MESTRADO INTEGRADO EM MEDICINA VETERINÁRIA CIÊNCIAS VETERINÁRIAS
Approach to fetomaternal
disproportion in cattle
Comparison between Portuguese and Belgian realities
João André Gomes Pires
Orientador:
Professora Drª Rita Maria Payan Martins Pinto CarreiraCo-Orientador:
Dr. Miguel Nuno Pinheiro QuaresmaTutor na Bélgica:
Professor Dr. Geert OpsomerUNIVERSIDADE DE TRÁS-OS-MONTES E ALTO DOURO VILA REAL 2010
MESTRADO INTEGRADO EM MEDICINA VETERINÁRIA CIÊNCIAS VETERINÁRIAS
Approach to fetomaternal
disproportion in cattle
Comparison between Portuguese and Belgian realities
João André Gomes Pires
Orientador:
Professora Drª Rita Maria Payan Martins Pinto CarreiraCo-Orientador:
Dr. Miguel Nuno Pinheiro QuaresmaTutor na Bélgica:
Professor Dr. Geert OpsomerUNIVERSIDADE DE TRÁS-OS-MONTES E ALTO DOURO VILA REAL 2010
ii
iii
ABSTRACT
The aim of this study was to compare two distinct geographic areas on what concerns fetomaternal disproportion (FMD) in cattle, on both the incidence of the problem and the clinical approach to the situation. Therefore, were compared data collected during two periods of clinical training: in the Veterinary Hospital from Ghent University, Belgium and the Veterinary Hospital from the University of Trás-os-Montes and Alto Douro, Portugal. Although limited in time, the results showed that in Belgian FMD is a frequently found problem in Belgian White and Blue (BWB) beef cattle, known to be prone to this situation due to overdeveloped muscularity, and consequently owners are aware of the benefits of an early intervention. In Portugal, during the training period a relatively high proportion of dairy cows with FMD was found in comparison to beef cattle, which could be related to the fact that the beef cattle population found in Vila Real area is predominantly belonging to the Maronês breed and these animals usually present a larger birth canal than Holstein-Friesian cows, which facilitates parturition. The cesarean section is the method of choice for solving FMD situation in Belgium, while in Portugal vaginal forced extraction was the method most frequently used. Besides differences between breeds included in this study, may be that cultural differences between these two regions exists as main reasons for this difference, but the economic situation and the farm value for the cow-calf segment may also contribute for the differences. Nevertheless, it should be noticed that data obtained in Portugal refers to a very particular region in terms of cattle production, and these data should not be generalized to the all country.
iv
RESUMO
Este estudo teve como objectivo comparar a metodologia de acesso à situação clínica de desproporção feto-materna (FMD) em bovinos nas duas áreas geográficas em que decorreu o estágio clínico. Para isso foram comparados os dados recolhidos durante a estadia no Hospital Veterinário da Universidade de Gent, Bélgica, e no Hospital Veterinário da Universidade de Trás-os-Montes e Alto Douro, Portugal. Embora limitados ao período em estudo, os resultados mostraram que na Bélgica a desproporção feto-materna é um problema frequentemente encontrado em bovinos de carne de raça BWB, que se caracteriza pela sua hipertrofia muscular, pelo que os proprietários de animais desta raça estão conscientes dos benefícios de uma intervenção precoce. Pelo contrário, em Portugal, no período do estudo foi registada uma maior proporção de FMD em bovinos de leite, o que poderá estar relacionado com o facto da população de bovinos de carne encontrados na área de Vila Real ser predominantemente da raça Maronesa e estes animais apresentarem, normalmente, um canal pélvico mais amplo do que o de vacas Holstein-Friesian, o que facilita o parto. A cesariana foi o método de eleição para a resolução da desproporção feto materna na Bélgica, enquanto em Portugal a extracção vaginal forçada foi o método usado mais frequentemente. Este facto poderá ser em parte explicado pela diferente morfologia das raças que integraram este estudo. Por outro lado, as diferenças culturais existentes entre estas duas regiões podem ser apontadas como uma das principais razões para estas diferenças, tendo subjacente a situação económica e o valor do segmento Vaca-Vitelo na exploração. É no entanto de referir que os dados obtidos em Portugal se referem a uma região muito própria em termos de produção bovina, não podendo estes dados generalizar-se a todo o país.
v
INDEX
ABSTRACT ... iii
RESUMO ... iii
INDEX ... iv
LIST OF FIGURES ... vii
LIST OF TABLES ... vii
LIST OF GRAPHICS ... viii
LIST OF ACRONYMS AND ABBREVIATIONS ... viii
ACKNOWLEDGEMENTS ... x
1. Introduction ... 11
1.1. Fetomaternal disproportion ... 14
1.1.1. The predisposing factors ... 16
1.1.1.1 Fetal factors... 17
1.1.1.2. Maternal factors ... 19
1.2. Diagnosis ... 21
1.3. Approach to a situation of fetomaternal disproportion ... 23
1.3.1. The decision ... 23
1.3.2. Vaginally forced delivery ... 25
1.3.2.2. Cranial/anterior presentation ... 26
1.3.2.3. Caudal/posterior presentation ... 28
1.3.2.4. Epidural anesthesia ... 28
1.3.2.5. Uterine relaxation ... 29
1.3.3. Cesarean Section ... 30
1.3.3.2. Preparing the surgery ... 32
1.3.3.3. Sedation ... 32
1.3.3.4. Uterine relaxation ... 33
1.3.3.5. Preparation of the surgical area ... 34
1.3.3.6. Anesthesia ... 34
1.3.3.5.1. Local infiltration ... 34
1.3.3.5.2. Paravertebral injection ... 36
1.3.3.7. Choice of surgical approach ... 36
1.3.3.8. Surgical techniques ... 37
vi
1.3.3.7.2. Standing right paralumbar celiotomy ... 41
1.3.3.7.3. Standing left oblique celiotomy ... 41
1.3.3.7.4. Recumbent left paralumbar celiotomy ... 42
1.3.3.7.5. Recumbent right paralumbar celiotomy ... 42
1.3.3.7.6. Recumbent ventral midline celiotomy ... 42
1.3.3.7.7. Recumbent ventral paramedian celiotomy ... 42
1.3.3.7.8. Ventrolateral celiotomy... 43
1.3.4. Fetotomy ... 43
1.3.4.1. Cranial/anterior presentation ... 45
1.3.4.2. Caudal/posterior presentation ... 45
2. Material and methods ... 45
3. Results ... 48
4. Discussion ... 57
5. Conclusion ... 60
vii
LIST OF FIGURES
Figure 1 – Maternal and Fetal causes of dystocia ... 13
Figure 2 – Maternal and fetal factors involved in fetomaternal disproportion ... 14
Figure 3 – Comparison of the size of the calf to the birth canal size ... 23
Figure 4 – Washing the genital part of the cow for obstetric examination ... 23
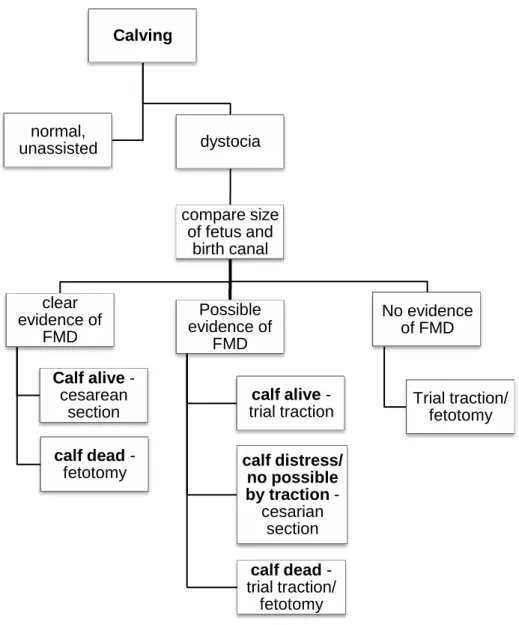
Figure 5 – Decision-making guidelines for FMD dystocia case treatment. ... 24
Figure 6 – Techniques to apply the ropes to the head (A) and limbs (B) of the calf ... 26
Figure 7 – Pelvic inlet (viewed from in front and somewhat below) ... 27
Figure 8 – Method to proceed to the epidural anesthesia ... 29
Figure 9 – Inverted L block local infiltration ... 35
Figure 10 – Way to insert the needle to perform the proximal (A) and distal (B) paravertebral anesthesia ... 36
Figure 11 – Technique to suture A – the uterus (Utrecht pattern); B – the skin ... 40
