Dear Sepsis-3, we are sorry to say that we don’t
like you*
On February 23rd, 2016, the Journal of the American Medical Association
(JAMA) published a proposal for new deinitions and criteria for sepsis, which the authors called Sepsis-3.(1) At the same time, the authors named the previous
sepsis deinitions Sepsis-1 (from 1991)(2) and Sepsis-2 (from 2001)(3) (Table 1).
he proposal was prepared by a task force appointed by the European Society of Intensive Care Medicine (ESICM) and the Society of Critical Care Medicine (SCCM), which was composed of 19 specialists in intensive care, infectious diseases, surgery and pneumology. he document was subscribed by 32 scientiic societies.(1)
Sepsis became deined as a “life-threatening organ dysfunction caused by a dysregulated host response to infection.”
he method used to prepare the proposal was a retrospective analysis of large hospital databases from two countries (the United States and Germany, with considerable predominance of the former) in the attempt to establish the clinical and laboratory parameters that best correlated with mortality among patients with suspected infection.
To identify this cohort of patients with suspected infection in large hospital databases, the authors used non-validated criteria, including patients treated with antibiotics within 72 hours after collection of biological samples for microbiological analysis or patients subjected to sample collection up to 24 hours after the onset of antibiotic treatment.
Because the deinition of sepsis came to be centered on “organ dysfunction”, the task force suggested using a score of organ dysfunction/failure [i.e., the Sequential Organ Failure Assessment (SOFA)](4) as the diagnostic criterion for
sepsis. According to this suggestion, a patient with an acute change in the SOFA score ≥ 2 meets the criteria for sepsis (Table 2). he task force established that the baseline SOFA score should be zero unless the patient was known to have preexisting (acute or chronic) organ dysfunction before the onset of infection.
However, due to the limitations of SOFA outside the intensive care unit (ICU), the task force recommended a new score [i.e., “quick SOFA” (qSOFA)]. his instrument, which was also developed by the task force and was not validated in clinical practice, comprised three clinical parameters that were easy to assess (Table 3) and were associated with high mortality when at least two of them were simultaneously present. In contrast, SOFA includes laboratory data and therapeutic approaches that have diferent scores according to pre-deined thresholds.
In turn, septic shock was deined as a “subset of sepsis in which underlying circulatory and cellular metabolism abnormalities are profound enough to substantially increase mortality.”
António Henriques Carneiro1, Pedro Póvoa2,3, José Andrade Gomes4
1. Department of Medicine, Emergency and Intensive Care, Hospital da Luz Arrábida - Gaia, Portugal.
2. Polyvalent Intensive Care Unit, Hospital de São Francisco Xavier, Centro Hospitalar de Lisboa Ocidental - Lisbon, Portugal.
3. NOVA Medical School, Faculdade de Ciências Médicas, Universidade Nova de Lisboa - Lisbon, Portugal.
4. Intensive Care Unit, Hospital da Luz - Lisbon, Portugal.
* “Dear SIRS, I’m sorry to say that I don’t like you” was the title under which Jean-Louis Vincent (Crit Care Med. 1997;25(2):372-4), one of the most reputed European intensivists, expressed his views on concept systemic inflammatory response syndrome (SIRS).
