Y
Histories of Medicine and Healing in the Indian Ocean'Vlorld: The Medieualand Early Modern Period, Volume One
Edited By Anna'ùØinterbottom and Facil Tesfaye
Histories of Medicine and Healing in tbe
lndian
Ocean'World: The Modern Period, Volume TwoEdited By Anna V/interborrom and Facil Tesfaye
Histories
of
Medicine and
Healing in
the
lndian
Ocean
World
The Modern
Period
Volume Two
Edited by
Ann o
Winterbottom ond
Focil Tesfoye
palgrave
macmilLan
#
HISÏORIES OF MEÞICINE AND HEALINC IN THE IND¡AN OCEAN WORTDSelection and editoriaI content @ Anna W¡nterbottom and Facit Tesfaye 2016
lndividuaI chapters @ their respect¡ve contr¡butors 201 6
Atl rights reserved. No reproduction, copy or transmission of this
publication may be made without wr¡tten permission. No portion of this publication may be reproduced, copied or transm¡tted savé with written
permission. ln accordance with the provisions of the Copyright, Designs
and Patents Act 1988, or under the terms of any licence permitting ümited
copying issued by the Copyright Licensing Agency, Saffron House, 6-l O
Kirby Street, London EClN 8TS.
Any personwho does any unauthorized act in relation to this pubtication
may be liable to criminal prosecution and civi[ claims for damages.
First published 2016by
PALCRAVE MACMILLAN
The authors have asserted their rights to be identified as the authors of this
work in accordance with the Copyright, Designs and patents Act 1 9Bg.
Patgrave Macmillan in the UK is an imprint of Macmil[an publishers
Limited, registered in England, company number 785998, of Houndmitts,
Bas¡ngstoke, Hampshire, RC21 6XS.
Palgrave Macmillan in the US is a divisíon of NatureAmerica, lnc., One
NewYork Plaza, Suite 4500, NewYork, Ny 1OOO4-1562.
Palgrave Macmillan is the global academic imprint of the above companies
and has companies and representatives throughout the world.
Hardback ISBN: 978- 1-1 3 7-567 61-1
E-PUB ISBN: 978-1-1 37-56759-8
E-PDF ISBN: 978-1-1 37-56758-1
DOI: 10.1 os7 I 978 1 1 3 7567s8 1
Distribution in the UK, Europe and the rest of the wortd is by palgrave
Macmillano, a division of Macmillan publishers Limited, registered in
Ëngland, company number 785998, of Houndmitts, Basingstoke,
Hampshire Rc21 6XS.
Library of Congress Cataloging-in-publication Data
Winterbottom, Anna,
1979-Histories of medicine and healing in the lndian Ocean wortd / Anna
Winterbottom and FaciI Tesf aye.
v.olumes cm.-(Palgrave series in lndian Ocean world studies) lncludes bibliographicaI references and index.
Contents: volume 1. The medieval and early modern period
-volume 2.The modern period
ISBN 978-1-1 37-567 61-1 (hardback : atk. paper)
1. Medicine-lndian Ocean Region-History. 2. Medicine-lndian
Ocean Region. 3. Medicine, Medieval-lndian Ocean Region. 4. Traditionat
medicine-lndian Ocean Region-History. 5.TraditionaI
medicine-lndian Ocean Region.6. Healing-lndian Ocean Region. Z. lndian Ocean
Region-History. L Tesfaye, Facil. ll. Title. R605.W46 2015
615.8'8091824-dc23
2015018001A catalogue record of the book is available from the British Library.
These volumes
ore
dedicotedto
medicol workersoround
the worldList of lllustrations
Acknowledgments
1
Making Medical
ldeologies: IndenturedLabor
inMauritius
Yoshinø
Hurgobin
2
Treating Black Deathsin
Egypt: Clot-Bey,African
Slaves, and the Plague Epidemicof
1834-1835
George Micbael La Rue
3
Rockefeller PublicHealth in Colonial
India ShirishN.
Kauadi4
Colonial
Madness:Community
and Lunacyin
Nineteenth-Century
India
Anouska Bhattacharyya
5
RussianMedical Diplomacy
in
Ethiopia,
1.896-1913 RashedChowdhury
6
Tropical
Disease and theMaking
of
Francein
Réunion Karine Aasgaard Jansen7
Medicine on the Edge: Luso-Asian Encountersin
the Islandof
Chiloane, SofalaCristiana Bastos and
Ana
Cristinø RoqueI
Zigua
Medicine, betweenMountains
and Ocean: People, Performances, and Objectsin
HealingMotion
Jonathan R. Wølz
9
Indian
Ocean'Worlds: Tracing SouthAfrican
"Indigenous
Medicine"
lulie
LaplanteContents
27 6T 89 115 147 1,7't 1,97 1Xxi
'1. 21,9viii
Contents Concluding Rernarks MichaelN.
PearsonBibliography
Contributors
lndex
24s 255 275)77
lllustrations
Figures
1.72 175 1,787.1.
Indian
Ocean map showing Chiloane, Goa, and Macau7.2
Medical
Schoolof
Goa7.3
TheHarbor
and Islandsof
Chiloane(
rrcT-cDI-
0 4 83-1.9 s2)7.4
Excerptfrom
the registrybook of
theplant
samples collected by Ezequiel da Silva
(1883)'
IICT,
AHU,
Códice-SEMU -21, I 67.5
Gynandropsis gynandrag.L
Rastafarian sakmanne photographed duringour visit
of
the medicinal
plant
garden,part of
the Indigenous Knowledge Lead(Health)
Programof
South Africa'sMedical
ResearchCouncii
at theDelft laboratory
facility
in November 2007 1.84 186 35 39 185 234Tables
34 2.1 2.2 L.J 7,7Plague
mortality
inAlexandria,
Egypt,in
the epidemicof
1834-1835
Mortality
rates inAlexandria,
Egypt,in
the plagueepidemic
of
1834-1835
Plague deaths
in
Cairo
in
1835, byethnicityinationality
7
Medicine on
the
Edge:
Luso-Asian
Encounters
in
the
lsland
of
Chiloane,
Sofala
Cristiona Bostos ond Ana Cristino Roque
lntroduction
In this
chapter we
addresscolonial
perceptions
of African botanical
knowledge and healing practices
as expressedin
the
writings of two
different social actors, both
connected
with
the
Portuguese empire
in
the Indian
Ocean,
both
living in
the island
of
Chiloane
(Sofala,
Mozambique)
in
the
1870s:
Arthur
Ignacio da Gama,
a
graduate
of
the
Medical School
of
Goa (India) placed
in
Sofala
in
1,876;and
Ezequiel
da Silva, a third-generâtion
Portuguese
local
teacherwhose ancestors
had
first
movecl
from
Portugal
to
Macau
(China)
and
from
there
to
Mozarnbique.
