ABSTRACT
http://dx.doi.org/10.1590/1678-775720150174
Deep pain sensitivity is correlated with
oral-health-related quality of life but not with prosthetic
factors in complete denture wearers
Yuri Martins COSTA1, André Luís PORPORATTI2, Priscila Brenner HILGENBERG-SYDNEY2, Leonardo Rigoldi BONJARDIM3, Paulo César Rodrigues CONTI2
1- Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Prótese, Bauru, SP, Brasil; Aarhus University, Department of Dentistry, Section of Orofacial Pain and Jaw Function, Aarhus, Denmark.
2- Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Prótese, Bauru, SP, Brasil.
3- Universidade de São Paulo, Faculdade de Odontologia de Bauru, Departamento de Ciências Biologicas, Bauru, SP, Brasil.
Corresponding address: Yuri Martins Costa - Departamento de Prótese - Faculdade de Odontologia de Bauru - Universidade de São Paulo - Al. Octavio
Pinheiro Brisolla, 9-75 - 17012-901 - Bauru - SP - Brazil - e-mail: [email protected]
6XEPLWWHG$SULO0RGL¿FDWLRQ-XO\$FFHSWHG-XO\
L
ow pressure Pain Threshold (PPT) is considered a risk factor for TemporomandibularDisorders (T0D) and is inÀuenced by psycholoJical variables 2bMectives To correlate deep pain sensitivity of masticatory muscles with prosthetic factors and Oral-Health-Related Quality of Life (OHRQoL) in completely edentulous subjects. Material and Methods: A total of 29 complete denture wearers were recruited. The variables were: a) Pressure Pain Threshold (PPT) of the masseter and temporalis; b) retention, stability, and tooth wear of dentures; c) 9ertical Dimension of Occlusion (9DO); d) Oral Health ,mpact Pro¿le (OH,P) adapted to orofacial pain. The Kolmogorov-Smirnov test, the Pearson Product-Moment correlation coef¿cient, the Spearman Rank correlation coef¿cient, the Point-%iserial correlation coef¿cient, and the %onferroni correction (D=1%) were applied to the data. Results: The mean age (standard deviation) of the participants was of 70.1 years (9.5)
and 2% of them were females. There were no signi¿cant correlations with prosthetic
factors, but signi¿cant negative correlations were found between the OH,P and the PPT of the anterior temporalis (r=-0.50, 95% CI-0.73 to 0.17, p=0.005). Discussion: The deep pain sensitivity of masticatory muscles in complete dentures wearers is associated with OHRQoL, but not with prosthetic factors.
Ke y w or ds: Complete denture. Masticatory muscles. Pain threshold. Quality of life.
I N TROD UCTI ON
Edentulism is highly prevalent in developing countries. In particular, 63% of the Brazilian elderly population wear complete dentures, and approximately 12% of the entire population is edentulous5. This warrants the need for a closer attention to this type of patient. The use of a complete denture is associated with impaired masticatory function, poor quality of life, and with oral lesions when the denture is inadequate8,12,28. However, the association with Temporomandibular Disorders (TMD) is tenuous; there is little solid evidence to the fact that edentulism is associated with TMD22. It is important to note that TMD is an
umbrella term that encompasses different clinical conditions affecting the Temporomandibular Joint (TMJ) and masticatory muscles21. Although the signs and symptoms of TMD are not necessarily risk factors for TMD onset, TMJ noises and masticatory muscle pain were the most prevalent in a sample of elderly Brazilians20.
historically associated with TMD14. Not only some mechanical/occlusal aspects are related to TMD signs or symptoms, but the biopsychosocial model for TMD development, as opposed to mechanistic concepts, has also been widely accepted16.
The Pressure Pain Threshold (PPT) can be de¿ned as the minimum intensity of a pressure perceived as painful. It is an accurate and valid method to measure deep pain sensitivity25. The outcome of a PPT test is very informative in terms of deciphering the pathophysiological mechanisms of pain perception, particularly when this test is associated with a comprehensive somatosensory assessment. Inasmuch as a low PPT is considered a risk factor for the onset of TMD23, it would be of valuable interest to determine whether any prosthetic aspect of complete dentures wearers can, in fact, be correlated with PPT values. In addition to these mechanical and structural aspects, it is also important to evaluate the inÀuence of Oral-Health-Related Quality of Life (OHRQoL) on the PPT of masticatory muscles, since psychological variables could play a role in the perception of muscle pain and in the variation of the PPT values27.