Conflict of interest: None Submitted on July 25, 2016 Accepted on November 11, 2016
Corresponding author:
António Manuel Machado Henriques Carneiro Departamento de Medicina, Urgência e Cuidados Intensivos do Hospital da Luz Arrábida
Praceta Henrique Moreira, 150 4400-346 Vila Nova de Gaia, Portugal E-mail: [email protected]
Table 1 - Sepsis-1(2) and Sepsis-2(3) criteria
Sepsis-1
Sepsis is a systemic inflammatory response in the presence of infection
SIRS criteria
Temperature > 38°C or < 36°C
Heart rate > 90/minute
Respiratory rate > 20/minute (or PaCO2 < 32 mmHg)
WBC > 12,000/µL or < 4,000/µL (or > 10% immature bands)
Sepsis-2
General signs and symptoms Hemodynamic variables
Fever (central temperature > 38.3°C) Arterial hypotension (systolic < 90 mmHg, MAP < 70 mmHg, or systolic reduction > 40 mmHg in adults or < 2 SD of the normal value for age)
Hypothermia (central temperature < 36°C) SvO2 < 70%
Heart rate > 90/minute or > 2 SD above the normal value for age Cardiac index > 3.5 L/min/m2
Tachypnea Indicators of organ dysfunction
Edema or positive fluid balance (> 20 mL/kg 24 hours) Arterial hypoxemia (PaO2/FiO2 < 300)
Hyperglycemia (glycemia > 120 mg/dL) in the absence of diabetes Abnormal state of consciousness
Inflammation markers Acute oliguria (urine output < 0.5 mL/kg/hour)
Leukocytosis (> 12,000/µL) or leukopenia (< 4,000/µL) Elevated creatinine > 0.5 mg/dL
Normal leukocytes but > 10% immature bands Coagulation disorders (INR > 1.5/aPTT > 60 s)
Serum C-reactive protein > 2 SD above the normal value Thrombocytopenia (< 100,000/µL)
Plasma procalcitonin > 2 SD above the normal value Hyperbilirubinemia (> 4 mg/dL or 70 mmol/L)
Indicators of tissue perfusion
Hyperlactatemia (> 1 mmol/L)
Reduced capillary refill and mottled skin
SIRS - systemic inflammatory response syndrome; PaCO2 - partial pressure of carbon dioxide; WBC - white blood cells; SD - standard deviation; MAP - mean arterial pressure; SvO2 - venous
oxygen saturation; PaO2/FiO2 - partial pressure of oxygen/fraction of inspired oxygen; INR - international normalized ratio; aPTT - activated partial prothrombin time.
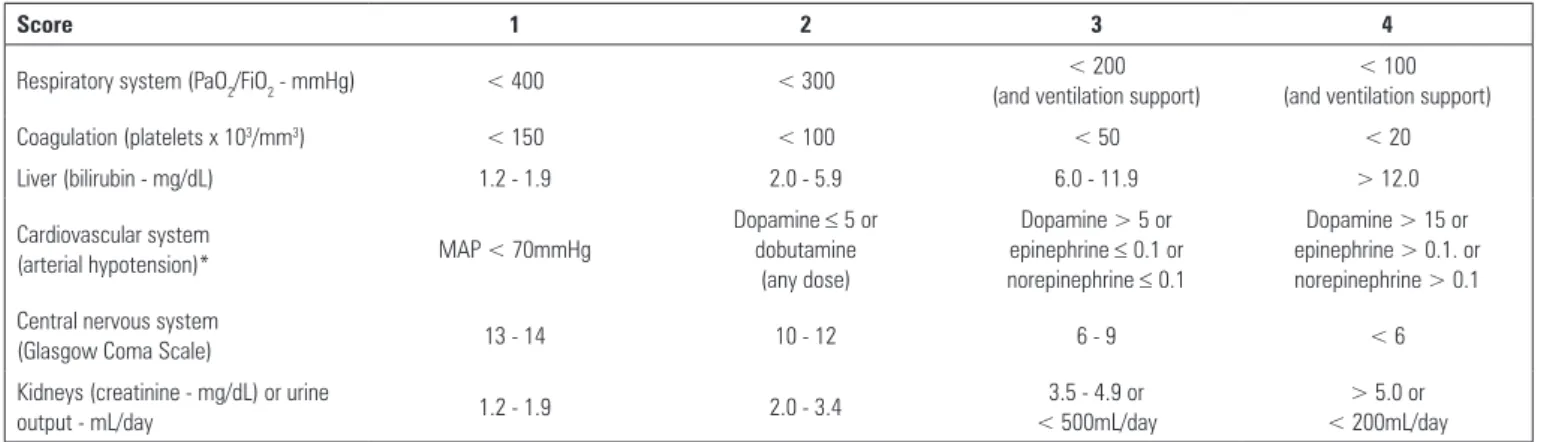
Table 2 - Sequential Organ Failure Assessment (SOFA) score(4)
Score 1 2 3 4
Respiratory system (PaO2/FiO2 - mmHg) < 400 < 300 < 200
(and ventilation support)
< 100 (and ventilation support)
Coagulation (platelets x 103/mm3) < 150 < 100 < 50 < 20
Liver (bilirubin - mg/dL) 1.2 - 1.9 2.0 - 5.9 6.0 - 11.9 > 12.0
Cardiovascular system
(arterial hypotension)* MAP < 70mmHg
Dopamine ≤ 5 or dobutamine
(any dose)
Dopamine > 5 or epinephrine ≤ 0.1 or norepinephrine ≤ 0.1
Dopamine > 15 or epinephrine > 0.1. or norepinephrine > 0.1
Central nervous system
(Glasgow Coma Scale) 13 - 14 10 - 12 6 - 9 < 6
Kidneys (creatinine - mg/dL) or urine
output - mL/day 1.2 - 1.9 2.0 - 3.4
3.5 - 4.9 or < 500mL/day
> 5.0 or < 200mL/day
* Adrenergic agents must be administered for ≥ 1 hour; doses are expressed as µg/kg/minute; PaO2/FiO2 - partial pressure of oxygen/fraction of inspired oxygen; MAP - mean arterial pressure.
Table 3 - Sepsis-3 criteria