lØe analyze
their
writings
within
the context
of the shifting
European
imperial politics in Africa
and
within
a large-scalecirculation of
people, things,
elementsof
knowl-edge,
practices, and
experiences acrossthe
Indian
Ocean.They stand
for
distinct
styles
of
circulation through the Indian
Ocean:
Arthur
Ignacio da
Gama
was part
of
a
flow
of
Goan skilled
professionals
who
sought
work
outside Goa and
saw themselves aspart of
aproj-ect
of civilizing
the
world
using moclern standards, European
medi-cine among them; Ezequiel da Silva
belonged
to
the more mobile
group
of
Indian-Ocean-born
Eurodescendants
who
lived close to
local populations
ancl usedlocal knowledge
for
practical
purposes,
I
177
Cristiana Bastos and Ana Cristina RoqueGoan
Physicians
and
Empire
Between
1842
and1961,
hundredsof
young
menand
arnuch
smallernumber
of
women studied
rneclicine,surgery,
or
pharmacy
in
theMedical School
of
Goa.
After
graduation, many
of
them
served in
the
Portuguesecolonial health
servicesin Asia
and
Africa,
in
placeslike
Macau,
in
China, the
easternsection
of
the island
of Timor
nearAustralia, the
CapeVerde islands
in
the
mid Atlantic,
the
SØestAfrica
coast
of
Guinea, or,
in
larger
numlrers,
Angola and
Mozambique
(Figure 7.1 ). Regardless
of what
might
have been thepersonal
motiva-tion
behind
eachof
theindividual
trajectories,
thecollective
endeavorof
Goar-r physicians inAfrica
during
the nineteenthcentury
would
later
be celebrated as a
pillar of
the Portuguese empire.In oral
lore,
in
¡rub-lic
ceremonies,or in print,
Goan doctors were depicted
as thosewho
had
beenout
therewhere
no
one elsewanted
to
be,risking their
livesfor
the
safetyof
the troops
and
for
the noble mission
of treating
theindigenous populations. Rather than products
of
empire, Goan
physi-cians were
presenteclâs
agentsof
empire-building.
Suchviews
weresoiemnly
expressedat the
centennial anniversary celebrations
of
themedical school
in
1942.1Yledicine on
the
Edge
173Given the
political
armosphereof the
1940s,it
isnot surprising
that
the government-appointed directors
of
the school
choseto
cheer, cel-ebrate,and befriend the
Portugueseadminjstration,
prescnt and
past,rather
than criticize it. Indian
nationalism was at its peak, the
British
rule
in the
subcontinent was near
the
end, and Goa was
thcn-after
having
been neglectedto
quasi-irrelevance
through
theeighteenth
andnineteenth
centuries-under
pressure
to
take
advantage
of
its
con-nections
to
Portugal and
keep
away
from
the surrounding
upheav-als.
lØhen India
becamea new nation,
in
1947, Goa
remained
oneodd
"Portuguesepirnple on the
faceof Mother India,"
asin
the
quoteattributecl to Nehru.
Neither diplomac¡ nor
thenationalist
struggleof
the satyagrahas
through the
1950s,or international
pressure, changedthe
stubborn position
of
Salazar's
Portugal;
the annexation
to
theIndian Union
occurred
only in
1,961,, after adisplay
of military
power
followed by
peaceful surrender.
In
1987, Goa
becamea
state
of
theIndian
Union,
after
a
referendum
(the 1967 Opinion Poll)
in
which
Goans showed
their
preferencefor
remaining
asmall
staterather than
merging
with
Maharashtra.2
Back
in
the
1940s,
Goa was
ât
the
crossroads
of
major
changesin
world politics. The
Portugueseadministration
insisted
on
follow-ing
anidiosyncratic path
againstdecolonization
and presentedempire
as an
imagined transcontinental
community in which different
identi-ties
happily
combined
with
one
another
and merged
in
a
single
des-tiny.
Goa was assigned aprominent
role
in that
imagined community.
Goa
wasthe
evidencethat
Westand
Eastcould
meet.Goa
evoked the golden ageof
sea trade, great churches, and heroes like Vasco da Gama and FrancisXavier. Lusotropicalism,
theideological
cementfabricated
in the
1950s and adopted
in the
1960s
by
the
Portuguesejust at
themoment
when the
European empires were collapsing
for
good,
wasyet
to
be available
with
its repertory
of
friendly colonialism and of
Portuguese
easywâys
in
the
tropics.3
In
the
L940s,
the rhetoric of
empire was
still
about
conquest, precedence,braver¡
and thecivilizing
mission. Those were also
the
key
words
in
the
speechesmade
at
thecentennial
of
themedical
school.It
is
not
clear whether
those
who
actually
served
in
the African
health
serviceswere imbued
with
the
senseof
mission
that
was later
attached
to
their
trajectories.
Did
they
chooseserving
in
Africa
andcaring
for
theAfrican
bodies and
souls,or
was
their route
more
of
a contingency?Did
they take sideswith
the Portuguese and feelthat they
were treated
like
equalsin
a sharedmission of
civilizing
by colonizing,
or
were they treated
ascolonial
subjectsand kept
in
secondary roles?On other
occasions, we have addressed theambiguities
experienced byllJI?1-{Ìt 'rt,iiÀl!
. .,-.-f '','"'!. ì'-:
174
Cristiana Bastos and Ana Cristina RoqueGoan
doctors in
Africa.