Based on the aforementioned, this study aimed to correlate the PPT values of the masticatory muscles with (1) retention, (2) stability, (3) tooth wear of dentures, (4) VDO, and (5) OHRQoL in completely edentulous subjects. The authors hypothesized a pr ior i that there would be a correlation among PPT values versus prosthetic factors (VDO, retention, stability and tooth wear) and versus the OHRQoL.
M ATERI AL AN D M ETH OD S
D e sign a n d e t h ics
This cross-sectional pilot study was conducted in accordance with the Declaration of Helsinki, and was approved by a local Human Research Ethics Committee.
Su bj e ct s a n d r e cr u it m e n t
The eligible subjects included complete edentulous patients of both genders, who sought prosthetic treatment from 2010 to 2011. The inclusion criteria were: a) older than 50 years of age; b) wearing maxillary and mandibular dentures for at least one year. The exclusion criteria were: a) history of facial trauma or craniofacial surgical procedures; b) oral lesions, xerostomia or other oral manifestations of systematic diseases, and neurological disorders; c) painful TMD ongoing or in the last 30 days; d) previous treatments performed in the last 6 months for TMD. Only one expert in prosthodontics and orofacial pain performed the clinical examination to assess eligibility. The study included 29 subjects who ful¿lled the above criteria. The informed consent was obtained from each
subjects selected, after fully explaining the study aims and procedures.
V a r ia ble s
The PPT, the quality of the dentures (retention, stability and tooth wear), the VDO and the OHRQoL were assessed. The measurements were performed by a different examiner, who was also an expert in prosthodontics and orofacial pain and blinded to the clinical assessment.
D e e p Pa in
The PPT was determined with a digital dynamometer (KRATOS®, Cotia, SP, Brazil), used to record both sides of the masseter (body) and of the temporalis muscle (anterior, middle, and posterior belly) (Figure 1). This device has a circular Àat tip (1 cm2) that was used to apply pressure with an application ratio of 0.5 kg/cm2/s. During the examination, the head of the subjects was ¿rmly supported by the hand of the examiner. The subjects were informed that the objective was to measure their pain threshold, and not their tolerance. The device also has a button controlled by the subject, who was asked to press it the instant a pain sensation was felt; at which time the pressure was stopped, the value was displayed and recorded. Each site was randomly measured twice, with a 5-minute rest interval between the readings. The ¿nal PPT values comprised the mean of 2 trials
made on both left and right sides.
D e n t u r e qu a lit y
The retention of the dentures was rated as satisfactory (slight to moderate resistance to vertical pull, and little resistance to lateral forces) or unsatisfactory (no resistance to vertical pull and lateral forces)3. Similarly, stability was classi¿ed as satisfactory (no more than slight horizontal displacement or rotation movements when under pressure) or unsatisfactory (severe horizontal displacement or rotation movements when under pressure)3. Tooth wear was scored subjectively as follows: 0=no wear, 1=slight wear and 2=severe wear.
V e r t ica l D im e n sion of Occlu sion ( V D O)
The VDO was assessed quantitatively (VDOquant) by the Willis Gauge (vertical measurement from the subnasal region to the lower border of the chin, with the teeth in occlusion). In addition, the quality (VDOquali) was considered adequate or inadequate, based on the following techniques: facial measurement (Willis Method), phonetics and esthetic appearance2.
O r a l - H e a l t h - R e l a t e d Q u a l i t y o f L i f e ( OH RQoL)
The inÀuence of the oral condition on quality of life was assessed using the Oral Health Impact Pro¿le (OHIP) questionnaire adapted for orofacial pain patients17. This version is a short form of the original OHIP-49, which was validated for Brazilian Portuguese and showed good psychometrics (Cronbach’s alpha=0.963)18. The subjects were asked to score how often they experienced the impact of 30 statements in the last 6 months, based on a 5-point ordinal scale (0-4). Accordingly, the OHIP scores could range from 0 to 150, in which the higher scores indicated poor quality of life. Moreover, the questions and scores can be categorized into 6 dimensions: functional limitation, psychological discomfort, physical disability, psychological disability, social disability, and handicap.
