ABSTRACT
Cystic ibrosis (CF) is an autosomal recessive genetic disorder characterized by
dysfunction of the CFTR gene. It is a multisystem disease that most often affects White
individuals. In recent decades, various advances in the diagnosis and treatment of CF
have drastically changed the scenario, resulting in a signiicant increase in survival and
quality of life. In Brazil, the current neonatal screening program for CF has broad coverage,
and most of the Brazilian states have referral centers for the follow-up of individuals with
the disease. Previously, CF was limited to the pediatric age group. However, an increase
in the number of adult CF patients has been observed, because of the greater number of
individuals being diagnosed with atypical forms (with milder phenotypic expression) and
because of the increase in life expectancy provided by the new treatments. However,
there is still great heterogeneity among the different regions of Brazil in terms of the
access of CF patients to diagnostic and therapeutic methods. The objective of these
guidelines was to aggregate the main scientiic evidence to guide the management
of these patients. A group of 18 CF specialists devised 82 relevant clinical questions,
divided into ive
categories:
characteristics of a referral center; diagnosis; treatment of
respiratory disease; gastrointestinal and nutritional treatment; and other aspects. Various
professionals working in the area of CF in Brazil were invited to answer the questions
devised by the coordinators. We used the PubMed database to search the available
literature based on keywords, in order to ind the best answers to these questions.
Keywords:
Cystic ibrosis/diagnosis; Cystic ibrosis/therapy; Cystic ibrosis/complications;
Practice guideline.
Brazilian guidelines for the diagnosis and
treatment of cystic ibrosis
Rodrigo Abensur Athanazio
1*, Luiz Vicente Ribeiro Ferreira da Silva Filho
2,3*,
Alberto Andrade Vergara
4, Antônio Fernando Ribeiro
5, Carlos Antônio Riedi
6,
Elenara da Fonseca Andrade Procianoy
7, Fabíola Villac Adde
2,
Francisco José Caldeira Reis
4, José Dirceu Ribeiro
5, Lídia Alice Torres
8,
Marcelo Bicalho de Fuccio
9, Matias Epifanio
10, Mônica de Cássia Firmida
11,
Neiva Damaceno
12, Norberto Ludwig-Neto
13,14, Paulo José Cauduro Maróstica
7,15,
Samia Zahi Rached
1, Suzana Fonseca de Oliveira Melo
4;
Grupo de Trabalho das Diretrizes Brasileiras de Diagnóstico e Tratamento da
Fibrose Cística.
Correspondence to:
Rodrigo Abensur Athanazio. Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina da Universidade de São Paulo, Avenida Dr. Enéas de Carvalho Aguiar, 44, CEP 05403-900, São Paulo, SP, Brasil.
Tel.: 55 11 3069-7201. E-mail: [email protected]
Financial support: This study received assistance in editorial matters and medical writing from Springer Healthcare, with inancial support from Roche Brasil, Teva Brasil, Zambon Laboratórios Farmacêuticos, and Vertex Pharmaceuticals. The authors take full responsibility for the content of this publication. The sponsors had no inluence on data collection or analysis or on the decision to publish the information presented here.
*Os autores contribuíram de forma equivalente para o trabalho. *These authors contributed equivalently to this work.
INTRODUCTION
Cystic ibrosis is an autosomal recessive genetic disorder characterized by
dysfunction of the
cystic ibrosis transmembrane conductance regulator (
CFTR)
gene, which encodes a protein that regulates chloride transmembrane conductance.
It is a multisystem disease that most often affects White individuals. In Brazil, the
incidence of cystic ibrosis is estimated to be 1 in 7,576 live births; however, there
are regional differences, with higher values being found in the southern states.
(1)In recent decades, various advances in the diagnosis and treatment of cystic ibrosis
have drastically changed the scenario of this disease, resulting in a signiicant increase
in survival and a gain in quality of life. In Brazil, the current neonatal screening
program for cystic ibrosis has broad coverage, and most of the Brazilian states
have referral centers for the follow-up of individuals with the disease. Previously,
cystic ibrosis was limited to the pediatric age group. However, an increase in the
number of adult patients with cystic ibrosis has been observed, because of the
1. Instituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
2. Instituto da Criança, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, São Paulo (SP) Brasil.
3. Hospital Albert Einstein, São Paulo (SP) Brasil.
4. Hospital Infantil João Paulo II, Rede Fundação Hospitalar do Estado de Minas Gerais – FHEMIG – Belo Horizonte (MG) Brasil. 5. Hospital de Clínicas, Universidade
Estadual de Campinas, Campinas (SP) Brasil.
6. Universidade Federal do Paraná, Curitiba (PR) Brasil.
7. Hospital de Clínicas de Porto Alegre, Porto Alegre (RS) Brasil. 8. Hospital das Clínicas, Faculdade
de Medicina de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto (SP) Brasil.