In this
chapter we readfurther into
thewriting
of
one
of
those doctors,
Arthur Ignacio da
Gama, and compare him
with
hiscontemporary
Ezequiel da Silva.Both
menlived
in
the
islandof
Chiloane
(Sofala)during
the
1870s.4Arthur
Gama:
A
Christian
Brahmin
from
the Goa
Medical School
Arthur Ignacio da
Gama
was born
in
1851 inVerna,
Salcete,into
afamily
of
Christian
Brahmins.
He
attended medical school
in
nearbyPanjim and
graduated
in
1875.5Although we do not know
enoughabout his childhood and
teenageyears
to
assertwh¡
when, and
if
he
wanted
to
become adoctor, we
know that
it
was
achoice
of
elec-tion
among
the
social
group
with
the peculiar
referenceof
Christian
Brahmins, about
whom
somecomment should
be made.Christianized
since
the sixteenth
century,
when
pressured
by
thePortuguese
to
convert
or
otherwise
leavetheir
land-which
somepre-ferred
to
do, and fled
to
the neighboring counties6-many
families
had adopted
the
language,religion, clothing,
architecture, and
tastesof
the Portuguese,while
keepingrelatively intact
their
role
in
thelocal
social
hierarchies.
Christian Brahmins
represented
the upper
crust
of
the accommodation
between
the
European
wâys
and the
caste-evoking
traditional
social hierarchy.
Highly influential in
the Catholic
Church, Brahmins
competed
with
the
Chardo, another prominent,
caste-evoking
group
that wâs influential
in
other
spheres,and with
the small rninority
of
Luso-descendants,who claimed direct
lineagefrom the ruling
Portugueseand
receivedthe highest privileges
in
theadministration.T
Some
Christian Brahmins had long
beenfamiliar
with
medicine,by learning
from their
elders,
from
assisting Portuguese
physiciansand
surgeons
in
the
military
or
religious hospitals,
or
yia
one-on-one
transmission
of
knowledge
by
the
headphysician
in
charge. Theinstitutionalizatíon
of
the
Medical School
of
Goa-which
should
be
credited
to
this group, who provided
the
majority
of
the
student
body-should
be seen as one stepin this
process,râther than
aninitia-tive of
the Portugueseadministration.s Partly
acontinuation of
along
process,
and
partly
arupture with
the pastand
anâttempt
to
endorseEuropean
modernit¡
the
school
allowed no
compromise
with
tradi-tional
medicines(Figure 7.2).Wh,atever
might
have been the students'previous
knowledge
of
local
healing
traditions, they were
supposedto
leayeit
outside the
walls
of
the Maquineses palace, where,
in
theA ¡oss¿ Frcol¡, nåo é o ûiste êdif¡cio plôntôdo i mårgem do M¿ndov,. Náo !åÕ ås iuås divi5ó65 intårnas æbret e monóton¿r, que o c€racterizam E à ruð evÕluçáo lenlð ðås progrêsiva j é a voz dor seus profelrores vieos ou.noilo, que nela tr¿ba
lh¡rôð! trabålh¡m ôihdåt é o ê€o de¡sa¡ vozes que ¡a'ndo de um obscuro cantrnho roam pelo mundo r¡lairo. Ê estê o facho iuminoso que ma¡cå a 5ua existêñc¡ð d! rane ete longo periodo êo meio de de¡rocada dås ånt€as conqu,stås ¿firn,êndo ainda c bendirendo a glóriâ dG uñt îsçåopeq!€ns no seu territónô ós! grande na sðlvé, Escola Médicâ d€ Goa, måe carinhosa qus ¿mbàla¡tos nor vossor braços 6morosor l¿ntor filhor que na ruô pótrið € n¿¡ duar Áft'øs deram o melhor rJo çeu
*forço parr .mpôrô. ¡ vidå d6 tantot pionêios då c¡vrh¡åçåo.
Nirguém * leñbra hoþ dos obscuros ioldados. mâs irso pou€o impotð S€n
ti.d às ondôi ftg¡dorô: do ódro o malquerenga mas falará mais alto seu verd¿de'ro
dorøimento. O facho de glório da Ê¡cola Médica. nåo ôstó nst måos deste nem daqæle ; somo:todos nó¡ os cor¡e<Jores do lucano. alumiando o caminho dc pôssado do pr€sntea dô futuro, .m obo út¡l ê proveito3a À huúùôidad€. Somo: como ¿s
abelhar quo na colmeia fab¡icm em sílêncio o mê|, e nenhuma se arroga o drrerto ¡ p.im¡¡,¡ ¡o tæb¡lho. A glória da Escola MËrtis de Go¡ é ¿ glória dã N¿çáo nelte reñolo O¡ie¡tâ. Ê' o eco do parsado æomodado às atrcuñlànci¿i prè5entes no
ooinho do pÞgc$o.
Eodt¡ ¿ nos¡¡ Ëscoia Médic¡ n¡ ¡ua snb ctu!ôdå I
Woli-ñao d¡ Etlv¡
( Dd Àlocdç¡d profdidâ t{lo Caotcn{íÒ dù llsóla )
ßigure7,2
Medical School of GoaSource: l. Pacheco and D. E. Figueiredo (7960), Escola Médico-Cirurgica de Goa-Esboço
Hi stórico (Bastorá: Tipografi a Rangel)
annex
of
the
military hospital, facing
the
Mandovi
River, the
schoolhad functioned
sinceits
foundationin1"842. Meanwhile, life went
onbeyond
the
school
walls,
and
headphysicians
reported that
studentsand
graduates
were so
immersed
in
local healing
that
they would
rather
usetraditional
medicines
when sick
and, sometilnes, included
them
in their clinical
practice.e\üe
do
not know if
the young
Arthur
Gamahad much exposure
to
traditional
medicinesbefore
heattended medical school.
Síe doknow
Medicine on
the
Edge
175Iseda llúd¡ro-tirúrgi{iâ ds ütra
176
Cristiana Bastos and Ana Cristina Roquethey
were not
encouraged
in
its
all-European
curriculum,
fashioned
after those
of
the
Medical-Surgical
Schools
of
Lisbon and
Porto,
which
had started
in
1836, offering
âmodern, hands-on
training,
asopposed
to
the
old
scholastic
ways
of
the
legendary
University of
Coimbra.
rühether
Arthur
hadhands-on
training
or
satthrough
amore
scho-lastic type
of
teaching
is
debatable.