qSOFA Septic shock
Respiratory rate ≥ 22/minute Systolic arterial pressure ≤ 100mmHg Altered mentation
Arterial hypotension requiring vasopressors to maintain mean arterial pressure ≥ 65mmHg and hyperlactatemia > 18mg/dL (2mmol/L) despite adequate vascular filling
he identiication of patients with this condition followed another method and used the Surviving Sepsis Campaign database (28,150 patients from 218 hospitals in 18 countries); this method employed the Sepsis-2 deinitions and clinical criteria for infection. he external validation was based on data from two large American hospitals. he criteria for septic shock became a cumulative presence of arterial hypotension (deined as the use of vasopressors) and hyperlactatemia (> 18mg/ dL or 2mmol/L) despite adequate volume resuscitation (Table 3).
We emphasize that the category “severe sepsis” was eliminated, which according to the previous criteria characterized septic patients with organ dysfunction and manifestations of hypoperfusion or arterial hypotension associated with sepsis that in prognostic terms had a mortality rate intermediate between sepsis and septic shock.
The controversy
he medical community became divided over the clinical value of the new criteria (i.e., regarding their actual impact and safety when applied at the bedside). he criticism mainly focused on the following three aspects: (1) underlying theoretical concepts; (2) the methods used to deine the criteria; and (3) their potential impacts on clinical practice.
Regarding the theoretical aspects, the criticism emphasized the oddity of applying diferent criteria to the suspicion and identiication of the same pathological phenomenon, which frequently exhibited the same clinical presentation, according to whether or not the patient was admitted to the ICU. he criticism stressed that the new criteria stemmed from a purely retrospective analysis of hospital databases created for completely diferent purposes, were quite limited in their geographic distribution, and deined for this particular objective, infection (i.e., a clinical concept) as a “collection of biological samples + prescription of antibiotics within a given time interval” (i.e., non-clinical concepts) and using physiological data collected in a manner that was not completely explained (i.e., the reliability of the Glasgow Coma Scale assessment or the respiratory rate, especially outside the ICU). Clearly, this criticism only applies to the development of the criteria for sepsis and not to the criteria for septic shock, which as mentioned above are based on another set of data.
Without downplaying the relevance of the irst two aspects, we believe that the future use of these criteria in
clinical practice (i.e., the potential clinical impact of their application at the bedside) is a cause of great concern. he Sepsis-3 criteria introduce no changes in the approach to sepsis, especially concerning antibiotic treatment, luid therapy, and vasopressor support, but neglect the early identiication of sepsis before the development of organ failure.