9. Hospital Júlia Kubitschek, Fundação Hospitalar do Estado de Minas Gerais – FHEMIG – Belo Horizonte (MG) Brasil. 10. Hospital São Lucas, Pontifícia
Universidade Católica do Rio Grande do Sul, Porto Alegre (RS) Brasil. 11. Universidade do Estado do Rio de
Janeiro, Rio de Janeiro (RJ) Brasil. 12. Irmandade da Santa Casa de
Misericórdia de São Paulo, São Paulo (SP) Brasil.
13. Hospital Infantil Joana de Gusmão, Florianópolis (SC) Brasil.
14. Serviço de Fibrose Cística e Triagem Neonatal para Fibrose Cística, Secretaria Estadual de Saúde de Santa Catarina, Florianópolis (SC) Brasil.
15. Universidade Federal do Rio Grande do Sul Porto Alegre (RS) Brasil.
Submitted: 4 March 2017 . Accepted: 22 May 2017.
greater number of individuals being diagnosed with
atypical forms (with milder phenotypic expression) and
because of the increase in life expectancy provided by
the new treatments.
(2-4)However, there is still great
heterogeneity among the different regions of Brazil in
terms of the access of patients with cystic ibrosis to
diagnostic and therapeutic methods. The objective of
this publication was to aggregate the main scientiic
evidence to guide the management of patients with
cystic ibrosis, this body of evidence being compiled
by the main health professionals involved in caring
for this disease in Brazil.
METHODS
A group of 18 cystic ibrosis specialists (coordinators)
devised 82 relevant clinical questions, divided into ive
categories: characteristics of a referral center; diagnosis;
treatment of respiratory disease; gastrointestinal and
nutritional treatment; and other aspects. Various
professionals working in the area of cystic ibrosis in
Brazil were invited to answer the questions devised
by the coordinators of the guidelines.
We used the PubMed database to search the available
literature based on keywords, in order to ind the
best answers to these questions. In addition, manual
searches of references in articles or books were
performed. The Oxford Centre for Evidence-Based
Medicine guidelines were used to classify the level of
evidence for the questions regarding the treatment
chapters. The guidelines include a classiication system
for levels of evidence of studies, with levels of evidence
ranging from “1” (highest level) to “5” (lowest level).
The classiication system was simpliied in 2011 in
order to facilitate its clinical application. Chart 1A (JBP
online appendix—
http://jornaldepneumologia.com.br/
detalhe_anexo.asp?id=51
) provides further details on
the current Oxford classiication system.
A total of 2,352 publications were identiied using
the keyword search strategy, manual searches, and
reference suggestions made by the authors. A total
of 243 articles were selected for the present paper.
The irst version of the text was written between
March and August of 2016. The coordinators of each
area were responsible for the validation of the level
of evidence classiication. In controversial cases, the
questions were brought to a consensus meeting of
coordinators on September 24, 2016. The inal version
was reviewed by the national coordinators (the irst
two authors) and sent to the editor of the JBP in
February of 2017.
CHARACTERISTICS OF A REFERRAL
CENTER
How important is a referral center in the
care of patients with cystic ibrosis?
The complexity of cystic ibrosis and the peculiarities of
its treatment result in the need for specialized treatment
centers.
(5)There is evidence that treatment at specialized
referral centers, which have a multidisciplinary team,
results in better clinical results, with an impact on
prognosis.
(6,7)What is a referral facility and what is a
referral center?
A referral center is deined as one that treats at
least 50 patients regularly. It should have a structure
that meets the needs related to diagnosis, follow-up,
and treatment.
A referral facility is one that treats fewer than 50
patients, and it can have a less complex structure.
It should be afiliated with a referral center for the
purposes of continuing education and of supplementing
any needs.
(5)How important is a multidisciplinary team?
What would be the composition of such a
team?
Given that cystic ibrosis is characterized by chronic
multisystem involvement, it requires a multidisciplinary
care model.
(5)The care provided by a multidisciplinary
team enables more comprehensive and effective
treatments, resulting in an increased patient life
expectancy.
(5,8,9)The minimum multidisciplinary team
for treating patients with cystic ibrosis should consist
of the following professionals: pediatricians (when
treatment is provided to children and adolescents);
pulmonologists; gastroenterologists; physical therapists;
nutritionists; nurses; psychologists; pharmacists; and
social workers.
Are there differences between pediatric
and adult centers? Are there advantages to
planning for transitioning from pediatric to
adult care?
Pediatric cystic ibrosis centers are quite different
from adult cystic ibrosis centers. Adults have control
and autonomy over their care. Pediatric centers need
to meet demands that are characteristic of childhood,
both in terms of structure and health professionals.
Adult centers need resources to treat cases of greater
complexity (comorbidities and different and more
frequent complications, as well as pregnancy).
(10)Transitioning an adolescent patient into an adult
center is challenging, and there is evidence that
transition programs optimize the process of transfer
to the adult center.
(11-15)What should the referral center
infrastructure be like? What are the basic
ancillary tests?
Patients should have 24-h/day access to the center
or to emergency facilities afiliated with the center.
