REVIEW
I INSERM U 870, INSA Lyon - Villeurbanne, France.
II Faculty of P h arm acy, Univ ers ity of B urg und y - D ij on, France. II As s ociation Rem ed es - O rlienas , France.
Em ail: nicolas .w ierns p erg er@ free.fr T el: 3 3 4 72 3 1 05 79
Receiv ed for p ublication on March 2 6 , 2 01 0 Firs t rev iew com p leted on Ap ril 06 , 2 01 0 Accep ted for p ublication on Ap ril 06 , 2 01 0
FRUCTOSE AND CARDIOMETABOLIC DISORDERS: THE CONTROVERSY WILL, AND
MUST, CONTINUE
Nicolas W ierns p erg er,I,III Alain G eloen,I J ean-Robert Rap inII,III
d oi: 1 0.1 5 9 0/ S1 807-5 9 3 2 2 01 000070001 3
Wiernsperger N, Geloen A, Rapin JR. Fructose and cardiometabolic disorders: the controversy will, and must, continue. C linics. 2 0 1 0 ; 6 5 ( 7 ) :7 2 9 - 3 8 .
T he present review updates the current k nowledge on the q uestion of whether high f ructose consumption is harmf ul or not and details new indings which f urther pushes this old debate. D ue to large dif f erences in its metabolic handling when compared to glucose, f ructose was indeed suggested to be beneicial f or the diet of diabetic patients. H owever its growing industrial use as a sweetener, especially in sof t drink s, has f ocused attention on its potential harmf ulness, possibly leading to dyslipidemia, obesity, insulin resistance/ metabolic syndrome and even diabetes. M any new data have been generated over the last years, conirming the lipogenic ef f ect of f ructose as well as risk s of vascular dysf unction and hypertension. Fructose ex erts various direct ef f ects in the liver, af f ecting both hepatocytes and K upf f er cells and resulting in non- alcoholic steatotic hepatitis, a well k nown precursor of the metabolic syndrome. H epatic metabolic abnormalities underlie indirect peripheral metabolic and vascular disturbances, f or which uric acid is possibly the culprit.
Nevertheless maj or caveats ex ist ( species, gender, source of f ructose, study protocols) which are detailed in this review and presently prevent any irm conclusion. New studies tak ing into account these conf ounding f actors should be undertak en in order to ascertain whether or not high f ructose diet is harmf ul.
K EY W O RD S: Fructose; T riglycerides; M etabolic syndrome; U ric acid; H ypertension; D iet.
INT RO D UC T IO N
I n recent years, there has been increasing interest in the role of dietary f ructose ( F) as a possible health risk . For decades, there has been a debate as to whether F, which has a lower glycemic index than glucose ( G) and does not induce insulin secretion, is a good dietary alternative f or diabetic patients. T his important q uestion has never been answered. M ore recently, it has been suggested that the
worldwide burden of obesity and type 2 diabetes ( T 2 D M ) in young adults might be link ed to a parallel increase in the
consumption of artiicially sweetened f ood, particularly sof t drink s.1 Freq uently in the U nited S tates, beverages ( sodas and f ruit j uices) are sweetened by F, which is added as high F corn syrup ( H FC S ) . H FC S has suddenly attracted
attention regarding its responsibility in causing these metabolic disturbances. H owever, it must be noted here that this phenomenon particularly applies to the U nited S tates because countries in E urope and elsewhere have limited the use of H FC S . T his is one reason, as will be seen later, f or the ongoing discrepancies and as- yet uncertain conclusions.
T he present review describes the various aspects of this important clinical q uestion, ex poses the reasons f or some maj or discrepancies and details some reasons why we are missing irm conclusions and what must still be done to reach them.
W H AT D O FRUC T O SE P H ARMAC O D Y NAMIC S
T ELL US?
Intes tines
and solid f oods. As will be seen later, this development has maj or conseq uences f or answering the q uestions addressed in this review.
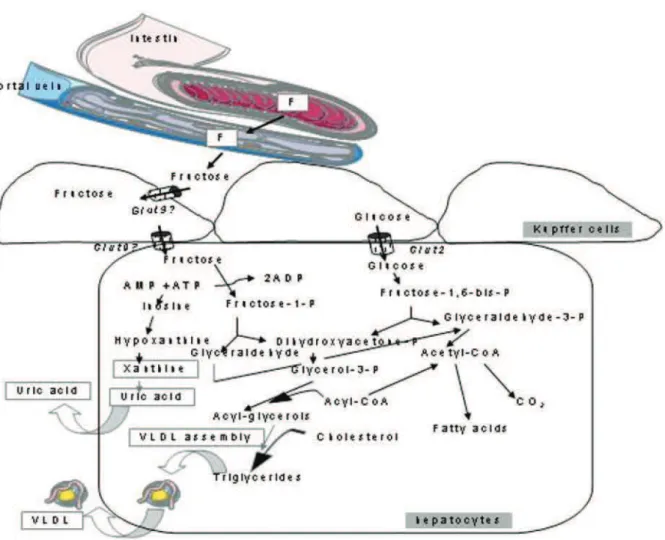
Although structurally similar, F behaves very dif f erently f rom G; it is absorbed in limited amounts, and most healthy subj ects ex hibit signs of intolerance at a daily F intak e of approx imately 5 0 g,2 f ree f atty acids and some amino acids f avor the absorption of F,3 ,4 which means that the threshold f or intolerance may be even lower. F is transported via a speciic glucose transporter, GL U T 5 , and ex its enterocytes via GL U T 2 transporters. I t is important to note that chronic F intak e upregulates GL U T 5 ex pression.3 T he lipidogenic ef f ect of F starts in the intestines because F increases the levels of f atty acids associated with ApoB 4 8 , which are released as chylomicrons.
H ep atocytes
O nce in the portal vein, F is rapidly and almost completely ex tracted by the liver; the hepatic irst pass is close to 1 0 0 % . H epatocytes can transf orm F into various metabolites: glucose, glycogen, lactate, and f at. I n contrast to G, F is rapidly converted into triose- P independently of insulin. F is also a good precursor f or gluconeogenesis because it generates lactate. Approx imately 1 7 % of F becomes glycogen, and approx imately 2 0 - 5 0 % of an F load leaves the liver as G.5 I n healthy individuals, compensatory mechanisms reduce other gluconeogenic pathways, maintaining constant total hepatic glucose production. O ver a long period of time, however, F decreases the insulin inhibition of hepatic glucose production, leading to hepatic insulin resistance. T he phosphorylation of F req uires high levels of AT P , leading to acute states of AT P depletion in hepatocytes and possible synthesis of uric acid ( discussed below) .
