Instituto do Coração do Hospital das Clínicas - FMUSP
Mailing address: Noedir A. G. Stolf Rua João Lourenço, 386 04508030 São Paulo, SP - Brazil
Objective – Assessment of incidence and behavior of mediastinitis after cardiac transplantation.
Methods – From 1985 to 1999, 214 cardiac trans-plantations were performed, 12 (5.6%) of the transplanted patients developed confirmed mediastinitis. Patient’s ages ranged from 42 to 66 years (mean of 52.3±10.0 years) and 10 (83.3%) patients were males. Seven (58.3%) patients showed sternal stability on palpation, 4 (33.3%) patients had pleural empyema, and 2 (16.7%) patients did not show purulent secretion draining through the wound.
Results – Staphylococcus aureus was the infectious agent identified in the wound secretion or in the mediasti-num, or both, in 8 (66.7%) patients. Staphylococcus
epider-midis was identified in 2 (16.7%) patients, Enterococcus faecalis in 1 (8.3%) patient, and the cause of mediastinitis
could not be determined in 1 (8.3%) patient. Surgical treat-ment was performed on an emergency basis, and the ex-tension of the débridement varied with local conditions. In 2 (16.7%) patients, we chose to leave the surgical wound open and performed daily dressings with granulated sugar. Total sternal resection was performed in only 1 (8.3%) patient. Out of this series, 5 (41.7%) patients died, and the causes of death were related to the infection. Autopsy revealed persistence of mediastinitis in 1 (8.3%) patient.
Conclusion - Promptness in diagnosing mediastinitis and precocious surgical drainage have changed the natu-ral evolution of this disease. Nevertheless, observance of the basic precepts of prophylaxis of infection is still the best way to treat mediastinitis.
Key words: mediastinitis, cardiac transplantation, immu-nosuppression
Arq Bras Cardiol, volume 74 (nº 5), 425-430, 2000
Noedir A. G. Stolf, Alfredo I. Fiorelli, Fernando Bacal, Luiz F. Camargo, Edimar A. Bocchi, Andréa Freitas, André Nicoletti, Daniela Meira
São Paulo, SP - Brazil
Mediastinitis after Cardiac Transplantation
In spite of developments in cardiac transplantation, re-jection and infection still constitute the major challenges for improving the results of that procedure, because they are the main causes of morbidity and mortality in the first mon-ths following transplantation 1. Infections delay postopera-tive recovery and are present in the majority of the compli-cations that cause transplantation failure. In other situati-ons, infection only represents the final ordinary via of the poor evolution of the patient operated upon.
Severity and frequency of infection are directly related to the degree of immunosuppression and intraoperative conditions. Different factors, such as associated diseases, the clinical status of the recipient and of the donor, the refi-nement of the surgical technique, and the conditions of the surgical environment, influence the transmission of infecti-ous agents.
Prevention is still one of the most important measures in the combat of complications of the surgical wound. Ho-wever, after infection is established, precocity in its diagno-sis, identification of the pathogen, and immediate applicati-on of the effective therapy capplicati-ontribute to solving the pro-blem. It is worth emphasizing, however, that immunosup-pression makes these patients more susceptible to invasion by microorganisms.
In conventional cardiac surgeries, the incidence of me-diastinitis has been reported to range from 0.4% to 8.0%, with a mortality rate of about 30% 2. In transplantation this complication is especially feared because of the resulting high mortality rate. The treatment of mediastinitis has impro-ved in recent years because of expansion of the available sources for investigation, allowing a reduction in the time re-quired for diagnosis and treatment 2-4.
This study aims to report the experience acquired in the treatment of patients developing mediastinitis after car-diac transplantation in the last 14 years.
Methods
analysis of this case series showed that 12 (5.6%) patients developed sternal osteomyelitis or mediastinitis, or both, in the postoperative period, therefore requiring cleaning and surgical drainage.