St a t ist ica l a n a ly sis
Quantitative variables (age, PPT, OHIP, and VDOquant) were expressed as means and as Standard Deviation (SD), and included a description of the gender distribution, denture retention, stability, tooth wear, and VDOquali. All quantitative variables were assessed for normal distribution, using the Kolmogorov-Smirnov test before performing the inferential analysis. The log10 transformation was applied in cases of abnormal distribution of the quantitative variables, i.e., social disability and handicap dimensions of the OHIP.
The Pearson Product-Moment Correlation
Coefficient was used to correlate PPT values with VDOquant and OHIP (total score and the 6 dimensions). Similarly, the Spearman Rank Correlation Coef¿cient was used to correlate PPT values and denture tooth wear. Lastly, the point-biserial correlation coef¿cient was used to correlate PPT values with denture retention and stability, and VDOquali. The magnitude of each effect measured was based on the r coef¿cient, and was scored as a small (r=0.3), moderate (r=0.5), or strong (r=0.7) correlation along with the 95% con¿dence interval (CI). The sample size in this study was considered too small to use regression models. In this respect, the problem of multiple comparisons was averted by applying a Bonferroni correction, lowering the signi¿cance level to 1% (Į=0.01) as the cut-off point to determine the statistical signi¿cance.
RESULTS
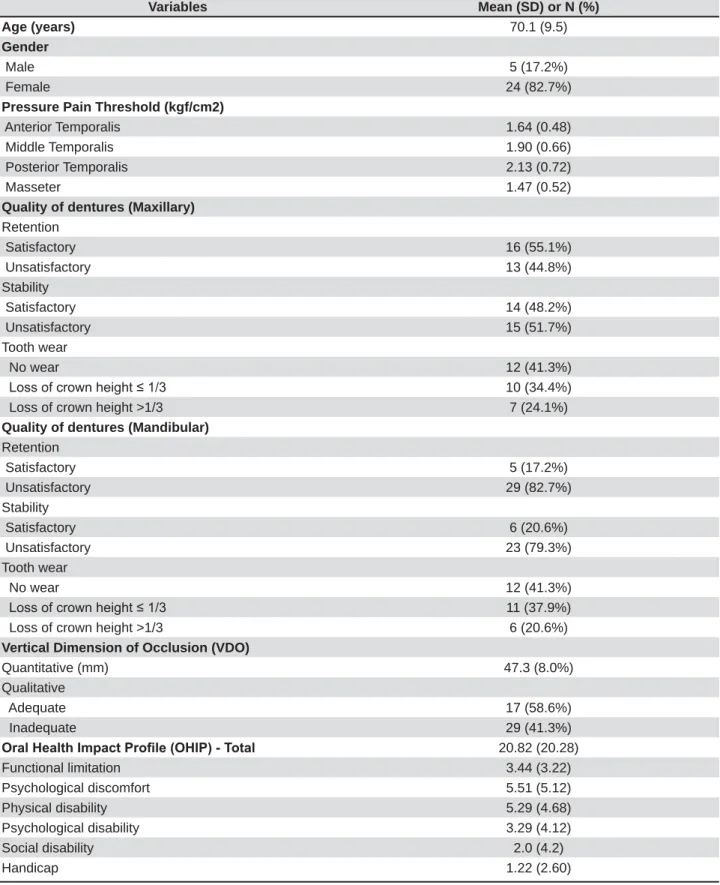
The clinical and demographic characteristics of the sample are detailed in Table 1. Mean age (SD) was 70.1 years (9.5) and 82% of the patients were females. The mean (SD) of the PPT values (kgf/ cm2) for all three bellies (anterior, middle, and posterior) of the temporalis and for the masseter muscles were 1.64 (0.48), 1.90 (0.66), 2.13 (0.72), and 1.47 (0.52), respectively. The distribution of the maxillary dentures quality was similar, with satisfactory retention (55%) and stability (48%). Most of the mandibular dentures had unsatisfactory retention (82%) and stability (79%). Twenty-four percent of the maxillary and 20% of the mandibular dentures had severe tooth wear. The mean (SD) of the VDO in mm was 47.3 (8.0), and was considered adequate (VDOquali) in 58% of the patients. Finally, the mean (SD) of the OHIP was 20.82 (20.28).
