w w w . r b o . o r g . b r
Original
article
Posterior
cruciate
ligament
injury:
characteristics
and
associations
of
most
frequent
injuries
夽
,
夽夽
Marco
Túlio
Lopes
Caldas
a,∗,
Gilberto
Ferreira
Braga
b,
Samuel
Lopes
Mendes
c,
Juliano
Martins
da
Silveira
d,
Robson
Massi
Kopke
daOrthopedistandTraumatologist;HeadoftheMedicalResidenceServiceofHospitalMariaAméliaLins,Fundac¸ãoHospitalardoEstado
deMinasGerais(FHEMIG);MemberoftheKneeGroupofHospitalMariaAméliaLins,FHEMIG,BeloHorizonte,MG,Brazil
bPreceptorofMedicalResidenceinOrthopedicsandTraumatology,HospitalMariaAméliaLins,FHEMIG,BeloHorizonte,MG,Brazil
cResidentPhysician(R4)inKneeOrthopedicsatHospitalMariaAméliaLins,FHEMIG,BeloHorizonte,MG,Brazil
dResidentPhysician(R4)inKneeOrthopedicsattheOrtolifeClinic,BeloHorizonte,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1July2012 Accepted3September2012
Keywords:
Retrospectivestudies Knee
Posteriorcruciateligament/injuries Posteriorcruciateligament/surgery
a
b
s
t
r
a
c
t
Objective:ToinvestigatetheprevalenceandcombinationsofPCLinjuriesandtheir
correla-tionswiththemechanism,theoccurrenceofevidentdislocationandassociatedfracture.
Method:Aretrospectivestudyof85lesionsofPCLoperatedbetween2003and2010.Diagnosis
byphysicalexaminationanddynamicradiography,comparedwithsurgicalfindings.
Results:InjuriesinvolvingthePCLweremoreprevalentinmen(78.8%)withameanageof33
years.Themaincausewastrafficaccidents(73.80%),and(49.4%)motorcycle.IsolatedPCL injuryoccurredin(15.3%)cases,andcombined(84.7%).Amongtheisolatedlesions,bone avulsionswerenine(10.6%).ThemostassociatedPCLinjuriesweretheACL(48.2%), fol-lowedbyLCLPCL/PLC(22.4%).FracturesweremoreassociatedwithcombiningPCL+LCL/PLC injuriesanddidnotappearinthePCL+MCL/PMC.Complicationsbeyondfractures: periph-eralnerveinjury(4.8%)andvascular(1.2%).Evidentdislocationinprimarycare(16.7%)was moreprevalentincombinedACL+PCL+MCL/PMC(44.4%).Halfthepatientswereoperated duringtheacutephase.Therewasastatisticallysignificantdifference(p<0.05)comparing eachcombinationofligamentinjurieswiththepresenceoffracture,dislocationorclear mechanismofinjury.
Conclusion: SurgicaltreatmentofPCLinjuriesinacenterfororthopedictraumacarewas
mostlymultiligamentandmainlyinvolvingtheACL.Asignificantassociationwasseen betweenthetypeofinjurywithmechanismofinjury,presentationoftheknee,ifdislocated orreduced,andthepresenceofassociatedfracture.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:CaldasMTL, BragaGF, MendesSL,daSilveiraJM,Kopke RM.Lesõesdoligamentocruzadoposterior: característicaseassociac¸õesmaisfrequentes.RevBrasOrtop.2013;48:427–431.
夽夽
StudyconductedattheHospitalMariaAméliaLins,Fundac¸ãoHospitalardoEstadodeMinasGerais,BeloHorizonte,MG,Brazil.
∗ Correspondingauthorat:RuaFlavitaBretas,29/901,Luxemburgo,BeloHorizonte,CEP30380410MG,Brazil.
E-mail:[email protected](M.T.L.Caldas).
Lesões
do
ligamento
cruzado
posterior:
características
e
associac¸ões
mais
frequentes
Palavras-chave:
Estudosretrospectivos Joelho
Ligamentocruzado posterior/lesões Ligamentocruzado posterior/cirurgia
r
e
s
u
m
o
Objetivo: Pesquisaraprevalênciadaslesõesdoligamentocruzadoposterior(LCP)esuas
combinac¸õesecorrelac¸õescomomecanismoeaocorrênciadeluxac¸ãoevidenteefratura associada.