Figure 12 – Cuts for complete fetotomy in cranial (A) and caudal (B) calf presentation .... 44
Figure 13 – C-section procedure.1 ... 53
Figure 14 – C-section procedure.2 ... 53
Figure 15 – C-section procedure.3 ... 53
Figure 16 – C-section procedure.4. ... 54
Figure 17 – C-section procedure.5 ... 54
Figure 18 – C-section procedure.6 ... 55
Figure 19 – C-section procedure.7. ... 55
Figure 20 – C-section procedure.8. ... 55
Figure 21 – C-section procedure.9 ... 56
viii
LIST OF TABLES
Table 1 – Different dystocia scoring systems ... 12
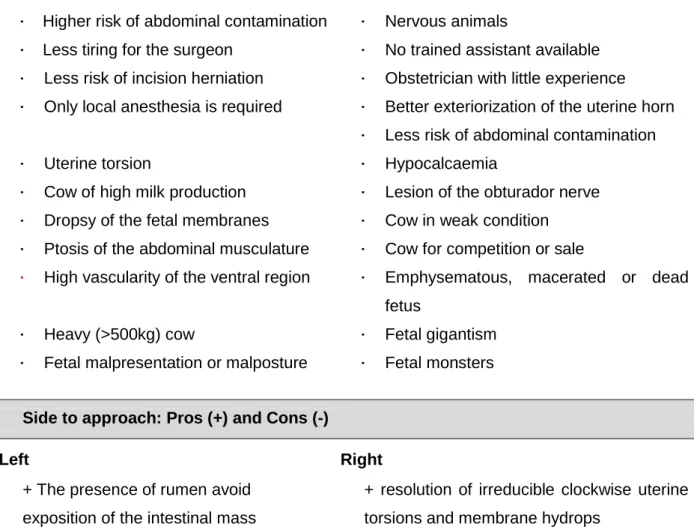
Table 2 – Choice of the surgical approach ... 37
Table 3 – Data distribution for the parameters “Time in labor”, “Cow general condition” and “Calf vitality” at arrival at the farm during the training period in Belgium and in Portugal. ... 48
Table 4 – Methodology used to solve the FMD, according to the breed ... 50
Table 5 – Drugs administered according to the selected technique and region of the training period. ... 52
LIST OF GRAPHICS
Graph 1 – Graphic representation of the parameters “Time in labor” (A), “Cow condition” (B) and “Calf vitality” (C) at arrival at the farm during the training period in Belgium and in Portugal. ... 49Graph 2 – Comparison of the used approaches for solution of FMD situations in Portugal and Belgium. ... 50
Graph 3 – Applied methodology in FMD situations according to the breed ... 51
Graph 4 – Distribution of FMD situations per breed ... 51
ix
LIST OF ACRONYMS AND ABBREVIATIONS
AI – artificial inseminationBWB – Belgian White and Blue BCS – body condition score cm – centimeter
cm2 – square centimeter C-section – cesarean section ° – degree
DM – double muscled € – euro
ECS – elective cesarean section FMD – fetomaternal disproportion G – Gauge
HCl – Hydrochloric acid
HVUTAD – Veterinary Hospital of the University of Trás-os-Montes e Alto Douro IA – intra abdominal IM – intramuscularly IU – international unit IV – intravenous kg – kilogram µg – microgram mg – milligram ml – milliliter
+/- – more and less NaCl – Sodium Chloride n – number of samples nº – number
% – percentage ™ – trade mark UK – United Kingdom
x
ACKNOWLEDGEMENTS
I want to thank to all those who throughout this journey believed in me. Special thanks and admiration for all that contributed to my technical and scientific skills at all levels.
I greatly acknowledge Prof. Dr. Rita Payan Carreira who always, through her commitment, drove me and helped me achieving this target.
To Dr. Miguel Quaresma, which I had the pleasure to trainee with at the Veterinary Hospital of The University of Trás-os-Montes and Alto Douro and that always shared his experience.
To Prof. Dr. Geert Ospsomer that gave me all the support during my stay in Belgium and that shared his wisdom while showing an enormous simplicity. To either all the residents, interns, trainee students, and auxiliary people with who I had the pleasure of share experiences during my trainee period both in Portugal and in Belgium, my acknowledgement.
I also thank to all my friends, both for long-standing as those with whom I shared these 6 years of academic life, those who will stay and will always be remembered.
To my parents, Valdemar and Joana, by their support that enabled me to realize this dream. To my grandparents with whom I love to share experiences during a long Sunday lunch. To my sister, Marta and my brother in law, Tiago for the way they patiently listen my stories and, of course to the new family member, my nephew Diogo. A special thanks to my aunt Maria by her inexhaustible availability. Besides these, to all my family members thank you.
Finally a very special acknowledge to someone very special. The one that was with me in the good but also in bad moments and that always, with all her love, believed in me and made me believe that this was possible, my girlfriend Raquel Carvalho.
All those who are living this moment with me, and everyone with whom I already lived many others
1. INTRODUCTION
Reproduction plays an important role in the entire economy of a cattle farm, whether it concerns the production of milk or meat. When we talk about reproduction we talk among other things about pregnancy, calving and calf survival and especially in dairy about milk production. The most frequent situation concerning parturition is a normal birth, defined as “eutocia”, but we can also have the opposite i.e. a difficult birth or “dystocia” and its diagnosis and treatment is important in veterinary practice (Ball and Peters, 2004; Jackson, 2004).
According to Mee (2008), the term dystocia comes from the Greek „dys’ meaning difficulty and „tocos’ meaning birth, and this situation may occur in many subjective cases and scales. Although no clear boundaries exist between eutocia and dystocia we can define dystocia as prolonged or difficult birth, when the first or the second stage of labor is prolonged and requires more assistance than desirable to deliver the calf (Noakes, 1997; Ball and Peters, 2004; Lopez de Maturana et al., 2007; Youngquist and Threlfall, 2007). We could wonder why dystocia is so important in the farm economy. Because it is the major factor in calf mortality at or near birth (Brinks et al., 1973; Laster et al., 1973; Bellows
et al., 1987). Martinez et al. (1983), in a study with Holsteins, found a mortality rate across
all parities about 6.65% but when the birth is classified in the most difficult category (score 5) 57% of all calves died and 27% in category 4. When looking for a uniform scale to classify dystocia we easily come to the conclusion that there is no consensus or standardized rules since various authors use different scoring systems like the examples shown in Table 1. Other scoring systems can be found in many reports (Bellows et al., 1971; Thompson et al., 1983; Djemali et al., 1987; Burfening, 1988; Naazie et al., 1989; Colburn et al., 1997; Dematawewa and Berger, 1997; Nix et al., 1998; Lopez de Maturana
et al., 2007; McGuirk et al., 2007), and may be helpful when approaching dystocia.
However, dystocia is also costly because it implies more labor, medication and losses among the cows (in production, delayed reproduction or decreased milk production) and therefore it significantly increases herd replacements which is economically unfavorable (Brinks et al., 1973; Djemali et al., 1987). This is also supported by Noakes et al. (2001), who defends the existence of numerous consequences for dystocia that will depend upon the severity, having unquantifiable effects on the welfare of dam and newborn and also financial consequences. According to this author, the consequences of dystocia are: increased stillbirth rate and mortality of the newborn, increased neonatal morbidity, increased mortality rate and reduced productivity of the dam, reduced subsequent fertility
and increased chance of sterility, increased likelihood of puerperal disease in the dam and increased likelihood of culling.
