rev bras ortop.2015;50(2):164–167
w w w . r b o . o r g . b r
Original
Article
Anatomical
reference
point
for
harvesting
a
flexor
graft
during
arthroscopic
reconstruction
of
the
anterior
cruciate
ligament
夽
Clécio
de
Lima
Lopes
∗,
Gabriel
Arantes,
Rodrigo
Victor
Lapenda
de
Oliveira,
Dilamar
Moreira
Pinto,
Marcelo
Carvalho
Krause
Gonc¸alves,
Romeu
Carvalho
Krause
Gonc¸alves
InstitutodeTraumatologiaeOrtopediaRomeuKrause,Recife,PE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5February2014 Accepted13March2014
Availableonline28February2015
Keywords:
Anteriorcruciateligament Tendons/anatomyandhistology Tendons/transplantation
a
b
s
t
r
a
c
t
Objectives:Toevaluatetheprevalenceofavascularnetworkadjacenttotheinsertionof thepesanserinus,sothatitcouldbeusedasananatomicalreferencepointtofacilitate harvestingflexorgraftsforarthroscopicreconstructionoftheanteriorcruciateligament (ACL).
Methods:ThirtypatientswithACLtearswhoweregoingtoundergoACLreconstructionusing thetendonsofthesemitendinosusandgracilismusclesasgraftswereselectedrandomly. Duringtheharvestingofthesetendons,thepresenceorabsenceofthisanatomicalreference pointwasnoted.
Results:Allthepatientspresentedavascularnetworkofgreaterorlesserdiameter.
Conclusion:Thevascularnetworkseemstobeagoodreferencepointduringharvestingof thetendonsofthesemitendinosusandgracilismuscles,forfacilitatinggraftharvesting.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Referência
anatômica
para
retirada
de
enxerto
de
flexores
na
reconstruc¸ão
artroscópica
do
ligamento
cruzado
anterior
Palavras-chave:
Ligamentocruzadoanterior Tendões/anatomiaehistologia Tendões/transplante
r
e
s
u
m
o
Objetivos:Avaliaraprevalênciadatramavascularadjacenteàinserc¸ãodapatadeganso, paraquepossaserusadacomoreferênciaanatômicaparafacilitararetiradadeenxertodos flexoresnareconstruc¸ãoartroscópicadoligamentocruzadoanterior(LCA).
Métodos:Foramselecionadosdeformaaleatória30pacientescomroturadoLCA,osquais foramsubmetidosàreconstruc¸ãodoLCAtendocomoenxertoostendõesdosemitendíneo
夽
Workdeveloped attheOrthopedicsandTraumatology Service,Institutode TraumatologiaeOrtopediaRomeuKrause,Hospital Esperanc¸a,RedeD’Or,Recife,PE,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](C.L.Lopes).
http://dx.doi.org/10.1016/j.rboe.2015.02.010
rev bras ortop.2015;50(2):164–167
165
(ST)egrácil(G).DurantearetiradadostendõesdoSTeG,foiobservadaapresenc¸aou ausênciadareferênciaanatômica.
Resultados: Todosospacientesapresentaramtramavascularemmenoroumaiordiâmetro.
Conclusão: OusodatramavascularduranteretiradadostendõesdoSTeGpareceseruma boareferênciaanatômicaparafacilitararetiradadoenxerto.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Arthroscopicreconstructionsurgeryontheanteriorcruciate ligament(ACL)hasbecomeoneofthecommonestprocedures withinorthopedicstoday.
Oneofthestepswithinthisprocedureconsistsof choos-ingthegraft.Thesemitendinosusandgracilisflexortendons (STandG)havebecomeaverycommongraftoptionusedin reconstructingtheACL.Incomparisonwithgraftsfromthe patellartendon,useoftheSTandGenableharvestingwith asmall incision andcause less pain atthedonor siteand lessdysfunctionoftheextensormechanism,butwithsimilar long-termclinicalresults.1
Useofautologousgrafts from the STand G,in relation toheterologousgrafts,presentsthefollowingbenefits:lower riskoffailure, absence ofrisk ofdisease transmissionand rapidincorporationofthegraft.Ontheotherhand, harvest-ing ofthis typeofgraft hassome potentialcomplications, suchas:difficulty inappropriatelyidentifying thetendons; nerveinjury;dehiscenceofthewound;amputationofthegraft andinadequatelength;andcosmeticallydisagreeableanterior scarontheknee.2
Theaimofthepresent studywastoevaluatethe preva-lenceofvasculartraumaadjacenttotheinsertionofthepes anserinus(PA),inordertouse thisasananatomical refer-encepointandtofacilitategraftharvestingfromtheflexors inarthroscopicreconstructionoftheACL.