Método: Estudo retrospectivo de 85 lesões do LCP operadas entre 2003 e 2010.
Diag-nósticopormeiodoexamefísicoedaradiografiadinâmica,confrontadoscomachados cirúrgicos.
Resultados: LesõesqueenvolveramoLCPforammaisprevalentesnoshomens(78,8%)com
médiadeidadede33anos.Acausaprincipalfoioacidentedetrânsito(73,80%),dosquais 49,4%demotocicleta.LesãoisoladadoLCPocorreuem15,3%doscasosecombinadaem 84,7%.Dentreaslesõesisoladas,noveforamavulsõesósseas(10,6%).Oligamentomais associadoàslesõesdoLCPfoiocruzadoanterior(48,2%),seguidodalesãocombinadado LCPcomoligamentocolaterallateral/cantopóstero-lateral(22,4%).Fraturasestiverammais associadasàcombinac¸ãoLCP+LCL/CPLenãoapareceramnaslesõesdoLCP+ligamento colateralmedial/cantopóstero-medial.Complicac¸õesalémdefraturas:lesãodenervo per-iférico(4,8%)evascular(1,2%).Luxac¸ãoevidentenoprimeiroatendimento(16,7%),mais prevalentenacombinac¸ãoLCP+LCA+LCM/CPM(44,4%).Metadedospacientesfoi oper-adanafaseaguda. Houvediferenc¸aestatísticasignificativa (p<0,05)nacomparac¸ãode cadacombinac¸ãodelesõesdeligamentoscomapresenc¸adefratura,luxac¸ãoevidenteou
mecanismodotrauma.
Conclusão: LesõesdoLCPsubmetidas atratamento cirúrgicoem centro deatenc¸ão ao
traumaortopédicoforamnasuamaioriamultiligamentareseenvolveramprincipalmenteo LCA.Houveassociac¸ãosignificativaentreotipodelesãocomomecanismodetrauma, a forma de apresentac¸ão do joelho, se luxado ou reduzido, e a presenc¸a de fratura associada.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Withtheexplosiveincreaseinthenumberofvehicles, espe-ciallymotorcycles,lower-limbinjuriesandparticularlyknee
injuries have become public health problems. They have
high social and economic costs. Improvements in
diagno-sis and advances in knowledge of anatomy, biomechanics
andsurgicaltechniqueshaveincreasedtheinterestin stud-iesinvolving theposterior cruciateligament (PCL).1–6 Large
number ofPCLinjuriesare caused byhigh-energytrauma,
and in these cases, knee injury may be difficult
particu-larlywhenpatientspresentfracturesoftheipsilateralfemur and/or tibia. In evaluating these patients, just as in
mul-tiple trauma cases, ligament injuries may gounnoticed at
theinitialattendance.7,8Fewstudieshaveevaluateddifferent combinationsofinjuriesthatinvolvethePCL,inrelationto themechanism,incidenceoffracturesinthekneeaffected or evident dislocation. Studying these characteristics may
contribute toward making a correct diagnosis during the
acutephaseandenablingappropriatetreatmentattheideal time.
Theobjective ofthisstudy wastoinvestigatethe preva-lenceofcombinedinjuriesofthePCLandtheircorrelations withthemechanism,occurrencesofevidentdislocationand associatedfractures.
Materials
and
methods
Byconsultingourinstitution’ssurgicalrecords,wesurveyed the medicalfilesofpatientswho underwentsurgical
treat-ment for PCL injuriesof the knee between May 2003 and
September2010andfound85casesin84patients.We
inves-tigated the trauma mechanism, the number of ligaments
injured,theprevalenceofdifferentcombinationsofinjuries
and the association of each of them with knee fractures,
evident dislocation, trauma mechanism and time elapsed
betweentheaccidentandthedefinitivetreatment.Inthe
insti-tutionwherethestudywasconducted,thediagnosesmade
inthe emergencysectorwascomparedwiththe diagnoses
thatresidentsundergoingspecializationtraining withinthe
KneeSurgeryGroupmadebymeansofhistory-taking,
phys-icalexaminationandradiographs.Afterwards,thediagnoses
were reviewed by knee surgeons, who made physical and
radiologicalexaminationsofstress(dynamicexaminations), underanesthesiaduringtheimmediatepreoperativeperiod.