Table 1 – Different dystocia scoring systems
* - mentioned by Zaborski et al. (2009) References Jacobsen et al.
(2008)* Bellows and Short (1978) Martinez et al. (1983) Brinks et al. (1973) Johnson et al. (1988) Gradation score 1 to 3 1 to 4 1 to 5 1 to 6 1 to 8 Catego ri es 1
1 Unassisted Unassisted No problem
Surgery necessary Unassisted 2 2 Requiring light traction Assisted, pulled by hand or slight pull with obstetrical chains Slight problem
Difficult with aid of fetal extractor
Straightened calf's legs, but
calf delivered without assistance 3 3 Requiring heavy traction Difficult pull, usually with a mechanical puller Needed assistance
Easy with aid of fetal extractor Hand assistance for 5 min 4 4 Extreme difficulty, usually a C-section delivery or very hard pull with a mechanical puller Considerable force Aid necessary – no instruments used Hand assistance for 10 min 5 5 Extreme difficulty
Aid given but calving might have been successful without aid
Mechanical puller for 5 min 6 6 No difficult and no aid Mechanical puller for 10 min 4 7 Mechanical puller for 15 to 30 min 8 8 C-section
There are many factors that can contribute to dystocia and for a better understanding of these factors they are usually divided in two groups: maternal or fetal factors (Figure 1) (Ball and Peters, 2004; Jackson, 2004; Youngquist and Threlfall, 2007).
Figure 1 – Maternal and Fetal causes of dystocia (Noakes et al., 2001; Ball and Peters, 2004; Jackson, 2004; Youngquist and Threlfall, 2007)
However, in spite of all the factors that might cause dystocia, one stands out as the primary cause of bovine dystocia: the fetomaternal disproportion (Colburn et al., 1997; Noakes, 1997; Jackson, 2004; Mee, 2008). Fetomaternal disproportion(FMD) is not only a factor by itself but a relationship between maternal and fetal factors and can be defined as an obstruction of calf expulsion originated by the calf size/birth weight or pelvic dimensions of the dam, that may have several factors in its origin (Figure 2) (Noakes, 1997; Mee, 2008).
Nevertheless, when looking for just one factor, derived either from the dam or from the calf, many authors mentioned that calf birth weight is the most important factor affecting calving difficulty (Bellows et al., 1971; Laster, 1974; Johnson et al., 1988; Naazie
et al., 1989; Colburn et al., 1997; Zaborski et al., 2009). Johanson and Berger (2003), cited by Zaborski et al. (2009), found that in Holstein cows the probability of dystocia increases
Maternal causes
Failure of
expulsive forces
Uterine (inertia [1st or 2nd degree], calcium deficiency, torsion, damage) Cervix (fails to dilate, fibrosis, congeni tal defect) Abdomi nal inability to strain (pain, debility, age)Anatomical
(birth canal)
abnormalities
Pelvis (area too small, fracture, exostos es) Over -fat Reprod uctive tract (conge nital defects of vulva and vagina)Fetal causes
Oversize
Relative Absolute (sire breed, prolonged gestation, monsters, calf birth weight)Disposition
Presentation - anterior - posterior Position - dorsal - ventral - lateral -oblique Posture - Flexed or devieted limbs - devieted head Twinsby 13% for each 1kg increase in calf birth weight, whilst Nix et al. (1998) observed a 0,2% increase in dystocia per each 1kg increase in calf birth weight in beef cattle. Laster et al. (1973) reported an increase of 2,3% in calving difficulty for each 1kg increase of birth weight in Hereford and Angus cattle.
Figure 2 – Maternal and fetal factors involved in fetomaternal disproportion (Jackson, 2004; Mee, 2008)
Rice and Wiltbank (1972), in a study with primiparous Hereford females, found an incidence of dystocia of 68,7% in cows with a pelvic area less than 200 cm2 when compared with 28% in cows with a pelvic area above this value, thus also demonstrating the importance of the pelvic area as a predisposing factor for dystocia.
1.1. F
ETOMATERNAL DISPROPORTIONIn cattle, it has been estimated that 46% of all cases of dystocia are caused by fetomaternal disproportion (Noakes et al., 2001). As already mentioned, this can result from a disproportion between maternal and fetal factors and can have considerable variation in degree (Noakes et al., 2001; Jackson, 2004; Mee, 2008). Some breeds, like the double muscular (DM) breeds, are more predisposed for dystocia than other cattle breeds. The higher incidence of dystocia in this kind of breeds, such as the Belgian-White-Blue (BWB), is thought to be originated by the particular conformation of the calf and the reduced size of the pelvic opening of the dams. In other words, by a fetomaternal disproportion (Arthur et al., 1988; Arthur et al., 1989; Kolkman et al., 2007). In this breed the over-developed muscular condition is caused by the absence of an 11 nucleotides segment in the myostatin gene and consequently to an un-restrained development of the muscles (Grobet et al., 1998; Lips et al., 2001; Kolkman et al., 2007). However this is not the only breed where this mutation exists, and other beef breeds like Parthenaise, Asturian
Fetomaternal
disproportion
Calf size/birth
weight
Gestation length, parity, sire, breed, nutrition of the dam,
climate, calf sex
Pelvic
dimensions of
the dam
Parity, weight at service, age and condition at calving,
and Red Galician are reported to have the same situation. In other breeds, like the Charolais, Maine Anjou, Piedmontese and Gasconne a mutation that “turn-off” the myostatin gene has been found, predisposing for extreme muscularity and fetomaternal disproportion. Despite this, several causes of excessive muscular development are possible (Lips et al., 2001). Arthur et al. (1988) found an incidence of dystocia of 19% in DM cows in comparison to just 6% in the control cows. In the same study, authors also found a smaller pelvic area in DM cows in comparison to the controls (289,9 cm2 and 306,5 cm2 , respectively). Hence, in such cases, the DM cow is not able or has a greater difficulty to deliver the calf without help since the second stage of labor is potentially compromised. When normal delivery within 2 hours is not achieved, the dam has been straining unproductively and if no good assistance will be given, the calf will die and there will probably follow severe consequences for the dam (Noakes et al., 2001; Jackson, 2004).Hoyer et al. (1990), cited by Uystepruyst et al. (2002), defend that Cesarean section (C-section) is the preferred obstetrical method to deliver calves in severe fetomaternal disproportion. The other methods to solve these cases are the forced extraction when vaginal delivery is considered to be possible and the fetotomy when the calf is dead and can be reached per vaginam. However, some clinicians around the world have lost the skills to perform a fetotomy because of the greater ease and increased effectiveness of C-section (Noakes et al., 2001; Uystepruyst et al., 2002; Jackson, 2004).To avoid the losses associated to a late detection of dystocia, in Belgium, where the BWB breed is the predominant beef breed, and because both farmers and veterinarians are aware of the high incidence of FMD in the BWB, C-section became an elective operation (ECS) (Kolkman et al., 2007). Anticipating the calving problem through this elective procedure, Michaux & Leroy (1997) and Detilleux (2000) [mentioned by Uystepruyst et al. (2002)] found that the neonatal survival rate in the BWB breed is higher than during vaginal deliveries, and now in Belgium 90% of the BWB calves are delivered by ECS with no traction attempts at all. Lips et al. (2001) referred that a considerable number of C-section in BWB in Belgium are not performed for biological but for economic reasons. They support their suggestion in the fact that the cost for this surgical procedure varies between 70€ to 85€ and the high value of the calf that, depending on the gender and the year among other factors, can yield from 500€ to 1000€. Therefore, the farmers do not want to take any risk to lose the calf because of a difficult calving and they ask for an ECS already in the earliest stages of labor (Lips et al., 2001; Kolkman et al., 2007). It is also mentioned that the degree of traction before the surgery is performed, is one of the major factors that determines the outcome both for the calf and the dam in cases of C-section, and this is one additional reason why farmers ask for ECS (Noakes et al., 2001). On the other hand, with the use of new and safer anesthetic drugs, C-section should not be considered like a
last resort but as a useful method of treating several cases of dystocia (Noakes et al., 2001). Nevertheless, according to Uystepruyst et al. (2002) the timing to perform this ECS is very important as it can influence the pulmonary function of the calves, among other things, and so the veterinarian should wait for full cervical ripening in order to avoid respiratory disease of the newborn, which is the most frequent cause of death in BWB calves.
