InternationalJournalofMedicalInformatics92(2016)54–61
ContentslistsavailableatScienceDirect
International
Journal
of
Medical
Informatics
jo u r n al h om e p a g e :w w w . i j m i j o u r n a l . c o m
Review
article
Information
and
communication
technologies
for
adherence
to
antiretroviral
treatment
in
adults
with
HIV/AIDS
Ivana
Cristina
Vieira
de
Lima
a,∗,
Marli
Teresinha
Gimeniz
Galvão
b,
Herta
de
Oliveira
Alexandre
a,
Francisca
Elisângela
Teixeira
Lima
b,
Thelma
Leite
de
Araújo
baFederalUniversityofCeará(UFC),Fortaleza,CE,Brazil
bFederalUniversityofCeará(UFC),NursingDepartment,Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received9September2015
Receivedinrevisedform22April2016
Accepted26April2016
Keywords: Technology Communication HIV
Medicationadherence
Efficacy
a
b
s
t
r
a
c
t
Introduction:Informationandcommunicationtechnologiessupportinterventionsdirectedatthe pre-ventionofHIVtransmissionandpatientmonitoringbypromotingimprovedaccessibilityandqualityof care.
Objective:Toevaluatetheefficacyofinformationandcommunicationtechnologiesintheadherenceto antiretroviraltreatmentinadultswithHIV/AIDS.
Methodology:SystematicreviewconductedfromMarchtoMayof2015inthreedatabases—the Cumula-tiveIndextoNursingandAlliedHealthLiterature(CINAHL);theLatin-AmericanandCaribbeanLiterature inHealthSciences(LILACS/BIREME)andSCOPUS;andtheCochranelibraryandtheMedicalLiterature AnalysisandRetrievalSystemOnlineportal(MEDLINE/PubMed).Thesampleconsistedofnine random-izedclinicaltrialsbasedontheuseofinformationandcommunicationtechnologiesforadherenceto antiretroviraltreatmentinadultswithHIV/AIDS.
Results:Threestudiesanalysedtheuseofashortmessageservice–SMS–twophonecalls,twoalarm devices,oneweb-enabledHand-helddeviceandonewebelectronicintervention.Improvementsinthe levelsofadherenceinthegroupsubjectedtotheinterventionwereidentifiedinsevenstudies.The phonewasthetypeofinformationandcommunicationtechnologywithprovenefficacywithrespect toadherence.Itwasusedtomakecalls,aswellastosendalertmessagesandremindersabouttaking medications.Pagerswerenotconsideredtobeeffectiveregardingadherencetoantiretroviraltherapy. Conclusion:Theintegrateduseofinformationandcommunicationtechnologieswithstandardcare pro-motesincreasedaccesstocare,strengtheningtherelationshipbetweenpatientsandhealthservices,with thepossibilityofmitigatingthedifficultiesexperiencedbypeoplewithHIVinachievingoptimallevels ofadherencetodrugtherapy.
©2016ElsevierIrelandLtd.Allrightsreserved.
1. Introduction
Informationand communication technologies (ICTs) include any communication devices, including radio, television, cell phones, computers, network equipment (hardware), programs (software)andsatellitesystems,aswellasthevariousservicesand
∗Correspondenceto:TipógrafoSalesSt.,992,AmadeuFurtado,60455-500
Fort-aleza,CE,Brazil.
E-mailaddresses:[email protected](I.C.V.d.Lima), [email protected](M.T.G.Galvão),[email protected]
(H.d.O.Alexandre),[email protected](F.E.T.Lima),
[email protected](T.L.d.Araújo).
applicationsforwhichtheyareused,suchasvideoconferencing, onlinechattinganddistancelearning[1].
Inhealthcare,theuseofICTgoesbeyondthetransmissionof information asitsupports self-care,behaviouralchanges, infor-mationexchangesamongpeersandemotionalsupport,aswellas providingbenefitsintrackingpeoplewithchronicdiseases[2,3].In thecontextofHIV/AIDS,ICTshavemediatedinterventionsdirected atpreventingthetransmissionofthevirusormonitoringpatients bypromotingimprovedaccessibilityandqualityofcare[4].
TheinfluenceoftheadvancementsinthetreatmentofHIV/AIDS in the transition from acute to chronic disease is highlighted. Antiretroviraltherapy(ART)hasimprovedhealth,reduced oppor-tunisticinfections,andincreasedsurvivalandimprovedqualityof lifeinapproximately9.7millionpeopleworldwide[5,6].
http://dx.doi.org/10.1016/j.ijmedinf.2016.04.013
Despitethesebenefits,thelong-termuseofARTimplies chal-lenges.The main difficultyfaced by persons livingwith HIV is adherence(representedbyingestingatleast95%oftablets)dueto thelargenumbersofpillsandsideeffectsandthehighfrequency ofdosesand/ortabletstakenperday[7,8].
Failureoftreatmentadherenceelicitsindividual(decreasedCD4 Tcells,viralresistance, riskbehaviour,progressiontoAIDSand death)and collectivelosses(increased transmissionof HIV and othersexuallytransmittedinfections,highertreatmentcostsand hospitalizations)[6,9].Forthesereasons,caretoolsaimedat contin-uousmonitoringandcounselling,aswellasstrategiesforpatient orientation/training,withafocusonachievingoptimallevelsof adherencetoART,areneeded[5].
Atheoreticalreviewpresentedconsiderationsregardingtheuse ofinformationtechnologyinthecontextofHIV,highlightingthe possibilityofa positive impactonthelevelsofsatisfaction and patientsafety,inadditiontoimprovementsinadherencetoART andcarequalityindicators.Moreover,theuseoftheInternet, digi-talmedia,informationsystems/monitoringandtelephoneprovides information for thediagnosis and treatmentof HIV, as wellas opportunitiesfortheelectronicregistrationofdataandincreased accesstoinformationforboththepatientandthemultidisciplinary team[4].