A typical f eature of F is the induction of hypertri gly-ceridemia ( H T G) , notably because of reduced clearance. T his is considered to be the most prominent negative ef f ect of F. I n addition to its ef f ects on T Gs, F also decreases H D L cholesterol levels.
K UP FFER C ELLS
I n the liver, the maj ority of cells are non- parenchymal cells. S inusoids are lined with a dense net of K upf f er cells ( K C s) and endothelial cells. K C s mak e up the largest proportion of macrophages in the body; they are strongly involved in detox if ication and inf lammatory reactions, liberating T NF , leuk otrienes, interleuk ins and T GF- .6 I nterestingly, K C s have a high density of insulin receptors and ex tract up to 5 0 % of a G load. T hus, K C s may play an
important but hitherto unrecogniz ed and poorly understood role in the regulation of metabolic homeostasis.7 T he f ew data sets that are presently available appear paradox ical. O ne might ex pect that K C impairment leads to metabolic disturbances because a block age of K C s has been shown to result in hyperinsulinemia8. Furthermore, the elimination of K C s by clodronate- encapsulated liposomes was recently shown to provok e non- alcoholic steatotic hepatitis ( NAS H ) due to the concomitant elimination of protective I L- 1 0 .9 P aradox ically, other models using gadolinium chloride to eliminate K C s have shown that this procedure improved insulin resistance and NAS H induced by high f at1 0 or S , one of the primary sources of F.1 1 T NF is considered to be responsible f or these disturbances. T hese data are intriguing, and it is dif icult to k now if this result is due to the use of gadolinium salt or to a massive overproduction of TNF , which would then overcome the beneicial ef f ects of these cells. Whatever the ex planation, we suggest that the role of K C s req uires clariication because this very important hepatic tissue might represent a k ey element in the problem.
W H AT D O ES P AT H O P H Y SIO LO G Y T ELL US?
Metabolic d is turbances
H igh F ( H F) is suspected to be involved in a series of diseases link ed to metabolic disturbances, the best k nown being H T G and insulin resistance. As will be discussed later, several mechanisms are responsible f or these direct and indirect ef f ects of F.
observed f or oral intak es up to approx imately 5 0 g/d.1 7 H T G and f asting ApoB was, however, increased in overweight or
obese women.1 8 Fasting increased levels of T G, V L D L - T AG and leptin without inducing insulin resistance or ectopic
f at deposition in healthy males af ter f our week s of H F administration.1 9 M ore recently, however, the same group reported that j ust one week of H F administration increased ectopic f at deposition in the liver and sk eletal muscle, with a greater ef f ect seen in the of f spring of diabetic parents than in healthy controls.2 0
T he lipogenic activity of F can be demonstrated in vitro; adding H FC S - 5 5 ( a sweetener widely used in the U nited S tates) to hepatocytes leads to H T G and the elevation of lipogenic proteins and ox idative stress. At the same time, insulin resistance and endoplasmic reticulum stress are increased, and mitochondrial dysf unction is illustrated by cytochrome C release.2 1 T his f inding f its with the mitochondrial disruption seen in human NAS H .
I n rats, the ef f ects of F appear to be stronger in adults than in young animals.2 2 F is usually administered in high doses to rats to rapidly produce insulin resistance, but lower, more relevant levels of F also induce G intolerance if they are administered over long periods of time.2 3 An H F diet in rats is considered to be a relevant model f or human NAS H , leading to typical hepatic lobular inlammation.2 4
I n humans, a high intak e of dietary F or sweetened f ruit j uice ( but not whole f resh f ruits) leads to impaired G tolerance in genetically susceptible individuals.2 5
I n addition to dyslipidemia and insulin resistance/ metabolic syndromes, the F in a daily regimen of two or more colas has been shown to increase the risk of gallstones2 6 and chronic k idney disease ( stones) .2 7
Vas cular d is turbances
B ecause of the high potential of F to glycate proteins compared to G, concern has been raised about the possible roles of F in cardiovascular complications. T he reason f or this is partly because the acyclic ( linear) f orm of the sugar ( which is the glycating f orm) is larger in F than in G.2 8 ,2 9 A meta- analysis showed that high F consumption increased cardiovascular risk by 2 4 % .3 0 T he direct ef f ects of F on protein glycation are q uestionable, however, because F is almost completely metaboliz ed by the intestines and liver, leaving little if any intact F in the blood. H F is commonly assimilated into sof t drink s; however, sof t drink s ( particularly colas) contain many other glycating ( or glycated) agents. T hus, there is possible conf usion about the real role of F in in vivo glycation. S ome direct glycation might occasionally occur when f ood and drink s come into direct contact during eating. I ndeed, the initial steps of the
M aillard reaction occur more rapidly with F than with G, and the glycation of f ood proteins decreases their digestibility.3 1
T he glycation of albumin occurs on L ys- 5 2 4 and leads to the f ormation of carbox ymethyllysine ( C M.3 2 L ) I nterestingly, vegetarians show higher levels of C M L than normal consumers, which can be ex plained by their high consumption of f ruits, honey and vegetables.2 8 F is k nown to be involved in cataractogenesis.3 3 H owever, this is more lik ely to be due to intracellular F f ormation resulting f rom the sorbitol pathway; when F synthesis increases, it can glycate lens crystalline.3 4
Atheromatous plaq ues are increased in hyper-cholesterolemic rabbits when F is added to their diet.3 5 F is also suspected to cause hypertension ( H T ) ; acute F intak e has been shown to increase blood pressure and heart rate in humans.3 6 ,3 7 I n rats, an H F diet does not automatically generate H T ; it seems that only some rat strains develop H T , which is dependent on an animal’s age and diet protocol. T his phenomenon may be due to the varying intra- and interspecies sensitivity toward F; indeed, rats, in contrast to humans, possess active uricase.3 8 ,3 9
V ascular reactivity is modiied with chronic H F diets, as endothelial dysf unction most lik ely occurs due to the inhibition of NO synthesis by F.4 0 O ur ex periments showed an abnormal reactivity of small terminal arterioles in the sk eletal muscles of chronically F- f ed rats.4 1
Finally, it is important to note that F also increases P AI -1 ,4 2 ,4 3 a ibrinolytic f actor that is k nown to be involved in the pathology of both metabolic and vascular disturbances of metabolic syndromes.4 4
MEC H ANISMS INVO LVED IN FRUC T O SE-IN-D UC ESE-IN-D SE-IN-D IST URB ANC ES
D irect effects in s p lanch nic org ans
relevant model in rats) . T he combined negative ef f ects on liver lipid content and lactate and lipid output5 2 mak es this organ a crucial ef f ector of H F- induced metabolic disturbances. I ndependently of an M S diagnosis, patients presenting NAS H were f ound to consume more sof t drink s than healthy subj ects.5 3 I nterestingly, when moderate intak e levels of various sweeteners were compared in rats during a ten- week period, both F and H FC S increased alanine aminotransf erase activity, although no other dif f erences were observed.5 4 T hese data show that the irst premises of f atty liver can be seen even f ollowing moderate F consumption. Figure 1 depicts the maj or f ate of F in the splanchnic area as well as some dif f erences between F and G.