Although ECS can reduce the losses derived from this kind of dystocia in cullard breeds, some authors consider this as an unethical procedure and thus claim that it should be avoided. Clinicians should also alert the farmers in order to prevent this kind of dystocia providing an adequate size of the birth canal of the dam and select for calves with size and conformation that can pass the birth canal (Noakes et al., 2001).
Drew (1986-87), referred by Noakes et al. (2001), proposed some guidelines to breed Holstein Friesian in UK in order to avoid this kind of dystocia. His guidelines were:
management measures at service: in the 80‟s decade it was advise to achieve a body weight above 260kg and the good choice of sire (both for AI and natural service); nowadays a limit body condition score at service of 2.75 to 3 is the goal; management measures before calving, including adequate nutritional level in order
to avoid over-fatness of the calf, restriction of energy intake during the last 3 weeks of pregnancy to avoid over-condition of the dam when lactation starts, check for depletion of iodine and selenium, ensure supplementary magnesium, provide an adequate exercise area and check the pregnant cows at least 4 times a day in the last 3 weeks;
management at calving that includes, among other things, providing the calving cow with a familiar place and watch the cow hourly during calving.
1.1.1. The predisposing factors
As was mentioned above, many factors influence the proportion between the calf size or his birth weight and the pelvic dimensions of the dam. The more important ones will be reviewed herein with a particular focus on how they influence the fetal or the maternal component (fetal factors and maternal factors, respectively).
1.1.1.1 Fetal factors
The gestation length is probably the major factor influencing the calf birth weight (Mee, 2008).The gestation length seems to be breed-dependent. With an average length of 283 days, it varies from an average of 279 days in Holstein Friesian to 287 days in Charolais (Barkema et al., 1992; Noakes et al., 2001; Jackson, 2004; Mee, 2008; Zaborski
et al., 2009). In late pregnancy, the weight of a calf may show a daily gain of 0,5kg
(Jackson, 2004) though this value varies between authors, as Holland and Odde (1992) refer that in beef calves the daily gain is between 0,1 to 0,25kg/day. Other authors also mentioned a steep increase of the fetal long-bone length (Jackson, 2004). Longer pregnancies can also be associated with developmental abnormalities, such as adrenal cortex hyperplasia, which can delay the onset of parturition. In addition, male calves and winter time have also been associated with longer pregnancies (Noakes et al., 2001). Nevertheless, Holland and Odde (1992) refer that gestation length is more accurately a function of birth weight than the opposite because it seems that the onset of parturition is dependent of fetal hypothalamic-hypophysial-adrenal axis. This opinion was supported by the studies of Bellows et al. (1971) who found that when the birth weight is constant there is no effect of gestation length on the occurrence of dystocia (Bellows et al., 1971; Noakes
et al., 2001).
Another predisposing factor for dystocia can be the parity of the dam. Apparently, the bigger the dam, the bigger the calf (Noakes et al., 2001; Zaborski et al., 2009), as it was reported by Colburn et al. (1997), who found that the birth weight of a second calf is greater than that of the first calf. Additionally, parity also influences the gestation length (Mee, 2008).
The sire might influence the occurrence of dystocia because they can affect the size and birth weight of calves and the pregnancy length, in a way that vary with the breed and the sire‟s genetic line (Holland and Odde, 1992; Colburn et al., 1997; Noakes et al., 2001; Zaborski et al., 2009). The experiments by Laster et al. (1973) showed a sire effect over the calving difficulty in both male and female calves, but being more pronounced in male calves. On the contrary, Nelson and Huber (1971) [cited by Laster et al. (1973)] didn‟t find a significant sire effect in their study whereas Sagebiel et al. (1969) [cited by Laster et
al. (1973)] referred that sire only affected dystocia in male calves.
Some breeds have a tendency for increased gestation length and for bigger or heavier calves in proportion to the maternal pelvic area. Consequently, these breeds typically appear on surveys with higher incidences of dystocia when compared with other breeds, like 6% in Holstein Friesian, 9% in Charolais or 80% in Belgian Blue heifers (Holland and Odde, 1992; Jackson, 2004; Zaborski et al., 2009). According to Laster
(1974) the breed exerts a significant effect on the percentage of dystocia, which is probably related with calf anatomy. For Heins et al. (2006) [cited by Zaborski et al. (2009)] crossbred calves may reduce the incidence of dystocia, as a result from heterosis.
Nutrition of the dam: when the dam is in poor condition, from being poorly fed, they deliver low viability calves, whilst overfed dams tend to deliver oversized or weighted calves. Both situations increase the risk of dystocia (Noakes et al., 2001; Jackson, 2004). Grunert (1979), cited by Mee (2008), defend that overfeeding the dam during the last trimester can result in fetal oversize leading to dystocia.
However the effects of maternal nutrition on calf birth weight remain a controversial topic, Holland and Odde (1992) reported that energy and crude protein intakes during the last half of the gestation might alter birth weight although with variable effects. On the other hand, Laster (1974) refers that even if higher levels of energy in the last trimester of pregnancy increased calf birth weight (due to an increase in soft tissue) in the Hereford and Angus breed, it did not significantly affect dystocia. In contrast, it has been found that older cows and heifers fed above standard levels became obese but didn‟t exerted any effect on calf birth weight (Meijering, 1984), whilst Bellows and Short (1978) reported that FMD is derived from fat deposits in the birth canal that consequently reduce its dimensions.
Some effects have been attributable to the climate: the season of the year and some environmental factors, like air temperature and wind chills, have been shown to influence calves‟ birth weight (Colburn et al., 1997; Noakes et al., 2001).Heavier calves of about 4.5kg are expectable in spring, after severe winter temperatures (Colburn et al., 1997), what may be due to an increased blood flow to the uterus during cold winters, with subsequent increase in the nutrient supply to the fetus, resulting in an increased birth weight (Holland and Odde, 1992; Colburn et al., 1997). Colburn et al. (1997) also defend that heifers consume more hay during colder winters that further increases the supply of nutrients to the fetus. These authors also state that December, January and February are the months with the greatest effect on fetal grow (Colburn et al., 1997; Johanson and Berger, 2003). Increased thyroid hormone concentration, increased gestation length and reduced plasma oestradiol concentrations were also found to be associated with the colder months, and might also lead to increased birth weight (Mee, 2008). Several other authors registered the calving of heavier calves in spring than in fall, and associated that fact to lower temperatures during the pregnancy (Holland and Odde, 1992).Because of the effect of climate factors on birth weight, we can expect differences in calf‟s birth weight among geographic localities (Holland and Odde, 1992).
The calf sex was the earliest factor recognized to influence birth weight (Holland and Odde, 1992). Irrespective of breed, male calves are usually heavier than female ones,
and frequently also have longer gestational periods, which as mentioned above can also lead to bigger or heavier calves (Bellows et al., 1971; Brinks et al., 1973; Laster et al., 1973; Meijering, 1984; Noakes et al., 2001; Jackson, 2004; Mee et al., 2009; Zaborski et
al., 2009). In Holstein cattle, Kertz et al. (1997) found an average increase of 8,5% in
weight of male calves in comparison to female calves. Johanson and Berger (2003) reported an increased probability of dystocia for the male fetus when compared to the female, the former reaching 25%. In the opinion of Mee (2008) not only the weight but also the calf morphology can contribute for increase risk of dystocia associated to male fetus. However, there is not much evidence to support this proposal (Meijering, 1984).The study from Nix et al. (1998) failed to demonstrate a significant contribution of calf sex to dystocia. In that study birth weight and calf sex might have worked as co-dependent parameters, as stated by the authors, whereas a clear association was found between male birth weight and dystocia. In a study with Hereford and Angus, Bellows et al. (1971) describe that calf sex is ranked second in importance of the factors attributable to the calf in incidence of dystocia.
