w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Colorectal
cancer:
comparative
analysis
of
clinical
and
pathological
characteristics
in
patients
aged
above
and
below
45
years
of
age
and
impact
on
prognosis
Joana
Sofia
Gomes
Pestana
a,
Sandra
Fátima
Fernandes
Martins
a,b,c,∗aUniversidadedoMinho,FaculdadedeCiênciasdaSaúde,LifeandHealthSciencesResearchInstitute(ICVS),Braga,Portugal
bPTGovernmentAssociateLaboratory,LifeandHealthSciencesResearchInstitute/3B’s(ICVS/3B’s),Braga/Guimarães,Portugal
cCentroHospitalardeTrás-os-MonteseAltoDouro,DepartamentodeCirurgia,Braga,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received23January2015 Accepted23April2016 Availableonline22June2016
Keywords:
Colorectalcancer Age
Clinicopathologicalfeatures Survival
a
b
s
t
r
a
c
t
Introduction:Colorectalcancer,inPortugal,presentsasthesecondmostcommoncancerand
ofcancerdeathcause.CRCisadiseaseoftheelderly;however,therehasbeenanincreaseof incidenceinyoungerpatientsanddoubtshaveemergedaboutitsbehavior,characteristics andprognosisinthisgroup.
Methods:Inthisstudy,wehaveevaluatedasampleof512patientsdiagnosedwithcolorectal
cancersubmittedtosurgicaltreatmentintheperiodbetweenJanuary1st,2005and Jan-uary1st,2010,throughacomparativeclinical,pathologicalandsurvivalanalysisofpatients underandover45yearsold(GroupsIandIIrespectively).
Results:GroupIpatientsaccountedfor5.5%ofthesample.Therewasapredominanceof
malesandthemostcommonsitewastheleftcoloninbothagegroups.Intheyoungergroup, thehistologicaltypepresentswithapredominanceoftumorswithamucinouscomponent andwithsignetringcells(p=0.001),however,therewasnodifferenceintermsofoverall survivalanddisease-freesurvival.
Conclusion:Inthisstudy,colorectalcanceratyoungeragesshowssimilarcharacteristicsto
thoseofolderpatients.
©2016SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](S.F.Martins).
http://dx.doi.org/10.1016/j.jcol.2016.04.010
Câncer
colorretal:
análise
comparativa
das
características
clínicas
e
anatomopatológicas
em
doentes
com
idade
superior
e
inferior
a
45
anos
de
idade
e
impacto
no
prognóstico
Palavras-chave:
Câncercolorretal Idade
Característicasclínicase anatomopatológicas Sobrevida
r
e
s
u
m
o
Introduc¸ão: OCâncerColorectal(CCR),emPortugal,constituiosegundocâncermais
fre-quenteem termosdeincidênciaedemortalidade.Éumadoenc¸adoidoso,noentanto, tem-seobservado umaumentoda incidênciaem pacientesmaisjovens,tendosurgido dúvidasacercadoseucomportamento,característicaseprognósticonestegrupoetário.
Métodos: 512pacientescomdiagnósticodeCCRoperadosentreJaneirode2005eJaneiro
de2010foramavaliadosatravésdaanálisecomparativadascaracterísticasclínicas, anato-mopatológicasesobrevidaemindivíduoscomidadeinferioresuperiora45anos(GrupoIe IIrespetivamente).
Resultados: OspacientesdoGrupoIrepresentaram5,5%daamostra.Houvepredomínio
dogêneromasculinoeolocalmaisfrequentefoiocólonesquerdoemambososgrupos. Nogrupomaisjovem,relativamenteaotipohistológicoocorreupredomíniosignificativo detumorescomcomponentemucinosoecélulasemaneldesinete(p=0,001),massem diferenc¸aaoníveldasobrevidaglobalesobrevidalivrededoenc¸a.
Conclusão: Nesteestudo,oCCRemidadesmaisjovensreveloucaracterísticassemelhantes
àsdospacientesmaisidosos.
©2016SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/
licenses/by-nc-nd/4.0/).