Asystematicreviewanalysed23publicationsand32ongoing projectsontheuseofthetelephone,Internetandsocialmediain healthcarein thecontextofHIV treatment.Therewas empha-sisontheuseoftechnologyinthefollowingsituations:primary preventionofHIVtransmission,promotionofHIVtesting, estab-lishmentofbondsandconservationcare,supportforstartingART, andpromotingadherencetoART,aswellasachievingincreased viralsuppressionandpreventingsecondaryinfections.Although increasingattentionhasbeendevotedtotheuseoftechnology,it isnecessarythatotherstudiesalsoanalysetheefficacyofthesecare tools[10].Thetermefficacyentailsthataninterventionproduces theexpectedresultunderidealcircumstances[11].
Furthermore,reviewshaveconsideredthepossibilitiesofthe useofICTsinthecontextofHIV/AIDS,butnosystematicreviews abouttheefficacyofthesetechnologiesintreatmentadherencein adultswithHIVhavebeenfound.Therefore,thefollowingresearch question was asked: “What is the efficacy of information and communicationtechnologiesinsupportingHIV/AIDS antiretrovi-raltreatmentadherenceinadults?”Inthisreview,weconsidered thetypesofICTthataremainlyusedtomonitorpeoplewithHIV: computers,phones,softwareandpagers.
Analysis of the efficacy of ICT as a health care instrument can identify alternatives to supportive care for people living withHIV/AIDS, aswell asthebenefits and limitations ofthese alternatives. Analysis also highlights the possibility of sharing withpractitioners and researchersthetheoretical and practical assumptionsforthereplicationofinformationandcommunication technologieswithprovenefficacywithrespecttotheadherenceto antiretroviraltreatmentinadultswithHIV/AIDS.
This study aimed to evaluate the efficacy of information and communication technologies withrespect to adherenceto antiretroviraltreatmentinadultswithHIV/AIDS.
2. Methods
Asystematicreview wasconductedaccordingtothe recom-mendationsoftheCochraneHandbookforSystematicReviewsof Interventions[12].Asystematicreviewisatypeofsecondarystudy thatenablesthedevelopmentofclinicalguidelinesfor decision-makingandfacilitatestheplanningofclinicalresearchinhealth care[13].
TheresearchquestionwasdesignedbasedonthePICO strat-egy,whichstandsforPatient(adultslivingwithHIV),Intervention (usingICT)Comparison(standardcare)andOutcomes(treatment) [14].
Weperformedintentionalsamplingfromclinicaltrialsbasedon theuseofICTforadherencetoantiretroviraltreatmentbyadults withHIV/AIDS,regardlessofthepublicationyearand language. Weexcludedrepeatpublications;thosethatdidnotanswerthe researchquestion;casereports,experiencereportsandtheoretical, qualitativeorcross-sectionalstudies;reviewpapers andclinical trialprotocols,aswellasclinicaltrialsthathaveaddressedtheuse ofinformationandcommunicationtechnologiesinHIVprevention andrapidtesting.
Theelectronicsearchwascarriedoutbytworeviewers simul-taneouslyinthreedatabases−theCumulativeIndextoNursing and Allied Health Literature (CINAHL); theLatin-American and CaribbeanLiteratureinHealthSciences(LILACS/BIREME)and SCO-PUS;andtheCochranelibraryandtheMedicalLiteratureAnalysis andRetrievalSystemOnlineportal(MEDLINE/PubMed),accessed throughthePortalCAPES(HigherEducationPersonnel Improve-mentCoordination).
ThefollowingcontrolleddescriptorsavailableinMeSH(Medical SubjectHeadings):Technology;HIV;Internet;CellPhones; Soft-ware;Telemedicine;eHealth;RemoteSensingTechnology;Clinical Trialwereused.Thecrossesperformedwere[HIVand Technol-ogy],[InternetandHIVandTechnology],[HIVandTechnologyand CellPhone],[HIVandTechnologyandSoftware],[HIVandNursing andTechnology],[HIVandTelemedicine],[HIVandeHealth],and [RemoteSensingTechnologyandHIV].Thecontrolleddescriptor ClinicalTrialwasincludedinallcrosses.
AfterthesearchwascompletedonMay22,2015,thearticles wereanalysedbytwoauthors,whoreadthetitlesandabstracts. Eli-giblestudiesweretranslatedintothenativelanguageoftheauthors (Portuguese)andreadinfull.
Tworeviewersassessedthequalityoftheclinicaltrialsandthe dataindependently.Incaseofdoubt,thereweremeetingsbetween thereviewerstoreachconsensus.Toanalysethescopeofthe stud-ies,thereviewersusedareferencelist.
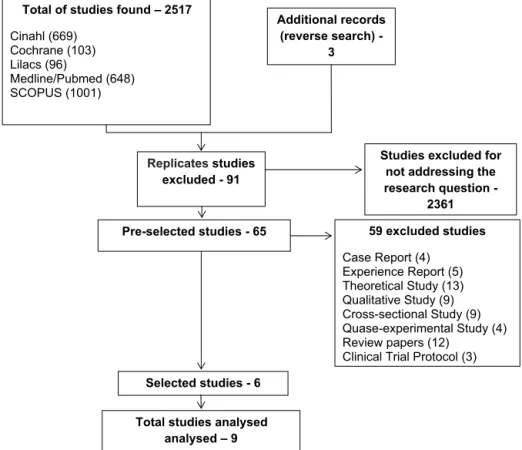
Fromthecrossesthatwerecarriedout,a totalof2517 stud-ieswerefoundintheinvestigateddatabases.Fromthesestudies, 91replicateswereremoved.Analysesofthetitlesandabstracts yielded65pre-selectedstudies;however,59studieswereexcluded becausetheywerenotclinicaltrials,asdescribedbelow:fourcase reports,fiveexperiencereports,13theoreticalstudies,nine qualita-tivestudies,ninecross-sectionalstudies,fourquasi-experimental studies,12reviewpapersandthreeclinicaltrialprotocols.Among thesixselectedarticles,threewerefoundinMEDLINE/PubMed, threewerefoundinSCOPUS,andthreewerefoundusingreverse search.Ultimately,thesampleconsistedofninestudies(Fig.1).
Analysisofthequalityofthestudieswasbasedonaqualityscale describedbyJadadetal.[15],inwhichthescorerangesfrom0to5 andiscalculatedfromthefollowingparameters:(1a)Thestudywas random(usingwordssuchas‘random’,“randomization”)?;(1b) Themethodwasappropriate?;(2a)Thestudywasdoubleblinded? (2b)Themethodwasappropriate?;and(3)Thereweredescriptions oflossesandexclusions?