There
is
evidence
that
studentsobjectecl
to
using
their
hands
in
generaland
in
dissectionsin
particu-lar; faculty
members condescendingly accommodated
themselvesto
the use
of
anatomical models rather than human
corpses,which,
they
claimed, were
in
shortageat
the hospital.l0 Therefore,
it
is
likely that
Arthur did not
haveto perform
dissections aspârt
of
his
schoolwork
routine.
He attended classes lecturedin
Portuguese byPortuguese-born
professors
or
by Goan doctors trained
in
Portugal;
hetook
his
examsin
Portuguese,after studying
French, Portuguese,or
Englishtextbooks,
and
used supplies shippedfrom
Europe. He
learnedwhat
was
learnedin
Europe, and
cameout
of
school
with
a
degreein
European
medi-cine.
Then
hewent on
to Africa.
From Goa
to
Mozambique
Besides
Africa, what
other options were
therefor
the
graduatesof
theMedical
School
of
Goa?Not
that
many.
Someof Arthur's
classmateswould
never evenprâctice medicine;
anumber
of
them
went into
thepublic administration, something
that
a
college
degree-regardless
of
its discipline-helped
make
possible.ll
Opening
a local clinic
washardly viable;
at
the time,
not
even
the higher-ranking
Portuguese-certified
physicians
stationed
in
India could make their living from
the earnings
of
aprivate prâctice.
Theycomplained
that
there wasnot
enough
local
clientelefor their
services,noting that most
peoplewould
rather
goto
traditional
healers, and theonly
clientsfor
Europeanmed-icine were
thefew
Portuguese residentswho felt entitled to
be treatedfor
freeby
their
compatriots.12Entering
a career as arnilitary
physician was a morelikely option
for
the graduates
of
theMedical
Schoolof
Goa,and many
of
them found
that this path
led them
to
distant
locations
in Asia
and
Africa.
Someof
their routes followed preexisting paths and
connections
through
the
Indian
Oceanand
into
theAtlantic, with
Portugal
as one possibledestination,
but
also
including
Bomba¡ the Gulf, and other parts of
the
world
asviable
placesto
settle, serve,come back
from,
and
even-tually go back
to, in
one
or
another's generation.
Thesetrajectories
followed broadly
the routes framed by
EngsengHo for
the
centuries-Yledicine on
the
Edge
177old
spreadof Muslim families throughout the Indian
Ocean,
aswell
as those
recently depicted
in
detail by Pamila Gupta,
SelmaCarvalho,
and
Stella Mascarenhas-Keyes
for
Goan
diasporas
in
Mozambique,
the
Gulf,
and East Africa.13Among
the many routes
acrossthe Indian
Ocean,the
path
to
thecoast
of Mozambique had
beenattracting
generations
of
Goans
and otherpopulations from
thenorthwestern
coast ofIndia.la Mozambique
had
beenunder the jurisdiction
of
Goa
until
the
eighteenth century
and many Goan families
extendedtheir trans-Indian
Oceannetworks
into
the
eastern coastof Africa;
when
JoãoJulião
daSilva referred
to
the
district of
Sofala, helisted
Goans asregular
residents.l5Collating
anumber
of different
sourcesfor
the nineteenth century,
we were able
to identify
40
graduatesof
theMedical
Schoolwho
held
official positions
in
the health
servicesin
Mozambique
(seeâppen-dixT.L).Willingly or unwillingly,
they provided
a steadyworkforce
ata
relatively low
cost
for
the
Portuguesegovernment, given
that their
training
had
mostly
beenself-financed and
their
earnings were
mea-ger.
Goan
graduateswere
kept in
secondarypositions and
could only
progress
in
their
careersif
they went
for further training in
Portugal-which most
did
not.
Many
complained
about
what
they
regardedas
an intrinsically
unfair
system
that
made
them eternal
subalterns,regardless
of
their
quality.l6
Adding insult
to
injur¡
some hadto
work
under
Portuguesesupervisors
who
scornedtheir
medical
degrees andlaced
their
comments
with
anti-Asian
prejudice.lTDespite
thesediffi-culties,
the
idea
that
Goans
would provide the ideal workforce for
the
Portuguesehealth
servicesin Africa
was
first
suggestedby
aGoan
doctor; not just
any doctor,
but
Rafael
Antonio
Pereira (1847-1.91.6),a
Benaulim-born
Christian
Brahmin
who
studiedmedicine
in
Portugal
and returned
to
Goa,where
heattained higher positions and directed
the medical
servicesbetween
1884 and 1893.
At
a time when
theschool was under
siegeand the
Portugueseadministration
consideredclosing its
doors, Rafael Pereira developed anargument about
thespe-cial
qualities
of
Goan doctors
for
the
colonial
services:they were
thebest intermediaries between Europeans and
Africans,
knowledgeable
enough
to
bethe carriers
of
civilization,
and accustomed
to tropical
harshness
and
illnesses.lsThe
sameline
of
argument
was later
pre-sentedto
the
Portugueseparliament
in favour of
the
Medical
Schoolof
Goa-with
success.leYet before Goan physicians were
defined
as thedoctors of
empirein
Africa, their
livesin
the
colonial
outposts were
often random
experi-ences
of
disorder and
improvisation
under
harshconditions
andwith
l7B
Cristiana Bastos and Ana Cristina Roqueown, albeit carrying
a senseof
mission,that
Arthur
Gama actedwhen
he
took
hisposition
Chiloane,
in
1.876,at
theyoung
ageoÍ
25, where
he
would
stayuntil
hispremarure
deathin
1882.Into
the
lsland
of
Chiloane
The capital
of
the Sofala District was transferred
from
the
main-land
port
of
Sofala
to
the Island
of
Chiloane, located nine
leaguessouthward,
in
theyear 1860,
owing to
environmental constraints and
political instability that included warfare and retaliation by African
groups.20
Portuguese
sailors had
been
using the island
as
an
alter-native
to
the mainland
port of
Sofala since
the mid-sixteenth
cen-tur¡
but
there was
no political
or military role
assignedto
the
place(Figure
7.3).