Introduction
Inrecentdecades,therehasbeenanincreasingprevalence ofcancersintheworld.1,2Colorectalcancer(CRC)isthemost
commonmalignancyofthegastrointestinaltract3,4anddueto
theincreasedincidenceandmortalitythatoccurredinrecent decades,andalsotothecoststhatareassociatedwith diag-nosisandtreatment,thiscancerhasbecomeamajorpublic healthproblemworldwide.5
Worldwide,CRCisthe3rdmostcommoncancerandthe 4thleadingcauseofdeathsbycancer;in2008,609,051deaths occurred,223,268oftheminEurope.3
About95%ofallCRCsarisefromadenomatouspolypsof the intestinalmucosa, with increasingincidencewith age; however,only10%ofadenomaswillresultinaCRC.6–9
Theknowledgeofthenaturalhistoryofthediseaseandthe possibilityofinterveningatanearlierstageledtothe imple-mentationofscreeningprograms,whichcurrentlycoverthe populationover50yearswithnoriskfactorsforCRC.10,11
There are several risk factors that are associated with the developmentofCRC, and someofthem implyan ear-lierscreening.12–14Ageisoneofthemainriskfactorsforthe
developmentofCRC,withover90%ofcasesoccurringin indi-vidualsagedover50years,withameanageofdiagnosisof65 years.14–16Forthisreason,CRCisconsideredadiseaseofthe
elderly.
Thepopulationunder50yearsandwithoutriskfactorsis excludedfrom the screening groupand istherefore some-whatneglected,andthisrequiresahighindexofsuspicion bythephysicianfortheestablishmentofadiagnosisofCRC. Althoughoccurringlessfrequently,CRCisalsodiagnosedin thisage group,and there hasbeenan increasedincidence
amongthesepeople,afactthatcannotbeignored.17–19
Pre-viousstudiesdescribeawidevariationofthisfrequency,with valuesfrom1.3%to37%,andthehighestvaluesarefoundin theAsianpopulation.19–27Thisissuehasarousedgreat
inter-estinthemedicalliterature,thoughwithcontroversialresults, and many studies havebeen conducted inorder to evalu-atepossibledifferencesinbehaviorandprognosisofCRCin youngpeoplecomparedwiththegeneralpopulationwiththis cancer.Mostauthorsarguethatyoungageisassociatedwith moreadvancedstagesofthe diseaseatdiagnosis andwith moreaggressivehistopathologiccharacteristics,forexample, alowerdegreeofdifferentiationandmucinsecretion.19,23,24
Someauthorsstilldescribeaworseprognosisinthisgroup.26
However,otherstudiescontradictthesefindings,describing resultssimilartothoseofpatientswithalaterdiagnosis,or evenwithimprovementintheirsurvival.21,22,27
Takingintoaccountthecontroversyonthissubjectandthe lackofstudiesinPortugal,thisprojectwascarriedoutinorder tomakeacomparativeanalysisoftheclinicalandpathological characteristicsofpatientswithCRCdiagnosedwithagesover andunder45years,andtoevaluatethepossibleimpactofthe agefactorinitsprognosis.
Methods
Exclusioncriteriawere:patientswithinflammatorybowel disease(IBD),namelyCrohn’sdiseaseandulcerativecolitis; patientswithhereditarysyndromessuchasfamilial adeno-matouspolyposis(FAP)andhereditarycolorectalcancernot associatedwithpolyposis(HCCNP);patientswithnoprimary diseaseofthecolonorrectum;patientsdiagnosedwithCRC butwhodidnotundergosurgery,andpatientswithCRC under-goingnon-curativesurgicaltreatment.
Theexclusionofpatientswithhereditarysyndromeswas performedafterconfirmedbygeneticstudiesinpatientsfor whomtherewasaclinicalsuspicion.
Tocollectinformation,aprospectivedatabaseofCRCwas surveyed,andthefollowingdatawerecollected:
Clinicaldataandpreoperativetests
Informationconcerningtheage,gender,clinicalpresentation, tumorlocationandthepresenceofmetastasiswasevaluated. Regardingage,thepatientsweregroupedintoageunderor equalto45years(GroupI)andmorethan45years(GroupII).