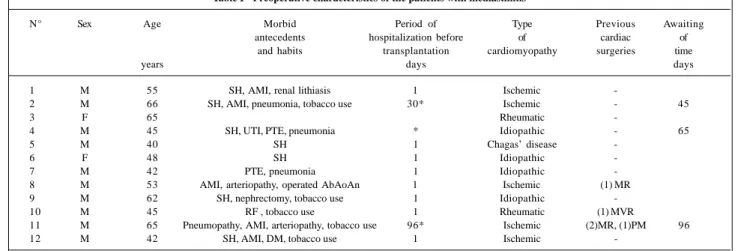
Patients’ ages ranged from 42 years to 66 years (mean of 52.3±10.0). Ten (83.3%) patients were males. In regard to the etiology of the heart disease requiring trans-plantation, it was ischemic in 5 (41.7%) patients, idiopathic in 4 (33.3%), rheumatic in 2 (16.7), and Chagas’ disease in 1 (8.3%) patient.
Seven (58.3%) patients had systemic hypertension, 4 (33.3%) patients had previous acute myocardial infarction, 4 (33.3%) experienced at least one episode of controlled in-fection, 4 (33.3%) experienced pulmonary thromboembo-lism, 2 (16.7%) showed signs of peripheral arteriopathy, and 5 (41.7%) were current or previous tobacco users.
Two (16.7%) patients had previously undergone myo-cardial revascularization, one of whom (8.3%) had undergo-ne 2 revascularizations and oundergo-ne pacemaker implantation. Another (8.3%) patient had undergone replacement of the mitral valve with a bovine pericardium bioprosthesis.
Two (16.7%) patients were in severe cardiogenic sho-ck and, consequently, transplantation was immediately per-formed.
Donor’s ages ranged from 37 years to 50 years (mean of 41±6.7). None of the donors had an active infectious or contagious disease and serum assessments for Chagas’ disease, syphilis, hepatitis, and acquired immunodeficiency syndrome were negative.
Table I shows the main characteristics of the patients studied who had mediastinitis after cardiac transplantation. In this study, we did not consider those patients with superficial infections of surgical wounds, only those with deep infection with or without spontaneous drainage of puru-lent secretion, involving the sternum or the mediastinum, or both, that required a reopening of the surgical incision.
The diagnosis of mediastinitis was considered
posi-tive when one of the following criteria adopted by the Com-mittee of Control of Hospital Infection at Incor was met: 1) positive culture of the mediastinal or sternal tissue or of the pericardial fluid obtained through aspiration biopsy or du-ring surgery; 2) evidence of mediastinitis or osteomyelitis through direct examination during surgery or in the histopa-thological examination; 3) existence of one of the following parameters without any known cause: fever higher than 38.0°C, thoracic pain, sternal instability associated with pu-rulent drainage of the sternum or mediastinum, positive blo-od culture, positive culture of the material drained from the sternal or mediastinum, enlargement of the mediastinum on radiological examination, and presence of fluid collection detected through computed tomography.
Antibiotic prophylaxis after transplantation was per-formed in the first 2 (16.7%) patients with 2g of cefoxitin and 2g of oxacillin by intravenous via, initiated in the anes-thetic induction and repeated every 6 hours until 8 doses were completed. In the remaining patients, 1.5g of cefuroxi-me was employed through intravenous via, started 2 hours before the surgery and repeated every 12 hours for 5 doses. Immunosuppression and management of the rejection episodes followed the same protocol previously published 5. Blood was withdrawn from donors for serum assessment of cytomegalovirus and toxoplasmosis after transplantation.
Antibiotic therapy was initially applied and modified, whenever possible, according to the sensitivity of the infec-tious agent and the clinical response of the patient. Empiri-cal administration, however, was reserved for special situa-tions of clinical severity, while identification of the pathogen was awaited.