Relationship between the Sepsis-1 and Sepsis-2 criteria and the new Sepsis-3 criteria
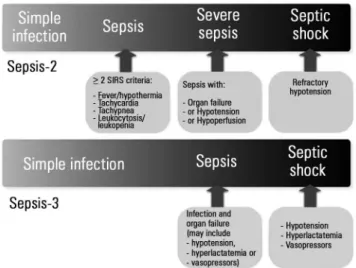
Following the Sepsis-3 criteria, the previous categorizations of the severity and consequent mortality due to infection that progressed from sepsis (infection meeting the criteria for systemic inlammatory response syndrome or SIRS) to severe sepsis (sepsis with organ failure, arterial hypertension, and/or hypoperfusion) to septic shock (arterial hypotension refractory to adequate volume resuscitation) were reduced to simple infection, sepsis (infection and manifestations of organ failure), and septic shock (arterial hypotension deined as the use of vasopressors and hyperlactatemia) (Figure 1). Sepsis-2 concept of severe sepsis roughly corresponds to the deinition of sepsis in the Sepsis-3 criteria, although this correlation is not absolute because sepsis, according to the new criteria, can include very diferent conditions, such as organ failure without hypotension nor hyperlactatemia, arterial hypotension even when vasopressors are used in any dose provided the lactate level is ≤ 18mg/dL (2mmol/L; i.e., vasoplegic shock), and also cryptic shock (hyperlactatemia without hypotension).(5-8)
he combination of the blood pressure values (or use of vasopressors after adequate volume resuscitation) and lactatemia has been long known to allow the identiication of patients with diferent severities and prognoses, which to date were systematized as follows:
1. Cryptic shock: deined as lactate concentration ≥ 4 mmol/L without arterial hypotension (or use of vasopressors).
2. Septic shock: hypotension induced by sepsis that persisted despite adequate volume resuscitation and might present as:
2.1. Vasoplegic shock: hypotension refractory to luid therapy with normal serum lactate.
2.2. Shock with tissue dysoxia: hypotension refractory to luid therapy with hyperlactatemia. he criteria deining the last group, which exhibits higher mortality, are the criteria the authors of Sepsis-3 considered necessary for the deinition of septic shock. In other words, the various phenotypic expressions of the severity of septic shock are not considered in Sepsis-3, because only dysoxic septic shock is taken into account and the vasoplegic and cryptic shock categories are ignored. he latter categories were classiied as sepsis.
Another major issue is whether we can undervalue the relevance of clinical manifestations that, according to the Task Force, are now called “infection” and that until recently were septic patients with diferent morbidities and mortalities. Besides, the mortality of these conditions is not negligible, as may be inferred from the tables published by the authors of the Sepsis-3 manuscript themselves.(9)
Do we need new criteria for sepsis?
As in every other situation, any change made should have a purpose. Are the previous criteria less useful and restrictive for the management of more severe infections? he clinical evidence points to the opposite situation. he ultimate goal of our action as physicians is to reduce morbidity and mortality.
he criteria for SIRS were the target of much criticism for having too high sensitivity but poor speciicity. In turn, the term “severe sepsis”, with its consequent organ dysfunction and/or tissue hypoperfusion and/or arterial hypotension associated with sepsis, was considered by several researchers (namely, the developers of Sepsis-3) to be the true onset of septic conditions.
From our perspective, the approach to sepsis should be grounded on three fundamental aspects that should be considered simultaneously and based on demonstrated
proof for its management and treatment as follows: (1) early recognition and stratiication of severity; (2) prevention of and support for organ dysfunction based on an optimal oxygen delivery; and (3) treatment of the cause and control of the infection site.
To attain these goals, the Surviving Sepsis Campaign (SSC) sets of documents are available. hese documents contain recommendations that indicate standardized, goal-oriented diagnostic and therapeutic actions according to the patient’s severity and response to treatment based on early identiication and stratiication of sepsis patients (Sepsis-2). hese recommendations were updated every four years, with the latest version published in 2013.(10)
Admittedly, the Sepsis-2/SSC partnership has an optimal record of success,(7,11,12) with a signiicant impact on
mortality by doing more with the available resources (i.e., without any new medication).