Pathologicaldata
Theparametersevaluatedincludedtumorsize,macroscopic appearance ofthe tumor, histologic type,tumor extension (pT), tálusdegreeofdifferentiation, the presenceoflymph nodemetastases(pN),presenceofvenousandlymphatic inva-sion,andstaging.
ThestagingwascarriedoutaccordingtotheTNM classi-ficationoftheAmericanJointCommitteeonCancer(AJCC), SixthEdition.28
Follow-up
Thepatientsweremonitoredregularly.
Thefollow-upofpatientswithCRCissubdividedintothree periods:1stand2ndyear,3rdto5thyear,andfrom6thyear postoperatively.Thus,inthe1stand2ndyears,thepatients areevaluatedinquarterlyconsultations;from3rdto5thyear, the assessment becomes biannual, and after 5 years, the patientisevaluatedannually.Intheseconsultations,besides patientobservation,tumormarkers(CEAandCA19-9)arealso accessed,andanannualchestX-rayisobtained.
Regardingcolonoscopy,theprocedureisperformedwithin oneyearaftersurgicalresection(or3–6monthsaftersurgery, if the colonoscopywas notperformed pre- or transopera-tively dueto anobstructive lesion) with repetition3years aftersurgery;subsequently,acolonoscopyisobtainedevery 5years,unlessafollow-upcolonoscopyrevealsevidenceofan advancedadenoma(villouspolyp,polyp>1cm,orhigh-grade dysplasia).Inthiscase,thecolonoscopyshouldberepeated1 yearafterpolypectomy.
Regardingtherealizationofcomputerizedaxial tomogra-phy,thisprocedureisperformedannuallyinthefirst three yearsaftersurgery,orwheneversymptomsoranincreaseof tumormarkerswarrantthisprocedure.Inthecaseofrectal cancer,apelvicNMRisalsoperformed6months postopera-tively,whichwillremainasreferenceNMR.
Themomentofdiagnosiswasusedasstartingpointfor survival analysis. In the case ofoverall survival, this was
calculated until the patient’s death for any reason, and disease-freesurvivalwasconsideredasthetimeelapseduntil the occurrenceofarelapse. Bothindicatorswereevaluated untilAugust31,2012.
Statisticalanalysis
TheStatisticalPackageforSocialSciencesforWindows(SPSS version19.0.0,SPSSInc.)wasusedinthedatabaseanalysis.
Statistical comparisonsbetweengroupswere performed usingthePearson’schi-squaredtest(X2)wheneverpossible,
andtheFisher’sexacttest(values<5).
Overallsurvivalanddisease-freesurvivalcurveswere cal-culatedusingtheKaplan–Meiermethod,andthecomparison betweenthe twogroupswas performedusingthe log-rank test.
p-values<0.05wereconsideredstatisticallysignificant. Thisstudywassubmittedto,andapprovedby,theBraga HospitalEthicsCommittee.
Results
IntheperiodbetweenJanuary1,2005,andJanuary1,2010,672 patientswithCRCwerediagnosedinBH;512patientsmetthe criteriapreviouslydescribed.
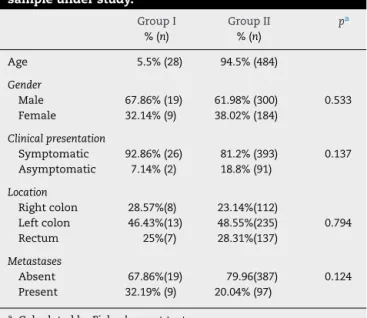
GroupIaccountedfor5.5%(n=28)ofthesampleandGroup IIfor94.5%(n=484).Inbothgroupsapredominanceofmales wasnoted:67.86%(n=19)forGroupIand61.98%(n=300)for GroupII,withnostatisticallysignificantdifference(p=0.533). Mostpatientsinbothgroupshadsymptomsatthemomentof diagnosis(92.86%,n=26and81.2%,n=393,respectively).The mostcommonsitewastheleftcolon,withatotalof48.44% ofcases(n=248)followedbytherectumwith28.13%(n=144) andtherightcolonwith23.44%(n=120).Comparingthesite byagegroup,wefoundsimilarresults.