(16)Each referral center should have or should ensure
access to:
•
A laboratory for conducting tests to conirm the
diagnosis of cystic ibrosis: sweat testing and/
or
CFTR
gene mutation analysis
•
A pulmonary function laboratory
•
A microbiology laboratory with experience in and
resources for identifying typical cystic ibrosis
pathogens
•
A radiology department with CT
•
A clinical pathology laboratory with the capacity
to perform routine tests, including hematologic
tests, liver and kidney function tests, serology,
and determination of proteins, vitamins, and
immunoglobulins.
How important is microbiological
segregation? How should it be done?
There is ample evidence that pathogen transmission
can occur among individuals with cystic ibrosis,
especially via droplets and contact. It can involve
virulent strains, worsening disease progression.
Infection control and prevention measures have been
effective in decreasing pathogen transmission. Patient
segregation should be instituted inside and outside
the hospital setting to prevent cross infection. Cystic
ibrosis centers should provide adequate structure and
have a clear Infection control and prevention policy,
including separate days of treatment for patients or use
of different treatment spaces on the basis of patient
colonization.
(5,17-19)How important is commitment to care,
research, and teaching?
A cystic ibrosis center should be committed to active
participation in clinical and translational research,
enabling patient participation in clinical trials. Education,
research, and contribution to cystic ibrosis registries
should be preferably performed by all centers. The
various members of the multidisciplinary team should
play an active role in research and education. Their
work contributes to increasing and disseminating
specialized knowledge, which plays a signiicant role
in improving the quality of care.
(5)What are the advantages of cooperation
with cystic ibrosis patient/parent
associations and with the Brazilian Cystic
Fibrosis Study Group?
Cystic ibrosis patient/parent associations aim at
defending the interests of this group of individuals,
which includes making the disease known and improving
diagnosis and treatment, in order to increase survival,
improve quality of life, and integrate patients into
society.
(5)In North America and Europe, some of these
associations still play an important role in promoting and
funding scientiic research and in registering patients.
In Brazil, bringing cystic ibrosis patient/parent
associations closer to health professionals working in
cystic ibrosis (currently represented by the Brazilian
Cystic Fibrosis Study Group) would offer great
advantages that could improve the current situation,
such as aid in the inclusion of all Brazilian patients in
the national registry (Brazilian Cystic Fibrosis Registry)
and monitoring of the availability of medications in
the various Brazilian states, in addition to the joining
of forces to submit to the Federal Government a new
(more comprehensive) directive on the care of the
cystic ibrosis patient.
DIAGNOSIS
How does one conirm the diagnosis of
cystic ibrosis after positive newborn
screening?
The cystic ibrosis newborn screening algorithm
used in Brazil is based on two determinations of
immunoreactive trypsinogen levels, the second of which
is performed within 30 days of life. If screening is positive
(i.e., two positive determinations), sweat testing is
performed to conirm or rule out cystic ibrosis. Sweat
chloride concentrations ≥ 60 mmol/L, as measured
by quantitative methods, in two samples, conirm the
diagnosis. Diagnostic alternatives are detection of two
cystic ibrosis-related mutations and CFTR functional
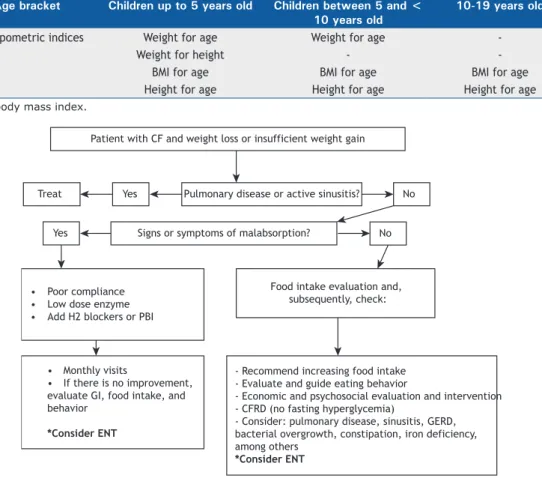
tests. Figure 1 shows a lowchart summarizing how
infants with positive newborn screening results should
be managed.
(20,21)Does a positive or negative newborn
screening result conirm or rule out the
diagnosis of cystic ibrosis?
No. Newborn screening for cystic ibrosis identiies
newborns at risk for the disease, but does not conirm
the diagnosis. The rate of false-positive results with the
algorithm based on measurement of immunoreactive
trypsinogen levels is quite high. Conversely, a negative
newborn screening result does not rule out the
diagnosis.
(22,23)After conirmation of the diagnosis of cystic
ibrosis in patients with positive newborn
screening results, when should the patients
be referred to a cystic ibrosis referral
center?
Immediately after diagnosis, because cystic ibrosis
requires early multidisciplinary management in order
to maintain normal nutritional status and timely treat
respiratory infections.
(20,23)What are the steps involved in sweat
testing? How does one ensure the quality of
sweat testing?
It is recommended that laboratories qualiied to
perform sweat testing should have internal and external
quality control and should perform at least 100 tests
per year (at least 10 tests per year per technician).
The percentage of insuficient sweat samples should
not exceed 5% of the total samples collected.
(24-26)What are the main approved methods of
quantitative sweat chloride determination?
Chart 1 describes the main methods of chloride
determination, all of which must be validated in each
laboratory before use.
