-risk behaviors are the exception. Relatively few women at low risk (e.g., women at- tending maternity clinics for prenatal examinations) have been found to be infected. Only in Haiti has elevated sero- prevalence (9.7%) been documented among the latter.
DISCUSSION
These data lead one to conclude that AIDS cases among women are increasing throughout Latin America and the Carib- bean; that the routes of transmission pos- ing the greatest risks for women are blood transfusion and sexual contact; that the reported incidence of AIDS in Caribbean women currently exceeds that found among their North American counterparts; and that limited serologic data suggest women with high-risk be- haviors in some parts of Central America and the Caribbean have high prevalences of HIV infection.
A more thorough investigation of het- erosexual HIV transmission to women is being carried out in one country (Hon- duras) where AIDS cases among females have increased dramatically in the last three years. Initial assessment of 162 cases in women has revealed that 112 (69%) could not definitely be attributed to any risk factor (5). Of the remaining 50
cases identified with some risk factor, 32 (64%) occurred in women who reported receiving a blood transfusion within the preceding 10 years and 17 (34%) occurred in women who reported sexual contact with a male infected with HIV or at risk of HIV infection.
Since outside of some parts of Central America and the Caribbean most women, even in high-risk groups, re- main uninfected, an opportunity for ef- fective prevention and control still exists.
Of course, efforts to assess the num- bers of women with HIV infection or AIDS are not new. The Global Program on AIDS has published global estimates of HIV infection in women (6). The extent of the problem in the United States has been well quantified (7) and is routinely addressed in surveillance reports. (It is noteworthy that AIDS has been recog- nized as the leading cause of death among women 25-34 years of age in New York City-a.) Information from coun- tries other than the United States is sparser, though a recent report from the United Kingdom has detailed the situa- tion in that country (9).
Naturally, epidemiologic information is only as valuable as the public health re- sponse it provokes. Efforts at screening all blood transfusions are underway, but the impact such efforts can have on pre- venting AIDS among women has not been widely appreciated. In Latin Amer- ica and the Caribbean “a woman’s role has generally been defined as a bearer of children” (lo), and the major causes of maternal death are hemorrhage and abortion. Both of these conditions often require emergency transfusions. The blood screening efforts of most national programs are designed to include institu- tions serving women suffering from com- plications of pregnancy and childbirth. The success of such efforts seems des- tined to have a significant effect upon levels of HIV infection among women.
Despite the fact that transmission from
men to women is more efficient than transmission from women to men (lZ), serosurveillance efforts in many Latin American countries have emphasized re- peated mandatory testing of female pros- titutes. In this same vein, it is widely be- lieved that bisexuality is more common than homosexuality among men in Latin America. Given that the HIV seropreval- ence among homosexual males is higher than among any other group in the Re- gion (4), it is reasonable to suppose that contacts between bisexuals and homo- sexuals may be serving as a bridge in the process of HIV transmission to women (22). Hence, additional studies are needed to document the role of bisexual males.
Some additional factors raising the risk of HIV transmission to women are known from experiences elsewhere in the world, experiences that could be in- corporated into information campaigns in Latin America and the Caribbean. Among other things, anal intercourse ap- pears to increase the risk of transmission (23, 14). Also, coincident venereal dis- ease, which is often more occult in women than in men, tends to favor HIV transmission. Unfortunately, currently available data about venereal diseases in the Americas are minimal, and studies on the relationship between venereal dis- ease and transmission of HIV have not yet been published for this Region. In ad- dition, exposure to an infected partner is obviously a key factor in HIV transmis- sion, but few programs are in place that encourage women to request information about their partners’ HIV status or that promote the use of condoms when the partner’s status is unsure. The need for such interventions has recently been reit- erated (15). Clearly, all these potential areas for preventive interventions remain to be tapped in the fight against AIDS.