Recently, the involvement of intestinal bacterial lora in the regulation of metabolic homeostasis has been the subj ect of intense interest.5 5 ,5 6 I n particular, studies have revealed that NAS H is associated with intestinal bacterial overgrowth and increased intestinal permeability, leading to the endotox in-dependent activation of K C s.5 5 T his ef f ect was also shown
with an H F diet in rats.5 7 T hus, intestinal ef f ects may add to hepatic ef f ects as causal ef f ectors of H F- link ed metabolic abnormalities.
While F intolerance does not seem to dif f er between normal subj ects and those suf f ering f rom irritable bowel syndrome,5 8 ,5 9 an improvement in F intolerance was observed in 1 / 3 of these patients af ter F restriction.6 0 C onversely, F and f ructans may induce irritable bowel syndrome and intestinal permeability.5 5 ,6 1 - 6 3
Ind irect m etabolic effects
B y increasing the liver lipid content and provok ing H T G, F leads to global metabolic derangements that are typical of M S s, eventually leading to T 2 D M . S everal studies have shown that H F induces hepatic insulin resistance, resulting in an elevated G output due to the lack of gluconeogenesis suppression. O nce in the circulation, T Gs may accumulate in sk eletal muscle cells and induce peripheral insulin resistance.
Fig ure 1 - Fructose is absorbed in the intestine by GL U T 5 and ex its enterocytes via GL U T 2 transporters. I t is tak en up by K upf f er cells and hepatocytes,
H ig h energ y intak e
I t has been suggested that energy intak e is higher with oral F than with oral G. T he reasons f or this belief are the f ollowing: 1 ) the thermic ef f ect of F is higher than G because of high AT P consumption, and 2 ) it was observed that the satiety phenomenon normally regulating f ood intak e did not always operate af ter chronic F. F lowers ghrelin and leptin levels to a lesser degree than does G, resulting in lower f ood intak e suppression.1 ,3 T his phenomenon applies mainly to liq uid F, leading to a higher energy balance than F in solid f ood.6 4 ,6 5 When sweetened beverages were tak en together with meals, a higher mean energy intak e of 1 0 4 k cal was measured.6 6 Nevertheless, the “energy balance” hypothesis of H F is still a subj ect of debate.6 7
Is uric acid th e culp rit?
U ric acid ( U A) is a maj or antiox idant, but, lik e most molecules of this category,6 8 it can also induce opposite ef f ects if concentrations are suf iciently high.6 9 T here are lik ely to be concentration thresholds delineating positive f rom negative ef f ects of such substances; acute and even relatively high U A levels protect against ox idative stress7 0, but chronically elevated U A levels are link ed to Ms, S reduced adiponectin and elevated E - selectin, in parallel with positive ef f ects such as reduced nitrotyrosine and increased total antiox idant capacity.7 1 T hus, high U A levels could be a compensatory mechanism that counteracts the ox idative stress related to metabolic or vascular disturbances.7 2
I n vitro U A increases NAD P H ox idase activity and ox idative stress in adipocytes, leading to increased p3 8 M AP k inase activity and insulin resistance.7 3 U A levels correlate with 2 4 - h urinary ex cretion, waist circumf erence, insulin concentrations and the H O M A index , which are all indices of a M 7 4S . H igh insulin levels reduce renal U A ex cretion, suggesting that hyperuricemia results f rom a combination of stimulated f ormation and reduced elimination. I n adolescents, body mass index and a number of M S components correlate with U A.7 5 I n the S an B ernardo S tudy, U A was a good predictor of T 2 D M in older adults with impaired f asting glycemia.7 6 E levated U A was shown to be link ed to NAS H independently of body mass index .7 7 - 8 0 I n elderly male subj ects, high levels of U A were correlated with M S components and elevated levels of P AI - 1 .8 1 T hus, it seems that at any age, high levels of U A are link ed to M S . D ecreasing U A levels in rats with allopurinol prevents M S , as shown by reductions in insulin, T G and weight.4 0
O n the vascular side, high levels of U A are link ed to cardiovascular diseases, especially H T .8 2 - 8 6 I f patients are already at risk , then U A represents a serious problem.8 7 ,8 8
M echanisms that are responsible f or the deleterious U A ef f ects are link ed to increased C reactive protein, inf lammation and reduced NO production, thereby hampering vascular reactivity.3 8 ,8 2 ,8 4 ,8 9
H F increases U A f ormation as a conseq uence of AT P consumption and high synthesis of AM P , which is then deaminated to f orm U A.3 ,9 0 S everal studies have shown that H F increases U A levels. H owever, in the irst phase of the Nanes I I I study, M S was not link ed to U A in subj ects who consumed diet sof t drink s9 1. U A is k nown to be responsible f or gout due to the deposition of monosaccharide urate crystals; this ef f ect is strongly related to diet.9 2 I n a prospective cohort study over 1 2 years, F intak e was correlated with gout regardless of whether sweetened sof t drink s, f ruit j uices or F- rich f resh f ruits were consumed.7 7 H owever, while this manuscript was in its inal phase, a new publication showed that an analysis of more recent data f rom the Nanes I I I database ( > 9 0 0 0 subj ects) f ailed to conirm an association between F and U A. T hus, over a long time period, U A might not be as harmf ul in an H F diet as was initially claimed, which is in agreement with other reports.9 3
FRUC T O SE VS. O T H ER SUG ARS
T Gs; H T G lasted f or over 2 4 hours in the insulin- resistant subgroup.1 2
Altogether, these data show that F has roughly the same harmf ulness whether it is administered as a concentrate such as H FC S or as sucrose. When the comparison is made with G, however, there are strong q ualitative dif f erences.
T h erap eutic effects
V arious clinical studies have shown that reducing F intak e improves ones’ metabolic situation, which is ex pected. T hus, intestinal side ef f ects due to F intolerance or ex cess F in f ood can be improved by a F- limited diet. M etabolic changes such as abdominal f at deposition, insulin resistance, ox idative stress and H T are improved by treatment with the antidiabetic metf ormin.3 7 ,1 0 2 - 1 0 5
C av eats and lim its of th e actual d atas et
As is of ten f ound in nutritional studies, many f actors, which can be controlled or not controlled, can bias interpretations of data. As a conseq uence, our present k nowledge must consider and eventually investigate these f actors bef ore delivering clear- cut conclusions.