1.1.1.2. Maternal factors
The parity of the dam can influence the “functional” pelvic area and thus dystocia (Nix et al., 1998; Mee, 2008). Lindhé (1966), mentioned by Noakes et al. (2001) postulated that the younger the heifer, the higher is the dystocia rate. A higher incidence of dystocia is reported for first calving heifers (Jackson, 2004).Mee et al. (2009), comparing the dystocia rate in primiparae versus pluriparae found the percentages of 9,3 and 5,8%, respectively, concluding that this might be due to immaturity and incomplete development in young heifers, being plausible to assume the ratio between calf size and pelvic dimensions to be more critical in primiparae than in pluriparae cows (Meijering, 1984). According to Johanson and Berger (2003) the probability of dystocia in Holstein heifers is 4.7 times higher than in Holstein cows. In the study by Sieber et al. (1989) it has been demonstrated that calving difficulty decreases as parity increases, and these authors found the frequencies of 52% dystocia for the first calving, 20% for the second, 17% for the third and fourth, and 14% for more than five parities – so, two or three times higher in first than in others parities.
Such as parity, weight of the dam at service can influence the effective pelvic area and thus dystocia (Mee, 2008). Postpone breeding until the cow reaches 400kg of body weight has reduced the incidence of dystocia in Holstein Friesian heifers (Jackson,
2004), but Mee (2008) refers that the current Teagasc target in the Dairy Business and Technology Program in Ireland, for Holstein Friesian heifers‟ weight at service is 325-350kg or 55-65% of mature body weight at 15 months.With this increase in body size and weight targets at service, the pelvic diameter and area will also increase, decreasing the predisposition for dystocia caused by FMD (Jackson, 2004).
Age at calving: most authors agree that more calving problems derived from FMD may be expected in heifers calving at a younger age than in mature cows (Meijering, 1984; Jackson, 2004; Mee et al., 2009). Gregory et al. (1992) estimated that 2 years old beef cows needed more than twice often assistance than cows being more than 3 years old. In beef cows, experiments by Newman et al. (1993) showed a rate of dystocia of approximately 12%, 2%, 0,3%, and 0,5% in 2,3,4 and 5 years old cows respectively. Also other authors have found increased rates of dystocia in 2 years old cows (Brinks et al., 1973; Laster et al., 1973). This may be due to poor pelvic development that can be found in 2 years old heifers which often is not fully compensated by a smaller calf (Laster et al., 1973; Meijering, 1984; Holland and Odde, 1992). The age of the cow at calving interferes with calving ease not only directly through its size but also by influencing the size of the calf (Zaborski et al., 2009). Klassen et al. (1990), cited by Zaborski et al. (2009) verified that older cows at first calving are usually considered to have easier calving even when the body weight is taken in account. In Simmental cattle, Burfening (1988) found an age-related decrease in the percentage of calving requiring assistance, and linked this effect to an increase in the physiological maturity of the dam and to their increase in body size. However, in other studies, although the probability of an assisted calving increases in primiparae calving at younger ages, this effect is small (Mee et al., 2009). A statistical relationship between age at first calving and dystocia was difficult to be demonstrated in such studies, probably due to an adequate target age of 24 months at calving, beyond a 85-90% of mature body weight (Mee et al., 2009). Meijering, (1984) reinforces the idea that the effect of age at first calving has to be considered against the maturity of each breed at a particular age. Taking this in to account, specific management measures to ensure adequate size or maturity of the dam at calving should be implemented, since pregnancy in immature heifers and consequently dystocia due to FMD can be considered as a welfare problem (Burfening, 1988; Borsberry, 2006).
The condition of the dam at calving is a major factor in dystocia. Generally, over-weighted heifers will have a substantial amount of retroperitoneal pelvic fat (excessive adipose deposit in the birth canal) that reduces the size of the birth canal and so are more prone to suffer from FMD than cows with a moderate or poor body condition (Meijering, 1984; Noakes et al., 2001; Mee, 2008). However, Spitzer et al., (1995) failed to demonstrate a correlation between body condition score (BCS) and dystocia, but in their
study they only compared heifers in mid-status condition (scores of 4, 5 and 6 in a scale from 1 – emaciated to 9 – obese). Commenting this study, Noakes et al. (2001) defend that those results cannot be extrapolated to extremes BCS. Mee (2008) mentions that the currently used Teagasc target for body condition score is 2.75 – 3.0 (on a 1 to 5 points scale) for primiparae at calving or 540 – 570kg being 85 – 90% of mature body weight at 24 months.
Genetics also influences the incidence of FMD in cattle. Beef cows experience significantly more dystocia than dairy cows (Zaborski et al., 2009).Laster´s studies (1974) demonstrated the existence of differences in pelvic size among different breeds that seemed to be due to differences in cow body weight, although a tendency for larger pelvic openings in larger cows was found. This author also observed that pelvic width, influenced by breed, determined dystocia rate to a large extent (Laster, 1974). Studying nine different beef breeds, Kriese et al. (1994) verified that Hereford cows had the smallest pelvic height, width and area, whereas Braunvieh had the largest pelvic width and Charolais the largest pelvic height and area. It was also found that 2 years old Limousine cows had the easiest calving while the Pinzgauer heifers had the most difficult ones. In contrast, Gregory et al. (1992) found the lowest incidence of dystocia in the Angus breed whereas the highest was found in Braunvieh heifers and Pinzgauer cows. Laster et al. (1973) comparing the calving ease between Angus and Hereford breeds, found that Hereford females had more difficulty at calving than the Angus.
1.2. D
IAGNOSISThe diagnosis of dystocia is based on the history and physical examination (Momont, 2005). In cases of FMD vaginal examination is often difficult. However, when called for acting on a dystotic labor, one must remember that all kinds of dystocia are possible, and that during clinical approach, some steps must be followed. Therefore, when called, a brief history of the case should be asked to the owner (Jackson, 2004). Upon arrival at the farm this information is completed by inquiring for additional details about the clinical history to obtain as much pertinent history as possible and this should include:
- the expecting calving date (gestation length); - information about the sire;
- if the cow is first calving or not, and, if pluripare, if previous calving evolved easily - for how long is the cow in labor;
- if some assistance has been given so far, and which measures were undertaken.
Some other questions about the recent health of the cow should also be asked (Noakes et al., 2001; Jackson, 2004; Momont, 2005; Youngquist and Threlfall, 2007) before starting the clinical examination, focusing on the following:
- physical condition and BCS of the cow; - is the cow standing or recumbent; - brief physical examination;
- if there are any membrane or fetal part visible in the vulva; if so, identify the membrane and its condition or the fetal presentation and position;
- is there any vaginal discharge that may indicate, for example, fetal death (Noakes
et al., 2001; Jackson, 2004; Youngquist and Threlfall, 2007).
Afterwards, one should follow to the obstetric examination per vaginam, where cleanliness and lubrication should prevail. The clinician must estimate the size of the fetus relative to the size of the maternal pelvic inlet and birth canal (Figure 3) and determine the fetal presentation. Palpation of the limbs and head of the calf may give some indications of the size. In addition, slight traction of the fetus in normal presentation and position can be tried to test for calf delivery. If the disproportion is confirmed, the diagnosis is dystocia by FMD. (Jackson, 2004; Drost, 2005; Momont, 2005; Kolkman et al., 2007; Youngquist and Threlfall, 2007).