Once the diagnosis of mediastinitis was established, the surgical treatment was immediately performed on an emergency basis. During surgery, we tried to determine the extension of the infectious process and to remove all necro-tic tissue, after which we washed exhaustively the surgical wound with saline solution and povidone iodine (PVPI). In
Table I - Preoperative characteristics of the patients with mediastinitis
N° Sex Age Morbid Period of Type Previous Awaiting
antecedents hospitalization before of cardiac of and habits transplantation cardiomyopathy surgeries time
years days days
1 M 55 SH, AMI, renal lithiasis 1 Ischemic
-2 M 66 SH, AMI, pneumonia, tobacco use 30* Ischemic - 45
3 F 65 Rheumatic
-4 M 45 SH, UTI, PTE, pneumonia * Idiopathic - 65
5 M 40 SH 1 Chagas’ disease
-6 F 48 SH 1 Idiopathic
-7 M 42 PTE, pneumonia 1 Idiopathic
-8 M 53 AMI, arteriopathy, operated AbAoAn 1 Ischemic (1) MR
9 M 62 SH, nephrectomy, tobacco use 1 Idiopathic
-10 M 45 RF , tobacco use 1 Rheumatic (1) MVR
11 M 65 Pneumopathy, AMI, arteriopathy, tobacco use 96* Ischemic (2)MR, (1)PM 96
12 M 42 SH, AMI, DM, tobacco use 1 Ischemic
all cases, continuous irrigation with 5% PVPI in saline solu-tion for 5 to 7 days was maintained.
Results
Total time for transplant surgery ranged from 4 hours and 50 minutes to 12 hours, with a mean of 7.6±2.1 hours; in 1 patient with previous cardiac surgeries this time was prolonged due to damage to the right ventricle during sternotomy. The period of use of the thoracic drains ranged from 3 to 5 days, with a mean of 3.7±0.7 days.
Six (50.0%) patients received intravenous pulse thera-py to control acute rejection before the manifestations of mediastinitis.
At the time of diagnostic confirmation of mediastinitis, 8 (66.7%) patients had a body temperature higher than 37.5°C, and only 2 (16.7%) patients did not develop leuko-cytosis.
Seven (58.3%) patients showed no sternal instability on palpation, 4 (33.3%) had signs of pleural empyema, and 2 (16.7%) did not show drainage of purulent secretion through the surgical incision. One (8.3%) patient evolved with severe thoracic pain, as an isolated manifestation 4 da-ys before confirmation of the diagnosis of mediastinitis.
Table II shows clinical and laboratory findings of the patients at the time the diagnosis of mediastinitis was esta-blished.
Staphylococcus aureus was the infectious agent
iden-tified in the secretions of the incision, of the mediastinum, or in both, of 8 (66.7%) patients; Staphylococcus epidermidis was found in 2 (16.7%) patients; Enterococcus faecalis in 1 (8.7%) patient; and in 1 (8.7%) patient the cause could not be determined.
In 2 (16.7%) patients, the infectious agent of mediasti-nitis was also isolated in the blood stream. All patients had other associated infectious foci. In 2 (16.7%) patients, 2 concomitant agents were identified in the mediastinal secre-tion. Table III shows the distribution of the agents causing
mediastinitis, the associated infections, and the antibiotic therapy employed.
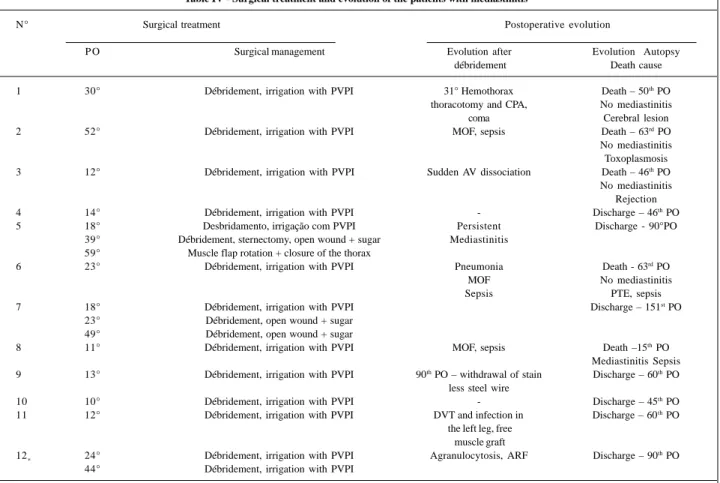
Once the diagnosis of mediastinitis was established, surgical treatment was performed on an emergency basis, from the 11th to the 52nd day of the posttransplantation pe-riod, with a mean of 19.8±11.9 days. Extension of débride-ment was directly proportional to the extension of infection observed during surgery. Total sternotomy was performed only in 1 (8.3%) patient due to the advanced stage of osteo-myelitis. In 2 (16.7%) patients, we decided to keep the surgi-cal wound open and apply daily dressings of granulated sugar.