Sp ecies
As discussed above, dif f erences in metabolic reactions to F have been described among various species: intra- species dif f erences among rat strains, inter- species dif f erences among mice, rats and hamsters and dif f erences between rodents and humans. T he presence of uricase in rats usually req uires the utiliz ation of high F concentrations in these animals, particularly when researchers wish to produce pathological individuals rapidly.
T yp e of food
I t is k nown that the source of F partly determines its harmf ulness; not only is it dif f erent among f resh fruits, f ruit j uices and sweetened sof t drink s, but some sources, such as honey, appear to be much saf er than others. Furthermore, several studies have shown that hormonal and metabolic reactions are more pronounced with liq uid F intak e than with solid F intak e, lik ely because of the bypass of the satiety process with liq uid F.
Another important caveat is that most clinical studies use sof t drink s as the source of F. H owever, usually other parameters, such as daily alimentary habits or lif estyle ( e.g., f ood type, activity levels) can af f ect ones’ metabolism. Focusing on F sof t drink s as the sole cause of metabolic
modiications limits the power of the data. T he same holds true f or vascular disturbances because colas and other sof t drink s contain many other molecules that could interf ere with vascular reactivity or induce glycation.
P rotocols
a) Study Duration
O ne maj or aspect of study protocols is the duration of the study. Available data have been obtained primarily f rom acute ( 2 - 2 4 h) or mid- term ( 1 - 4 week s) administration of F; only some data have been obtained f rom long-term investigations. I t is clear that acute and short- long-term administration of moderate and even high F will cause tissues to react against what they might sense as an aggression. We k now that metabolic disturbances take years to manif est as clinical symptoms due to stepwise developing compensations, metabolic adaptations and new eq uilibrium levels ( the development of T 2 D M is a good ex ample) . C oncerning F, the U A aspect may also illustrate how an initially positive reaction ( hyperuricemia) may turn into a negative one. Acute and chronic F administration can yield dif f erent results. T his has been observed f or T G levels, which were increased in acute but not chronic H F diets.1 0 1 M oreover, a recent report did not observe a correlation between F and U A over long time periods.9 3
b) Gender/Populations
c) Dosage
As discussed previously, F is only partly absorbed and rapidly leads to intestinal intolerance, which illustrates the f act that an H F condition is very dif f erent f rom a low F condition. H owever, most studies deal with high or very high F concentrations, which are not relevant to daily F consumption in humans, even if one considers ‘cola-addicted’ young people. M oreover, many studies were perf ormed in the U nited S tates using H FC S , a sweetener that is not used or is used only in limited amounts in many other countries. T hus, ex treme caution should be tak en when trying to develop irm conclusions.1 7 I n rats, moderate intak e of various sweeteners ( F, H FC S or agave) f or 3 nights per week during a 1 0 - week period increased serum alanine aminotransf erase levels, but no other serious disturbances, such as those seen with H F, were observed.5 4 I n humans, the
deleterious ef f ects seen with 2 0 - 2 5 % F as an energy source were not observed when more realistic q uantities of 4 - 1 2 % F were investigated.9 6
C O NC LUSIO NS
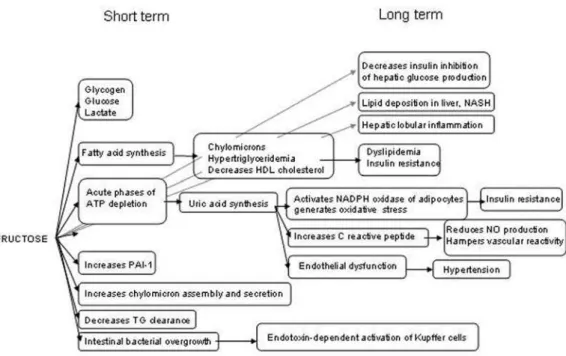
T he controversy that has ex isted f or the last 1 0 years regarding the potential harmf ulness of ex cess f ructose is legitimate in view of the dramatic increases in both sweetened beverage consumption and the burdens of obesity, M S and T 2 D M .1 0 8 T here is no doubt f rom many preclinical and clinical studies that H F can induce negative ef f ects on both energy metabolism and blood vessels ( summariz ed in Figure 2 ) .
U nf ortunately, the vast maj ority of the studies were perf ormed using protocols in which the duration or dosage of F administration was not relevant to common daily usage in the general population. Nevertheless, the merit of these studies was to provide valuable inf ormation as to what can be ex pected f rom ex cessive F intak e and the nature of the underlying mechanisms. H owever, many important conf ounding f actors were ignored, which mak es data interpretation too haz ardous to draw conclusions about the deleterious nature of H F.
Assuming there is no F intolerance, we inf er f rom the available dataset that F is harmless in healthy individuals, at least at levels below 5 0 - 1 0 0 g/ d. H owever, it also appears clear that individuals at risk f or metabolic syndromes, T 2 D M or cardiovascular diseases should be cautious because evidence shows that they are much more susceptible to H F than the general population. T hus, the controversy continues, and new protocols that tak e into account our present k nowledge and eliminate the af orementioned conf ounding f actors are req uired. From the available literature, f our main aspects of F intak e appear to be particularly important: a) the use of “natural” F sources ( sucrose) instead of H FC S or sweetened sof t drink s ( which contain many additional substances) , b) the use of relevant F concentrations based on ex isting data about common daily F consumption in the general population, c) the mix ing of male and f emale subj ects and d) the investigation of moderately elevated F over long periods of time.
REFERENC ES
1 . T appy L , L e K A. M etabolic ef f ects of f ructose and the worldwide increase in obesity. P hysiol Rev. 2 0 1 0 ; 9 0 :2 3 - 4 6 .
2 . Rao S S , Attaluri A, Anderson L , S tumbo P . Ability of the normal human small intestine to absorb f ructose: evaluation by breath testing. C lin Gastroenterol H epatol. 2 0 0 7 ; 5 :9 5 9 - 6 3 .
3 . Johnson RJ, P erez - P oz o S E , S autin Y Y , M anitius J, S anchez - L oz ada L G, Feig D I , et al. H ypothesis: could ex cessive f ructose intak e and uric
acid cause type 2 diabetes? E ndocr Rev. 2 0 0 9 ; 3 0 :9 6 - 1 1 6 .
4 . S k oog S M , B harucha AE . D ietary f ructose and gastrointestinal symptoms: a review. Am J Gastroenterol. 2 0 0 4 ; 9 9 :2 0 4 6 - 5 0 .
5 . Nuttall FQ , K han M A, Gannon M C . P eripheral glucose appearance rate f ollowing f ructose ingestion in normal subj ects. M etabolism. 2 0 0 0 ; 4 9 :1 5 6 5 - 7 1 .