No signi¿cant correlations were found between the PPT values and denture quality or VDOquant/
quali after performing the Bonferroni correction (p!0.01). However, the correlation was signi¿cant, when considering the standard signi¿cance level (p<0.05) between tooth wear and PPT values of the anterior temporalis (maxillary denture, r= -0.38, 95% CI -0.66 to -0.01, p=0.03; mandibular denture, r=-0.38, 95% CI -0.66 to -0.01, p=0.03).
handicap dimension presented signi¿cant negative correlations of moderate magnitude with the PPT values for the anterior (r=-0.57, 95% CI -0.77 to -0.26, p=0.001), middle (r=-0.47, 95% CI -0.71 to -0.13, p=0.008), and posterior temporalis muscle
(r=-0.48, 95% CI -0.72 to -0.13, p=0.008) (Figure 3).
Variables Mean (SD) or N (%)
Age (years) 70.1 (9.5)
Gender
Male 5 (17.2%)
Female 24 (82.7%)
Pressure Pain Threshold (kgf/cm2)
Anterior Temporalis 1.64 (0.48)
Middle Temporalis 1.90 (0.66)
Posterior Temporalis 2.13 (0.72)
Masseter 1.47 (0.52)
Quality of dentures (Maxillary) Retention
Satisfactory 16 (55.1%)
Unsatisfactory 13 (44.8%)
Stability
Satisfactory 14 (48.2%)
Unsatisfactory 15 (51.7%)
Tooth wear
No wear 12 (41.3%)
/RVVRIFURZQKHLJKW 10 (34.4%)
Loss of crown height >1/3 7 (24.1%)
Quality of dentures (Mandibular) Retention
Satisfactory 5 (17.2%)
Unsatisfactory 29 (82.7%)
Stability
Satisfactory 6 (20.6%)
Unsatisfactory 23 (79.3%)
Tooth wear
No wear 12 (41.3%)
/RVVRIFURZQKHLJKW 11 (37.9%)
Loss of crown height >1/3 6 (20.6%)
Vertical Dimension of Occlusion (VDO)
Quantitative (mm) 47.3 (8.0%)
Qualitative
Adequate 17 (58.6%)
Inadequate 29 (41.3%)
2UDO+HDOWK,PSDFW3UR¿OH2+,37RWDO 20.82 (20.28)
Functional limitation 3.44 (3.22)
Psychological discomfort 5.51 (5.12)
Physical disability 5.29 (4.68)
Psychological disability 3.29 (4.12)
Social disability 2.0 (4.2)
Handicap 1.22 (2.60)
SD=Standard Deviation
D I SCUSSI ON
This cross-sectional pilot study evaluated the correlation between deep pain sensitivity of masticatory muscles and prosthetic aspects, and also between the former factor and the oral-related quality of life of complete denture wearers. The main ¿ndings were: a) there is no correlation between masticatory muscle sensitivity and prosthetic aspects; b) the greater the temporalis muscle sensitivity, the poorer the OHRQoL.
Our sample was composed of subjects without any ongoing TMD, presenting no complaints of masticatory myofascial or TMJ pain. There is
no consensus on TMD prevalence or incidence either in the elderly population or in complete denture wearers. However, a recently published cross-sectional study that adopted the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) showed similar prevalence ¿gures for the various types of TMD in Brazilian complete denture wearers: myofascial pain (16.3%), disc displacements (10.8%), and arthralgia, osteoarthritis and osteoarthrosis (19.5%)19. Furthermore, ¿ndings of low impact on OHRQoL related to facial pain were similar to the evidence revealed in previous studies6.
Muscle pain in the elderly population could be Figure 2-&RUUHODWLRQEHWZHHQSUHVVXUHSDLQWKUHVKROG337RIWKHDQWHULRUWHPSRUDOLVDQGWKH2UDO+HDOWK,PSDFW3UR¿OH
associated with the effects of aging and also with weak and impaired muscle activity, resulting from the long-term use of complete dentures8,15. In fact, pain in the masseter area or masticatory muscle pain on palpation has been associated with the use of complete dentures22. Moreover, among the collection of signs and symptoms of TMD, muscle pain could be considered a risk factor for TMD onset23. Indeed, epidemiological studies have shown that low PPT values were signi¿cantly associated with a higher prevalence of chronic TMD, and could be considered a predictor of TMD incidence23. Furthermore, the lower PPT values of the ¿rst-onset of TMD cases represented a signi¿cant predictor that TMD could become persistent24. For this reason, measuring PPT values in the TMD-free subjects is valuable in terms of devising preventive strategies or performing risk analyses.