At diagnosis, we found that 32.19% (n=9) and 20.04% (n=97),respectively,hadmetastases.Astothevariables stud-ied,nosignificantdifferenceswereobservedbetweengroups
(Table1).
Table1–Distributionofvariablesrelatedtoclinicaland preoperativetestdata,accordingtotheagegroup,inthe sampleunderstudy.
GroupI GroupII pa %(n) %(n)
Age 5.5%(28) 94.5%(484)
Gender
Male 67.86%(19) 61.98%(300) 0.533
Female 32.14%(9) 38.02%(184)
Clinicalpresentation
Symptomatic 92.86%(26) 81.2%(393) 0.137
Asymptomatic 7.14%(2) 18.8%(91)
Location
Rightcolon 28.57%(8) 23.14%(112)
Leftcolon 46.43%(13) 48.55%(235) 0.794
Rectum 25%(7) 28.31%(137)
Metastases
Absent 67.86%(19) 79.96(387) 0.124
Present 32.19%(9) 20.04%(97)
a CalculatedbyFisher’sexacttest.
in43.95%(n=225)ofcases.Thesmaller thedifferentiation, thelowerthefrequency.However,inGroupI,themost fre-quentcategorywasthatof“moderatelydifferentiated”tumor, occurringin42.86%(n=12)ofcases.Itwasalsofoundinthis groupthatwell-differentiatedgradewaslessfrequent;poorly differentiatedgradewasmoreoftenseen,with32.14%(n=9) and18%(n=5),respectively,comparedtoGroupII,with44.63% (n=216)and9.09%(n=44),respectively.
Inthisgroup,wealsofoundalowerfrequencyofwell dif-ferentiatedgradetumorsand ahigher frequencyofpoorly differentiatedgradetumors,with32.14%(n=9)and18%(n=5), respectively,comparedtogroupII,with44.63%(n=216)and 9.09%(n=44),respectively.
InGroupI, therewere morepatients withthe presence (53.57%)versusabsence(42.86%)ofnodalmetastases;Onthe otherhand,the oppositeoccurred inGroupII, with40.29% and56.61%,respectively.Thevenousinvasionoccurredmore ofteninGroupI,50%ofcases,asopposedtoGroupII,41.32%. Inbothagegroups,thepresenceoflymphaticinvasion pre-vailed,57.14% and 52.45% respectively. As for staging, the stagesII,III and IVwerethe mostfrequentinthe sample, with28.57%(n=8)35.71%(n=10)and28.57%(n=8)patients, respectively, inGroup Iand 36.98% (n=179), 35.71% (n=10) and30.99%(n=150),respectively,inGroupII.Comparingthe twoagegroups,ahigherfrequencyofstagesIIIandIVwas notedin GroupI. For the several variables studied, signifi-cantdifferences betweengroupswere notobserved,except forhistologicaltype(Table2).
Thefollow-uptimerangedfrom2to7years.Overall sur-vivalwas63%,withamediansurvivalofapproximately63±2 months(Fig.1).
Group I showed a 5-year overall survival of61% and a mediansurvivalofapproximately58±6months.InGroupII, 5-yearoverallsurvivalwas63%andthemediansurvivalwas approximately63±2months(Fig.2).Therewasnostatistically significantdifferencebetweengroupswithrespecttosurvival (p=0.738).
Table2–Distributionofvariablesrelatedtopathological data,accordingtotheagegroup,inthesampleunder study.