6 . K miec Z . C ooperation of liver cells in health and disease. Adv Anat E mbryol C ell B iol. 2 0 0 1 ; 1 6 1 :I I I - X I I I , 1 - 1 5 1 .
7 . S polarics Z , O ttlak an A, L ang C H , S pitz er JJ. K upf f er cells play a maj or role in insulin- mediated hepatic glucose uptak e in vivo. B iochem B iophys Res C ommun. 1 9 9 2 ; 1 8 6 :4 5 5 - 6 0 .
8 . C ornell RP . M echanisms of acute hyperinsulinemia af ter K upf f er cell phagocytosis. Am J P hysiol. 1 9 8 0 ; 2 3 8 :E 2 7 6 - 8 3 .
9 . C lementi AH , Gaudy AM , van Rooij en N, P ierce RH , M ooney RA. L oss of K upf f er cells in diet- induced obesity is associated with increased hepatic steatosis, S T AT 3 signaling, and f urther decreases in insulin signaling. B iochim B iophys Acta. 2 0 0 9 ; 1 7 9 2 :1 0 6 2 - 7 2 .
1 0 . Neyrinck AM , C ani P D , D ewulf E M , D e B ack er F, B indels L B , D elz enne NM . C ritical role of K upf f er cells in the management of diet- induced diabetes and obesity. B iochem B iophys Res C ommun. 20 0 9 ; 3 8 5 :3 5 1 - 6 .
1 1 . H uang W, M etlak unta A, D edousis N, Z hang P , S ipula I , D ube JJ, et al. D epletion of liver K upf f er cells prevents the development of diet- induced
hepatic steatosis and insulin resistance. D iabetes. 2 0 1 0 ; 5 9 :3 4 7 - 5 7 .
1 2 . T ef f K L , Grudz iak J, T ownsend RR, D unn T N, Grant RW, Adams S H , et al. E ndocrine and metabolic ef f ects of consuming f ructose- and
glucose- sweetened beverages with meals in obese men and women: inluence of insulin resistance on plasma triglyceride responses. J C lin E ndocrinol M etab. 2 0 0 9 ; 9 4 :1 5 6 2 - 9 .
1 3 . L ivesey G, T aylor R. Fructose consumption and conseq uences f or glycation, plasma triacylglycerol, and body weight: meta- analyses and meta- regression models of intervention studies. Am J C lin Nutr. 2 0 0 8 ; 8 8 :1 4 1 9 - 3 7 .
1 4 . B erk ey C S , Rock ett H R, Field AE , Gillman M W, C olditz GA. S ugar- added
beverages and adolescent weight change. O bes Res. 2 0 0 4 ; 1 2 :7 7 8 - 8 8 .
1 5 . B arros C M , L essa RQ , Grechi M P , M ouco T L , S ouz a M G, Wiernsperger N, et al. S ubstitution of drink ing water by f ructose solution induces hyperinsulinemia and hyperglycemia in hamsters. C linics. 2 0 0 7 ; 6 2 :3 2 7 -3 4 .
1 6 . Jurgens H , H aass W, C astaneda T R, S churmann A, Koebnick C , D ombrowsk i F, et al. C onsuming f ructose- sweetened beverages increases body adiposity in mice. O bes Res. 2 0 0 5 ; 1 3 :1 1 4 6 - 5 6 .
1 7 . L ivesey G. Fructose ingestion: dose- dependent responses in health research. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 4 6 S - 5 2 S .
1 8 . S warbrick M M , S tanhope K L , E lliott S S , Graham JL, K rauss RM , C hristiansen M P , et al. C onsumption of f ructose- sweetened beverages f or 1 0 week s increases postprandial triacylglycerol and apolipoprotein- B concentrations in overweight and obese women. B r J Nutr. 2 0 0 8 ; 1 0 0 :9 4 7 - 5 2 .
1 9 . L e K A, Faeh D , S tettler R, I th M , K reis R, V ermathen P , et al. A 4 - wk high- f ructose diet alters lipid metabolism without af f ecting insulin
sensitivity or ectopic lipids in healthy humans. Am J C lin Nutr. 2 0 0 6 ; 8 4 :1 3 7 4 - 9 .
2 0 . L e K A, I th M , K reis R, Faeh D , B ortolotti M , T ran C , et al. Fructose overconsumption causes dyslipidemia and ectopic lipid deposition in
healthy subj ects with and without a f amily history of type 2 diabetes. Am J C lin Nutr. 2 0 0 9 ; 8 9 :1 7 6 0 - 5 .
2 1 . C ollison K S , S aleh S M , B ak heet RH , Al- Rabiah RK , I nglis AL , M ak houl NJ, et al. D iabetes of the liver: the link between nonalcoholic f atty liver
disease and H FC S - 5 5 . O besity ( S ilver S pring) . 2 0 0 9 ; 1 7 :2 0 0 3 - 1 3 .
2 2 . de M oura RF, Ribeiro C , de O liveira JA, S tevanato E , de M ello M A. M etabolic syndrome signs in Wistar rats submitted to dif f erent
high-f ructose ingestion protocols. B r J Nutr. 2 0 0 9 ; 1 0 1 :1 1 7 8 - 8 4 .
2 3 . B lak ely S R, H allf risch J, Reiser S , P rather E S . L ong- term ef f ects of moderate f ructose f eeding on glucose tolerance parameters in rats. J
Nutr. 1 9 8 1 ; 1 1 1 :3 0 7 - 1 4 .
2 4 . K awasak i T , I garashi K , K oeda T , S ugimoto K , Nak agawa K , H ayashi S , et al. Rats f ed f ructose- enriched diets have characteristics of
nonalcoholic hepatic steatosis. J Nutr. 2 0 0 9 ; 1 3 9 :2 0 6 7 - 7 1 .
2 5 . S artorelli D S , Franco L J, Gimeno S G, Ferreira S R, C ardoso M A. D ietary f ructose, f ruits, f ruit j uices and glucose tolerance status in Japanese-B raz ilians. Nutr M etab C ardiovasc D is. 2 0 0 9 ; 1 9 :7 7 - 8 3 .
2 6 . T sai C J, L eitz mann M F, Willett WC , Giovannucci EL . D ietary carbohydrates and glycaemic load and the incidence of symptomatic gall stone disease in men. Gut. 2 0 0 5 ; 5 4 :8 2 3 - 8 .
2 7 . S aldana T M , B asso O , D arden R, S andler D P . C arbonated beverages and chronic k idney disease. E pidemiology. 2 0 0 7 ; 1 8 :5 0 1 - 6 .
2 8 . K raj covicova- K udlack ova M , S ebek ova K , S chinz el R, K lvanova J. Advanced glycation end products and nutrition. Physiol Res. 2 0 0 2 ; 5 :3 1 3 - 6 .