(24,25)What is the role of sweat conductivity testing?
Despite the high level of agreement between sweat
conductivity results and sweat chloride concentrations,
Table 1. Reference values for sweat test.Result
Chloride,
mmol/L
Electrical
conductivity,
mmol/L
Normal
< 30
< 60
Intermediate
30-59
60-90
Positive
a≥ 60
> 90
aQuantitative chloride analysis in sweat should be carried out on a different day in order to conirm the result.
Figure 1. Management of cases with positive neonatal screening for cystic ibrosis. CF: cystic ibrosis; and IRT: immunoreactive trypsinogen. Adapted from Farrel et al.(21)
Neonatal screening results for CF:
IRT/IRT (1st quantification within 5 days of age, 2nd quantification within 30 days of age)
Evaluation at the Cystic Fibrosis Center:
4-6 weeks Up to 4 weeks
≥ 60 mmol/L 30-59 mmol/L ≤ 29 mmol/L
2 CF mutations FC
0-1 mutation OR no genetic study
Confirmed CF diagnosis Possible CF diagnosis
Improbable CF diagnosis
Referral to CF Center: - Identification of mutations - Clinical evaluation - Treatment onset for health maintenance - Sweat test in siblings
CF mutation identification: panels or CFTR
gene sequencing
Supporting methods
1-2 months
2-6 months
Repeat sweat test Sweat test (2 samples)
Age
sweat conductivity testing is still considered a screening
test.
(26)It is recommended that a patient with a sweat
conductivity result greater than or equal to 50 mmol/L
should undergo quantitative testing. Sweat conductivity
testing has the advantages of being easy to use and
yielding immediate results.
(24,27,28)What are the minimum criteria for a
laboratory to perform CFTR mutation
studies?
•
Certiication by the Brazilian National Health
Oversight Agency
•
Capability to perform DNA extraction with different
methods and from different sample types
•
Ability to identify the F508del mutation and other
more prevalent mutations
•
Availability to perform
CFTR
mutation panel
analysis and/or complete
CFTR
sequencing, either
in its facilities, or by referral to other laboratories
•
Capability to interpret and report pathogenic
variants
Should all patients with cystic ibrosis
undergo genetic testing? How important is it
to undergo genetic testing?
allowing the diagnosis of cystic ibrosis (Chart 2). In
addition, there are drugs that act on speciic mutations
(CFTR protein correctors and potentiators), some
of which have been approved in various countries,
whereas others are in development.
(21,29-32)What mutation panel should be
investigated?
The investigation of mutations in the
CFTR
gene is
described in Chart 3.
(31-35)When are CFTR functional tests indicated?
CFTR functional tests are indicated when sweat
testing and genetic analysis are inconclusive. In
essence, these tests assess CFTR protein function by
measurement of chloride transport. Currently, nasal
potential difference and intestinal current measurements
are internationally standardized. Other promising tests,
such as assessment of CFTR function by evaporimetry
and by sweat gland potential difference measurement,
are being studied.
(36,37)TREATMENT OF RESPIRATORY DISEASE
What types of respiratory samples are most
appropriate, how are they obtained, and how
important are they?
Respiratory secretion samples are essential for
follow-up of chronic bacterial infection of the airways in
patients with cystic ibrosis, as well as for identiication
of opportunistic infections and as a follow-up method for
therapeutic interventions. Expectorated sputum is the
specimen of choice. For children who cannot expectorate,
collect oropharyngeal cough swabs (tonsillar region
and soft palate), nasopharyngeal aspirates, secretion
following inhalation of 5% hypertonic saline solution,
or bronchoalveolar lavage luid. These samples should
be delivered to the laboratory immediately or kept
under refrigeration for up to 3 h.
(38,39)(Level of evidence: 4)
When should the samples be collected?
The samples should be collected at visits (with a
maximum interval of 3 months), during exacerbations,
and following treatment to eradicate the infection.
Annual screening for mycobacteria and fungi is
recommended for patients who cannot expectorate
or for those with an unfavorable clinical course.
(40)(Level of evidence: 5)
What are the routine culture methods and
media?
Bronchoalveolar lavage luid specimens must be
quantitatively cultured. The recommended culture
media for routine microbiological investigation in cystic
ibrosis are as follows:
•
Blood agar: universal for routine microbiological
investigations
•
Mannitol agar: selective for
Staphylococcus aureus
•
MacConkey agar: for gram-negative bacilli
(inclu-ding
Pseudomonas aeruginosa
,
Achromobacter
spp., and
Stenotrophomonas
spp.)
•
Burkholderia cepacia
complex-selective agar
•
Chocolate agar for Streptococcus pneumoniae
and
Haemophilus inluenzae
•
Sabouraud agar – for fungi, including
Aspergillus
spp. – supplemented with chloramphenicol or
gentamicin
•
Liquid culture media, depending on the automation
available, and a solid medium, such as
Lowenstein--Jensen agar. For non-tuberculosis mycobacteria,
blood agar and
Burkholderia cepacia
selective
agar can also be used provided that these media
are incubated for 14 days.