After washing the genital parts of the cow (Figure 4) and the arms and hands of the obstetrician, the internal examination starts. During this examination the vagina, vulva and the uterus should be checked for possible injuries, to ascertain the dilatation of the cervix and finally the position, viability and size of the calf (Noakes et al., 2001; Jackson, 2004; Drost, 2005; Momont, 2005; Kolkman et al., 2007; Youngquist and Threlfall, 2007).When stenosis of the cranial vagina is detected during the vaginal examination, a rectal examination is also indicated to confirm the existence of uterine torsion. (Youngquist and Threlfall, 2007)
If the obstetrician suspects an FMD the vaginal examination continues with a lubricated hand to feel the parts of the calf near the pelvis of the mother, and then must be moved in a circular fashion around the calf in order to estimate the space between the calf and pelvis.
In some situations, like the mother being clearly young, it may be immediately obvious that the calf will be too big to be delivered per vaginam. (Jackson, 2004).
Figure 3 – Comparison of the size of the calf to the birth canal size (from Jackson, 2004)
Figure 4 – Washing the genital part of the cow for obstetric examination
1.3. A
PPROACH TO A SITUATION OF FETOMATERNAL DISPROPORTION1.3.1. The decision
In case of FMD, three resolutions may be possible: forced extraction, C-section or fetotomy. Each case being unique, a decision should be made on the best option.
In a FMD situation, a decision about how to extract the calf based on the fetal presentation and the free space resulting from the comparison between the fetal size and the size of the birth canal evaluated during the vaginal examination for diagnosis, should be taken. The diagram in figure 5 might be helpful to take a decision.
Figure 5 – Decision-making guidelines for FMD dystocia case treatment (adapted from Jackson, 2004).
Sometimes the practitioner may be pressured by the cow´s owner to take a different decision, like to perform a C-section in DM cows, or to use excessive traction to avoid spending too much money with a C-section, but the practitioner must always act according his best knowledge and taking into consideration the welfare of both dam and calf. For example, some major determining factors for the C-section outcome, for both the calf and the dam, are the degree of traction which the cow was subjected before the surgery and the time between the start of calving and the practitioner first aid, and those factors could also influence the decision (Noakes et al., 2001).
Calving dystocia compare size of fetus and birth canal clear evidence of FMD Calf alive -cesarean section calf dead -fetotomy Possible evidence of FMD calf alive -trial traction calf distress/ no possible by traction -cesarian section calf dead -trial traction/ fetotomy No evidence of FMD Trial traction/ fetotomy normal, unassisted
1.3.2. Vaginally forced delivery
Pulling on a calf should only be done when the normal presentation and posture of the calf are observed. This applies either to an anterior or a posterior presentation. The anterior (forward) presentation in dorsal position and extended posture is the most normal situation at calving, which means that the calf appears with the forelegs first, followed by the head and then the rest of the body and the hind limbs at the end (Ball and Peters, 2004). The way to deliver the calf in anterior or posterior longitudinal presentation will be discussed in this section, discarding defects in posture or position, such as head or limbs defects. This is usually the first approach in a simple FMD case if the wideness of the birth canal is sufficient. To perform a controlled traction, obstetric chains or ropes around the pastern of the calf can be used or, in more complicated cases, a mechanical fetal extractor. Whatever the traction source used, it is always important to use ample lubrication (Noakes et al., 2001; Jackson, 2004; Drost, 2005; Youngquist and Threlfall, 2007). In cases of excessive or uncontrolled traction some problems are expected for the dam, like damage of the pelvic nerves, laceration or contusion of the soft tissues, and sacral displacement or fracture. Consequently, one should be aware of the risks, to avoid complications (Noakes et al., 2001; Youngquist and Threlfall, 2007). In cattle, the shoulders and hips of the calf are the largest parts. In most cases, whenever these parts can fit within the cow‟s pelvis, vaginal delivery is possible, although it may not be true in cases of DM calves, because they present excessively larger shoulders and larger hindquarters, which may be retained. Hence, it is possible that in DM calves in anterior presentation, the head and perhaps the chest may emerge easily, but the calf‟s hips may not pass the maternal pelvis. The extractive force should be only applied simultaneously with the dam‟s abdominal press, releasing the tension when she ceases to strain (Noakes
et al., 2001; Drost, 2005; Momont, 2005; Youngquist and Threlfall, 2007). The extraction
can be performed in a standing cow, yet Drost (2005) refers 4 advantages of performing delivery with the cow lying down:
The cow can angle her pelvis more favorably by bringing her legs forward and she can slightly spread her legs;
The operator that is pulling can sit on the ground and exert more traction force; The calf doesn‟t have to come up out of the abdomen against the force of gravity; The cow will not fall down in the middle of the extraction process.
1.3.2.2. Cranial/anterior presentation
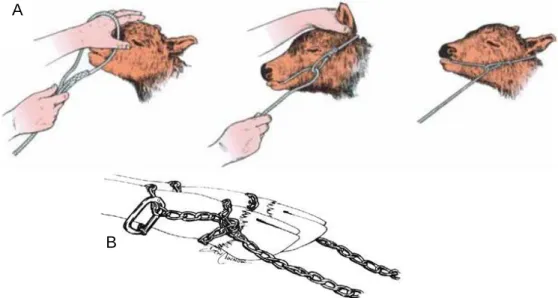
This is the most common presentation. The best way to deliver the calf is still controversial, and some authors recommend application of simultaneous traction to both forelimbs while others defend that alternating traction applied to one limb at a time makes the extraction easier. The in vitro studies by Becker et al. (2010) support the recommendations for alternate traction to the forelimbs of the calf, with a difference of advancement of about 10 cm, until the elbows enter the pelvic cavity. These authors propose that this asynchronism in the entry of the elbows into the pelvis may lead to a better adaptation of the head and forelimbs to the available space in the pelvic cavity. Nevertheless, they also found that after exposition of the head, simultaneous limb traction is beneficial. When the calf is in anterior position it is usually possible to access his head and forelimbs and so ropes can be applied to both or obstetrical chains to the forelimbs (Figure 6), regardless that the rope in the head is often unnecessary (Noakes et al., 2001; Jackson, 2004). The best technique to attach the chain is placing a loop around the part of the leg above the fetlock and then make a half hitch and tighten it below the joint and above the foot in the pastern. With this technique the extractive force will be applied over a larger area, reducing chances of injuring the calf (Youngquist and Threlfall, 2007; Selk and Sparks, 2008). After applying the ropes/chains the delivery can start. This should be a very gradual process. Ideally this should occur with two people pulling in the ropes under orders of the practitioner, which should ascertain if the delivery is proceeding well each time that the cow strains and the calf advance, with further examination and applying more lubricant whenever necessary (Noakes et al., 2001).
Figure 6 – Techniques to apply the ropes to the head (A) and limbs (B) of the calf (Jackson, 2004; Youngquist and Threlfall, 2007)
B A
Calf delivery can be divided into several phases:
The initial pulling, as the calf enters the pelvis, should be upwards (slightly dorsally); As the head passes through the pelvis the direction should be directed horizontally backwards;
As soon the head has passed through the pelvis and is in the vulva, the direction of traction should change to downward;
The next obstacle in this delivery are the hips and the stifle joints because at this level the width of the calf is greater than its height and so the calf should be rotate to a dorso-ilial position to allow this portion to adapt to the largest diameter of the dam´ pelvic canal. This rotation must be performed before the hips contact the pelvic inlet. This step is very important to prevent hiplock.
After all this steps and as soon as the fetal pelvis has passed the birth canal, the delivery is quickly completed (Noakes et al., 2001; Jackson, 2004; Drost, 2005; Youngquist and Threlfall, 2007).
These changes on the direction of pulling are necessary to allow advantage to be taken of the greatest diameters of the pelvic canal of the cow that is oval in shape, being the greatest diameter between the sacrum and the pubis (Figure 7) (Jackson, 2004; Drost, 2005; Youngquist and Threlfall, 2007).