The diagnosis was complemented bythe surgical findings
fromthecasesoperatedduringtheacutephase.
Descriptive analysis was performed on the study
Table1–Frequenciesofinjuredligamentsandtrauma mechanism.
Frequency Percentage
Numberofligamentsinjured
1 12 14.1
2 37 43.5
3 35 41.2
4 1 1.2
Traumamechanism
Motorcycle 42 49.4 Beingrunover 17 20.0
Sprain 12 14.1
Carcollision 8 9.4 Fallfromheightormartialarts 3 3.5
Table2–Frequencyofassociatedinjuries,evident dislocationandPCLboneavulsion.
Frequency Percentage
Fracturea 17 20.5
Peripheralnerveinjuryb 4 4.8
Vascularinjuryb 1 1.2
Evidentdislocationb 14 16.7
PCLboneavulsion 9 10.6
a Twocaseswithoutinformation(2.4%).
b Onecasewithoutinformation(1.2%).
Pearson’schi-squaretestwasalsoused,inordertocompare proportions, and Fisher’s exact test for small samples. For
numericalvariables,thenonparametricMann–Whitneytest
ortheKruskal–Wallistestwasused,becauseofthe asymmet-ricalnatureofthevariablestested.Thesignificancelevelwas takentobe5%.TheSPSS15.0softwarewasused.
Results
TheincidenceofPCL injurieswas greater amongthe men
(78.8%).Themeanagewas32.9years,withastandard devia-tionof11.9.Mostofthecasespresentedtwo(43.5%)orthree (41.2%)injuredligaments.TheprevalenceofPCLinjuryalone
was 15.3%. Nine (10.6%) of the injuries were due to bone
avulsion.Trafficaccidentswereresponsiblefor73.8%ofthe injuriesandofthese,themostfrequenttraumamechanism (49.4%)wasmotorcycleaccidents,followedbybeingrunover (20%)(Table1).
Table2showsthefrequenciesofassociatedinjuries, evi-dentdislocationandPCLavulsion.
PCLinjuriescombinedwithotherligamentsaccountedfor 84.7%ofthecases,andofthese,thelargestnumberinvolved
the anterior cruciate ligament (ACL) (48.2%), followed by
thelateralcollateralligament/posterolateralcorner(LCL/PLC) (22.4%).Theprevalenceofinjuriestobothcruciateligaments withoutcombinationwithperipheralligamentsorwith evi-dentdislocationwas 7.1%.Inanalyzing therelationship of eachinjurycombinationwiththecause,motorcycleaccidents werethemostfrequentcause,withastatisticallysignificant difference(p-value<0.05),exceptforpatientswiththe com-bination of PCL+medial collateral ligament/posteromedial
corner (MCL/PMC), forwhombeing runover was themost
frequentmechanism(41.7%)(Table3).
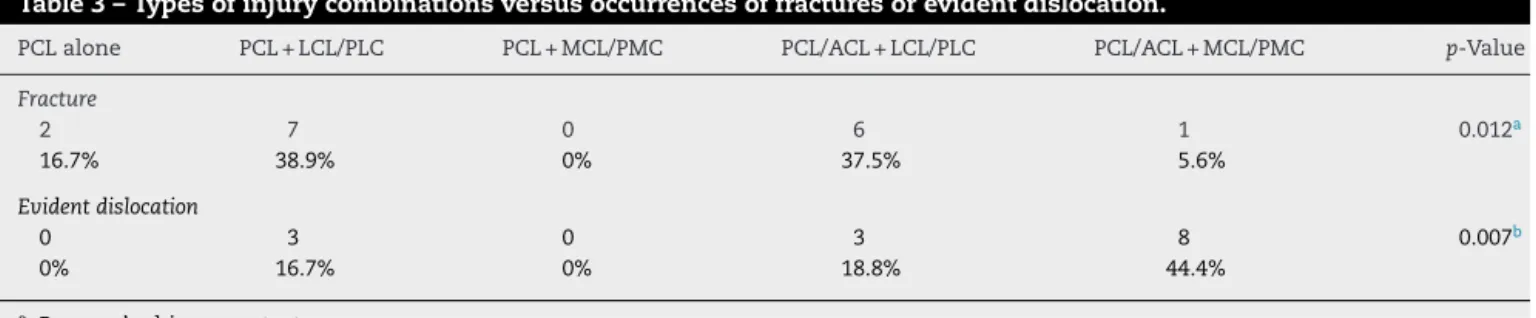
There was a significant difference (p<0.012) in
compar-ing the different combinations of ligament injuries with
occurrences of fractures or presentation of evident dislo-cation at the emergency service (p<0.007). Fractures were moreassociatedwiththecombinationsPCL+LCL/PLC(38.9%) andPCL/ACL+LCL/PLC(37.5%),whileevidentdislocationwas
more associatedwith the combination PCL/ACL+MCL/PMC
(44.4%)(Table4).
