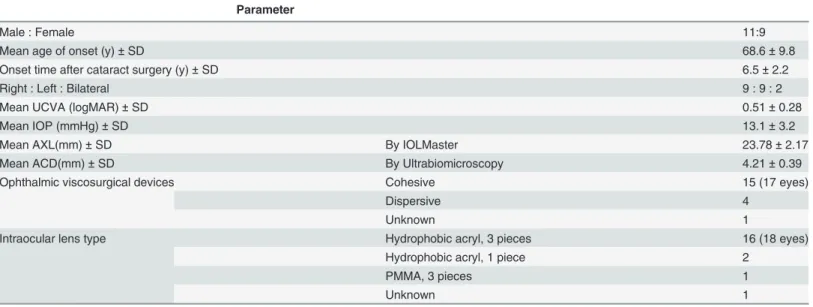
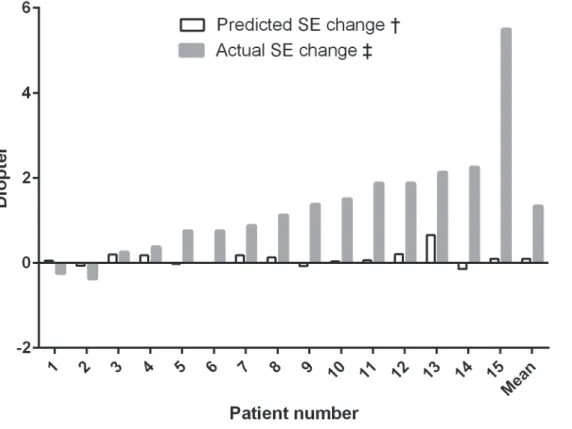
Anterior chamber depth and refractive change in late postoperative capsular bag distension syndrome: a retrospective analysis.
Texto
Imagem

Documentos relacionados
Representation of late horizontal repositioning measures: distances measured from reference points between early postoperative tracings (in red) and late postoperative tracings
Postoperative atrial fibrillation occurred in two (8%) patients of the Control Group and in three (12%) patients who underwent ventral cardiac denervation.. The risk of
Purpose: To investigate the relationship between biomechanical properties of the cornea and postoperative refractive changes in patients with low-level astigmatism after
In the present study, we found clear evidence of lipid peroxidation in erythrocytes from patients with schistosomiasis mansoni, who had undergone clinical and surgical treatment,
In this retrospective study, peripapillary choroidal thickness parameters in 34 eyes of 34 patients who had undergone diseased-eye evisceration between March 2014 and May 2016
In the present study, we evaluated the clinical characteristics and response to treatment with corticosteroids in adult patients with proteinuria and histological diagnosis of MCD
Objective: Aim of this study was to evaluate the clinical and urodynamic results in patients who had undergone orthotopic bladder substitution with ileocaecal (Mainz pouch procedure)
In this retrospective analysis, we identified the clinical characteristics, including molecular subtypes, and treatment outcomes associated with the prognosis of pediatric patients