No relationship was found between PPT and prosthetic factors. This is in line with the current concept that considers the multifactorial etiology of muscle pain, particularly masticatory myofascial pain, since mechanical and occlusal aspects seem to play a minor role in TMD development16. The evidence supporting the association of prosthetic factors with signs and symptoms of TMD is tenuous, and there is no association of these factors with TMD diagnosis19,22. Nonetheless, there was a trend in the correlation between PPT of the anterior temporalis and tooth wear. This could be related to the weakening of jaw muscles, or an impaired muscle function associated with the use of complete dentures7.
The inÀuence of emotions and psychological aspects on clinical and experimental pain is well-established11. In particular, stress periods are associated with decreased PPT values in masticatory myofascial pain patients27. Moreover, depression symptoms and catastrophic thoughts could partially explain the PPT variation related to neck muscles29. In line with these concepts, a patient’s perception of oral health also bears implications on pain symptomatology. A study similar to ours showed that a high degree of pressure pain sensitivity is correlated with a poor quality of life in the working population4. Our results also support the biopsychosocial model of pain, considering that low PPT values of the anterior temporalis were associated with a poor OHRQoL. The muscle of the temporalis had a bearing on the results of all the correlations. This could be explained by the microstructural differences between the masseter and the temporalis. The latter is mainly responsible for moving or stabilizing the mandible, whereas the former is a power muscle with high fatigue resistance26. Lastly, it is important to note that the PPT could be inÀuenced by other factors, such as metabolism, lifestyle, and aging15,30. The effect of
aging on PPT is controversial; however, evidence related to the temporalis muscle showed that PPT increases with age, thus reinforcing the signi¿cance of our results13.
The correlations between functional limitation and handicap domains with the PPT values of the muscle of the temporalis were also an interesting ¿nding. The subscale analysis showed divergent results in a TMD population, in which the mainly affected dimensions were psychological discomfort and disability10. These differences could be explained by the particularities of this study sample (elderly and edentulous). Moreover, we cannot rule out the potential response bias related to unspeci¿c facial pain symptoms not necessarily related to TMD pain, which could affect this population12. Although the internal consistency of the OHIP is high (Cronbach’s alpha = 0.963)18, it is important to note the psychometric properties of the OHIP are characteristics of the instrument in a speci¿c population and not of the instrument itself. That said, the use of instruments originally designed for the elderly population, e.g., the Geriatric Oral Health Assessment Index (GOHAI)9, may be more adequate. Therefore, more research is needed to explore the relationship between PPT and OHRQoL in the elderly in greater detail.
This study offers some insights concerning the relationship between prosthetic aspects and masticatory muscles, and between quality of life of complete denture wearers and masticatory muscles. However, some major limitations should be pointed out: 1) the lack of a control group of dentate patients and of patient self-assessment of denture quality, which makes the drawing of convincing conclusions unsubstantial and precludes the control of confounding factors; 2) there is a possibility of examiner bias associated with the subjective methods used to evaluate the quality of dentures and of the VDO. Although the present study followed guidelines taken from the evidence of other studies3, the authors recognize the paucity of criteria with high enough values of validity and reliability to assess the prosthetic aspects of complete dentures.
CON CLUSI ON
ACKN OW LED GM EN TS
We thank the Scholarship Program for Scienti¿c Initiation (PIBIC) of the National Council for Scienti¿c and Technological Development (CNPq).
REFEREN CES
1- Abdelnabi MH, Swelem AA. InÀuence of defective complete dentures renewal on TMD; an MRI and clinical controlled prospective study. Gerodontology. 2015;32:211-21.
2- Abduo J, Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012;57:2-10. 3- Alfadda SA. The relationship between various parameters of complete denture quality and patients' satisfaction. J Am Dent Assoc. 2014;145:941-8.
4- Ballegaard S, Petersen PB, Gyntelberg F, Faber J. The association between pressure pain sensitivity, and answers to questionnaires estimating psychological stress level in the workplace. A feasibility study. Scand J Clin Lab Invest. 2012;72:459-66.
5- Brazil. Ministry of Health. SB BRAZIL 2010: National Research on Oral Health: main results. [cited Oct. 2014]. Available from: http://189.28.128.100/dab/docs/geral/projeto_sb2010_relatorio_
¿nal.pdf.
6- Calderon PS, Hilgenberg PB, Rossetti LM, Laurenti JV, Conti PC. InÀuence of tinnitus on pain severity and quality of life in patients with temporomandibular disorders. J Appl Oral Sci. 2012;20:170-3.