In 3 (25.0%) patients, we had to repeat the débridement because of persistent infection. However, in case 12 (8.3%), reoperation on the 44th postoperative day was indicated because of persistent fever and worsening of the clinical fin-dings; signs of active mediastinitis, however, were not found and the culture of the material collected locally was negative. Two (16.7%) patients were readmitted because of recrudescence of infection.
In our series, 5 (41.7%) patients died and their causes of death were somehow related to infection. Autopsy sho-wed persistent mediastinitis in only 1 patient (case 8).
Table IV shows the surgical management and evolu-tion of the patients.
Discussion
Mediastinitis substantially changes the natural evolu-tion of the patients in the postoperative period because of high rates of morbidity and mortality. It also prolongs hospi-talization and increases hospital costs 6. Precocious diag-nosis and prompt surgical treatment prevent infectious dis-semination and its frequently devastating sequelae.
Incidence of mediastinitis in conventional cardiac sur-geries has not shown a high frequency, usually lower than 1%, even though during the ‘80s, the mortality rate attribu-ted to this entity ranged from 14% to 47% 1,7. Recently, the
Table II - Clinical and laboratory findings of the patients developing mediastinitis
N° Surgery duration Duration of Rejection *Clinical and laboratory findings
thoracic before T °C Leukocyte counting Sternum Purulent secretion
hours drainage mediastinitis Incision Mediastinum Pleura
days
1 4:50 3 3-B 36.5 14 300 unstable No Yes Yes
2 6:40 4 - 38.0 16 400 stable Yes Yes No
3 6:00 4 1-A 38.0 18 900 stable Yes Yes No
4 7:00 3 - 37.5 14 700 stable Yes Yes No
5 7:30 3 3-B 37.5 11 000 unstable Yes Yes Yes
6 4:30 3 3-A 36.5 8 100 stable Yes Yes No
7 7:50 3 3-A 37.5 15 900 unstable Yes Yes No
8 7:30 5 - 38.0 12 000 stable Yes Yes Yes
9 10:00 3 1-A and 1-B 36.5 23 500 unstable Yes Yes No
10 9:00 4 3-A 36.5 22 600 stable Yes Yes No
11 12:00** 4 1-B 37.5 16 600 unstable No Yes Yes
12 8:00 3 3-A 38.0 7 300 stable Yes *** Yes No
Table III - Diagnosis of mediastinitis and antibiotic therapy
N° Identification of the infectious agent Associated Antibiotic therapy infection during mediastinitis Blood Incision and/or mediastinum
1 - S. epidermidis Pneumonia Cefoxitin, clindamycin,
Oral candidiasis cefoxitin PM site
2 - S. aureus Toxoplasmosis Vancomycin, cefoxitin
CMV, sepsis
3 - - Pneumonia Cefoxitin, clindamycin,
CMV, UTI cefoxitin
4 - S. aureus Empyema Vancomycin, clindamycin,
Sepsis ceftazidime, ceftriaxone
5 S. epidermidis S. epidermidis Empyema Vancomicina, cefoxitina
Oral herpes candidiasis
Oral
6 - S. aureus Candida Vancomycin, fluconazole,
Enterobacter sp sepsis neomycin
7 - E. faecalis Oral candidiasis Vancomycin, ciprofloxacin,
P. aeruginosa aztreonam, clindamycin
8 - S. aureus Empyema Vancomycin, clindamycin,
ceftazidime, ceftriaxone
9 - S. aureus Pneumonia Vancomycin, cefuroxime
10 S. aureus S. aureus Pneumonia Vancomicina, cefuroxima
11 - S. aureus Left leg Vancomycin, ciprofloxacin
12 - S. aureus Pneumonia Vancomycin, clindamycin, ceftazidime
E- Enterococcus; P- Pseudomonas; S- Staphylococcus; PM- pacemaker; UTI- urinary tract infection; CMV- cytomegalovirus.