GroupI %(n)
GroupII %(n)
pa
Measurement
≤45mm 50%(14) 58.06%(281) 0.963
>45mm 32.14(9) 36.57%(177)
Macroscopicaspect
Polypoid 60.71%(17) 50.41%(244)
Ulcerative 14.29%(4) 23.97%(116) 0.588
Infiltrative 3.57%(1) 8.68%(42)
Exophytic 10.71%(3) 8.06%(39)
Villous 0.0%(0) 0.41%(2)
Histologicaltype
Adenocarcinoma 78.57(22) 88.26(432)
Mucinous 14.29(4) 10.33(50) 0.001
Signetringcells 7.14(2) 0.41(2)
Differentiation
Welldifferentiated 32.14%(9) 44.63%(216)
Moderatelydifferentiated 42.86%(12) 41.53%(201) 0.337 Poorlydifferentiated 18%(5) 9.09%(44)
Undifferentiated 0.0(0) 0.83%(4)
Ganglionicmetastases
Absent 42.86%(12) 56.61%(274) 0.153
Present 53.57%(15) 40.29%(195)
Venousinvasion
Absent 46.43%(13) 53.72%(260) 0.394
Present 50.0%(14) 41.32%(200)
Lymphaticinvasion
Absent 39.29%(11) 41.32%(200) 0.699
Present 57.14%(16) 51.45%(249)
Stage
I 7.14%(2) 15.5%(75)
II 28.57%(8) 36.98%(179) 0.224
III 35.71%(10) 30.99%(150)
IV 28.57%(8) 14.05%(68)
a CalculatedbyFisher’sexacttest.
1.0 Survival
function Censored
0.8
0.6
0.4
0.2
0.0
0 20 40 60
Time (months) Overall survival
Cum
ulativ
e sur
viv
al
80 100
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40
Time (months) Overall survival
Age group
≤45
≤45-censored
>45
>45-censored
Cum
ulativ
e sur
viv
al
60 80 100
Fig.2–Cumulativeoverallsurvivalbyagegroupinthe sampleunderstudy.CalculatedbyLog-Ranktest.p=0.738.
SurvivalcurveswereestimatedbytheTNMstagingsystem; itwasfoundthatthemoreadvancedthestageatdiagnosis, thelowerthe5-yearoverallsurvival,with91%instageI,70%in stageII,56%instageIIIand33%instageIV.Five-yearsurvival onstageIwas100%inGroupIand91%inGroupII;onstageII, 88%and69%,respectively;onstageIII,70%and55%, respec-tively;andonstageIV,13%and36%,respectively.Comparing thetwoagegroups,wefoundabettersurvivalinGroupIfor thosecasesinwhichthediagnosiswasestablishedinstages I,IIandIII,andaworsesurvivalinstageIV.However,these differenceswerenotstatisticallysignificant,despitethetrend observedforstageIV(stageI:p=0.659,stageII:p=0.252;stage III:p=0.504;stageIV:p=0.061).Inthestudysample,the5-year disease-freesurvivalwasapproximately86%,withameanof 83±1month(Fig.3).InGroupItherewasa5-yeardisease-free survivalof81%,withameanof82±3months,aslightlylower resultversusGroupII,inwhichthisparameterwas86%with ameanof83±1months,butwithoutstatisticallysignificant difference(p=0.578)(Fig.4).
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40
Time (months) Disease-free survival
Cum
ulativ
e sur
viv
al
60 80 100
Survival function Censored
Fig.3–Disease-freesurvivalinthesampleunderstudy.
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40
Time (months) Disease-free survival
Age group
≤45
≤45-censored
>45
>45-censored
Cum
ulativ
e sur
viv
al
60 80 100
*P=.578
Fig.4–Disease-freesurvivalbyagegroupinthesample understudy.*CalculatedbyLog-Ranktest.
Discussion
CRC is a disease of the elderly, occurringmore frequently in the sixth and seventh decades of life, although it was observedincreasedincidenceinyoungerindividualsinrecent decades.17–19Intheliterature,theimpactof“age”inthe
prog-nosis ofpatientswithCRC isanobject ofcontroversy and hasbeen thesubject ofmuchinterest andresearch. Taken intoaccountthattherearenodataonthePortuguesereality, thisstudysoughttobetterunderstandthisissueinpatients treatedattheBragaHospital,throughananalysisofclinical andpathologicalcharacteristicsofCRCinpatientsdividedinto twoagegroups,andtheassessmentoftheimpactofthisfactor onsurvival.