In 85% of the cases, the knee ligaments were operated
withinthe firsteightmonths,and 50%oftheseoperations wereperformedintheacutephase,uptothreeweeksafter theinjury.
Discussion
Inthisstudy,85PCLinjurieswereevaluated,inpatientswho
underwentsurgicaltreatmentinanorthopedictraumacare
center betweenMay2003and December2010. The
diagno-siswasdonebymeansofclinicalexamination,withdynamic
assessmentofthekneeunderanesthesia,andwas
comple-mentedbythesurgicalfindingsinthecasesoperatedinthe acutephase.Withregardtogender,therelationshipconsisted ofapproximatelyfourmenforeverywoman,andthegreatest incidencewasinthethirddecadeoflife,i.e.similartoreports intheliterature.9,10
Fanellietal.11,12reportedthattheincidenceofPCLinjury was44%inatertiary-leveltraumacarecenter,amongknees
withhemarthrosisthatunderwentexaminationunder
anes-thesiaand arthroscopy.Themaincauseswere high-energy
trauma (81.5%) and sports injuries (18%). PCLinjury alone
occurred in 7.5% and combinations with other ligament
injuriesin92.5%.LaPrade13assessedkneeligamentinjuries andobservedthatPCLruptureoccurredin14.4%ofthecases,
and in8.2% ofthe patients withhemarthrosis after acute
trauma.
Acute-phase knee ligament injuries are diagnosed by
meansoftakingadetailedhistory,makingacarefulphysical
examinationandproducing stressradiographsunder
anes-thesia.Magneticresonanceimagingisconsideredtobethe goldstandard.13–17Insomecases,theligamentinjuryisnot
diagnosedbecausethesymptomsmayremainmaskedwhen,
forexample,ipsilateralfracturesoccur,asreportedbyBraga et al.18Intheir study,28 patientswith29unstablefemoral
fractures were treated with locking intramedullary nails
and were evaluated inthe immediatepostoperativeperiod
with the aim of determining the incidence of associated
ligamentinjuries.Eightpatients(28.6%)presentednineknee ligament injuries(32.1%; onebilateral case).None ofthese injurieshadbeenreportedattheemergencyservice.Inthe same study,therewasastatisticallysignificant association betweencomplexkneeinjuryandbeingrunover(p=0.004).
These authors emphasizedthat theknees ofpatientswith
ipsilateral femoral fractures caused by high-impact injury shouldberoutinelyexamined.
Table3–Typesofinjurycombinationsversusoccurrencesoffracturesorevidentdislocation.
PCLalone PCL+LCL/PLC PCL+MCL/PMC PCL/ACL+LCL/PLC PCL/ACL+MCL/PMC p-Value
Fracture
2 7 0 6 1 0.012a
16.7% 38.9% 0% 37.5% 5.6%
Evidentdislocation
0 3 0 3 8 0.007b
0% 16.7% 0% 18.8% 44.4%
a Pearson’schi-squaretest.
b Fisher’stest.
from 70% for grade I injuries to 97% for grades II and
III.19Resultsfromclinicalexaminationsanddynamic
radio-graphsshouldbecomparedwithmagneticresonanceimaging
(MRI).20Unfortunately,fewhospitalswithintheBrazilian set-tingprovideaccesstoMRIintheemergencysector.Thus,itis importanttohavestudiesthatanalyzetheresultsfrom assess-mentsonacuteligamentinjuriesbasedondynamicphysical andradiologicalexaminationunderanesthesia.