Table IV - Surgical treatment and evolution of the patients with mediastinitis
N° Surgical treatment Postoperative evolution
P O Surgical management Evolution after Evolution Autopsy
débridement Death cause
1 30° Débridement, irrigation with PVPI 31° Hemothorax Death – 50th PO thoracotomy and CPA, No mediastinitis
coma Cerebral lesion
2 52° Débridement, irrigation with PVPI MOF, sepsis Death – 63rd PO
No mediastinitis Toxoplasmosis 3 12° Débridement, irrigation with PVPI Sudden AV dissociation Death – 46th PO
No mediastinitis Rejection
4 14° Débridement, irrigation with PVPI - Discharge – 46th PO
5 18° Desbridamento, irrigação com PVPI Persistent Discharge - 90°PO
39° Débridement, sternectomy, open wound + sugar Mediastinitis 59° Muscle flap rotation + closure of the thorax
6 23° Débridement, irrigation with PVPI Pneumonia Death - 63rd PO
MOF No mediastinitis
Sepsis PTE, sepsis
7 18° Débridement, irrigation with PVPI Discharge – 151st PO
23° Débridement, open wound + sugar 49° Débridement, open wound + sugar
8 11° Débridement, irrigation with PVPI MOF, sepsis Death –15th PO
Mediastinitis Sepsis 9 13° Débridement, irrigation with PVPI 90th PO – withdrawal of stain Discharge – 60th PO
less steel wire
10 10° Débridement, irrigation with PVPI - Discharge – 45th PO
11 12° Débridement, irrigation with PVPI DVT and infection in Discharge – 60th PO the left leg, free
muscle graft
12* 24° Débridement, irrigation with PVPI Agranulocytosis, ARF Discharge – 90th PO 44° Débridement, irrigation with PVPI
mortality rate has dropped to figures lower than 10%, even in cases of cardiac transplantation 2,8. In our study, the inci-dence of mediastinitis and its mortality confirmed the seve-rity of that entity, which was observed by other authors 3, 6,8. Grossi et al 7, in an analysis of 7,949 patients under-going cardiac operations, observed that only 0.97% of pa-tients developed mediastinitis. They identified the following as risk factors: associated operative procedures, bleeding, low cardiac output, and prolonged mechanical ventilation.
Karwande et al 8 found mediastinitis in 2.8% of pati-ents after cardiac transplantation and a mortality rate of 8.3%. On the other hand, Albat et al 9 reduced the incidence of mediastinitis after transplantation with a reduction in corticoids.
Lack of uniformity in the results found in the literature occurs, among other causes, because of the different defini-tions attributed to the extension of the infection in the ope-rative wound. Complications of sternotomy vary from small sterile dehiscence to suppurative mediastinitis with severe systemic involvement. The terms mediastinitis and sternal osteomyelitis are frequently used as synonyms to refer to deep infection of the surgical wound. However, deep infec-tions confined to the subcutaneous and muscular tissues without bone involvement, usually have a benign evolu-tion. Considering these facts, in our series we adopted well-defined criteria of case selection to make the analysis of the results obtained easier.
Cardiac transplantation is considered a clean surgery; however, it facilitates the development of microorganisms because of the extensive surgical aggression and immuno-suppression. Gram positive bacteria are the most commonly isolated agents. The incidence of Staphylococcus aureus and of Staphylococcus epidermidis in our series of patients is in accordance with the observations of other authors in whose series those pathogens accounted for more than 80% of the cases of mediastinitis 7,10. Gram negative bacteria and fungi are rarely found and mixed infections are reported in about 40% of the cases 11, 12.
Concomitance of different pathogens observed in our series may have been facilitated by immunosuppression, which predisposes to hematogenic dissemination. Identifi-cation of Toxoplasma gondii in the mediastinum at autopsy of one patient was attributed to the extensive dissemination of toxoplasmosis, and it was not considered the causative agent of the mediastinitis.
The beginning of mediastinitis and its sequential evo-lution are not easily characterized because different factors influence the pathogenesis of that entity. Inappropriate drainage of the mediastinum resulting in maintenance of se-rosanguineous collections in the retrosternal space predis-poses to colonization and propagation of microorganisms. In other situations, bone instability and skin disruption are the factors predisposing to infection. Usually, in the preco-cious phases, osteomyelitis is confined to local tissues and sternal instability, which appears in a few days, reflects the advanced stage of the infection. Chronic mediastinitis that
occurs a few weeks after operation is characterized by fistu-lae or circumscribed collections and provides an opportu-nity for treatment with more satisfactory results 13.