Materials
and
methods
Thirty patients with ACL injuries were selected non-probabilisticallyandconsecutively.Thefollowingweretaken asinclusion criteriafor this study: the patients needed to presentACLinjurieswithoutassociatedinjuries(except possi-blymeniscalinjuries);therewerenoagerestrictions,andthe meanagewas30.7years(range:16–52);therewereno restric-tionsonsex,andtherewere23men(76.67%)andsevenwomen (23.33%);andtherewerenorestrictionsonside,andtherewere 21injuries(70%)intherightkneeandnine(30%)intheleft knee.Patientswhopresentedassociatedinjuriesor anatomi-caldeformitiesorprevioussurgeryinthekneeaffectedwere excludedfromthestudy.
Allthepatientswereoperatedbythekneesurgerygroupof theRomeuKrauseInstituteofTraumatologyandOrthopedics, betweenJanuaryandDecember2013.
Thisproject was approvedbythe Institution’s Research Ethics Committee,inaccordance withResolution 196/96of
theNationalHealthCouncil(GuidelinesandRulesRegulating ResearchInvolvingHumanBeings).Eachpatientwasinformed abouttheaimsofthestudyandwasaskedtosignafreeand informedconsentstatement.Ifthepatientwasconsideredto beincapableofdoingthis,acloserelativewasaskedtodoit.
Anatomical
considerations
The pes anserinus is the common insertion point, on the anteromedialfaceofthetibia,ofthetendonsofthe semitendi-nosus,gracilisandsartoriusmuscles.3
Thetendonsusedasgraftswerethesemitendinosusand gracilis. Althoughthese are separatestructuresproximally, they convergetowardstheir anterior insertionin thetibia. Theinsertionofthegracilisisabovethatofthe semitendi-nosus. The pes anserinus is located around 19mm (mean value, between10 and25mm)distallyand 22.5mm (mean value, between13 and30mm)mediallytothe apex ofthe anteriortuberosityofthetibia.4
Theinsertionofthepesanserinusissurroundedbya vas-culararchforwhichthebloodsupplycomesfromthethree mainarteriesoftheknee:(1)medialinferiorgenicularartery (superficialanddeepbranches);(2)lateralinferiorgenicular artery;and(3)anteriortibialrecurrentartery5(Fig.1).
Surgical
technique
AllthepatientsoperatedarthroscopicallyforACL reconstruc-tionusingSTandGgraftsunderwentemptyingofthelimb bymeansofelevationandischemiausinganEsmarchband andpneumatictourniquetatapressureof300mmHg, inde-pendent ofthe diameter ofthe thighor the mean arterial pressure.
Inallcases,thevascularnetworkoftheinsertionofthepes anserinuswasidentifiedandusedasareferencepointfor har-vestingthegraft,inaccordancewiththetechniquedescribed above.
ToharvestthegraftfromtheSTandG,ananteromedial accessofaround2cmwasmadeinthetibia,starting2cm dis-tallyand2cmmediallytotheapexoftheanteriortuberosity ofthetibia.
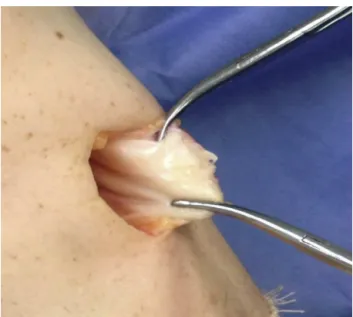
Aftersectioningtheskinandsubcutaneoustissue,the vas-culararchadjacenttotheinsertionofthepesanserinuswas identified(Fig.2).