As already noted, women in the Amer-
icas appear to develop AIDS at an earlier age than men. Although most studies of the natural history of HIV infection have been carried out in men, and there is little
documentation of the natural history of the illness in women, it seems likely that earlier exposure to HIV rather than a dif- ferent course of the HIV infection, is causing the earlier age of cases observed. And, if exposure to HIV tends to occur at an earlier age among women, then edu- cational interventions directed at protect- ing women need to be carried out early, probably in early adolescence rather than adulthood.
Cases of AIDS in children are increas- ing. Total fertility rates and birth rates are higher in Latin America and the Carib- bean than in North America. Therefore, the heightened prevalence of AIDS cases among women in the Caribbean presages a considerable incidence of pediatric cases occasioned by perinatal HIV trans- mission in that area.
While the incidence of pediatric AIDS cases is higher in North America than in Latin America, a smaller percentage of pediatric cases in North America is attrib- uted to perinatal transmission than in Latin America. This supports the hypoth- esis that fertility is affecting the two areas’ HIV transmission patterns.
It is also worth noting that contracep- tive acceptance has been increasing throughout Latin America and the Carib- bean over the last 10 years. Within this context, the AIDS epidemic may change the type of contraceptives promoted for birth control. (What effect, if any, that oral contraceptives have on susceptibility to HIV disease is unclear-16.)
of AIDS in women climbing, the need for 9. information on such issues in Latin America and the Caribbean is becoming 10.
urgent; for it seems evident that in order to protect themselves and their children against AIDS, women wiU need the most
11 ’
complete and accurate information
possible.
12.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
Participants at AIDS conference decry lack of focus on diseases’ impact on 13 women. Med World News. 27 July . 1987;28(14):12.
Mexico, Direccidn General de Epidem- iologfa. Bolefin mensual SIDAIETS. 1991;5(1). 14. Bras& Mini&o da Safide. Bolefim Epidem- iolcjgico AIDS. 1991;3(9). (Epidemiological week ending 29 December 1990).
Pan American Health Organization. An- nual surveillance report: 1989; AIDS in the Region of the Americas. Washington, 15. DC: 1990.
Guereiia F, Rausch K. Trip report: initial assessment of AIDS in Honduras. United 16. States Centers for Disease Control, 1990. (Personal communication).
Chin J, Mann J. The global patterns and prevalence of HIV infection in women. 17. 1988. (GPAIWHO).
Guinan M, Hardy A. The epidemiology of AIDS in women in the United States, 1981-1986. JAMA. 1986;257:2039-42. 18. New York City, Department of Health. AIDS surveillance update. May 1988.
Jones L, Catalan J. Women and HIV dis- ease. Br J h’osp Med. 1989;41:526.
Fuenzahda H, LaVertu D. Women and AIDS. World health. (Submitted for publication).
AIfredo N. Different susceptibility of woman and man to heterosexual trans- mission of HIV San Francisco: VI Interna- tional Conference on AIDS; 1990. (Ab- strac t ThC 585).
Magis L, Garcia ML, Septilveda J, et al. Sexuality in women and AIDS in a Latin American country. San Francisco: VI In- ternational Conference on AIDS; 1990. (Abstract FC 591).
Melbye M, Ingerslev J, Biggar RJ, et al. Anal intercourse as a possible factor in heterosexual transmission of HTLV-III to spouses of hemophiliacs. N Engl J Med. 1985;312:857.
Benettuci J, Da Bouza J, Multare S, Corti M, Gomez CariIlo M. Risk of HIV hetero- sexual transmission in women from Buenos Aires City. San Francisco: VI In- ternational Conference on AIDS; 1990. (Abstract ThC 566).
Stein Z. HIV prevention: the need for methods women can use. Am J Public Heulfh. 1990.
Sumansen JN, Plummer FA, Ngugi EN, et al. HIV infection among lower socio- economic strata prostitutes in Nairobi. AIDS. 1990;4(2):139-44.
Batter V, et al. Fertility rates in HIV posi- tive women in Zaire. San Francisco: VI International Conference on AIDS; 1990. (Abstract FB 459).
Chin J. Current and future dimensions of the HIV/AIDS pandemic in women and children. Lancef. 1990;336(8709):221-24.
444