Described
in
the
sourcesas
of
"six
leaguesnorth
andsouth, and the
same eâst
and
west,"21it
was either
presented as
apotentially
welcoming location
for
settlers,with
its
deep and shelteredba¡ well
supplied
with
pastures,fish, wood,
andplant
resources,or
asa
barren
desertwith
no
comparison
to
the
fruitful
land
of
the
conti-nent where people had
their
farms. In
the absenceof
anofficial
census,it
is
believedthat until the
1860s the island was
inhabited
seasonallyby fishermen
or
used âs âsort
of
trade station,
for
transshipment
anddistribution of
goods, bylocal
traders.In
1890, there wereabout
threethousand
peoplein
the place,of which
fifty
were classified âs"white"'
Figure
7.3
The Harbor and Islands of Chiloane (IICT-CDI-0483-19521. (courtesyof the Historical Overseas Archive [AHU] and the Tropical Research Institute [IICT],
Lisbon.)
Medicine on
the
Edge
179there were eight
European-descent"children
of
the land," plus
someLuso-Asian families,
while the majority were drawn from the
indig-enous population.22
\lhen
Arthur
Ignacio
da
Gama was appointed
to
Chiloane, in
1876,he
was estrangedby
what
heconsidered its wilderness, and did
not
abstain
from exhibiting
his
impressionsin
theofficial
report.23 Incontrast
with
Ezequiel
da
Silva'sappreciative depictions
of
the
place (seeinfra),
Gama's
writings
were
all
about disillusionment
with
thelocal lack
of
infrastructure, lack
of
civilization, lack
of
perspectives,and lack
of
viability. He
suggestedthat
the
Portuguese
administra-tion
should
not
insist
on colonizing
the
place,which might better
beleft
to
the clouds
of
insectsthat
emanated
from its
swamps.24In
hisopinion,
therewere more
appropriate
environments
for
settlersin
themainland;
hedid not
referto
the reasonswhy
thecapital
hadmoved
to
the island
in
the
first
place.The
Portuguesewould
indeed move back
to
the mainland
in
duetime;
in
1.892,the capital
of
Sofalawâs
trans-ferred
to
Chiveve,renamed
City of
Beira
in
1907,
which would
havea
notorious
future
asMozambique's
secondcity.
Gamawould not
live
to
seethe new
capital:
hedied
in
1882, succumbing
to
the
feversthat
plagued the
island.Ahead
of
Gama
were the many
tasks
assignedto
colonial
physi-cians.
They
had
to
handle
the patients-mostly
soldiers
and
settlers, asthe indigenous
populations
were
reluctant about
receiving medical
care
from
the Portuguese;2sthey
hadto report
to
their
superiors
in
theMinistry of
Navy
themorbidity
andmortality
figures;
andthey
hadto
provide
aninventory
of
the
causesbehind
thehealth conditions
in
theplace, according
to
the
prevailing
beliefs
on the
influence
of
climate
on
human
health.
Apart
from
these duties,
they
also
had
to
act
asnaturalists
and gather
scientific
data,
samples,and
objects;
they
hadto
observe,collect, and
report on
zoological, botanical, and
mineral-ogical matters. They were required
to
send specimens,plants, grains,
seeds,
and whatever objects
might
beof
interest
to
the
museums andscientific
collections
of
the
kingdom-such
as the
Real
Gabinete
deHistória Natural
daAiuda in
Lisbon, the
institution that
later
evolvedinto
theMuseum
of Natural
History.26People
in
theposition
of
Gama were
pressuredto
compile,
amass,and
report, not just
for
the
sake
of
knowledge
as
a goal,
but
alsobecause
knowledge
was a commodity
in
the
inter-European
compe-tition for
the political and
economic
control
of
Africa. Lisbon
wasa
center
of
knowledge compilation,
with
multiple outsourced
datagâtherers,
but
the
whole
endeavor
did not
match up
to the
ambitious
claims held
by Portuguesegovernments
for Africa. Colonial
officers
in
I
IlB0
Cristiana Bastos and Ana Cristina Roquethe
field
wererequired
to
helpfill
the gaps.Explorers
sponsored by theGeographical Society
had the
mandate
to
map river
sources,moun-tains, and
potential
mines.27 Practicing physicians hadto compile local
knowledge
on plants
and
remedies.In
a
booklet clearly
madefor
thepurpose
of
inter-European competition, Joaquim
Almeida
Cunha,
anofficer
of
the colonial administration
in
Mozambique,
gathered
theknowledge on medical plants that had
beencompiled
in
thefirst
placeby
Ezequiel da Silvain
Chiloane.28Arthur
Ignacio da
Gama
did not show
much personal interest
in
the
medical
usesof
local plants.
Hewrote
thereport
using secondhandknowledge,
for,
heclaimed,
hecould
not afford
the
time to
go
out in
the
field to
collect data when
he was needed as adoctor in what
wasoften
alife-and-death
struggle.He
wasneither
eâgerto
survey,collect,
and
report on
the minerals,
flora,
and fauna,
nor to know
the
indig-enous peoples close
enough
to
report their
lifestyles
and ship their
artifâcts into
somedistant
Etrropean destination;
hewas
not
trained
as a
knowledge-collector,
but
as adoctor,
who did not
rrade
his place at thepatient's
bedsidefor
theoutdoors, wandering
for
bits
and piecesthat might,
or might not,
berelevant
for
humankind.2eFor
someonewho
was sononchalant about
datacollecting,
Gama'sdepiction
of
the healing
rituals
practiced by
theindigenous
peoplesof
Chiloane
isimpressive-making it
asort
of
ethnomedical narrative all
too similar
to
those
produced
in
the twentieth
century.
He
depictedthe role
of
the "inhamessoro"
(nyamasoro),
the
people's
quest for
hís
or
her
services,the
sort of afflictions
they
brought
to
the
healers,the worldview they
espoused,the
instruments,
gestures, dress code,sounds, smokes, substances,
and
other material
elementsinvolved in
diagnosis
and treatment.
He
also made anattempt
to attribute
mean-ing to all
thesethings.
His
prejudice, though, was parenr
all through
the
narration.
Gamacould not
helpbut
formally
distancehimself
from
traditional
healing, perhaps as agood
child of
hisalma
mater, perhapsas someone
who
hadto
always emphasize, morethan
otherswho took
it for
granted,
his Europeaness and hiscommitment
to civilization
andscience.