Thestudieswerealsoanalysedforallocationconfidentialityand wereclassifiedasCategoryA—theallocationconfidentiality pro-cesswasadequate;CategoryB—theallocationconfidentialitywas notdescribed,butitwasstatedinthetextthatthestudywas ran-dom;CategoryC—theallocationconfidentiality wasinadequate; andCategoryD—thestudywasnotrandom[12].
56 I.C.V.d.Limaetal./InternationalJournalofMedicalInformatics92(2016)54–61
Studies excluded for not addressing the research question -
2361
Selected studies - 6 Pre-selected studies - 65
Replicates studies excluded - 91
Additional records (reverse search) -
3 Total of studies found – 2517
Cinahl (669) Cochrane (103) Lilacs (96)
Medline/Pubmed (648) SCOPUS (1001)
59 excluded studies
Case Report (4) Experience Report (5) Theoretical Study (13) Qualitative Study (9) Cross-sectional Study (9) Quase-experimental Study (4) Review papers (12)
Clinical Trial Protocol (3)
Total studies analysed analysed – 9
Fig.1.Flowchartoftheidentification,selectionandinclusionofstudies.
Fortheethicalquestions,theintegrityofthearticlesandthe copyrightwererespected,withnomodificationofthecontentin favourofthisresearch.
3. Results
Table1 characterizesthestudiesbasedontheauthor, coun-try,proposedtechnology,sample,clinicaltrial,improvementsin adherence,Jadadscalescoreandallocationconfidentiality.
Theyearsofthestudies’publicationwerefrom2008to2015.All studieswererandomizedandincludedatotalof1866adultswith HIVusingARTwhowererecruitedfromoutpatientclinics[16–21] andhospitals[22–24].Regardinglocation,mostofthestudieswere developedintheUnitedStatesofAmerica(USA)[16,19,20–23]and inAfricancountriessuchasKenya[15,16,18]andCameroon[22] (Table1).
Theproposedtechnologieswereshortmessageservices—SMSs [18,22,23,24], phone calls [16,19], pagers [17,23], web-enabled hand-helddevicepluspersonalhealthrecord[20]andweb elec-tronicintervention[21].Thesubjects’timesoffollow-upranged from4(1month)to72weeks(18months).Improvementsin adher-encelevelsinthegroupsubjectedtotheinterventionbasedon theuseoftechnologywereidentifiedinsevenstudies[16,18–23] (Table1).
Regardingthetypeofcommunication,intwostudies,telephone callsweresynchronouslyused[16,19];infivestudies,thefeedback wasasynchronousfromthesubjectafterreceivinganSMS[22–24], web-enabledHand-helddevice[20]andwebelectronic interven-tion[21].Intwostudies,thesubjectsreceivedasynchronouspager messages,webelectronicinterventionandSMSwithout provid-ingfeedback[17,18].Thequalityoftheevaluationofthestudies showedgoodmethodologicalquality,withapredominantscoreof 3[17,18,23,24].Regardingallocationconfidentiality,therewasan emphasisplacedonCategoryA—theallocationconfidentialitywas
adequate,exceptfortwostudies,whoseallocationconfidentiality hasbeenpreviouslydescribed[16,18](Table1).
Table2providesinformationontheuseoftechnologyandthe measurementofadherence.
Regardingtheuseofinformationandcommunication technolo-gies,therewasapredominanceofthecombinationoftheabove technologieswithstandard care,whichincludedpatient educa-tion[16,20],counsellingsessionsforARTuse[17,21]andfollow-up visits[18–20,22,23].Inonestudy,technologywasalsousedin iso-lation[30].Inanotherstudy,technologywasusedbothinisolation andincombinationwithothertherapies[17](Table2).
Regardingthefrequencyofofferinginformationtechnology,the dailyratewaspredominant[17,19].Onestudyusedamonthly fre-quency[16],onestudyusedaweeklyfrequency[24],andanother study compared the daily and weekly use of technology [18]. Regarding the professionals who implemented the technology, differenthealthprofessionalswerenoted,includingnurses, phar-macistsanddoctors[16–23]orqualifiedprofessionalsfromother areas[18,19,24](Table2).
Regardingthemethods of ARTadherencemeasurement and self-reportedadherence [16,22–24],the useof other measures, suchasadherenceself-efficacy[20,21],pillcounts[17,21],drug monitoringsystems [17,19], visual analogue scales[19,24] and pharmacy records on replenishment [24] was also noted. The combination ofdifferentforms of adherencemeasurement was observedintwoclinicaltrials[23,24].Additionally,multiple adher-encemeasuresduringthestudyperiodwerehighlighted,fromthe beginningofthefollow-upperiodtothe72ndweek(Table2).
4. Discussion
measure-I.C.V.d.
Lima
et
al.
/
International
Journal
of
Medical
Informatics
92
(2016)
54–61
57
Studycharacterizations.
Authors,Year,Country Technologiesproposed Sample Typeofclinicaltrial Timeoffollow-up Results Jadad scale/Allocation confidentiality
Reynoldsetal.(2008), USA
Phonecall 109 Classic 64weeks/16months AdherencerateintheIG99.7%
(p=0.023)andintheCG97.3% (p=0.019)
2/B IGa:54
CGb:55
Lesteretal.(2010),
Kenya
SMSc 538 Classic 48weeks/12months Self-reportedadherenceby168ofthe273
IG,comparedwith132ofthe265inthe
CG(RRdtononadherence=0.81;95%;
CIe=0.69-0.94;p=0.006)
2/A aIG:273
bCG:265
Chungetal.(2011),
Kenya
Alarmdevice×Counselling 400 Factorial 72weeks/18months Nosignificantimpactofthealarm
deviceusageinadherence
(HRf=0.93;95%;CI=0.65–1.32;
p=0.7)
3/A aIG:300
bCG:100
Pop-Elechesetal.