Itwasfoundthat5.5%ofpatientswereaged45yearsor younger(GroupI),whichisconsistentwiththevaluesfound intheliterature.Malegenderwasthemostfrequentinthis study,bothinthetotalsampleandinagegroups,whichis inlinewiththegeneraldistributionofgenderinthosecases ofCRCdescribedbyGLOBOCAN2008,3andinsomestudies
basedonyoungpopulations,21,23withnostatisticaldifference
regardingthisparameter.Otherstudiesbasedonyoungpeople describeanequaldistributionbetweengenders.19,24,26
Inbothgroups,thepresenceofsymptomsprevailedat diag-nosis,indicatingthatthecorrectvaluationandassessmentof symptomsthroughadditionalteststoanaccurate establish-mentofthediagnosisisessentialforthediagnosisofCRC, regardlessofage.Theseresultsareinagreementwiththose foundbyotherstudies.27
The sites most commonly affected by CRC are sigmoid colonandrectum,19,21,27whichisinlinewithourresults,in
whichleftcolonpredominancewasnotedinbothgroups. Tumorswithsize≤45mmoccurredingreaternumbersand themacroscopicappearancemoreoftenseenwasthe poly-poidtypeinbothgroups;theseparametersarenosubjectof differencebetweenagegroups.
mucinousandsignetringcell/mucinousareatypes,a statisti-callysignificantdifferencewasnoted;theselattertypeswere moreoftenseeninGroupI(p=0.001),asalreadymentioned byotherauthors.19,24,26Despitethedescriptionofthese
histo-logicaltypesinassociationwithaworseprognosis,30thiswas
notthecaseinthisstudy,andtheoverallsurvivalwassimilar inbothgroups.
Severalstudieshavereportedlowerdifferentiationgrades inyounger patients, whichwould characterize CRC inthis groupasamoreaggressivetumor;19,24however,otherstudies
contradictingthesefindingswerepublished.21,27Inourstudy,
the degreefoundmorefrequently was the moderately dif-ferentiated;inGroupI,awell-differentiatedgradewasfound lessfrequently,andpoorlydifferentiatedgradewasthemost prevalent, although without statistical difference between groups.ThisfindingshowsthatCRCinyoungerpatientsdoes notshowmoreaggressiveness.
Thepresenceofvenousandlymphaticinvasionwassimilar inbothgroups.Thevenousinvasionoccurredinabouthalfthe cases,andlymphaticinvasionoccurredingreaterproportion, contributingtoamoreadvancedstageinthesample,which agreeswithresultsfromotherstudies.21,27
Severalauthorsdescribethepresenceofamoreadvanced diseaseatdiagnosisinyoungerpatients.24,26 Inthissample,
advancedstagesweremorefrequent,reflectingtheinsidious andusuallysilent(orwithfewsymptoms)natureofthis dis-ease,whichresultsindelayeddiagnoses.Despite theslight predominanceofstagesIIIandIVinGroupI,therewasno statisticaldifference;andtheresultswereequivalenttothose ofGroupII.MostCRCswereseeninstageT3,nodalmetastases werepresentinabout41%ofthesample,andmetastasesat diagnosiswereuncommon,butfornoneofthesevariablesa statisticaldifferencewasobserved,confirmingthatthestage issimilarinbothagegroups.Somestudieshaveconfirmedthe resultsofthisstudywithrespecttothestage.19,21,27,29
Someauthors reporta lower survivalrate26 inyounger
patients;however,mostoftherecentlypublishedstudieshave foundopposite results.19,21,22,24,27 In this study, there were
nosignificantdifferencesinoverallsurvivalanddisease-free survival.IngroupI,inpatientsaged45yearsorlessthe over-allsurvivalwas61%and thedisease-freesurvivalwas81% –valuessimilar tothosefoundinGroup II.These findings demonstratethatadiagnosisinyoungerpatientsisnot asso-ciatedwithaworseprognosis.