(39,41-45)(Level of evidence: 5)
What are the methods of bacterial
identiication?
•
Phenotypic methods: typical
S. aureus
,
P.
aeruginosa
, and
Stenotrophomonas maltophilia
colonies are easily recognized, and few tests
are needed.
•
Commercial, non-automated phenotypic kits:
when associated with typical characteristics, they
can be used for the identiication of
S. aureus
and some glucose-nonfermenting gram-negative
Chart 1. Methods of quantitative of sweat chloride determination.
Method
Description
Observation
Titration or colorimetry
Chloride concentration is quantiied by
measuring the absorption of a speciic light
wavelength. The intensity of the color is
directly proportional to the concentration
of chloride. The Schales & Schales manual
titration method using mercury nitrate is
commonly used.
It depends on the experience of the
technician in performing the procedure.
Possible subjectivity during the analysis.
Coulometry
Analytical chemistry technique that uses an
electrolysis reaction to measure changes in
current resistance between the electrodes.
The chloride concentration is equivalent to
the generated current.
It requires a chloridometer.
Selective ion electrode
It converts the activity of a speciic ion
dissolved in a solution into an electrical
potential that is measured by a voltmeter.
Low sensitivity.
bacilli, such as
P. aeruginosa
,
S. maltophilia
, and
Achromobacter
spp., but are not suitable for the
identiication of
B. cepacia
complex,
Burkholderia
gladioli
,
Pandoraea
spp., or
Ralstonia
spp.
•
Automated methods: they are not recommended
for the identiication of most
glucose-nonfermen-ting gram-negative bacilli.
•
Molecular tests: they are recommended for the
characterization of
Achromobacte
r spp.,
B. cepacia
complex, and the genera
Ralstonia
,
Cupriavidus
and
Pandoraea
.
•
Matrix-assisted laser desorption ionization
time--of-light (MALDI-TOF) mass spectrometry (MS): it
represents a rapid alternative, but has limitations,
especially in identifying glucose-nonfermenting
gram-negative bacilli.
(42,43,46)(Level of evidence: 5 for all methods, except MALDI-TOF
MS for the identiication of glucose-nonfermenting
gram-negative bacilli—level of evidence: 2)
What is the role of pulmonary function
testing in the management of patients with
cystic ibrosis?
Spirometry should be performed starting at age 5
years at every clinical visit or at least twice a year. Testing
with and without bronchodilators is recommended.
Washout techniques, with determination of the lung
clearance index, have increasing and promising use
in identifying early lung disease.
Studies have shown that FEV
1is essential for assessing
the course and progression of cystic ibrosis, as well as
for early detection of acute pulmonary exacerbations,
being correlated with quality of life. FEF
25-75%should
also be taken into consideration, since it may be altered
earlier. Whole-body plethysmography and oscillometry
can complement the functional assessment.
(9,47-50)(Level of evidence: 5)
What imaging tests should be performed in
patients with cystic ibrosis? How often?
Chest X-ray is the most widely used test in the
evaluation of patients with cystic ibrosis and is
correlated with pulmonary function testing in detecting
disease progression.
(51,52)Chart 2. Beneits from the study of CFTR gene mutations.
Benefits from the study of CFTR gene mutations
1. Patients with an established diagnosis of CF:
- indication of mutation-speciic therapy
- determination of prognosis (genotype-phenotype correlation)
2. Investigation of atypical forms of CF
a3. Genetic counseling:
- Asymptomatic individuals with no family history of CF, when the spouse has CF or is an asymptomatic carrier of a
mutation in the
CFTR
gene (heterozygote)
- Asymptomatic individuals when they have irst-degree, second-degree, or third-degree relatives with CF in the
family
4. Prenatal/preimplantation genetic diagnosis of CF:
- Current or future pregnancy, in couples who already have a child with CF
- Heterozygous couples if the test cannot be done on a child with CF
- Embryos of heterozygous couples
When the fetus has a hyperechoic bowel, dilatation of intestinal loops, growth retardation, or overgrowth suggestive
of uniparental disomy
CF: cystic ibrosis. aAtypical forms of CF: symptoms consistent with CF and intermediate results in the sweat chloride test.
Chart 3. Stepwise molecular analysis for the identiication of CFTR mutations.
Mutation
Technique
Reason
F508del
Conventional or real-time PCR
Higher prevalence
Research of two mutations
already identiied in the
family
PCR site-directed mutagenesis; RFLP, reverse dot blot
hybridization; ARMS; minisequencing or similar technique
Index case in the family
Individual identiication
of mutations of higher
prevalence by targeted
panels
Real-time PCR using hybridization probes; commercial
mutation arrays and kits
High prevalence;
need for limited
infrastructure
Mutations not identiied in
previous tests
Bidirectional sequencing of the
CFTR
gene by Sanger or
next-generation sequencing of all exons and lanking exons/introns
of the
CFTR
gene, including poly-T variants in intron 8
Identiication of
less prevalent
CFTR
mutations
Mutations not identiied in
previous tests
Analysis of large rearrangements in the
CFTR
gene, including
deletions, insertions, and duplications, by semiquantitative
techniques, such as real-time PCR, MLPA, or quantitative
luorescent techniques (luorescent multiplex PCR)
Identiication of
less prevalent
CFTR
mutations
Chest HRCT is more accurate in the diagnosis and
follow-up of lung lesions in individuals of all ages,
including children with normal pulmonary function.