(2011),Kenya
SMSdaily×SMSmonthly 431 Classic 48weeks/12months 90%ofIGadherencecompared
with40%ofCGadherence(p=0.03)
3/B aIG:302
bCG:139
Hardyetal.(2011),USA SMS×Alarmdevice 22 Classic 6weeks/1.5months Self-reportedadherenceinIG
92.6%(CI=77.5–107.7)andinCG
72.4%(CI=56.5–88.3)
3/A aIG:12
bCG:11
Mbuagbawetal.
(2012),Cameroon
SMS 200 Classic 24weeks/6months Nosignificanteffectofthe
interventiononadherence
measuredbythevisualanalogue
scale(RR=1.06;95%;CI=0.89,
1.29;p=0.542)
3/A aIG:101
bCG:99
Belzeretal.(2014),USA PhoneCall 37 Behavioural 48weeks/12months Self-reportedadherence
significantlyhigherinIGcompared
toCG(p=0.007)
2/A aIG:19
bCG:18
Fiscellaetal.(2015),
USA
Web-enabledHand-helddevice
plusPersonalHealthRecord
32 Classic 52weeks/13months Largerimprovementsin
self-efficacyandself-reported
adherenceinIG
4/A
aIG:Notmentioned
bCG:Notmentioned
Clabornetal.(2014),
USA
WebElectronicintervention 97 Classic 4weeks/onemonth Self-efficacyandself-reported
adherencesignificantlyhigherinIG
(Mg=8.79;SDh=1.34/M:80.53;
SD=26.29)comparedtoCG
(M=7.96;SD=1.67/M=81.40;
SD=25.21).
4/A aIG:47
bCG:50
aIG:Interventiongroup.
b CG:Controlgroup.
c SMS:ShortMessageService.
d RR:Riskratio.
eCI:Confidenceinterval.
f HR:Hazardratio.
gM:Mean.
58 I.C.V.d.Limaetal./InternationalJournalofMedicalInformatics92(2016)54–61
Table2
Informationontheuseoftechnologyandthemeasurementofadherence.
Author/year Useoftechnology Technologyproviding frequency
Professionalwhomeasuredthe technology
Adherence
measurementmethod
Measurement frequency
Reynoldsetal.(2008) Combinedwithpatient education
Monthly Nurse Self-reported
adherence
Weeks4,16,48and64
Lesteretal.(2010) Combinedwith appointments
Notmentioned Nurseordoctor Self-reported adherence
Weeks24and48
Chungetal.(2011) Isolatedandcombined withcounselling sessionsforHAART
Daily Pharmacist Tabletscount Weeks4,8,12,16,20, 24,28,32,36,40,44, 48,52,56,60,64,68,72 Pop-Elechesetal.(2011) Combinedwith
appointments
Dailyandweekly Commercialservicesprovider Monitoringdrug eventssystem
Weeks4,8,12,16,20, 24,28,32,36,40,44,48 Hardyetal.(2011) Combinedwith
appointments
Daily Nurse,doctor, pharmacistand counsellor
—Self-reported adherence;
Weeks0,3and6.
—Tabletscount; —Monitoringdrug eventssystem Mbuagbawetal.(2012) Combinedwith
appointments
Weekly Secretary —Visualanalogue
scale;
Weeks12and24
—Self-reported adherence;
—Pharmacyrecordson replenishment Belzeretal.(2014) Combinedwith
appointments
Daily Adherencefacilitator Visualanaloguescale Weeks6,12,24,36and 48
Fiscellaetal.(2015) Combinedwithgroup sessionsandvisits
Notmentioned Doctor Self-efficacyand
Self-reported adherence
Weeks8–10,14–24
Clabornetal.(2014) Combinedwith counselling
Notmentioned Pharmacistand Pharmacy’sstudent
—Self-efficacyand Self-reported adherence
Weeks0and4
—Tabletscount
mentmeasuresof theoutcome variable,multipleinterventions withvariousformsofapproachandinsufficientstatisticaldata.
Theuseofinformationandcommunicationtechnologiesto pro-videhealthcarebeganinthe1990s,withanexpansioninrecent yearsviathemobileweb,smartphonesandsocialmedia.These technologieshaveproveneffectiveasmediationtoolsofinteraction andhealtheducation,withsatisfactorycost-benefits.Inaddition, thesetechnologiesconstituteinnovativemeansofhealth promo-tionanddiseaseprevention[11].
InthecontextoftheHIVepidemic,informationtechnologies havebeensuggestedastoolsforexpandingaccesstohealthcare byreducing thegeographicbarriersandcostsinvolvedin infec-tionpreventionand treatment.If theyare usedin combination withstandard care,itwillbepossibletostrengthenhealth ser-vicesandimprovementsincarequality[4,25].TheUnitedNations ProgrammeonHIV(UNAIDS)andtheWorldHealthOrganization supportinitiativesfocusedonmobilecommunicationasastrategic action[6].
AfricancountriessufferfromtheeffectsoftheAIDSepidemic becausetheyhavelimitedhumanandmaterialresourcestocare forpeoplelivingwithHIV,withrepercussionsrelatedtodecreased adherencetoARTbeingobservedover time[22,26].Clinical tri-alspublishedinthisregionshowconsistencywiththescientific literature[27,28]anddemonstratethebenefitsofusing informa-tionandcommunicationtechnologies,especiallymobilephonesto sendSMSs[18,22],toimproveadherencetoARTinplaceswith lim-itedresources.Ithasbeensuggestedthattheapplicationofmobile telephonesasamethodofcaringforpeoplelivingwiththevirusin otherunderdevelopedcountriesisefficacious.
Mobiletelephoneshavebeenidentifiedas acaretool inthe contextofHIVduetheirfeasibility,acceptance,potentialfor large-scaleuse,potentialforinteractivefeedbackandefficacy[29,30]. Thefindingsofthisreviewsupportthisevidence.Onlyone clin-icaltrialusingmobilephonesdidnotnoteimprovedadherence toART[24].However,thisstudyutilizedmonitoringforonlysix months,whereasinotherreviews,monitoringwaspredominantly
performedfora periodequal toorgreaterthantwelvemonths [16,18,19].Inaddition,inthisstudy,themessageshada motiva-tionalnatureandwerenotdirectlyassociatedwithART.