This latter observation seems to have significantly in-fluenced the evolution of the patients studied because control of the infection was easier in those patients in whom the mediastinitis appeared in the 2nd or 3rd week after trans-plantation. In this subgroup of patients, other factors, such as preexisting clinical conditions, precocity of reinterven-tion, intensity and virulence of the aggressive agent, may have positively influenced and helped to block the infec-tious process.
Mediastinitis maintained its local activity in only 8.3% of the patients; in the remaining patients, remission occur-red, even in those who eventually died, in whom the autop-sy identified organization of the process. This suggests that the treatment applied was effective in subduing the lo-cal infection.
The major risk factors for the development of infections in the mediastinum are the following: tobacco use, pneu-mopathies, prolonged preoperative hospital stay, inappro-priate preparation of the skin for surgery, bleedings, reope-rations, prolonged intubation, and immunosuppression 1,2,7. Identification of these factors and the refinement of the ope-rative technique constitute important tools in the preven-tion of postoperative infecpreven-tions. Surgical precaupreven-tions range from sternotomy with adequate hemostasis to the rational use of the electrocautery and bone wax 10,11.
Classical signs and symptoms of acute infection usually found in mediastinitis may be masked by the tho-racic pain proper of the postoperative period or other asso-ciated infections. Suppuration through the incision and sternal instability that characterize mediastinitis do not always appear as the first manifestations of infection, as occurred in 83.3% and 41.6%, respectively, of the cases stu-died. In different experiences, those manifestations have been reported with an incidence of up to 90% 7,8.
In the present study, the low incidence of sternal insta-bility may have resulted from the precocity of the surgical treatment, which did not allow time for bone involvement.
Only 1 patient had severe thoracic pain as an isolated manifestation for 4 days, before confirmation of the clinical finding of mediastinitis could be established. Fever and leu-kocytosis, which are frequently found in infectious proces-ses, were present in the initial phase of the diagnosis of me-diastinitis in 66.7% and 83.3% of the patients, respectively. Daily clinical carefull follow-up provides the best means for identifying mediastinitis because laboratory in-vestigation is not specific and only supports the clinical suspicion. Blood cultures were positive in 16.7% of the patients studied. Kohman et al12 found bacteremia in 59.2% of the patients developing mediastinitis after myocardial re-vascularization. Immunosuppression certainly changes the natural inflammatory response observed in mediastinitis.
analysis of echocardiography and computed tomography provides substantial information concerning the appearance of pericardial or retrosternal collections because transplanta-tion significantly modifies mediastinal anatomy 3. It should be emphasized that more important than isolated analysis of a single examination is the daily clinical observation asso-ciated with clinical and laboratory findings.
The treatment of mediastinitis as applied in this study varies from a very simple débridement, partial or total re-section of the sternum, to more complex procedures with ro-tation of muscle flaps 7,9,13. Isolated antibiotic therapy and surgical cleaning were not used in any situation and are not accepted in the current practice.
The technique of débridement and primary closure of the sternum with continuous antibiotic irrigation of the me-diastinum was initially and successfully described by Shu-macker and Mandelbaum 14 in 1963 in the treatment of mediastinitis caused by Staphylococcus after cardiac sur-gery. Irrigation with antibiotics or 0.5% iodine solution have significantly reduced mortality rates due to mediastinitis, even though morbidity and mortality rates are still high in that affliction 15. Irrigation in its different forms aims to me-chanically clean and remove necrotic material.
Use of muscle flaps or epiploon has been controver-sial, and surgical aggression and opportunities for using this technique should be considered 15-17. In our patients, the
orientation adopted has always been directed at an initial débridement of necrotic tissues, multiple drainage of the me-diastinum and thoracic cavity, primary closure of the ster-num and maintenance of continuous irrigation with a solution of 0.5% povidone iodine for 5 to 7 days.