Inthepresentseries,itwasfoundthat78.8%oftheinjuries were from trafficaccidents, ofwhich 49.4% were motorcy-cleaccidents.Theseresultswere closetothose ofFanelli,1 whofoundthat81.5%oftheircasesresultedfromhigh-energy trauma.Schulzetal.9studied494patientsandreportedthat thecommonestcausesweretrafficaccidents(45%)andsports injuries(40%),andthatmotorcycleaccidents(28%)andsoccer injuries(25%)werethecommonestspecificcauses.
Identifyingdifferenttypesofkneeligamentinjuryis impor-tant forthe prognosis and fordefining the treatment. PCL injuryalonehaslowincidence(7.5%)andthoseofgradesIand IIhavegreaterchanceofhealing,inthesamewayasmedial collateralligament(MCL)injuries.20,21PCLinjuriesalonemay beasymptomatic,asreportedbyParolieandBergfeld,21who foundthattheincidenceofthischaracteristicwas2%among playersintheAmericanNationalFootballLeague(NFL).Inour series,wefoundthattheincidenceofPCLinjuriesalonewas 15.3%andthat69.2%ofthemwereduetoboneavulsion.All ofthesecasesunderwentsurgicaltreatment.
Thereiscontroversyregardingthebesttreatmentforgrade III PCL injuries that occur in isolation and for those that arecombinedwithmedialorperipheralligaments.3–5Inthe
presentseries,surgicaltreatmentwasindicatedforcomplete PCLinjury(gradeIII)orforcombinedinjurywhenthe poste-riordisplacementofthetibiawas>10mm.8,19Inconcordance withareportintheliterature,5surgerywasthetreatment indi-catedforinjuriesthatinvolvedthePCLorPCL/ACLcombined withlateralstructures.Hammoudetal.22conductedareview study on21caseseriesofPCLinjuryalone and10of
com-bined injuries.They concludedthattherewas noevidence
regardingthebest treatmentorthebestsurgicaltechnique tochoose, andthat despitethereportsofgood results fol-lowingPCLreconstruction,evaluationswithlongerfollow-up suggestedthatinmostcases,normalkneestabilitywasnot restored.
Our series included onlythe casesthat underwent
sur-gical treatment inwhich the main injury mechanism was
high-energytrauma.Thischaracteristicmayexplainthehigh numberofcasesinvolvingtwoormoreligaments(85.9%ofthe cases).Inconcordancewithotherstudies,PCLinjuryappeared ingreatestnumberinvolvingtheACL,i.e.asinjuriesofboth cruciateligaments,orincombinationwithmedialorlateral peripheralligaments.10,19
Therewasastatisticallysignificantdifferencein compar-ingthecombinationsofligamentinjurieswiththeprevalence offracturesorevidentdislocation.Associationswithfractures
were morecommonincombinations betweenthe PCLand
lateral peripheral ligaments.Evident dislocationwas more
associated with the combination of PCL/ACL with lateral
peripheralligamentsanddidnotoccurincasesofPCLinjury aloneorincombinationsbetweenthePCLandmedial periph-eralligaments.Theprevalenceoffracturesorboneavulsions
Table4–Comparisonoftypesofinjurycombinationsversusmechanism.