166
rev bras ortop.2015;50(2):164–167Fig.1–Anatomicalspecimenfromthekneeofafresh
cadaverinwhichthefemoralarterywascatheterizedand
receivedadministrationofagelatinoussolutionofIndia
ink,whichshowedthevasculararchthatsurroundsthe
insertionofthepesanserinus.Arrowsshowthetributaries
ofthevasculararch:(1)medialinferiorgenicularartery
(superficialanddeepbranches);(2)lateralinferiorgenicular
artery;(3)anteriortibialrecurrentartery.5
noted(Fig.4).TheSTandGtendonswerethenidentifiedand distinguished(Fig.5).
Results
Outofthe30patientswhounderwenttheprocedureof arthro-scopicreconstructionoftheACLinvolvinguseofthetendons
Fig.2–Presenceofthevasculararchadjacenttothe
insertionofthepesanserinus.
Fig.3–Incisioninthepesanserinus,whichfollowsthe
pathofthevasculararch.
oftheflexormuscles(STand G),all ofthempresentedthe vasculararchwithagreaterorsmallerdiameter.
Discussion
Theproceduresforligamentreconstructionarewell dissemi-natedwithinorthopedics,andparticularlythoseoftheknee. ToreconstructtheACL,surgeonshavearangeofpossibilities forchoosingthegraft.Theseincludeallografts,forthosewho haveaccesstotissuebanks;graftsfromthequadricepsand patellartendons;and,overthelastfewyears,graftsfromthe semitendinosusandgracilistendons.
InparallelwithuseoftheSTandGtendons,various com-plications relating to their harvesting have arisen.Among these, thefollowingcan behighlighted:injurytothe tibial
rev bras ortop.2015;50(2):164–167
167
Fig.5–Identificationofthesemitendinosusandgracilis
tendons.
collateral ligament; erroneous harvesting of the sartorius muscle;prolongeddurationoftheoperationduetodifficulty inisolatingandextractingtheSTandGtendons6;injuryto theinfrapatellarbranchofthesaphenousnerve7; andeven healingproblemsattheincisionthatismadeforharvesting thegrafts.8
Thesecomplicationscanbeexplainedpartlybythelack ofreports in the literature,particularly with regard to the techniquesforgraftharvesting,fromananatomicalreference pointthatwouldguideandfacilitatetheirharvesting.
Inthepresentstudy,theprevalenceofavascularnetwork intheformofanarch,adjacenttotheinsertionofthepes anserinus,wasanalyzed.A100%associationbetweenthis vas-culararchandtheareaofincisionforgraftharvestingwas seen,whichfavoredeasierharvestingwithoutcomplications, inaccordancewiththetechniquedescribedhere.
Conclusion
Giventheprevalenceandeaseofidentificationofthevascular network of the pes anserinus, this is a useful and repro-ducibleanatomicalreferencepointforharvestinggraftsfrom thesemitendinosusandgracilistendons.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.CharalambousCP,KwaeesTA.Anatomicalconsiderationsin hamstringtendonharvestingforanteriorcruciateligament reconstruction.MusclesLigamentsTendonsJ.2013;2(4): 253–7.
2.WilsonTJ,LubowitzJH.Minimallyinvasiveposterior hamstringharvest.ArthroscTech.2013;2(3):e299–301.
3.MochizukiT,AkitaK,MunetanT,SatoT.Pesanserinus:layered supportivestructureonthemedialsideoftheknee.ClinAnat. 2004;17(1):50–4.
4.PagnaniMJ,WarnerJJ,O’BrienSJ,WarrenRF.Anatomic considerationsinharvestingthesemitendinosusandgracilis tendonsandatechniqueofharvest.AmJSportsMed. 1993;21(4):565–71.
5.ZaffagniniS,GolanòP,FarinasO,DepasqualeV,StrocchiR, CortecchiaS,etal.Vascularityandneuroreceptorsofthe pesanserinus:anatomicstudy.ClinAnat.2003;16(1):19–24.
6.OliveiraVM,AiharaT,CuryRP,AvakianR,DuarteJúniorA, CamargoOP,etal.Estudoanatômicodainserc¸ãodosmúsculos grácilesemitendíneo.ActaOrtopBras.2006;14(1):7–10.
7.LuoH,YuJK,AoYF,YuCL,PengLB,LinCY,etal.Relationship betweendifferentskinincisionsandtheinjuryofthe infrapatellarbranchofthesaphenousnerveduringanterior cruciateligamentreconstruction.ChinMedJ(Engl). 2007;120(13):1127–30.