2 9 . S ak ai M , O imomi M , K asuga M . E x perimental studies on the role of f ructose in the development of diabetic complications. K obe J M ed S ci.
2 0 0 2 ; 4 8 :1 2 5 - 3 6 .
3 0 . B ray GA. S of t drink consumption and obesity: it is all about f ructose. C urr O pin L ipidol. 2 0 1 0 ; 2 1 :5 1 - 7 .
3 1 . D ills WL , Jr. P rotein f ructosylation: f ructose and the M aillard reaction. Am J C lin Nutr. 1 9 9 3 ; 5 8 ( 5 S uppl) :7 7 9 S - 8 7 S .
3 2 . H inton D J, Ames JM . S ite speciicity of glycation and carbox ymethylation
of bovine serum albumin by f ructose. Amino Acids. 2 0 0 6 ; 3 0 :4 2 5 - 3 4 .
3 3 . Gul A, Rahman M A, H asnain S N. Role of f ructose concentration on cataractogenesis in senile diabetic and non- diabetic patients. Graef es Arch C lin E x p O phthalmol. 2 0 0 9 ; 2 4 7 :8 0 9 - 1 4 .
3 4 . M iyaz awa N, K awasak i Y , Fuj ii J, T heingi M , H oshi A, H amaok a R, et al. I mmunological detection of f ructated proteins in vitro and in vivo.
3 5 . T ok ita Y , H irayama Y , S ek ik awa A, K otak e H , T oyota T , M iyaz awa T , et al. Fructose ingestion enhances atherosclerosis and deposition of
advanced glycated end- products in cholesterol- f ed rabbits. J Atheroscler T hromb. 2 0 0 5 ; 1 2 :2 6 0 - 7 .
3 6 . B rown C M , D ulloo AG, Y epuri G, M ontani JP . Fructose ingestion acutely elevates blood pressure in healthy young humans. Am J P hysiol Regul I ntegr C omp P hysiol. 2 0 0 8 ; 2 9 4 :R7 3 0 - 7 .
3 7 . Wang X , Jia X , C hang T , D esai K , Wu L . Attenuation of hypertension development by scavenging methylglyox al in f ructose- treated rats. J
H ypertens. 2 0 0 8 ; 2 6 :7 6 5 - 7 2 .
3 8 . K hosla U M , Z harik ov S , Finch JL , Nak agawa T , Roncal C , M u W, et al. H yperuricemia induces endothelial dysf unction. K idney I nt.
2 0 0 5 ; 6 7 :1 7 3 9 - 4 2 .
3 9 . T erz uoli L , P orcelli B , P onticelli F, M arinello E . P urine nucleotide catabolism in rat liver. C ertain preliminary aspects of uricase reaction. Nucleosides Nucleotides Nucleic Acids. 2 0 0 9 ; 2 8 :1 9 3 - 2 0 3 .
4 0 . Nak agawa T , H u H , Z harik ov S , T uttle K R, S hort RA, Glushak ova O , et al. A causal role f or uric acid in f ructose- induced metabolic syndrome. Am J P hysiol Renal P hysiol. 2 0 0 6 ; 2 9 0 :F6 2 5 - 3 1 .
4 1 . Wiernsperger N, Nivoit P , D e Aguiar L G, B ousk ela E . M icrocirculation and the metabolic syndrome. M icrocirculation. 2 0 0 7 ; 1 4 :4 0 3 - 3 8 .
4 2 . Alz amendi A, Giovambattista A, Raschia A, M adrid V , Gaillard RC , Rebolledo O , et al. Fructose- rich diet- induced abdominal adipose tissue
endocrine dysf unction in normal male rats. E ndocrine. 2 0 0 9 ; 3 5 :2 2 7 - 3 2 .
4 3 . S celles V , Alessi M C , Raccah D , Juhan- V ague I , Vague P . P lasma plasminogen activator inhibitor activity in rats with nutritionally induced insulin resistance. T hromb H aemost. 1 9 9 5 ; 7 4 :8 0 6 - 7 .
4 4 . K osugi T , Nak amura M , S unagawa M . T ransition of pathophysiological signiicance of plasminogen activator inhibitor- From a chief player in antiinlammation, antiibrinolysis to that in the development of insulin resistance. P athophysiology.; 1 7 :1 0 9 - 1 8 .
4 5 . B asciano H , Federico L , Adeli K . Fructose, insulin resistance, and metabolic dyslipidemia. Nutr M etab ( L ond) . 2 0 0 5 ; 2 :5 .
4 6 . H sieh J, H ayashi AA, Webb J, Adeli K . P ostprandial dyslipidemia in insulin resistance: mechanisms and role of intestinal insulin sensitivity. Atheroscler S uppl. 2 0 0 8 ; 9 :7 - 1 3 .
4 7 . C hong M F, Fielding B A, Frayn K N. M echanisms f or the acute ef f ect of f ructose on postprandial lipemia. Am J C lin Nutr. 2 0 0 7 ; 8 5 :1 5 1 1 - 2 0 .
4 8 . M ayes P A. I ntermediary metabolism of f ructose. Am J C lin Nutr. 1 9 9 3 ; 5 8 ( 5 S uppl) :7 5 4 S - 6 5 S .
4 9 . T opping D L , M ayes P A. T he immediate ef f ects of insulin and f ructose on the metabolism of the perf used liver. C hanges in lipoprotein secretion,
f atty acid ox idation and esteriication, lipogenesis and carbohydrate metabolism. B iochem J. 1 9 7 2 ; 1 2 6 :2 9 5 - 3 1 1 .
5 0 . K oo H Y , Wallig M A, C hung B H , Nara T Y , C ho B H , Nak amura M T . D ietary f ructose induces a wide range of genes with distinct shif t in
carbohydrate and lipid metabolism in f ed and f asted rat liver. B iochim B iophys Acta. 2 0 0 8 ; 1 7 8 2 :3 4 1 - 8 .
5 1 . O uyang X , C irillo P , S autin Y , M cC all S , B ruchette JL , D iehl AM , et al. Fructose consumption as a risk f actor f or non- alcoholic f atty liver
disease. J H epatol. 2 0 0 8 ; 4 8 :9 9 3 - 9 .
5 2 . T obey T A, M ondon C E , Z avaroni I , Reaven GM . M echanism of insulin resistance in f ructose- f ed rats. M etabolism. 1 9 8 2 ; 3 1 :6 0 8 - 1 2 .
5 3 . Abid A, T aha O , Nseir W, Farah R, Grosovsk i M , Assy N. S of t drink consumption is associated with f atty liver disease independent of
metabolic syndrome. J H epatol. 2 0 0 9 ; 5 1 :9 1 8 - 2 4 .