PCLalone PCL+LCL/PLC PCL+MCL/PMC PCL/ACL+LCL/PLC PCL/ACL+MCL/PMC p-Value
Traumamechanism 0.022a
Beingrunover 0 2 5 3 6
0% 11.8% 41.7% 18.8% 35.3%
Car 2 1 0 2 2
15.4% 5.9% 0% 12.5% 11.8%
Sprain 0 2 2 5 1
0% 11.8% 16.7% 31.3% 5.9%
Motorcycle 11 12 3 6 7
84.6% 70.6% 25.0% 37.5% 41.2%
Others 0 0 2 0 1
0% 0% 16.7% 0% 5.9%
was20.5%.Injurytobothcruciateligaments(ACL/PCL)without combinationwithmedialorlateralperipheralligamentsand withoutassociationwithevidentdislocationappearedin7.1% ofthecases.Thiswasmuchlowerthanwhatwasreportedby Lustigetal.23whofoundthiscombinationin25%ofthecases inamulticenterstudybytheFrenchSocietyofOrthopedics andTraumatology.Itwasobservedthattheseauthorsdivided thecomplexmulti-ligamentinjuriesintothoseaffectingboth cruciateligaments(25.4%)andthosewithclassicaltraumatic dislocation(74.6%).Theyusedepidemiologicalcriteriasuchas age,presenceofassociatedinjuriesandtypeofinjuryinorder toindicateornotindicatesurgicaltreatment.Theychoseto reconstructthePCLduringtheacutephase,inpatientsunder theage of60 years withoutassociatedvascular injuriesor exposeddislocation,whentheposteriordrawerwasgreater than10mmand/orthefrontal,medialorlateralopeningwas greaterthan15mm.TheydidnotindicateACLreconstruction intheacutephase.
Inthe series evaluatedin ourstudy, onlyonecasewas referredwithareportofpoplitealarteryinjury. Itwas also seenthattherewaslowprevalence(4.8%)ofcommonfibular nerveinjury,comparedwithotherstudies.6,24
In 85% ofthe cases, the patients were operated within eightmonths,and50%ofthesewereoperatedwithinthefirst threeweeks,i.e.duringtheacutephase.Thegreatestmedian timebetweentheinjuryandthesurgery(105days)occurred amongpatientswithPCL+LCL/PLCinjuriesandthesmallest time(8.5days)amongthosewithPCLinjuryaloneduetobone avulsion.SevereinjuriessuchasthoseofthePCL+LCL/PLC wereoperatedlateroninsomecases,whichiscontrary to the idealmanagement ofgiving priorityto earliersurgical treatmentforthiscombinationofinjuries.Intheinstitution
wherethe study was conducted, multipletrauma patients
whohaveundergonedamagecontrolareoftenreceived,and this also often postpones the definitive treatment for the ligamentinjury. Inseriessuchasthat ofSchulz etal.9 the knee specialistsonlyreceived 10.3%of thepatients within thefirst30daysaftertheinjury.Surgerywasperformedafter ameantimeperiodof44.4months.
Thecriterionofonlyincluding patientswho underwent surgicaltreatmentinvolvingthePCLwasanattempttocreate
agroupthatwouldbemorehomogenousintermsofcause
andeffect. However,inastudy on kneedislocation, Buiet al.20foundthattraumathatwasconsideredtobelow-energy wasthemechanismin15cases(75%),suchasamateursports orsimplefalls,andthatonly20%were duetohigh-energy trauma,suchascaraccidents.
The number of 85 cases studied seems to have been
statisticallyadequate,giventhe relatively low incidenceof PCLinjuriesinthegeneralpopulation.Inthedataanalysis, consideringthelargenumberofcombinedinjuries,somewith very low prevalence, statistical analysis for small samples
wasused.
Conclusion
ThePCLinjuriesthatunderwent surgicaltreatmentinthis orthopedictraumacenterweremostlyaccompaniedby multi-ligamentinjuries.Themostprevalenttraumamechanismwas
trafficaccidents,notablywithinvolvementofmotorcyclesand
affectingmaleindividuals.TheACLwastheligamentmost
frequently injuredinassociation withthePCL, followedby lateralperipheralinjury.Therewasasignificantassociation
betweenthetypeofinjuryandthetraumamechanism,form
ofkneepresentation(dislocatedorreduced)andpresenceof associatedfractures.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.FanelliGC,BeckJD,EdsonCJ.Currentconceptsreview:theposteriorcruciate ligament.KneeSurg.2010;23:61–72.
2.HarnerCD,HoherJ.Evaluationandtreatmentofposteriorcruciateligament injuries.AmJSportsMed.1998;26:471–82.
3.ShelbourneKD,JenningsRW,VaheyTN.Magneticresonanceimagingof posteriorcruciateligamentinjuries:assessmentofhealing.AmJKneeSurg. 1999;12:209–13.