(53-55)This beneit is questionable in infants, and there are
technical obstacles inherent to this age group.
(56)Magnetic resonance imaging of the chest has advanced
in recent years and may become a future option because
it is a radiation-free method.
(57)Although there is no consensus regarding the
frequency of imaging tests, an annual chest X-ray
is recommended. In addition, it is suggested that,
in the presence of clinical, functional, or radiological
deterioration, a chest HRCT should be performed.
Periodic follow-up with chest HRCT every 2 to 4 years
may be indicated on a case-by-case basis. In cases of
pulmonary exacerbation in cystic ibrosis, chest X-ray
and chest HRCT can be used, always considering the
use of the lowest radiation dose possible.
(58,59)(Level of evidence: 2 for chest HRCT in individuals of
all ages, except infants) (Level of evidence: 5 for chest
X-ray and magnetic resonance imaging)
How important are nebulizers in the
treatment of lung disease in cystic ibrosis?
The daily treatment of lung disease in cystic ibrosis
includes nebulization of various medications that are
key to maintaining lung health, and an inhaler system
is essential for all patients with cystic ibrosis.
(60-62)(Level of evidence: 5)
What inhaler system should be used for
each type of inhalation therapy in cystic
ibrosis?
Matching a substance to be inhaled with the right
type of inhaler system is essential for ensuring the
eficacy of treatment. Given the great variability of
devices, it is recommended that the inhaler systems
tested in the clinical trials of the medications should
be used.
(63,64)The following types are often used for each
therapy
(64,65):
•
Ultrasonic nebulizers: hypertonic saline
•
Air-jet nebulizers: tobramycin; colistimethate;
dornase alfa; and hypertonic saline
•
Active vibrating mesh nebulizers: tobramycin;
colistimethate; dornase alfa; and aztreonam
•
Passive vibrating mesh nebulizers that adjust
to the patient’s breathing pattern: tobramycin
and colistimethate
(Level of evidence: 2)
What care should be given to inhalation
therapy and chest physiotherapy devices?
Devices for the treatment of lung disease in cystic
ibrosis include nebulizers and equipment used in
chest physiotherapy for secretion removal. Bacterial
contamination of nebulizers of patients with cystic
ibrosis has been described, and educational programs
on cleaning and disinfection of these devices have
an impact on this situation. Cleaning after each use
and daily disinfection by boiling, 70-90% alcohol,
isopropyl alcohol, or 3% hydrogen peroxide are
recommended.
(17,66-69)(Level of evidence: 3)
What chest physiotherapy techniques are
indicated in the treatment of lung disease?
Chest physiotherapy techniques should be performed
daily after diagnosis in all patients with cystic ibrosis.
(70)Chest physiotherapy has proven clinical beneits when
compared with no intervention; however, there is no
evidence of the superiority of one technique over the
other. Patient preference is an essential factor for
adherence to treatment, but the use of devices such
as positive expiratory pressure masks and oscillatory
positive expiratory pressure devices such as the
Flutter
®, the Shaker
®, and the Acapella
®is of great
value and gives the patient independence.
(71)The use
of high-frequency chest wall oscillation devices, despite
also giving the patient independence, was found to be
inferior to the use of positive expiratory pressure masks
in a recent study.
(72)Noninvasive ventilation may be
used as an adjunct to airway clearance therapy and
in patients with advanced disease and hypercapnic
respiratory failure.
(73-76)(Level of evidence: 2 for chest physiotherapy)
(Level of evidence: 2 for the superiority of positive
expiratory pressure masks vs. high-frequency chest
wall oscillation devices)
(Level of evidence: 2 for noninvasive ventilation vs. no
noninvasive ventilation as an adjuvant in the treatment
of patients with advanced disease and hypercapnia)
What is the role of exercise in cystic
ibrosis?
Exercise (aerobic and anaerobic) can aid in functional
and postural outcomes, as well as in the self-esteem
of patients with cystic ibrosis. An exercise frequency
of 3-5 times a week and an exercise duration of 20-30
min are recommended, with beneits being observed
from 6 weeks onward. Exercise should be part of the
recommendations for patients with cystic ibrosis,
including during hospitalizations. Physical activity does
not replace chest physiotherapy.
(77-82)(Level of evidence: 2)
What are the indications for the use of
dornase alfa and what is its dosing schedule?
Inhaled dornase alfa can be used at any time, at least
30 min before chest physiotherapy.
(93,94)(Level of evidence: 1)
When should dornase alfa be used in
children under 6 years of age?
The use of dornase alfa should be considered in
younger patients with persistent respiratory symptoms
or with evidence of early lung disease (bronchiectasis,
for example).
(40,95-97)(Level of evidence: 2)
What is the role of hypertonic saline and
mannitol? What are their recommended
concentrations?