Figure 7 – Pelvic inlet (viewed from in front and somewhat below) with oval shape. The black arrow indicate the greater diameter between the sacrum and pubis (adapted from Frandson and Spurgeon, 1992)
1.3.2.3. Caudal/posterior presentation
The risk to lose a calf during delivery in this presentation is higher than in the anterior presentation. This is due to an earlier rupture of the umbilical cord, with the head of the calf still inside of the dam pelvis, and to avoid the calf from becoming hypoxic or even die the delivery should be complete soon (Noakes et al., 2001; Jackson, 2004; Drost, 2005; Youngquist and Threlfall, 2007). Similarly to procedures described for the anterior presentation, the obstetrical chains or ropes, to be placed just above the fetlock joint of the hindlimbs, can be used (Noakes et al., 2001; Jackson, 2004).To start the delivery, the calf should be rotated to a dorso-ilial position, like in the final step of the delivery in anterior presentation, to make the hips to approach the widest diameter of the pelvis inlet of the dam (Youngquist and Threlfall, 2007). Once the calf hips have passed the pelvic inlet and starts exit the vulva, the delivery should be completed quickly because this coincides with the time that the umbilical cord becomes trapped against the maternal pelvis. Therefore, continuous traction, and not just when the cow strain, should be applied from this stage until the calf has been delivery (Noakes et al., 2001; Drost, 2005; Youngquist and Threlfall, 2007).Jackson (2004) recommends to pull in a slightly upwards direction as the calf enters the pelvis, subsequently backwards, as the calf starts to go through the pelvis, and then downwards and backwards.
In some situations both in anterior and posterior presentation, the use of a mechanical calf puller can be helpful if used with caution.
1.3.2.4. Epidural anesthesia
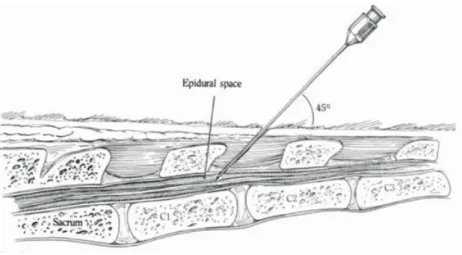
Although not essential, the caudal epidural anesthesia may be useful in most cases of vaginal forced delivery, and it is recommended and used, for fetotomy or cesarean section, irrespective of the surgical approach (Frazer and Perkins, 1995; Jackson, 2004; Newman and Anderson, 2005; Kolkman et al., 2007; Newman, 2008). As a result of an anesthesia of the anus, perineum, vulva and vagina this anesthesia will prevent the straining, the prolapse of the ruminal wall or intestines and tail movements during the procedure (Frazer and Perkins, 1995; Noakes et al., 2001; Jackson, 2004). To perform the epidural anesthesia, lidocaine hydrochloride 2% is introduced in the epidural space between the last sacral and first coccygeal vertebrae or in the first intercoccygeal space (between the first and second coccygeal vertebrae) (Figure 8). To find the correct location the practitioner should move the tail up and down using the other hand to find the spinal processes and the space between the vertebrae. The drug should be given in low, small
doses (5 to 10 ml) to avoid recumbence of the cow, and anesthetic administration should only be done after the site for injection be prepared and cleaned. The needle is inserted cranially and ventrally in an approximate angle of 45°, then the syringe is attached and the injection should evolve easily and without resistance (Turner et al., 1989; Caulkett et al., 1993; Noordsy, 1994; Hanzen et al., 1999; Fubini and Ducharm, 2004; Jackson, 2004; Carreira et al., 2005; Newman and Anderson, 2005; Kolkman et al., 2007). Time to onset and duration of analgesia are usually 10 to 20 minutes and 30 to 150 minutes respectively (Fubini and Ducharm, 2004).
It is also possible to use xilazine HCL for epidural anesthesia. Caulkett et al. (1993) in their study found that xilazine HCL in a dose of 0,07mg/kg + NaCl 0,9% to a final volume of 7,5 ml generally produced adequate analgesia for C-section. This procedure shows a major disadvantage on the time to onset the analgesia (+/- 25 minutes) and on the tendency to lie down in deeply sedated animals. Thus, the authors suggest the use of xilazine HCL as an adjunct to traditional techniques, instead the use as a technique for surgical anesthesia and sedation for C-section.
Figure 8 – Method to proceed to the epidural anesthesia in the first intercoccygeal space (from Turner, 1989)
1.3.2.5. Uterine relaxation
The use of a tocolyticum agent such as clenbuterol, although controversial in Portugal, or isoxuprine can be helpful in some situations. The procedure is described below, in section 1.3.3.4.
1.3.3. Cesarean Section
This is one of the oldest surgeries performed in Veterinary Medicine and probably the most common surgical procedure performed in cattle practice (Green et al., 1999; Wyn-Jones, 2004; Newman and Anderson, 2005). Newman and Anderson (2005) referred the preservation of the cow, calf and the future reproductive efficiency of the female as the basic goal of performing this surgical procedure. Schultz (2010) and Bicalho (2009) state that the goal is to limit the contamination of the abdominal cavity with uterine contents, especially when the calf is dead, since this contamination greatly increases the risk of peritonitis and limits the cow‟s productivity and chances of survival (Schultz et al., 2008; Bicalho, 2009; Schultz, 2010). Hoyer et al. (1990), cited by Uystepruyst et al. (2002), refers that C-section is the preferred method to deliver calves in severe cases of dystocia associated to FMD while other authors referred FMD as a major indication for C-section (Frazer and Perkins, 1995; Noakes et al., 2001). However, beside FMD, there are other indications that can be classified in maternal or fetal indications for C-section. Incomplete cervical dilatation, irreducible uterine torsion, immature heifers, pelvic deformities, uterine tear and hydrops are some additional maternal factors. Within the fetal factors anomalies in calf presentation, a high valuable calf (from embryo transfer or cloning), fetal anasarca and fetal monsters such as shistosomus reflexus and emphysematous fetus are described (Oehme and Prier, 1974; Bouchard et al., 1994; Noordsy, 1994; Parish et al., 1995; Hanzen et al., 1999; Noakes et al., 2001; Jackson, 2004; Newman and Anderson, 2005; Kolkman et al., 2007; Newman, 2008). It has also been reported that cows previously submitted to C-section are more predisposed to be submitted to a new C-section than other cows. Also long pregnancy period, heifer‟s age lesser than 2 years, preceding long interval from first service to conception are risk factors to perform C-section (Barkema et
al., 1992; Newman and Anderson, 2005).
Newman and Anderson (2005) suggested the C-section to be classified in 3 different categories: elective, emergency with a non-emphysematous calf or emergency with emphysematous calf. Furthermore, they state that the most important parameter to determine the success of the procedure is the health status of both dam and calf at the time of the procedure. Thus, cows subject to an emergency C-section are more likely to encounter intra and post-operative complications and less likely to survive compared with cows submitted to elective surgery, since the prognosis is proportional to the duration of dystocia. The calf may not survive more than 8 hours in a second stage of labor and also the mortality of the dam rises when surgery is not performed in first 24 hours after the beginning of dystocia or if the calf became dead and emphysematous (Jackson, 2004; Newman and Anderson, 2005). Newman and Anderson (2005) also refer to forced
extraction, fetal limb fractures, delayed delivery, uterine trauma or rupture, emphysematous fetus, anorexia, fetal abnormalities or death, obturador or sciatic nerve damage, uterine inertia and sever trauma during manipulation as pre operative complications.