4.HermansS,CortenK,BellemansJ.Long-termresultsofisolatedanterolateral bundlereconstructionsoftheposteriorcruciateligamenta6-to12-year follow-upstudy.AmJSportsMed.2009;37:1499–507.
5.AllenCR,KaplanLD,FluhmeDJ,HarnerCD.Posteriorcruciateligament injuries.CurrOpinRheumatol.2002;14:142–9.
6.McDonoughEB,WojtysEM.Multiligamentousinjuriesofthekneeand associatedvascularinjuries.AmJSportsMed.2009;37:156–9.
7.DicksonKF,GallandMW,BarrackRL,NeitzschmanHR,HarrisMB,MyersL, etal.Magneticresonanceimagingofthekneeafteripsilateralfemurfracture. JOrthopTrauma.2002;16:567–71.
8.WalkerDM,KennedyJC.Occultkneeligamentinjuriesassociatedwith femoralshaftfractures.AmJSportsMed.1980;8:172–4.
9.SchulzMS,RusseK,WeilerA,EichhornHJ,StrobelMJ.Epidemiologyof posteriorcruciateligamentinjuries.ArchOrthopTraumaSurg. 2003;123:186–91.
10.CamargoOPA,ChameckiA,LemosPEG,PecoraRAM.Lesãodoligamento cruzadoposterior–Incidênciaetratamento.RevBrasOrtop.1996;31:491–6. 11.FanelliGC.Posteriorcruciateligamentinjuriesintraumapatients.
Arthroscopy.1993;9:291–4.
12.FanelliGC,EdsonCJ.Posteriorcruciateligamentinjuriesintraumapatients: partII.Arthroscopy.1995;11:526–9.
13.LaPradeRF,WentorfFA,FrittsH,GundryC,HightowerCD.Aprospective magneticresonanceimagingstudyoftheincidenceofposterolateraland multipleligamentinjuriesinacutekneeinjuriespresentingwitha hemarthrosis.Arthroscopy.2007;23:1341–7.
14.FischerSP,FoxJM,DelPizzoW,FriedmanMJ,SnyderSJ,FerkelRD.Accuracy ofdiagnosesfrommagneticresonanceimagingoftheknee:amulti-center analysisofonethousandandfourteenpatients.JBoneJointSurgAm. 1991;73:2–10.
15.MargheritiniF,ManciniL,MauroCS,MarianiPP.Stressradiographyfor quantifyingposteriorcruciateligamentdeficiency.Arthroscopy. 2003;19:706–11.
16.MarianiPP,MargheritiniF,ChristelP,BellelliA.Evaluationofposterior cruciateligamenthealing:astudyusingmagneticresonanceimagingand stressradiography.Arthroscopy.2005;21:1354–61.
17.ClancyWG,SutherlandTB.Combinedposteriorcruciateligamentinjuries. ClinSportsMed.1994;13:629–47.
18.BragaGF,CunhaFM,LazaroniAP.Instabilidadedojoelhoassociadaafratura dofêmur.RevBrasOrtop.1999;34:329–32.
19.RubinsteinRA,ShelbourneKD,McCarrollJR,VanMeterCD,RettigAC.The accuracyoftheclinicalexaminationinthesettingofposteriorcruciate ligamentinjuries.AmJSportsMed.1994;22:550–7.
20.BuiKL,IlaslanH,ParkerRD,Sundaram.Kneedislocations:amagnetic resonanceimagingstudycorrelatedwithclinicalandoperativefindings. SkeletalRadiol.2008;37,653–61M.
21.ParolieJM,BergfeldJA.Long-termresultsofnonoperativetreatmentof isolatedposteriorcruciateligamentinjuriesintheathlete.AmJSportsMed. 1986;14:35–8.
22.HammoudS,ReinhardtKR,MarxRG.Outcomesofposteriorcruciateligament treatment:areviewoftheevidence.SportsMedArthrosc.2010;18:280–91. 23.LustigS,LerayE,BoisrenoultP,TrojaniC,LaffargueP,SaragagliaD,etal.
Dislocationandbicruciatelesionsoftheknee:epidemiologyandacutestage assessmentinaprospectiveseries.OrthopTraumatolSurgRes.
2009;95:614–20.