Trying
to
be objective,
yet
unsympathetic, Gama displayed
hisprejudice
against
African islanders'
lifestyles,
which he
regarded
asmarked
by
a
negligent attitude
of
living
for
the moment,
founded
upon
what
we
would
refer
to
today
as genderinequities: women
hadto perform
all
the
hard
labor, and men
measuredtheir wealth
by
thenumber
of
wives
they
controlled.3OGama's
opinions
seemro
accordwith
the
establishedviews about Africans held by
Portuguese settlers,lYedicine on
the
Edge
lBladministrators, and missiolaries.
\íhat
stands
out
in
his writings
isthat
despite his distanceand disdain
for
empirical
work,
heprovides
adetailed, ethnographic-like account
of African
healing.
Could
he haveobtained
it
from
Ezequiel
da Silva,who
was
soimmersed
in
the local
life to
thepoint
of
being depicted as a Ganga, the"halfway
witch-doc-tor,"
by the
officer
Cunha
in
1883?Or
perhapsfrom
Cunha
himself?With no
record
of their interaction, we
can
only
guessby
comparing
their
writings-and
conclude
that
Gama's
depiction
is
a much
more
diluted and
impressionist approach
to
local
knowledge
than
that of
Ezequiel,
who
wasfully
immersedin
local culture.
Plants, Healing,
and Knowledge
It
is unlikely that
in
such
a small
place as Chiloane
Arthur
Ignacio
da
Gama and Ezequiel
da
Silva never met,
asboth
were
part
of
theinner circle
of thoseupon
whom
the Portugueseauthorities relied' The
Portuguese
community living in
Sofala hadalways
beenquite
small.'11 Peoplefrom
Portugal (reinóis) were very
few
and most
of
thosewho
qualified
as Portuguesehad
first
gone
to
India or Macau
before
set-tling
in
Sofala. There
were also convicts
or
prisoners,
who did
not
represent
mainstream European culture.
In
other words,
the
local
Portuguese
community
wassociall¡
culturall¡
andhistorically
distant
from
Europe; theymight
rather
be regarded asbelonging
to
theIndian
Ocean'Vlorld
(IO\ø). Unlike
Gama,who
had comefrom India
imbued
with
a senseof
mission
about
rescuingand
"civilizing"
Africans,
peo-ple
like
Ezequiel
did not
feel
obliged
to follow
any external
agendaregarding
theindigenous
peoples-in
fact,
Ezequiel andhis folks
were regardedby
the Portugueseauthorities
ashalfway
nativeswho
sharedmuch
of
the lifestyle
of
the actual indigenous
population.
Ezequiel was
the
son
of
Zacarias
Herculano da
Silva,
who
began his career as amilitary
man
in
Sofala
in
1810.
His
grandfathers were
João
Julião
da Silva, a second-generation Portuguesewho
wasborn in
Macau in1769
and movedto
Sofalain
1'790, and FranciscoHonorato
da
Costa,
who
in
the early
níneteenth
century had
beendirector of
the
"Cassangefair,"
atrading
post
in the
Cuango,
Angola.
Ezequiel'sfamily
was closely connected
to
the
Portuguesecolonial
administra-tion, like many
others;
unlike many
others, however,
was their
pro-found
knowledge
of Africa
and
of
the
experienceof
the IO\ü. Joining
the
Portugueseadministration at
ayoung
age,Ezequiel da Silva
took
the
position
of
schoolteacherin
Chiloane. He
was
aheady therewhen
l82
Cristiana Bastos and Ana Cristina RoqueBesides
their
differences
in
social background
and
education,
Ignacio and Ezequiel had different worldviews and different
atti-tudes
about the
place
they were
in
and the
people
who lived
there.Ignacio
was âpasserby; Ezequiel was
aresident.
Ignacio
wasan
out-side observer; Ezequiel
was part
of
the community.
Those
different
positions are apparent
in
the ways they
observe
and
describe
theisland
of
Chiloane, its
characteristics, resources,
and potentialities.
The
worthless,
unsuitable island
described
by Ignacio is referred to
by
Ezequiel da Silva as
a
complex
ecosystem,providing
different
resources
that local
people
knew how
to
useand capitalize
upon.32Unlike
Ignacio's, Ezequiel's observations were the
direct
result
of
hisown knowledge
of
the region. He combined observation and
living
experier-rce
in
acontinuous
learning
processlegitimized by local
tra-ditional
usesand practices. Therefore
he was ableto look
far
beyond
the
"poor
lanclsof
Chiloane,"
identifying
resources
and
potentiali-ties,
namel¡ medicinal
herbs
and plants that,
once analyzed,
could
come
to
integrate the
Western
pharmacopoeia and be
a
source
of
income
for
the
colony.33Informing
on thedifferent medicinal
herbs andplants existing in
theisland
of
Chiloane,
Ezequiel da Silvaprovides
dataon
thelocal
ecosys-tem and specificdifferent habitats-sandy
lands, sandydry
lands,wet-lands,
sandywetlands, mangroves,
beaches,and coastal
lagoons-all
of
them testifying
to
the island's
biodiversity
and his
own
knowledge
on
the
territory. For this
reasonCunha
refersto him
asa
Ganga, the
"graduate
healer,"
the
one
to
beconsulted whenever the
community
had a health
or
apolitical
problem.3a \ü/heninforming on traditional
knowledge
andpractices related
to
theknowledge,
identification,
and useof
medicinal
flora,
Ezequiel showshow
he wasân insider
to
local
culture. Moreover,
he suppliesadditional information
on theway
peo-ple
exploit
and manage thelocal natural
resources.This "being
part of
the
group"
became essentialeither
to report
usesand
prove its
effec-tiveness
or to
substantiate
traditional
knowledge.
As
a physician
and having to
face the
many difficulties
related
to
the
operability
and effectivenessof
thehealth
servícesin Mozambique
(lack
of
funds
to
guarantee
basicoperating
services,lack of
facilities,
lack
of
human and technical
resources,and
lack of
medicines), Gama gavepriority
to clinical
observations,
seekingto
act according
to
hisscientific background
and neglecting â moreempirical approach to
thelocal medical solutions. This approach
would
haverequired long-term
research,
for which
he
had no time
to
spareand was
not
convinced
would
beworthwhile.