Asystematic reviewontheuseofmobiletelephonesin HIV preventionandtreatmentanalysed64publicationsinitsmajority descriptive.Inaddition,similarresultstothisstudywere identi-fiedinrelationtotheprevalenceofsendingtextmessagesaspart oftheprovisionofcarecomparedwithothertechnologies. Approxi-mately60%ofthestudiesanalysedinthereviewprovidedwarnings andreminders,usingmobilemessagestoencouragedisease treat-ment[25].
SMScanbeusedasamethodofasynchronouscommunication withandwithoutfeedbackfromsubjectsaftertheyreceive mes-sages.Thefeedbackfromthesubjectsaftertheyreceivemessages, withinaspecifiedperiod,provestobemoreeffectiveand strength-enstherelationshipsamongstakeholdersandenablesprofessional supportforproblem-solving[22].However,thepotentialforthe lossofprivacy,confidentialityandsecrecyshouldbeconsidered withrespecttotheuseofthistechnology[24].
Shortmessagessentbycellphoneareassociatedwithhigh sat-isfactionindicatorsinadultswithHIV.Inaddition,theyassistin thereductionoferrorsandforgetfulnessandstrengthenthelink betweenthepatientandtheprofessionalfrominteractive commu-nicationamongpeers[31].
Inturn,mobiletelephonyisasubtypeoftelephonecallwhose useallows the provisionof information, patienteducation and development of effective skills that can influence behavioural changes[32].InmonitoringchronicconditionssuchasHIV infec-tion,itenablesreal-timeproblem-solving,withapositiveimpact ontreatmentself-efficacy[16].
evaluationoftheuseoftechnologyandhealthservicesinrealtime [16,19].
Thetwoclinicaltrialsthatusedphonecallshadpositiveresults regardingadherenceinadultsaffectedbyHIV[16,19],butinone ofthetrials,thesamplewasreduced [19].Theauthorsofthese studiesissuedawarningregardingthegeneralizabilityofsamples withdifferentcharacteristicsandsuggestedconducting compara-tivestudiesontheefficacyofphonecallsandtextmessaging.
Anothertype ofinformation and communication technology usedtosupportthetreatmentof peoplewithHIV iselectronic devicereminders(pagers),alow-costtechnologywitheasy han-dling and distribution [17]. Despite these positive points, the literatureshowssimilarresultstothisreviewwithrespecttothe limitedefficacyofthisdeviceintheadherencetoART[27,33,34]. Ontheotherhand,theuseofaweb-enabledhand-helddevice(a mobiletelephonyfeaturewithusability,interactionand versatil-itysuperiortopager)combinedwithinteractivePersonalHealth Recordshowntobeeffectivein improvingtheself-efficacyand self-reportedadherence[20].
This result may be correlated with the lack of interper-sonal interactions with the user, which differs from mobile telephony,wherethereiscontinuousfeedbackbetween patient-to-professionalorpatient-to-patient[31].Thealarmdevicedoesnot capturebarrierstogoodadhesion,suchasdepressionandstigma, whichcanbebetterdetectedinperson[17].Anotherfactorthat contributestotheineffectivenessof thistechnologyisthe abil-itytogeneratecuriositybythosewholivewithpeoplewithHIV, indirectlyviolatingconfidentiality[23].
These review results agree with studies that demonstrate the success of eHealth interventions in Promoting changes in behaviour,self-efficacy, knowledge, and clinicaloutcomes [35]. Therewasemphasisontheuseoftoolssuchasvideos,quizand web-hand-helddevice[20,21]tomotivateadherencetoARTand adherenceself-efficacy.Inaddition,mostpublishedstudiesaddress theuseofeHealthinprimarypreventionofHIV[10],so,itwasnot possibletoestablishmorespecificcomparison.
Therelationshipbetweeninterventionsandbehaviouralchange modelsisan importantfactor.Thereis consensusinthe litera-tureabouttheimportanceofsupportandprofessionalmonitoring guidedbyemotionalprocesses,suchaschangesinbehaviourof peoplewithHIV[16,17,19].Whenmotivated,subjectscandevelop skillstoimproveadherence[17].
However,theuseofonlythemotivationalapproachasan inter-ventionframeworkinICTisnotsufficient[24].Otherbehavioural cognitivestrategies,suchasmotivationalinterviewing,mustbe usedto furtherimprovetheefficacyof technologiesfor adher-encetoART.Theaimistopromoteself-efficacy,socialsupportand copingstrategiesfocusedproblem-solvinganddecreasingstress [19].
Despitetheavailableinformationanddiversityof communica-tiontechnologies,themajorityoftheabovementionedclinicaltrials wererestrictedtomobilephonesandpagers.Withthepopularity ofsocialmediaandsmartphoneapplications,itisexpectedthat futureresearchwillbedevelopedtodemonstratetheuseofthese toolsandtheirefficacyinstimulatingadherencetoantiretroviral treatment.Theexistenceofstudiesintheliteratureontheuseof thesetoolstomediateprimaryandsecondarypreventioninthe contextofHIVhasbeenemphasized[10].
Regardingthequality of theanalysed clinicaltrials, noneof thestudiesreachedthemaximumscoreintheJadadScale[15]. Thecauseofthisfindingwasthelackofblinding.Althoughitwas notpossibletoperformadouble-blinded(investigatorsand peo-plewhoreceivetheintervention)study,itissuggestedthatfuture clinicaltrialsusesimpleblindingtominimizebias.Additionally, therandomizationtechniquedecreasesselectionbias[36].
Anotherimportantfactortonoteistheaccuracyofthe mea-surements of adherencetoARTasan outcome variablefor the useof informationand communication technologiestosupport treatment.Therearetwotypesofadherencemeasurement meth-ods:directandindirect.Thedirecttypemeasuresthepresenceof antiretroviraldrugsin theblood,urineorotherbodilyfluidsby theanalysisofmetabolitesandmarkers.Theindirecttypeassesses otherantiretroviraluseindicatorsbyself-reporting,clinical evalu-ations,reviewsofmedicalrecords,outpatientcareorbehavioural observation(pill counts,pharmacy refillrecords,and electronic drugmonitoring)[37].Inthisreview,wehighlightedtheindirect methodsofadherencemeasurement.