Hypertonic saline solution and mannitol are
mucokinetic substances. They function as moisturizers
on the airway surface, as osmotic agents, changing
the rheological properties of mucus.
Twice-daily administration of 7% hypertonic
saline solution reduces the number of respiratory
exacerbations and produces improvement in pulmonary
function and quality of life. Long-term studies are
needed to determine whether there is sustained
improvement.
(87,98-100)Mannitol is available as dry-powder for inhalation
(400 mg twice daily). Its use is associated with reduced
nebulizer treatment time, clinical improvement, and
pulmonary function improvement.
(101-103)The use
of mannitol is safe and well tolerated but should be
preceded by the use of inhaled bronchodilators, given
that they can act as irritating substances. Both are
complementary approaches to dornase alfa therapy.
(Level of evidence: 1 for hypertonic saline and for
mannitol)
What should P. aeruginosa eradication
therapy be like?
Eradication therapy in cases of irst acquisition of
P.
aeruginosa
or early infection with
P. aeruginosa
aims
to eradicate the bacterium and delay chronic infection.
There are various therapeutic strategies, none being
superior to the other. The most widely recommended
strategy is to use inhaled tobramycin (300 mg)
twice daily for 28 days.
(104-107)Sodium colistimethate
(1,000,000 to 2,000,000 IU, twice daily) is an alternative
with consistent results and should be associated with
oral ciproloxacin for 2-3 weeks.
Inhalation therapy may be extended for 2-3 months.
Intravenous antibiotic therapy for 2 weeks may be an
option in selected cases and should always be followed
by inhaled antibiotic therapy. Successful eradication
is deined as negative bacterial culture results over a
1-year period after treatment completion. Eradication
therapy, in addition to having signiicant clinical beneits,
may be cost-effective.
(103-107)(Level of evidence: 1)
What should therapy for eradicating B.
cepacia complex strains be like?
The
B. cepacia
complex consists of a group of more
than 80 closely related species,
(108,109)B. multivorans
and
B. cenocepacia
being the predominant species
infecting people with cystic ibrosis.
(110)Clinical manifestations in cystic ibrosis range from
no symptoms to severe conditions with rapid clinical
deterioration and fulminant progression to necrotizing
pneumonia, respiratory failure, and sepsis (cepacia
syndrome).
(110)Treatment of
B. cepacia
complex
is dificult because of intrinsic resistance of these
organisms to most antimicrobial agents available. It
is therefore recommended that, whenever possible,
antibiogram-guided combination therapy be used.
There is no available evidence assessing the eficacy
of its eradication, nor are there recommendations for
inhalation therapy for chronic infection.
(110,111)(Level of evidence: 4)
What should therapy for eradicating
methicillin-resistant S. aureus be like?
Chronic infection with methicillin-resistant
S. aureus
is associated with worse clinical outcomes in patients
with cystic ibrosis.
(112)There have been reports of
methicillin-resistant
S. aureus
eradication therapies
using combinations of oral, topical, and inhaled drugs,
such as sulfamethoxazole/trimethoprim, rifampin, fusidic
acid, and chlorhexidine, in addition to vancomycin.
Linezolid may be considered, but on the basis of less
evidence.
(113)Shorter treatment protocols (< 3 weeks)
appear to be as effective as longer ones, as well as
being less likely to result in intolerance and adverse
effects. Combination therapy appears to have a greater
likelihood of success than does monotherapy.
(114,115)There is still no clear evidence of the beneits of
eradication of methicillin-resistant
S. aureus
in patients
with cystic ibrosis.
(113,114,116)There is also no evidence
to recommend inhaled antibiotic therapy for chronic
infection with this pathogen.
(Level of evidence: 4)
What are the recommendations for chronic
use of inhaled antibiotics in cystic ibrosis?
Table 2 shows the inhaled antibiotics that are
used for suppression of chronic infection with
P.
aeruginosa.
(23,117,118)The regular use of inhaled antibiotics
delays deterioration of pulmonary function in patients
chronically infected with
P. aeruginosa.
(23,87,117-119)Chart
4 presents the Leeds criteria, which classify respiratory
infection with
P. aeruginosa
in patients with cystic
ibrosis on the basis of respiratory secretion culture
results obtained in the last 12 months.
(120)other options.
(23,87,123,124)Tobramycin inhalation powder
has been used and shown to have equivalent eficacy
to tobramycin inhalation solution, being associated
with reduced treatment administration time and not
requiring the use of nebulizers.
(125)The recommendation of using suppression therapy
in alternating months is aimed at preventing the
development of bacterial resistance. In cases that are
more severe, however, continued use of therapy or
switching antimicrobial agents may be recommended.
(124)It is advisable that the irst inhalations be performed
under supervision to allow for assessment of occurrence
of drug-induced bronchoconstriction (wheezing,
dyspnea, and chest tightness). Bronchodilator use
is recommended, followed by bronchial hygiene via
chest physiotherapy and, inally, antibiotic use in order
to ensure greater medication deposition.
(87,119,126,127)(Level of evidence: 1)
What are the indications for the use of
azithromycin in patients with cystic ibrosis
and how should azithromycin be used?