35Medicine on
the
Edge
lB3Thus,
although both Ignacio
and Ezequiellooked
into
theproblems
of
disease and healing,their
perspectives wererather different. Ignacio
advocated
the
defenseof
scientific medicine
and its role
asa
vector
of
civilization; whether
or
not
he might be personally
sympathetic
to
traditional
healing,
or
even exposed
to
it
outside medical
school,his formal training was
all
about rejecting the argument that
non-European knowledge
might
bevalual'rle
and
effective;
for
him, only
European
medicineshould
besupported,
used, andpromoted.
In
sucha
corner
of
the
world,
with
so
many
adversaries,he
might
have
felt
that
histask
was immenseand
perhaps he wasalone
as thepaladin of
scientific
medicine.Unlike lgnacio,
Ezequiel waswell
âwareof
hislack
of "scientific training" in
medicine;
on
the
other
hand,
he hacl apro-found
knowledge
of
the place,its
resources, and the usespeople
madeof
them-particularly
in
the
field
of
herbal medicine.
He
stressed theimportance of making a rigorotts and
systematic survey
of
the
local
medicinal-pharmaceutical flora, which
recluiredlearning about
its usesfrom
the local
practitioners;
the results
of
such research, he foresaw,would
have animpact
not only in
Sofala andMozambique but
alsoin
the
other
Portuguese overseasterritories
and
evenin
Europe.36This particular position
of
Ezequiel
doesnot
mean he completely
supported
the healing practicesperformed
by thelocal
healers.In fact,
though he
understood
the role
of
the
healers
in
the
communit¡
hewas very critical
of
their performance and
even
doubted
that
their
prâctices
could
beaptly
namedmedicine, although
hereferred to them
as
"Kaffir
medicine."37He
distinguished
clearly
between
the
healer'sperformance
and thehealing properties of certain plants when applied
to practical
situations.
He
regarded
the
healers' procedureswith
sus-picion;
only
in
a very few situations
did
he consider
the
efficacy
of
the
way
the
healer acted.As
for
the
medicines used,they were
worth
considering
becausethey proved
to
be effective.3s 'SØhilepointing
out
the lack
of
a
pharmacopoeia
in
the
Slesternsense and the
difficulty
of compiling
recipesin
the absenceof
preestab-lished
doses, Ezequiel'swork
combined modern scientific methods
of
registry
andcollection
of
samplesfor
study (Figure
7.4
andTable
7.1')with traditional
proceduresof
diagnosisand
treatment.3eEzequiel's
work
revealsa profound
knowledge
of
Sofala'snatural
environment and
of
the
local
phytotherapeutic practices
basedon
theperceived
relationship
between
disease,plant, and habitat
of
occur-rence.His
aim was
to identify
possible solutions
for
health problems
both in
Sofala andin other
regionsunder
Portugueserule.
He collectedi.,
l84
CristianaBafos
and AnaCrilina
Roque/,,!//t ¿ ,/n/
'/ t'/e/ia
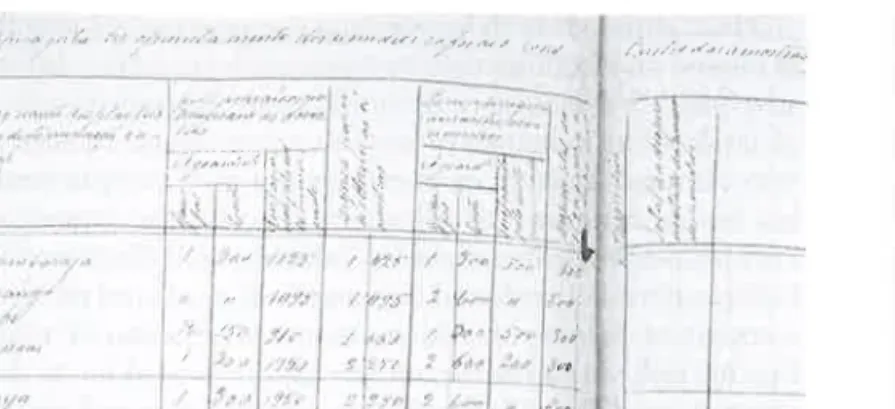
Table
7.1
Registry table fo¡ the collected samples. Reproduction of the table usedby Ezequiel da Silva for the registry of the medicinal herbs and plants collected (AHU Manuscript, fl.8v-9)
Number of plants providing these samples 3
.: i (t ,l .1 /.";,,:ì..jI \
ì
t /t.1.|,, .r/,. ' /)¿, ./ it 1J,
,7¿" Root Leave Resin Pounds Ounces Octaves Pounds Ounces Octaves Pounds Ounces Octaves Pounds Ounces C)ctâves 1\
/.J /' '.t / Bark Designation of the speciesof the several samples
and weight
Figure
7.4
Excerpt from the registry book of the plant samples collected by Ezequielda Silva (1883),
IICI
AHU, Códice-SEMU_2186. (courtesy of the Historical OverseasArchive [AHU] and the Tropical Research Institute [ICT], Lisbon.)
used
in
Chiloane and
SofalaDistrict,
and compiled the
different
reci-pes
listed
in
1883 by Cunha
in
his
booklet.a0As often
acknowledged,
"one could
take considerable
advantagesfrom
the
useof
most
of
thesemedici¡ss"-¿¡d
thus
headvocated
theuse
of
the local medicinal
flora
and its study (including both plant
potentialities and
habitat of
occurrence), assumingthat
certain health
problems,
in
other regions,
could
beavoided
with
the
introduction of
specific
medicinal plants
that did not grow nâturally
there.alEzequiel
illustrated
thispoint
with
the cases ofDurura,
Chicarafunda,
Gambacamba,
andMutiuari.
Durura
andChicarafunda,
if
introduced
into
regionswith similar
habitats, could provide possible solutions to
decrease
the
neonatal
mortality
rate.