Interviews and questionnaires based on self-reporting have advantages,suchaslowcost,easeandapplicationspeed,aswell asthepotentialtocapturespecificinformationaboutdosagesand adherencetodietaryrequirements[38].Despiteitshigh reliabil-ityandspecificity,self-reportingissusceptibletorecallbiasand canprovideinaccurateinformation;therefore,itmustbecombined withothermethods[37].
The visual analogue scale (VAS) is an indirect method of adherencemeasurementthatconsistsofcharacteristicorattitude measurementinstrumentsthatarenoteasilymeasuredandare subjective.Thepatientmarksahorizontallinelength,which rep-resentstheirperceptionoftheircurrentstate[39].
Anotherindirectmethodofmeasuringadherenceisthe quan-tificationofremainingpillsthatmaybeheldbythepharmacist formedicationrefill.Itisameasuresubjecttobiasbecauseofthe possibilityofpillomissionbythepatient[17].Amoreaccurate mea-surementisbasedonadrugeventmonitoringsystemheldbythe pharmacistthatusesmicrosensorsthatarelocatedinthemedicine bottle,allowingtheanalysisofthenumberofopenings[17].
5. Conclusion
Theuseofinformationandcommunicationtechnologiesin sup-portingthecareofadultswithHIVisconsideredtobeeffectivein improvingadherencetoART.Theadvantagesofthesetechnologies includetheirpotentialforinteraction,collaboration,lowcostand useinareaswithlimitedhumanandmaterialresourcesforthe pro-visionofcare.However,accesstoelectronicdevicesandtheneed forusertrainingareimportantconsiderations.
The most effective type of information and communication technologywasthephone,whichwasusedtodelivercallsandsend alertmessages,aswellasremindersabouttakingmedications.The electronicdevicealarm(pager)wasnotconsideredtobeeffective forARTadherence.
Apreference fortechnologiesenabling synchronous commu-nication(telephonecalls)asynchronouslyfeedbackfromsubjects (SMS)fortheformationofclosertiesandthepromotionof profes-sionalsupportinrealtimewasnoted.Thisreviewwasunableto comparetheuseofICTsincombinationwithstandardcarewith classroomtechnologies.
TheeHealthinterventionssuchasvideos,quizand web-hand-held device were effective to motivate adherence to ART and adherence self-efficacy. It is recommended that clinical trials involvingspecificallytheuseofthesetechnologiestosupportthe treatmentofHIVareconducted.
60 I.C.V.d.Limaetal./InternationalJournalofMedicalInformatics92(2016)54–61
Summarytable
Whatwasalreadyknownonthistopic?
• Information and communication technologies subsidize
interventionsaimedatpatientmonitoringorpreventingthe transmission of HIV bypromoting improved accessibility andqualityofcare.
• Theliteraturehighlightsthepossibilityofapositiveeffect
onthelevelsofsatisfactionandpatientsafety,inadditionto improvingadherencetoantiretroviraltherapywiththeuse ofinformationandcommunicationtechnologiestosupport care.
Whatthisstudyaddedtoourknowledge?
• Theuseofinformationandcommunicationtechnologiesto
supportcareinadultswithHIVwasconsideredtobeeffective inimprovingadherencetoART.
• Themostprominenttypeofinformationandcommunication
technologywasthephone,whichwasusedtodeliver tele-phonecallsandsendalertmessages,aswellasreminders abouttakingmedications.
• Theelectronicdevicealarmwasnotconsideredtobe
effec-tiveforadherencetoART.
• Nostudiesmeetingthe inclusioncriteria focusing onthe
useofinteractive technologies,suchassmartphoneapps andsocialmediamonitoringinadultswithHIV,havebeen found.Therefore,conductingclinicaltrialsregardingtheuse ofthesetechnologiesto supportthetreatmentof HIVare recommended.
Forfutureexperimentalstudiesontheuseofinformationand communicationtechnologies,wesuggesttheanalysisof interven-tionsmediatedbysmartphonesandsocialmediaapplicationsand theirassociationwithadherencemeasurementmethods,aswell astheconductionofclinicaltrialsofthefactorialtype(multiple interventions),detaileddescriptionsofrandomizationandtheuse ofsimpleblinding.
Finally,informationtechnologiesareaninstrumentofproven efficacyandgreatcost-benefitswithrespecttotheexpansionof accesstocare.Moreover,thisreviewalsohighlightedthe narrow-ingoftherelationshipbetweenpatientsandhealthservices,with thepossibilityofmitigatingthedifficultiesexperiencedbypeople withHIVinachievingoptimallevelsofadherencetoART.
Authors’contributions
TheauthorICVLparticipatedinthemanagementofthe system-aticreviewwordingprocess.TheauthorsICVLandHOAcontributed duringthedifferentstagesofthereview,includingtheselection ofarticlesandthecriticalreading andanalysisofabstractsand selectedarticles.Theresearchers MTGG,FETLand TLAcritically analysedtheconstructionofthearticleandprovidedcomments. Finally, all authors read and approved the final version of the manuscript.
Acknowledgements
TheauthorsaregratefultotheNationalCouncilforScientificand TechnologicalDevelopment(CNPq)forprovidingfinancialsupport. WewouldalsoliketothankthemembersoftheStudyGroupon HIV/AIDSandAssociatedDiseasesoftheFederalUniversityofCeará fortheirencouragementandcontributions.
References
[1]V.V.Zotov,Informationandtelecommunicationtechnologiesandinformation
andcommunicationmedia:problemsofdefinitionandinterrelation,
Telecommun.RadioEng.68(17)(2009)1555–1560,http://dx.doi.org/10.
1615/TelecomRadEng.v68.i17.60.
[2]E.Murray,J.Burns,T.S.See,R.Lai,I.Nazareth,Interactivehealth communicationapplicationsforpeoplewithchronicdisease,Cochrane DatabaseSyst.Rev.4(2005)CD004274.