The use of oral azithromycin 3 times a week in cystic
ibrosis patients over 5 years of age who are chronically
colonized with
P. aeruginosa
results in improvement
in pulmonary function and reduction in the number
of exacerbations.
(119,127-133)(Level of evidence: 1)
In patients who were not colonized with
P. aeruginosa
and had an FEV
1> 50% of the predicted value,
azithromycin was found to reduce exacerbations by
50%, although with no improvement in pulmonary
function.
(134)(Level of evidence: 1)
The continued use of azithromycin is recommended,
despite the lack of long-term assessment studies.
Initial use for at least 6 months is suggested for
assessment of response to therapy.
(135,136)Side effects,
such as epigastric pain, electrocardiographic changes,
ototoxicity, and nontuberculous mycobacterial infection,
should be monitored.
(Level of evidence: 1)
The use of azithromycin (250 mg for body weight <
40 kg and 500 mg for body weight > 40 kg; 3 times a
week) is recommended in patients chronically colonized
with
P. aeruginosa
who are over 5 years of age, as well
as in those who are not colonized with
P. aeruginosa
and have frequent pulmonary exacerbations. Sputum
sample collection for investigation of the presence of
nontuberculous mycobacteria is recommended before
initiation of azithromycin.
(132,134)(Level of evidence: 2)
Given the possibility of a drug interaction between
azithromycin and aminoglycosides, combined
azithromycin and inhaled tobramycin use should
be reassessed especially in patients with frequent
exacerbations despite optimal treatment.
(137)(Level of evidence: 3)
How does one recognize an acute pulmonary
exacerbation?
Acute pulmonary exacerbations are characterized
by clinical indings of increased cough, changes in
secretion appearance, fever, abnormalities on pulmonary
auscultation, decreased FEV
1, decreased saturation,
radiological abnormalities, and weight loss.
(23)(Level of evidence: 5)
What therapy is indicated for acute
pulmonary exacerbations?
For mild exacerbations (without hypoxemia or
signiicant respiratory distress), use oral antimicrobial
Chart 4. Leeds criteria for the classiication of respiratory infection by Pseudomonas aeruginosa in patients with cystic ibrosis.Classification
Definition
Chronic infection
> 50% positive Pa culture results in the last 12 months
intermittent infection
≤ 50% positive Pa culture results in the last 12 months
Cured of Pa infection
Previous positive Pa culture results; only negative PA culture results in the last 12 months
Never infected
All of Pa culture results have always been negative
Pa: Pseudomonas aeruginosa. Adapted from Lee et al.(120)
Table 2. Treatment with inhaled antibiotics in accordance with a European consensus.(118)
Inhaled antibiotic
Dose
aTrade name
Aztreonam
75 mg (3 times/day)
Cayston
Colistimethate sodium*
< 2 years of age: 0.5 million IU
2-10 years of age: 1 million IU
> 10 years of age: 2 million IU
Colistin/Colomycin/Promixin
Colistimethate sodium
b(dry powder inhaler)
1 capsule
Colobreathe
Tobramycin
> 6 years of age: 300 mg
Bramitob/Tobi
Tobramycin (dry powder inhaler)
> 6 years of age: 112 mg
(4 capsules of 28 mg)
Zoteon
agents, on the basis of the last respiratory secretion
culture result. For severe exacerbations or in cases of
intolerance to oral medications, intravenous therapy
(usually in hospital) is recommended,
(139)but the
choice of medications depends on previous respiratory
secretion culture results and on patient history.
(23)Antibiotic pharmacokinetics is different in individuals
with cystic ibrosis, and dosage regimens should
be adjusted
(139)(Table 3). For
P. aeruginosa
, the
combination of two or more antibiotics (usually a
beta-lactam and an aminoglycoside) is recommended.
Treatment time for an acute pulmonary exacerbation
depends on clinical response, with the recommendation
being 8 to 14 days. Patients with more severe disease
may beneit from longer antimicrobial therapy.
(138,140-142)In addition to antibiotic therapy, the treatment
of exacerbations requires the participation of a
multidisciplinary team, because there is often need for
oxygen supplementation, use of long-term intravenous
devices, intensiied chest physiotherapy, and a different
nutritional approach.
(138,143,144)(Level of evidence: 5)
How does one assess response to treatment?
One should observe clinical parameters, such as
respiratory symptoms, fever, and weight gain, as well
as improvement in pulmonary function with a view to
it returning to its baseline levels. Despite intensive
treatment, approximately 25% of the patients who have
an acute pulmonary exacerbation requiring intravenous
therapy fail to recover completely to pre-exacerbation
levels of pulmonary function,
(23,138-142)emphasizing
the need for maintenance therapies to prevent acute
pulmonary exacerbations.
(Level of evidence: 5)
When and how should oxygen therapy be
used in patients with cystic ibrosis?
In hypoxemic patients, continuous oxygen
supplementation is associated with increased exercise
tolerance and mild improvement in sleep and school/
work attendance, but does not result in increased
survival.
Table 3. Antimicrobial agents commonly used against acute pulmonary exacerbations in cystic ibrosis patients.a