5 4 . Figlewicz D P , I oannou G, B ennett Jay J, K ittleson S , S avard C , Roth C L . E f f ect of moderate intak e of sweeteners on metabolic health in the rat. P hysiol B ehav. 2 0 0 9 ; 9 8 :6 1 8 - 2 4 .
5 5 . Rapin JR, Wiernsperger N. P ossible link s between intestinal permeability and f ood processing: a therapeutic niche f or glutamine? C linics. 2 0 1 0 ; in press.
5 7 . S pruss A, K anuri G, Wagnerberger S , H aub S , B ischof f S C , B ergheim I . T oll- lik e receptor 4 is involved in the development of f ructose- induced hepatic steatosis in mice. H epatology. 2 0 0 9 ; 5 0 :1 0 9 4 - 1 0 4 .
5 8 . S k oog S M , B harucha AE , Z insmeister AR. C omparison of breath testing with f ructose and high f ructose corn syrups in health and I B S . Neurogastroenterol M otil. 2 0 0 8 ; 2 0 :5 0 5 - 1 1 .
5 9 . C orlew- Roath M , D i P alma JA. C linical impact of identif ying lactose maldigestion or f ructose malabsorption in irritable bowel syndrome or
other conditions. S outh M ed J. 2 0 0 9 ; 1 0 2 :1 0 1 0 - 2 .
6 0 . C hoi Y K , K raf t N, Z immerman B , Jack son M. Fructose , Rao S S intolerance in I B S and utility of f ructose- restricted diet. J C lin Gastroenterol. 2 0 0 8 ; 4 2 :2 3 3 - 8 .
6 1 . B eyer P L , C aviar E M , M cC allum RW. Fructose intak e at current levels in the U nited S tates may cause gastrointestinal distress in normal adults.
J Am D iet Assoc. 2 0 0 5 ; 1 0 5 :1 5 5 9 - 6 6 .
6 2 . Gibson P R, Newnham E , B arrett JS , S hepherd S J, M uir JG. Review article: f ructose malabsorption and the bigger picture. Aliment
P harmacol T her. 2 0 0 7 1 5 ; 2 5 :3 4 9 - 6 3 .
6 3 . Fernandez - B anares F, E steve M , V iver JMe- sorbitol . Fructos malabsorption. C urr Gastroenterol Rep. 2 0 0 9 ; 1 1 :3 6 8 - 7 4 .
6 4 . D iM eglio D P , M attes RD . L iq uid versus solid carbohydrate: ef f ects on f ood intak e and body weight. I nt J O bes Relat Mtab D isord. e 2 0 0 0 ; 2 4 :7 9 4 - 8 0 0 .
6 5 . V an Wymelbek e V , B eridot- T herond M E , de L a Gueronniere V , Fantino M . I nluence of repeated consumption of beverages containing sucrose
or intense sweeteners on f ood intak e. E ur J C lin Nutr. 2 0 0 4 ; 5 8 :1 5 4 - 6 1 .
6 6 . D ellaV alle D M , Roe L S , Rolls B J. D oes the consumption of caloric and non- caloric beverages with a meal af f ect energy intak e? Appetite.
2 0 0 5 ; 4 4 :1 8 7 - 9 3 .
6 7 . B antle JP . D ietary f ructose and metabolic syndrome and diabetes. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 6 3 S - 8 S .
6 8 . Wiernsperger NF. O x idative stress: the special case of diabetes. B iof actors. 2 0 0 3 ; 1 9 :1 1 - 8 .
6 9 . S anchez - L oz ada L G, M u W, Roncal C , S autin Y Y , Abdelmalek M , Reungj ui S , et al. C omparison of f ree f ructose and glucose to sucrose in the ability to cause f atty liver. E ur J Nutr. 2 0 1 0 ; 4 9 :1 - 9 .
7 0 . V uk ovic J, M odun D , B udimir D , S utlovic D , S alamunic I , Z aj a I , et al. Acute, f ood- induced moderate elevation of plasma uric acid protects
against hyperox ia- induced ox idative stress and increase in arterial
stif f ness in healthy humans. Atherosclerosis. 2 0 0 9 ; 2 0 7 :2 5 5 - 6 0 .
7 2 . Nieto FJ, I ribarren C , Gross M D , C omstock GW, C utler RG. U ric acid and serum antiox idant capacity: a reaction to atherosclerosis? Atherosclerosis. 2 0 0 0 ; 1 4 8 :1 3 1 - 9 .
7 3 . S autin Y Y , Nak agawa T , Z harik ov S , Johnson RJ. Adverse ef f ects of the classic antiox idant uric acid in adipocytes: NAD P H ox idase- mediated ox idative/ nitrosative stress. Am J P hysiol C ell P hysiol. 2 0 0 7 ; 2 9 3 :C 5 8 4 - 9 6 .
7 4 . Y oo H G, L ee S I , C hae H J, P ark S J, L ee Y C , Y oo WH. P revalence of insulin resistance and metabolic syndrome in patients with gouty arthritis. Rheumatol I nt. 2 0 0 9 ; 2 0 .
7 5 . C roymans D M , S anchez A, B arth JD , Roberts C K . C arotid intima- media thick ness, dietary intak e, and cardiovascular phenotypes in adolescents: relation to metabolic syndrome. M etabolism. 2 0 1 0 ; 5 9 :5 3 3 - 9 .
7 6 . K ramer C K , von M uhlen D , Jassal S K , B arrett- C onnor E . S erum uric acid levels improve prediction of incident type 2 diabetes in individuals
with impaired f asting glucose: the Rancho B ernardo S tudy. D iabetes C are. 2 0 0 9 ; 3 2 :1 2 7 2 - 3 .
7 7 . C hoi H K , C urhan G. S of t drink s, f ructose consumption, and the risk of gout in men: prospective cohort study. B mj . 2 0 0 8 ; 3 3 6 :3 0 9 - 1 2 .
7 8 . L ee K . Relationship between uric acid and hepatic steatosis among K oreans. D iabetes M etab. 2 0 0 9 ; 3 5 :4 4 7 - 5 1 .
7 9 . L in K P . T he relationship between serum uric acid concentration and metabolic syndrome in university f reshmen. J Nurs Res. 2 0 0 9 ; 1 7 :2 8 6 - 9 2 .
8 0 . Nak agawa T , T uttle K R, S hort RA, Johnson RJ. H ypothesis: f ructose-induced hyperuricemia as a causal mechanism f or the epidemic of the metabolic syndrome. Nat C lin P ract Nephrol. 2 0 0 5 ; 1 :8 0 - 6 .
8 1 . C hang C H , C hen Y M , C huang Y W, L iao S C , L in C S , T ang Y J, et al. Relationship between hyperuricemia ( H U C ) and metabolic syndrome
( M S ) in institutionaliz ed elderly men. Arch Gerontol Geriatr. 2 0 0 9 ; 4 9 S uppl 2 :S 4 6 - 9 .