How should we ground our action in the face of infection?
We should always keep in mind that there is no pathophysiological aspect that is pathognomonic of sepsis and that the diagnosis of infection results from the intersection of three vectors (systemic manifestations, manifestations of organ dysfunction, and microbiological documentation), because no speciic marker is known at present.
In reality, we do not know whether the Sepsis-2 or the Sepsis-3 criteria best identify the most severe cases of infection that demand more timely therapeutic management. However, we fear that downplaying infectious conditions that do not meet the current Sepsis-3 criteria (i.e., the earliest cases and cases that have a less severe presentation) will hinder their identiication, resulting in an unnecessary increase in both morbidity and mortality due to their inexorable progression in the following hours. We admit that this risk is purely theoretical at present.
We anticipate that studies comparing the performance of both criteria in the real world will be conducted in the near future. Independent from their results, our approach to the patient with suspected infection should always be clinical. We should strive to achieve the identiication of the initial and sometimes subtle manifestations of organ failure and hypoperfusion in all patients with suspected infection; however, these manifestations are devalued in the Sepsis-3 criteria in favor of scores (SOFA and qSOFA).
the early stratiication of infection. When these criteria are followed by the application of the SSC recommendations, they have an impressive history of success in reducing the mortality of sepsis in several areas of the world.(5,11-13) he
authors of Sepsis-3 conclude their text by asserting, “hese updated deinitions and clinical criteria should clarify long-used descriptors and facilitate earlier recognition and more timely management of patients with sepsis or at risk
REFERENCES
1. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801-10.
2. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101(6):1644-55.
3. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM, Vincent JL, Ramsay G; International Sepsis Definitions Conference. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003;29(4):530-8.
4. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707-10.
5. Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Intensive Care Med. 2010;36(2):222-31.
6. Puskarich MA, Trzeciak S, Shapiro NI, Heffner AC, Kline JA, Jones AE; Emergency Medicine Shock Research Network (EMSHOCKNET). Outcomes of patients undergoing early sepsis resuscitation for cryptic shock compared with overt shock. Resuscitation. 2011;82(10):1289-93. 7. Sterling SA, Puskarich MA, Shapiro NI, Trzeciak S, Kline JA, Summers RL,
Jones AE; Emergency Medicine Shock Research Network (EMSHOCKNET). Characteristics and outcomes of patients with vasoplegic versus tissue dysoxic septic shock. Shock. 2013;40(1):11-4.
8. Ranzani OT, Monteiro MB, Ferreira EM, Santos SR, Machado FR, Noritomi DT; Grupo de Cuidados Criticos Amil. Reclassifying the spectrum of septic patients using lactate: severe sepsis, cryptic shock, vasoplegic shock and dysoxic shock. Rev Bras Ter Intensiva. 2013;25(4):270-8.
9. Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of Clinical Criteria for Sepsis: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):762-74. Erratum in: JAMA. 2016;315(20):2237.
10. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb S, Beale RJ, Vincent JL, Moreno R; Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165-228.
11. Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749-55. 12. Rhodes A, Phillips G, Beale R, Cecconi M, Chiche JD, De Backer D, et al.
The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence Study on Sepsis (the IMPreSS study). Intensive Care Med. 2015;41(9):1620-8.
13. Cardoso T, Carneiro AH, Ribeiro O, Teixeira-Pinto A, Costa-Pereira A. Reducing mortality in severe sepsis with the implementation of a core 6-hour bundle: results from the Portuguese community-acquired sepsis study (SACiUCI study). Crit Care. 2010;14(3):R83.
14. Antonelli M, DeBacker D, Dorman T, Kleinpell R, Levy M, Rhodes A. Surviving Sepsis Campaign Responds to Sepsis-3. March 1, 2016[ Internet]. [cited 2017 Jan 13]. Available from: http://www.survivingsepsis.org/ SiteCollectionDocuments/SSC-Statements-Sepsis-Definitions-3-2016.pdf.