Survivaldependslargelyonthestageatdiagnosis:themore advancedthestage,theworsethesurvival,withvaluesof91%, 70%,56%and33%forstagesI,II,IIIandIV,respectively,which agreeswiththevaluesfoundintheliterature.
Conclusion
Inthis study,it wasfound thatseveral clinical and patho-logicalparameters evaluatedwere verysimilar inbothage groupsanalyzed,andanincreasedincidenceoftumorswith mucinousandsignetringcomponentswerefoundinGroupI; however,thesefindingsdidnotimpactonthelevelofsurvival. Itisessentialthathealthprofessionalsareawareofthis diagnosis,eveninpatientsatyoungerages;Itshouldalsobe emphasizedtheimportanceofhealthpromotioncampaigns
tochangehabitsandlifestyles,andtodiseasepreventionwith screening programs,inorder toachieve areductionin the incidenceandmortalityassociatedwiththisdisease.
Webelievethatthisstudyisonlyapreliminaryassessment oftheimpactoftheagefactoronthesurvivalofpatientswith CRC.Takingintoaccountthatthisisastudyofpatientsfrom onlyonehospital,itwouldbeimportanttoextendittoother centersaswellastoincreasethefollow-upperiod,tobetter knowthePortuguesereality.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.BoyleP,LevinB,editors.Worldcancerreport2008.Lyon,
France:WorldHealthOrganization,InternationalAgencyfor
ResearchonCancer;2008.
2.JemalA,BrayF,CenterMM,FerlayJ,WardE,FormanD.Global
cancerstatistics.CACancerJClin.2011;61:69–90.
3.FerlayJ,ShinHR,BrayF,FormanD,MathersC,ParkinDM. GLOBOCAN2008v2.0,cancerincidenceandmortality worldwide:IARCCancerBaseNo.10[Internet].Lyon,France: InternationalAgencyforResearchonCancer;2010.Available from:http://globocan.iarc.fr/[accessed12.07.12].
4.PimentelJ.;2009.Cancrocolo-rectal[Internet].PROCTOS– CentrodeColoproctologiadeCoimbra.Availablefrom:
http://www.proctos.pt/[accessed06.11.12].
5.Teliarova-FoucherE,O’CallaghanM,FerlayJ,MasuyerE, FormanD,ComberH,etal.Europeancancerobservatory: cancerincidence,mortality,prevalenceandsurvivalin Europe[Internet].EuropeanNetworkofCancerRegistries, InternationalAgencyforResearchonCancer;2012.Available from:http://eco.iarc.fr[accessed20.08.12].
6.MendesV.PreveniroCancrodoCóloneRecto.JPortGastr.
2008;15:153–5.
7.TeixeiraAV.PóliposeCancrodoCóloneRecto.ArquiMed.
2009;23:209–16.
8.JohnsHopkinsColonCancerCenter;2012.Colorectalcancer overview[Internet].Availablefrom:http://www.
hopkinscoloncancercenter.org[accessed20.11.12].
9.TownsendCM,BeauchampRD,EversBM,MattoxKL.Sabiston
textbookofsurgery.18thed.Elsevier;2009.p.1393.
10.MinistériodaSaúdeAltoComissariadodaSaúde
Coordenac¸ãoNacionalparaasDoenc¸asOncológicas.Plano NacionaldePrevenc¸ãoeControlodasDoenc¸asOncológicas 2007/2010(PNPCDO):Orientac¸õesProgramáticas.
11.PlanoOncológicoNacional2001–2005.DiáriodaRepública,Ia
Série-B(no.199).2001:5241–7.
12.AmericanCancerSociety;2012.Colorectalcancer[Internet]. Availablefrom:http://www.cancer.org/[accessed20.09.12].
13.HaggarFA,BousheyRP.Colorectalcancerepidemiology:
incidence,mortality,survival,andriskfactors.ClinColon
RectSurg.2009;22:191–7.