8 2 . Feig D I , K ang D H , Johnson RJ. U ric acid and cardiovascular risk . N E ngl J M ed. 2 0 0 8 ; 3 5 9 :1 8 1 1 - 2 1 .
8 3 . Forman JP , C hoi H , C urhan GC . U ric acid and insulin sensitivity and risk of incident hypertension. Arch I ntern M ed. 2 0 0 9 2 6 ; 1 6 9 :1 5 5 - 6 2 .
8 4 . K anellis J, K ang D H . U ric acid as a mediator of endothelial dysf unction,
inlammation, and vascular disease. S emin Nephrol. 2 0 0 5 ; 2 5 :3 9 - 4 2 .
8 5 . S undstrom J, S ullivan L , D ’Agostino RB , L evy D , K annel WB , V asan RS . Relations of serum uric acid to longitudinal blood pressure track ing
and hypertension incidence. H ypertension. 2 0 0 5 ; 4 5 :2 8 - 3 3 .
8 6 . Wex ler B C , Greenberg B P . E f f ect of increased serum urate levels on virgin rats with no arteriosclerosis versus breeder rats with preex istent
arteriosclerosis. M etabolism. 1 9 7 7 ; 2 6 :1 3 0 9 - 2 0 .
8 8 . S traz z ullo P , P uig JG. U ric acid and ox idative stress: relative impact on cardiovascular risk ? Nutr M etab C ardiovasc D is. 2 0 0 7 ; 1 7 :4 0 9 - 1 4 .
8 9 . K ang D H , P ark S K , L ee I K , Johnson RJ. U ric acid- induced C - reactive protein ex pression: implication on cell prolif eration and nitric ox ide
production of human vascular cells. J Am S oc Nephrol. 2 0 0 5 ; 1 6 :3 5 5 3 - 6 2 .
9 0 . Angelopoulos T J, L owndes J, Z uk ley L , M elanson KJ, Nguyen V , H uf f man A, et al. T he ef f ect of high- f ructose corn syrup consumption on triglycerides and uric acid. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 4 2 S - 5 S .
9 1 . C hoi JW, Ford E S , Gao X , C hoi H K . S ugar- sweetened sof t drink s, diet sof t drink s, and serum uric acid level: the T hird National H ealth and
Nutrition E x amination S urvey. Arthritis Rheum. 2 0 0 8 ; 5 9 :1 0 9 - 1 6 .
9 3 . S un S Z , Flick inger B D , Williamson- H ughes P S , E mpie M W. L ack of association between dietary f ructose and hyperuricemia risk in adults.
Nutr M etab. ( L ond) . 2 0 1 0 ; 7 :1 6 .
9 4 . M elanson K J, Z uk ley L , L owndes J, Nguyen V , Angelopoulos T J, Rippe JM . E f f ects of high- f ructose corn syrup and sucrose consumption on circulating glucose, insulin, leptin, and ghrelin and on appetite in normal- weight women. Nutrition. 2 0 0 7 ; 2 3 :1 0 3 - 1 2 .
9 5 . M urphy S P . T he state of the science on dietary sweeteners containing f ructose: summary and issues to be resolved. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 6 9 S - 7 0 S .
9 6 . S chaef er E J, Gleason JA, D ansinger M L . D ietary fructose and glucose dif f erentially af f ect lipid and glucose homeostasis. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 5 7 S - 6 2 S .
9 7 . T hresher JS , P odolin D A, Wei Y , M az z eo RS , P agliassotti M J. C omparison of the ef f ects of sucrose and f ructose on insulin action and glucose tolerance. Am J P hysiol Regul I ntegr C omp P hysiol. 2 0 0 0 ; 2 7 9 :R1 3 3 4 - 4 0 .
9 8 . S oenen S , Westerterp- P lantenga M S . No dif f erences in satiety or energy intak e af ter high- f ructose corn syrup, sucrose, or milk preloads. Am J C lin Nutr. 2 0 0 7 ; 8 6 :1 5 8 6 - 9 4 .
9 9 . S tanhope K L , Grif f en S C , B air B R, S warbrick M M , K eim NL , H avel P J. T wenty- f our- hour endocrine and metabolic prof iles f ollowing
consumption of high- f ructose corn syrup- , sucrose- , f ructose- , and glucose- sweetened beverages with meals. Am J C lin Nutr. 2 0 0 8 ; 8 7 :1 1 9 4 - 2 0 3 .
1 0 0 . Ngo S ock E T , L e K A, I th M , K reis R, B oesch C , T appy L . E f f ects of a short- term overf eeding with f ructose or glucose in healthy young males.
B r J Nutr. 2 0 0 9 2 4 :1 - 5 .
1 0 1 . S tanhope K L , H avel P J. Fructose consumption: considerations f or f uture research on its ef f ects on adipose distribution, lipid metabolism, and insulin sensitivity in humans. J Nutr. 2 0 0 9 ; 1 3 9 :1 2 3 6 S - 4 1 S .
1 0 2 . Anurag P , Anuradha C V . M etf ormin improves lipid metabolism and attenuates lipid perox idation in high f ructose- f ed rats. D iabetes O bes M etab. 2 0 0 2 ; 4 :3 6 - 4 2 .
1 0 3 . B aret G, P eyronnet J, Grassi- K assisse D , D almaz Y , Wiernsperger N, Geloen A. I ncreased intraabdominal adipose tissue mass in f ructose
f ed rats: correction by metf ormin. E x p C lin E ndocrinol D iabetes. 2 0 0 2 ; 1 1 0 :2 9 8 - 3 0 3 .
1 0 4 . Faure P , Rossini E , Wiernsperger N, Richard M J, Favier A, H alimi S . An insulin sensitiz er improves the f ree radical def ense system potential and
insulin sensitivity in high f ructose- f ed rats. D iabetes. 1 9 9 9 ; 4 8 :3 5 3 - 7 .
1 0 5 . S rividhya S , Anuradha C V . M etf ormin improves liver antiox idant potential in rats f ed a high- f ructose diet. Asia P ac J C lin Nutr. 2 0 0 2 ; 1 :3 1 9 - 2 2 .
1 0 6 . T ran L T , Y uen V G, M cNeill JH . T he f ructose- f ed rat: a review on the mechanisms of f ructose- induced insulin resistance and hypertension.
M ol C ell B iochem. 2 0 0 9 ; 3 3 2 :1 4 5 - 5 9 .
1 0 7 . O da E , K awai R, S uk umaran V , Watanabe K . U ric acid is positively associated with metabolic syndrome but negatively associated with
diabetes in Japanese men. I ntern M ed. 2 0 0 9 ; 4 8 :1 7 8 5 - 9 1 .