7- Caloss R, Al-Arab M, Finn RA, Lonergan O, Throckmorton GS. Does long-term use of unstable dentures weaken jaw muscles? J Oral Rehabil. 2010;37:256-61.
8- Caloss R, Al-Arab M, Finn RA, Throckmorton GS. The effect of denture stability on bite force and muscular effort. J Oral Rehabil. 2011;38:434-9.
9- Campos JA, Zucoloto ML, Geremias RF, Nogueira SS, Maroco J. Validation of the Geriatric Oral Health Assessment Index in complete denture wearers. J Oral Rehabil. 2015;42:512-20. 10- Dahlstrom L, Carlsson GE. Temporomandibular disorders and oral health-related quality of life. A systematic review. Acta Odontol Scand. 2010;68:80-5.
11- Fillingim RB, Ohrbach R, Greenspan JD, Knott C, Diatchenko L, Dubner R, et al. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013;14:T75-90.
12- Jainkittivong A, Aneksuk V, Langlais RP. Oral mucosal lesions in denture wearers. Gerodontology. 2010;27:26-32.
13- Jensen R, Rasmussen BK, Pedersen B, Lous I, Olesen J. Cephalic muscle tenderness and pressure pain threshold in a general population. Pain. 1992;48:197-203.
14- Klasser GD, Greene CS. Oral appliances in the management of temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:212-23.
15- Lautenbacher S, Kunz M, Strate P, Nielsen J, Arendt-Nielsen L. Age effects on pain thresholds, temporal summation and spatial summation of heat and pressure pain. Pain. 2005;115:410-8.
16- Maixner W, Diatchenko L, Dubner R, Fillingim RB, Greenspan JD, Knott C, et al. Orofacial pain prospective evaluation and risk assessment study - the OPPERA study. J Pain. 2011;12:T4-11. e1-2.
17- Murray H, Locker D, Mock D, Tenenbaum HC. Pain and the quality of life in patients referred to a craniofacial pain unit. J Orofac Pain. 1996;10:316-23.
18- Pires CP, Ferraz MB, Abreu MH. Translation into Brazilian Portuguese, cultural adaptation and validation of the oral health impact pro¿le (OHIP-49). Braz Oral Res. 2006;20:263-8. 19- Ribeiro JA, Resende CM, Lopes AL, Farias-Neto A, Carreiro AD. Association between prosthetic factors and temporomandibular disorders in complete denture wearers. Gerodontology. 2014;31:308-13.
20- Santos JF, Marchini L, Campos MS, Damiao CF, Cunha VP, Barbosa CM. Symptoms of craniomandibular disorders in elderly Brazilian wearers of complete dentures. Gerodontology 2004;21:51-2.
21- Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014;28:6-27.
22- Sipill K, Nlplnkangas R, K|n|nen M, Alanen P, Suominen AL. The role of dental loss and denture status on clinical signs of temporomandibular disorders. J Oral Rehabil. 2013;40:15-23. 23- Slade GD, Fillingim RB, Sanders AE, Bair E, Greenspan JD, Ohrbach R, et al. Summary of ¿ndings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder: implications and future directions. J Pain. 2013;14:T116-24.
24- Slade GD, Sanders AE, Ohrbach R, Fillingim RB, Dubner R, Gracely RH, et al. Pressure pain thresholds Àuctuate with, but do not usefully predict, the clinical course of painful temporomandibular disorder. Pain. 2014;155:2134-43.
25- Svensson P, Baad-Hansen L, Pigg M, List T, Eliav E, Ettlin D, et al. Guidelines and recommendations for assessment of somatosensory function in oro-facial pain conditions - a taskforce report. J Oral Rehabil. 2011;38:366-94.
26- Van Eijden TM, Turkawski SJ. Morphology and physiology of masticatory muscle motor units. Crit Rev Oral Biol Med. 2001;12:76-91.
27- Vedolin GM, Lobato VV, Conti PC, Lauris JR. The impact of stress and anxiety on the pressure pain threshold of myofascial pain patients. J Oral Rehabil. 2009;36:313-21.
28- Visscher CM, Lobbezoo F, Schuller AA. Dental status and oral health-related quality of life. A population-based study. J Oral Rehabil. 2014;41:416-22.
29- Walton DM, Levesque L, Payne M, Schick J. Clinical pressure pain threshold testing in neck pain: comparing protocols, responsiveness, and association with psychological variables. Phys Ther. 2014;94:827-37.