That could
be
the
casefor
theInhambane
District
(south
of
Sofala),noted
Ezequiel,who knew that
none
of
those
plants were growing
there
either
becausehe had
theopportunity
to
gothere
or
because he had agood
informant
on
rhosematters.42
As
for
Gambacamba and
Mutiuari,
introducing them
to
other
areas
could
provide
good local
substitutesfor
the marshmallow roots
(Abhaea
officinalis)
and the extract
of liquorice (Glycyrrhiza
glabra),
thereby
minimizing
theconstant failures of
these drugsin
thepharma-cies
of
hospitals and health
care centers.Knowing
the
diversity
and specificity
of
eachhabitat
and the way
it
influences
the
occurrence
or
absenceof
certain
speciesand,
con-sequently,
the fact that they are
used
there
or
not, Silva
underlines
that the
useof
each
plânt
for
the treatment
of
a
specific
disease isLocal name Goche
Type and
habitat
Trailer with long and rough leaves living in sandy areasAreas of
ocurrence
Chilluane Island and SofalaQuantities used Root Bark Leave Resin Pounds Ounces Octaves Pounds Ounces Octaves Pounds Ounces Octaves Pounds Ounces Octaves
Medicinal
vi¡tues
Fevers, marsh-fevers, and urinary problems Preparation andapplication
Decoction of the leaves, branches, and roots. Drink hot for
the fevers and cold for the urinary problems
Efficient ¡esults in both cases though it seems that it is not relevant the fact it is taken hot o¡ cold. The reason I mention this is because I was told these were the right procedures accordingly to each disease.
l86
CristianaBafos
and Ana Cristina Roquean important
part of
the cultural
heritage
of
each
communit¡
thusrevealing
both
asolid knowledge of
thelocal natural
resources and the capacityof
usingthem to
solvetheir
basic needs.a3This explained how,
in
asmall island
such asChiloane,
theinhabitants
of
the
sandy landsknew that
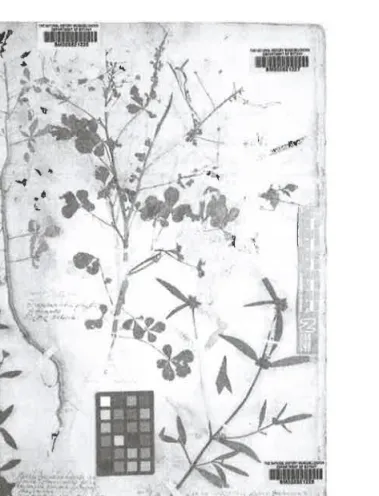
the leaves andflowers oÍ Muanga (Gynandropsis gynandra)
(Figure 7.5)
would
heal
fevers associatedwith
colds,
while
those
liv-ing
in
the mangrovesof
the
sameisland, where Muanga do
not
occur,knew
that Mutungumuja
leaveswould
cure the same symptoms.a4lYedicine on
the
Edge
lB7All
these referencesunderline what
is
common knowledge
basedon life
experience and
traditional
use,complementing the more
spe-cific
know-how
of
the
traditional
healei
that no
community
candecline,
with
that
of
each
specific habitat,
so
that
people
find
dif-ferent solutions
to
solve
trivial
daily problems always
in
view of
preserving
their
balance and welfare as
a
community. Just as in
Paracelsus's
saying
that
"each
country
has specific
diseases
andfor
each country
nature provide[s]
the
solution
to
heal
them,"46Ezequiel's
findings reveal different types
of
herbs and plants
with
medicinal
virtues-in
wetlands, salt-marshy
areas,
dried,
or
sandy
lands.
These
herbs were applied
to
solve
or
slow down the
most
common
ailments and
diseases.Concluding
Note
In
brief,
in
the context
of
establishing the
Portuguese
colonial rule
in
Mozambique
there
is
evidence
that
many
âctors-Africans,
Europeans,
Luso-Africans, and Luso-Asians-were involved
in
dif-ferent forms
of
knowledge
exchanges, someof
them
with
therapeu-tic
value. The
brief
analysis
of
two
different colonial actors who
lived at
the
sametime in
the island
of
Chiloane, Sofala, and referred
to
local knowledge
of
plants and healing
practices,
show
that
thescope
of
interactions
acrossthe
Indian
Ocean ismultisided,
complex,
and irreducible
to
a monolithic understanding
of
the relationship
between colonizers
and colonized, foreigners and
locals,
and
exter-nal
and indigenous knowledge.
Arthur
Ignacio
da
Gama
went
to
Mozambique like many
of
his
Goan
peers-a
colonial
subject
born
into a local
elite, achieved
higher education
in
Goa,
and started
hiscareer
in colonial
medicine by serving
in Africa.
In
Africa
he enactedEuropeanness
and
expressed
reservations regarding
the
lifestyles
of
local populations,
their
healing practices, and
their
knowledge
about
them-ât
least, those
that
he
got
to
partially know.
Ezequiel
da Silva,
on
the
other
hand, was
athird-generation
Eurodescendant
whose grandparents had
beencrossing the
Indian
Oceanand serving
the
empire
in
severallocations. He lived
closer
to
local populations
and adopted much
of
their knowledge-particularly
in
matters
of
potentially
healing plants,
which
hecompiled
carefully. Ezequiel
hadno higher training, yet
he
usedhis skills
and
proximity
to the
local
population
to gather knowledge
andmake
it
available
to
thecolonial
and
European circles,
which
used
them
in
ways
that
areyet
to
beknown in detail
and
deservefurther
research.-ffiffi
$
t
? I¡
"ffiffi
L*t
Þ ,é.t
,'.ff 'E. ì¡hç
t/ -i I I i{Þ
I
I Ì,:\ì
"4,l! T(
IÅ
¡"ffiffiì
{'
I .1 ¡ J Irümffiur
Figure 7..5 Gynandropsis gynandra
Source: Hermann Herbarium, Natural History Museun, London

![Figure 7.3 The Harbor and Islands of Chiloane (IICT-CDI-0483-19521. (courtesy of the Historical Overseas Archive [AHU] and the Tropical Research Institute [IICT], Lisbon.)](https://thumb-eu.123doks.com/thumbv2/123dok_br/19292002.993507/9.1262.157.601.532.797/islands-chiloane-courtesy-historical-overseas-tropical-research-institute.webp)