Some authors pretend that C-section is the major abdominal surgery performed in a contaminated environment and that cannot be considered as a sterile procedure but, nevertheless, it should be performed under surgical sterility to avoid contamination (Kolkman et al., 2007; Kolkman et al., 2009). They also refer that, in Belgium, in consequence of the selection towards hypermuscularity, the hypermuscled calves can no longer be born per vias naturals. Consequently, they state that while in dairy cows the C-section is the last option, for Belgium veterinarians C-C-section has become the first choice approach and cows are operated in very early stages of parturition, often without attempt to extract the calf. Also in Belgium, Hanzen et al. (1999) reported, for 1986, a percentage of 72 for calving by cesarean section in breeds carrying the cullard gene, with the percentage rising to 87 in 1994. In 1992, Barkema et al. (1992) also reported an increase of the percentage of calf delivery by C-section in Netherlands, which was associated to the increase in the use of double-muscled and beef breed sires. Newman and Anderson (2005) revealed that when a C-section is considered as an ultimate choice, a negative outcome is more likely, but when it is performed in an early stage of parturition its outcome is more rewarding. Consequently, in Belgium, C-section became an additional production technique and is performed in the beginning of the second stage of parturition (as an elective C-section) (Carreira et al., 2005). Uystepruyst et al. (2002) found that BWB calves delivered by ECS after full cervical dilatation had better lung function in comparison with calves delivered before full cervical dilatation. Thus, these authors advice to wait for full cervical dilatation before surgery, to minimize the losses resulting from respiratory disease. Jackson (2004) point to a maternal survival rate between 80 and 90% in case of ECS and also defend a good fetal survival rate, although a decrease in fetal viability should be expected with an increasing in duration of second stage of labor.
There are 8 different techniques to deliver a calf by C-section, each one having its own advantages and disadvantages, and they should be chosen according to the type of dystocia, the condition of the female and if she‟s able to stand during the procedure, the environmental conditions, the preference of the surgeon and the assistance available. These techniques are: the standing left paralumbar celiotomy, standing right paralumbar celiotomy, standing left oblique celiotomy, recumbent left paralumbar celiotomy, recumbent right paralumbar celiotomy, recumbent ventral midline celiotomy, recumbent ventral paramedian celiotomy and ventrolateral celiotomy (Schultz et al., 2008; Bicalho, 2009; Schultz, 2010). These techniques will be discussed below.
As one actor that may influence the choice of the surgical approach is the uterine horn in which is the fetus located, determining the fetus location before starting C-section is an important step (Jackson, 2004).
1.3.3.2. Preparing the surgery
Even though there are several techniques, the pre-surgical procedures are common to them all. Before the beginning of the surgery all the necessary material should be prepared. It should include (Hanzen et al., 1999; Jackson, 2004; Kolkman et al., 2007):
Medication for sedation, local anesthesia, analgesia, antibiotics and any other drug that might be useful (such as clenbuterol and oxytocin);
Material to prepare the surgical site, such as soap, razor, povidone-iodine and alcohol;
A Surgery box with sterilized material, which must contain: o scalpel and disposable scalpel blade;
o rat-toothed forceps; o scissors;
o towel clamps;
o blood vessel clamps;
o obstetrical ropes/chains and handles for calf extraction;
o different kinds of needles for suturing (cutting and round needles); o needle holder;
o uterine forceps Sterilized swabs
Suture material (absorbable and non-absorbable suture)
1.3.3.3. Sedation
The goal for sedation is the chemical restraint of animals, but not all practitioners use sedation for C-section. Actually, sedation should only be used in cases of agitated or aggressive cows (Jackson, 2004; Carreira et al., 2005; Newman and Anderson, 2005; Kolkman et al., 2007). Although the activity of α2-agonists decreases with agitation of the animals (Kolkman et al., 2007), these drugs are widely used for sedation, in particular xilazine. Xilazine, in a doses of 0,05-0,1mg/kg IV (Allen et al., 2005), is currently used to cause sedation and analgesia (Noakes et al., 2001; Fubini and Ducharm, 2004; Jackson,
2004; Carreira et al., 2005; Newman and Anderson, 2005). Its major inconvenience is to increase myometrial tone contraction, which difficult exteriorization of the uterus, as this drug has a direct myotonic effect. Another negative side effect associated to xilazine use is the ruminal bloat (Frazer and Perkins, 1995; Noakes et al., 2001; Jackson, 2004; Newman and Anderson, 2005; Schultz et al., 2008; Schultz, 2010).In addition,Newman (2008)also describes ataxia following xilazine administration, which can be an undesirable effect in the standing approach. Thus, to provide good standing for 1 hour, he proposes a combination of ketamine hydrochloride (0,04 mg/kg IM), butorphanol tartrate (0,01 mg/kg IM) and xylazine hydrochloride (0,02 mg/kg IM). To perform the C-section in a recumbent animal the dose recommended for xilazine is 0,2 mg/kg IM (Noakes et al., 2001).
Some other drugs can be used for sedation in cattle, like acepromazine, diazepam, pentobarbital, butorphanol and choral hydrate (Fubini and Ducharm, 2004). However, they are seldom used in the field practice.
1.3.3.4. Uterine relaxation
To block the uterotonic effects of xilazine when sedation is used for C-section tocolyticum agents can be used (Frazer and Perkins, 1995).Clenbuterol,a β2-agonist, can be used as tocolyticum, in a dose of 0,6 µg/kg, injected slowly in the tail vein rather than intramuscularly. Clenbuterol act as antagonist to the effects of oxytocin and prostaglandins and is reported to be the most potent uterine myometrial relaxant. Thus, it will relax the uterus helping in the manipulation during the surgical procedure and the suture. Moreover can also be helpful during manipulations to correct fetal malpresentation or malposture in cases of manual correction of dystocia and in fetotomy procedures (Menard and Diaz, 1987; Menard, 1994; Hanzen et al., 1999; Noakes et al., 2001; Jackson, 2004; Kolkman et
al., 2007).
Isoxsuprine is also a β2-agonist referred in the literature as a widely employed agent as tocolytic since it relaxes myometrial and vascular smooth muscle (Frazer and Perkins, 1995).
The use of both clenbuterol and isoxuprine is not permitted in food animals in United States, and its use in Europe is regulated by the European Council Directive nº 96/22/CE, modified in the Directive 2008/97/CE. This regulation was transposed to the Portuguese law (Dec.-Lei nº 185/2005, which received new lettering in the Dec.-Lei nº 146/2009). In the later, in its article 6th–A, item b, β-agonists drugs may be used therapeutically in individual females to induce tocolysis, under the Veterinarian surveillance.
50 to 100% of the European practitioners currently use uterine relaxants (Newman and Anderson, 2005). The study by Menard and Diaz (1987)showed a reduced incidence of uterine adhesions and retained fetal membranes in cows submitted to C-section when clenbuterol was used as a uterine relaxant.
In response to the constraints to the use of β-agonists drugs new studies have focus on with the use of ritodrine and terbutaline as tocolyticum agents (Frazer and Perkins, 1995; Newman and Anderson, 2005; Newman, 2008). Newman (2008) also studied the use of epinephrine to relax the myometrium, and has found that in spite of myometrial relaxation, the uterine wall tend to thinning, making the suture of the uterus more challenging.
1.3.3.5. Preparation of the surgical area
The area for the surgical approach varies with the C-section method. Nevertheless the pre surgical steps to prepare this area are the same. Briefly, it consists in washing, shaving, and disinfecting the area to allow local anesthesia to be performed in a cleaned animal; then the area should be rewashed with iodine soap, dried and finally disinfected with alcohol and povidone iodine solution (Kolkman et al., 2007).
1.3.3.6. Anesthesia
This can be made in two steps: Epidural anesthesia (already described in section 1.3.2.4.) and the local/regional anesthesia.
This may be accomplished through several techniques that are influenced by the surgical approach: local infiltration by line block or inverted L block and the proximal or distal paravertebral injection, which are performed after the preparation of the surgery site. Lidocaine hydrochloride is the most frequently used drug for this anesthesia and each technique has its own advantages and disadvantages (Fubini and Ducharm, 2004; Jackson, 2004; Newman and Anderson, 2005; Weaver et al., 2005; Newman, 2008).
1.3.3.5.1. Local infiltration
The local infiltration can be obtained using procaine hydrochloride containing 4% of adrenaline (Kolkman et al., 2007) or 2% lidocaine with adrenaline (Noakes et al., 2001; Fubini and Ducharm, 2004). Association of adrenaline to the local anesthetic allows to minimize the bleeding, to increase the duration and to decrease the toxicity of the