14.NationalCancerInstitute.Whatyouneedtoknowabout
cancerofthecolonandrectum.Bethesda,MD:National
InstitutesofHealth;2006.
15.HowladerN,NooneA,KrapchoM,NeymanN,AminouR, AltekruseS,etal.SEERcancerstatisticsreview1975–2009 [Internet].Bethesda,MD:NationalCancerInstitute.Available from:http://seer.cancer.gov/csr/19752009pops09/results
SEERdatasubmission,postedtotheSEERwebsite2012 [accessed20.09.12].
16.ParramoreJ,WeiJ,YehK.Colorectalcancerinpatientsunder
forty:presentationandoutcome.AmSurg.1998;64:563–7.
17.SiegelRL,JemalA,WardEM.Increaseinincidenceof
colorectalcanceramongyoungmenandwomeninthe
UnitedStates.CancerEpidemiolBiomarkPrev.
2009;18:1695–8.
18.MeyerJE,NarangT,Schnoll-SussmanFH,PochapinMB,
ChristosPJ,SherrDL.Increasingincidenceofrectalcancerin
patientsagedyoungerthan40years:ananalysisofthe
surveillance,epidemiology,andendresultsdatabase.Cancer.
2010;116:4354–9.
19.GanapathiS,KumarD,KatsoulasN,MelvilleD,HodgsonS,
FinlaysonC,etal.Colorectalcancerintheyoung:trends,
characteristicsandoutcome.IntJColorectalDis.
2011;26:927–34.
20.SvendsenLB,SorensenC,KjersgaardP,MeisnerS,Kjærgaard
J.Theinfluenceofageuponthesurvivalaftercurative
operationforcolorectalcancer.IntJColorectalDis.
1989;4:123–7.
21.SheK,WangH,ChenJ,MarH,ChenC,ChiangF,etal.
Colorectalcancerinyoungerthan30yearsoldgroupisnot
associatedwithpoorprognosis.JSocColonRectalSurgeon
(Taiwan).2011;22:93–8.
22.WangL,HollenbeakCS,StewartDB.Nodeyieldandnode
involvementinyoungcoloncancerpatients:istherea
differenceincancersurvivalbasedonage?JGastrointest
Surg.2010;14:1355–61.
23.DrumondCA,FerroRAF,NogueiraAMF,LuzMMP,Conceic¸ão
SA,SilvaRG,etal.Câncercolorretalempacientescomidade
inferiora30anos.RevBrasColoproctol.2003;23:147–54.
24.O’ConnellJB,MaggardMA,LiuJH,EtzioniDA,LivingstonEH,
KoCY.Doyoungcoloncancerpatientshaveworseoutcomes?
WorldJSurg.2004;28:558–62.
25.VanLangenbergA.Carcinomaofthelargebowelinthe
young.BrMedJ.1972;3:374–6.
26.DomergueJ,IsmailM,AstreC,Saint-AubertB,JoyeuxH,
SolassolC,etal.Colorectalcarcinomainpatientsyounger
than40yearsofage.Cancer.1988;61:835–40.
27.QuahHM,JosephR,SchragD,ShiaJ,GuillemJG,PatyPB,etal.
Youngageinfluencestreatmentbutnotoutcomeofcolon
cancer.AnnSurgOncol.2007;14:2759–65.
28.GreeneFL,ComptonCC,FritzAG,ShahJ,WinchesterDP.AJCC
cancerstagingatlas.NewYork,NY:Springer;2006.p.352.
29.NurdjanahS,TaroenoS,BayupurnamaP,MadusenoS,
RatnasariN.Colorectalcancerinyoungpatient:a
distinguisheddiseaseentity?IndonesianJGastroenterol
HepatolDigestEndosc.2005;6:37–41.
30.NumataM,ShiozawaM,WatanabeT,TamagawaH,
YamamotoN,MorinagaS,etal.Theclinicopathological
featuresofcolorectalmucinousadenocarcinomaanda
therapeuticstrategyforthedisease.WorldJSurgOncol.