[3]M.Siddiqui,M.Y.Islam,B.A.I.Mufti,N.Khan,M.S.Farooq,M.G.Muhammad, M.Osama,D.Kherani,A.N.Kazi,A.M.Kazi,Assessingacceptabilityof hypertensive/diabeticpatientstowardsmobilehealthbasedbehavioral interventionsinPakistan:apilotstudy,Int.J.Med.Inform.84(11)(2015) 950–955.
[4]M.A.Chiasson,S.Hirshfield,C.Rietmeijer,HIVpreventionandcareinthe
digitalage,J.Acquir.ImmuneDefic.Syndr.55(2)(2010)94–97,http://dx.doi.
org/10.1097/QAI.0b013e3181fcb878.
[5]S.G.Deeks,S.R.Lewin,D.V.Havlir,Theendofaids:HIVinfectionasachronic
disease,Lancet382(9903)(2013)1525–1532,http://dx.doi.org/10.1016/
S0140-6736(13)61809-7.
[6]Unaids,GlobalReportUNAIDSReportontheGlobalAidsEpidemic,2012,
Availablefrom:http://www.unaids.org.br/documentos/UNAIDSGR2012em
en.pdf(assessed07.05.15).
[7]B.L.Genberg,I.B.Wilson,D.R.Bangsberg,J.Arnsten,K.Goggin,R.H.Remien,J.
Simoni,R.Gross,N.Reynolds,M.Rosen,H.Liu,Patternsofantiretroviral
therapyadherenceandimpactonHIVRNAamongpatientsinNorthAmerica,
AIDS26(11)(2012)1415–1423,http://dx.doi.org/10.1097/qad.
0b013e328354bed6.
[8]J.Côté,G.Godin,Y.G.Guéhéneuc,G.Rouleau,P.Ramirez-Garcìa,J.Otis,C.
Tremblay,G.Fadel,Evaluationofareal-timevirtualinterventiontoempower
personslivingwithHIVtousetherapyself-management:studyprotocolfor
anonlinerandomizedcontrolledtrial,Trials5(October(13))(2012)187,
http://dx.doi.org/10.1186/1745-6215-13-187.
[9]J.Hickner,ShiftingourfocustoHIVasachronicdisease,J.Fam.Pract.63(7) (2014)355.
[10]K.E.Muessig,M.Nekkanti,J.Bauermeister,S.Bull,L.B.Hightow-Weidman,A
systematicreviewofrecentsmartphone,InternetandWeb2.0interventions
toaddresstheHIVcontinuumofcare,Curr.HIV/AIDSRep.12(March(1))
(2015)173–190,http://dx.doi.org/10.1007/s11904-014-0239-3.
[11]G.Gartlehner,R.A.Hansen,D.Nissman,K.N.Lohr,T.S.Carey,Criteriafor DistinguishingEffectivenessFromEfficacyTrialsinSystematicReviews. TechnicalReview12,AgencyforHealthcareResearchandQuality,Rockville, MD,2006(PreparedbytheRTI-International—UniversityofNorthCarolina Evidence-basedPracticeCenterunderContractNo.290-02-0016,AHRQ Publication6(0046)).
[12]J.P.T.Higgins,S.Green,CochraneHandbookforSystematicReviewsof
InterventionsVersion5.1.0,TheCochraneCollaboration,2011,Available
from:www.cochrane-handbook.org(accessed21.05.15).
[13]M.Clarke,Cochranecollaboration,in:P.Armitage,T.Colton(Eds.),
EncyclopediaofBiostatistics,seconded.,JohnWiley&Sons,Chichester,2005. [14]A.K.Akobeng,Principlesofevidencebasedmedicine,Arch.Dis.Child.90
(August(8))(2005)837–840.
[15]A.R.Jadad,R.A.Moore,D.Carroll,C.Jenkinson,D.J.Reynolds,D.J.Gavaghan, H.J.Mcquay,Assessingthequalityofreportsofrandomizedclinicaltrials:is blindingnecessary?ControlClin.Trials17(February(1))(1996)1–12. [16]N.R.Reynolds,M.A.Testa,M.Su,M.A.Chesney,J.L.Neidig,I.Frank,S.Smith,J.
Ickovics,G.K.Robbins,Telephonesupporttoimproveantiretroviral medicationadherence:amultisite,randomizedcontrolledtrial,J.Acquir. ImmuneDefic.Syndr.47(January(1))(2008)62–68.
[17]M.H.Chung,B.A.Richardson,K.Tapia,S.Benki-Nugent,J.N.Kiarie,J.M.Simoni,
J.Overbaugh,M.Attwa,G.C.John-Stewart,Arandomizedcontrolledtrial
comparingtheeffectsofcounselingandalarmdeviceonHAARTadherence
andvirologicoutcomes,PLoSMed.8(March(3))(2011)1–11,http://dx.doi.
org/10.1371/journal.pmed.1000422(EpubMarch1,2011).
[18]C.Pop-Eleches,H.Thirumurthyc,J.P.Habyarimanae,J.G.Zivinf,M.P.
Goldsteing,D.Walqueg,L.MacKeenh,J.Haberer,S.Kimaiyoj,J.Sidle,D.
Ngarem,D.R.Bangsberg,Mobilephonetechnologiesimproveadherenceto
antiretroviraltreatmentinaresource-limitedsetting:arandomized
controlledtrialoftextmessagereminders,AIDS25(March(6))(2011)
825–834,http://dx.doi.org/10.1097/qad.0b013e32834380c1.
[19]M.E.Belzer,S.Naar-King,J.Olson,M.Sarr,S.Thornton,S.Y.Kahana,A.H.Gaur,
L.F.Clark,Theuseofcellphonesupportfornon-adherentHIV-Infectedyouth
andyoungadults:aninitialrandomizedandcontrolledinterventiontrial,
AIDSBehav.18(4)(2014)686–696,
http://dx.doi.org/10.1007/s10461-013-0661-3.
[20]K.Fiscella,M.Boyd,J.Brown,J.Carroll,A.Cassells,R.Corales,W.Cross,N.
El’Daher,S.Farah,S.Fine,R.Fowler,A.Hann,A.Luque,J.Rodriquez,M.
Sanders,J.Tobin,ActivationofpersonslivingwithHIVfortreatment,the
greatstudy,BMCPublicHealth15(1)(2015),http://dx.doi.org/10.1186/
s12889-015-2382-1.