The surgical wound was maintained open in 16.7% of the patients. These were special situations in which failure in the primary treatment or extensive sternal involvement oc-curred requiring wide bone resections. These patients were removed from the prolonged mechanical ventilation after recovery of the general clinical condition and the sur-gical wounds were kept open. This favors cleaning and drainage of the secretions, avoids dissemination of the infection and helps healing. Compressing the thorax with bandages allows approximation of the sternum resulting in wound healing. Rotation of the rectus abdominis muscle was employed in one case with total sternal resection.
In conclusion, treatment of mediastinitis is still a major challenge for the medical team because that entity drastica-lly changes the postoperative evolution of cardiac trans-plantation and may leave sequelae. The early diagnosis and precocious reintervention have modified the natural evolu-tion of that process. However, observaevolu-tion of the basic pre-cepts of infectious prophylaxis still constitutes the best way to treat mediastinitis.
1. Maria R, Minoli L, Parolini M, et al. Prognostic determinants of six-month morbi-dity and mortality in heart transplant recipients. The Italian Study Group on Infection in Heart Transplantation. J Heart Lung Transplant 1996; 15:124-35. 2. Culliford AT, Cunningham JN, Zeff RH, Isom OW, Teiko P, Spencer FC. Sternal and costchondral infections following open-heart surgery. A review of 2594 cases. J Thorac Cardiovasc Surg 1976; 72: 714-26.
3. MisawaY, Fuse K, Hasegawa T. Infections mediastinitis after cardiac operations: computed tomographic findings. Ann Thorac Surg 1998; 65: 622-4. 4. Quirce R, Serano J, Arnal C, Banzo I, Carril JM. Detection of mediastinitis after
heart transplantation by gallium-67 scintigraphy. J Nucl Med 1991; 32: 860-1. 5. Fiorelli AI, Stolf NAG. Cuidados no pós-operatório do transplante cardíaco. Rev
Bras Cir Cardiovasc 1996; 11: 30-8.
6. ReeceIJ, Painvin A, Chandler LB, et al. Infection after cardiac transplantation: treatment and prognosis. Texas Heart Institute J 1984; 11: 32-7.
7. Grossi EA, Culliford AT, Krieger KH, et al. A survey of 77 major infectious com-plications of median sternotomy: a review of 7 949 consecutive operative proce-dures. Ann Thorac Surg 1985; 40: 214-23.
8. Karwande SV, Renlund DG, Olsen SL, et al. Mediastinitis in heart transplantati-on. Ann Thorac Surg 1992; 54: 1039-45.
9. Albat B, Trinh Duc P, Boulfroy D, Picard E, Wintrebert P, Thevenet A.
Mediasti-nitis in heart transplant recipients: successful treatment by closed local irriga-tion. Cardiovasc Surg 1993; 1: 657-9.
10. Demmy TL, Park SB, Liebler GA, et al. Recent experience with major sternal wound complications. Ann Thorac Surg 1990; 49: 458-62.
11. Sarr MG, Gott VL, Townsend TR. Mediastinal infection after cardiac surgery. Ann Thorac Surg 1984; 38: 415-23.
12. Kohman LJ, Coleman MJ, Parker FB. Bacteremia and sternal infection after coro-nary artery bypass grafting. Ann Thorac Surg 1990; 49: 454-7.
13. Majure JA, Albin RE, O’Donnell RS, Arganese TJ. Reconstruction of the infected median sternotomy wound. Ann Thorac Surg 1986; 42: 9-12.
14. Shumacker HB, Mandelbaum I. Continuous antibiotic irrigation in the treatment of infection. Arch Surg 1963; 86: 384-7.
15. Acinapura AJ, Godfrey N, Romita M, et al. Surgical management of infected median sternotomy: closed irrigation vs. Muscle flaps. J Cardiovasc Surg 1985; 26:443-6. 16. Scully HE, Leclerc Y, Martin RD, et al. Comparison between antibiotic irrigation and mobilization of pectoral muscle flaps in treatment of deep sternal infection. J Thorac Cardiovasc Surg 1985; 90: 523-31.
17. Pervosti LG, Subramainian A, Rothaus KO, Dineen P. A comparison of the open and closed methods in the initial treatment of sternal wound infections. J Cardio-vasc Surg 1989; 30: 757-63.