[21]R.K.Claborn,T.R.Leffingwella,M.B.Miller,E.Meier,JohnnyR.Stephens,Pilot
studyexaminingtheefficacyofanelectronicinterventiontopromoteHIV
medicationadherence,AIDSCare26(3)(2013)404–409,http://dx.doi.org/10.
1080/09540121.2013.824534(EpubAugust5,2013).
[22]R.L.Lester,P.Ritvo,E.J.Mills,A.Kariri,S.Karanja,M.H.Chung,W.Jack,J.
Habyarimana,M.Sadatsafavi,M.Najafzadeh,C.A.Marra,B.Estambale,E.
Ngugi,T.B.Ball,L.Thabane,L.J.Gelmon,J.Kimani,M.Ackers,F.A.Plummer,
Effectsofamobilephoneshortmessageserviceonantiretroviraltreatment
adherenceinKenya(WelTelKenya1):arandomisedtrial,Lancet376(9755)
(2010)1838–1845,http://dx.doi.org/10.1016/s0140-6736(10)61997-6.
[23]H.Hardy,V.Kumar,G.Doros,E.Farmer,M.L.Drainoni,D.Rybin,D.Myung,J.
personalizedcellularphoneremindersystemtoenhanceadherenceto
antiretroviraltherapy,AidsPatientCareSTDS25(3)(2011)153–161,http://
dx.doi.org/10.1089/apc.2010.0006(EpubFebruary16,2011).
[24]L.Mbuagbaw,L.Thabane,P.Ongolo-Zogo,R.T.Lester,E.J.Mills,M.Smieja,L.
Dolovich,C.Kouanfack,TheCameroonMobilePhoneSMS(CAMPS)trial:a
randomizedtrialoftextmessagingversususualcareforadherenceto
antiretroviraltherapy,PLoSOne7(December(12))(2012)1–7,http://dx.doi.
org/10.1371/journal.pone.0046909.
[25]C.Catalani,W.Philbrick,H.Fraser,P.Mechael,D.M.Israelski,MHealthforHIV
treatment&prevention:asystematicreviewoftheliterature,OpenAIDSJ.13
(August(7))(2013)17–41,http://dx.doi.org/10.2174/1874613620130812003
(eCollection2013).
[26]J.E.Haberer,J.Kiwanuka,D.Nansera,I.B.Wilson,D.R.Bangsberg,Challenges
inusingmobilephonesforcollectionofantiretroviraltherapyadherencedata
inaresource-limitedsetting,AIDSBehav.14(December(6))(2010)
1294–1301,http://dx.doi.org/10.1007/s10461-010-9720-1.
[27]S.B.Mannheimer,E.Morse,J.P.Matts,L.Andrews,C.Child,B.Schmetter,G.H. Friedland,TerryBeirnCommunityProgramsforClinicalResearchonAIDS, Sustainedbenefitfromalongtermantiretroviraladherenceintervention. Resultsofalargerandomizedclinicaltrial,J.Acquir.ImmuneDefic.Syndr.43 (Suppl.1)(2006)S41–47.
[28]R.H.Remien,M.J.Stirratt,C.Dolezal,J.S.Dognin,G.J.Wagner,A. Carballo-Dieguez,N.El-Bassel,T.M.Jungle,Couple-focusedsupportto improveHIVmedicationadherence:arandomizedcontrolledtrial,AIDS19 (May(8))(2005)807–814.
[29]B.K.C.Mukund,P.J.Murray,Cellphoneshortmessagingservice(SMS)for HIV/AIDSinSouthAfrica:aliteraturereview,Stud.HealthTechnol.Inform. 160(Pt.1)(2010)530–534.
[30]R.Lester,S.Karanja,Mobilephones:exceptionaltoolsforHIV/AIDS,health,
andcrisismanagement,LancetInfect.Dis.8(December(12))(2008)738–739,
http://dx.doi.org/10.1016/s1473-3099(08)70265-2.
[31]N.Dowshen,L.M.Kuhns,A.Johnson,B.J.Holoyda,R.Garofalo,Improving adherencetoantiretroviraltherapyforyouthlivingwithHIV/AIDS:apilot studyusingpersonalized,interactive,dailytextmessagereminders,J.Med. InternetRes.14(April(2))(2012)e51.
[32]N.R.Reynolds,Theproblemofantiretroviraladherence:aself-regulatory modelforintervention,AIDSCare15(February(1))(2003)117–124.
[33]J.Wise,D.Operario,Useofelectronicreminderdevicestoimproveadherence
toantiretroviraltherapy:asystematicreview,AIDSPatientCareSTDS22
(June(6))(2008)495–504,http://dx.doi.org/10.1089/apc.2007.0180.
[34]J.M.Simoni,D.Huh,P.A.Frick,C.R.Pearson,M.P.Andrasik,P.J.Dunbar,T.M. Hooton,Peersupportandpagermessagingtopromoteantiretroviral modifyingtherapyinSeattle:arandomizedcontrolledtrial,J.Acquir.Immune Defic.Syndr.52(December(4))(2009)465–473.
[35]R.Schnall,J.Travers,M.Rojas,A.Carballo-Diéguez,eHealthinterventionsfor
HIVpreventioninhigh-riskmenwhohavesexwithmen:asystematicreview,
J.Med.InternetRes.16(5)(2014)e134,http://dx.doi.org/10.2196/jmir.3393.
[36]S.B.Hulley,S.R.Cummings,W.S.Browner,D.G.Grady,T.B.Newman,Designing ClinicalResearch,fourthed.,LippincottWilliams&Wilkins,USA,2013. [37]J.M.Simoni,A.E.Kurth,C.R.Pearson,D.W.Pantalone,J.O.Merrill,P.A.Frick,
Self-reportmeasuresofantiretroviraltherapyadherence:areviewwith recommendationsforHIVresearchandclinicalmanagement,AIDSBehav.10 (May(3))(2006)227–245.
[38]G.Wagner,L.G.Miller,Istheinfluenceofsocialdesirabilityonpatients’ self-reportedadherenceoverrated?J.Acquir.ImmuneDefic.Syndr.35 (February(2))(2004)203–204.