REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
MISCELLANEOUS
Correlation
of
bispectral
index
(BIS)
monitoring
and
end-tidal
sevoflurane
concentration
in
a
patient
with
lobar
holoprosencephaly
Dario
Galante
a,∗,
Donatella
Fortarezza
a,
Maria
Caggiano
a,
Giovanni
de
Francisci
b,
Dino
Pedrotti
c,
Marco
Caruselli
daUniversityDepartmentofAnesthesiaandIntensiveCare,UniversityHospitalOspedaliRiunitiofFoggia,Italy
bDepartmentofAnesthesiaandIntensiveCare,AgostinoGemelliHospital,CatholicUniversityoftheScaredHeart,Rome,Italy cDepartmentofAnesthesiaandIntensiveCare,S.ChiaraHospital,Trento,Italy
dDepartmentofAnesthesiaandIntensiveCare,LaTimoneChildren’sHospital,Marseille,France
Received27March2014;accepted3July2014 Availableonline25October2014
KEYWORDS
Holoprosencephaly;
Bispectralindex;
Sevoflurane; Seizures
Abstract
Objective: Thebispectralindex(BIS)isaparameterderivedbyelectroencephalography(EEG) whichprovidesadirectmeasurementoftheeffectsofsedativesandanestheticsonthebrain andoffersguidanceontheadequacyofanesthesia.TheliteraturelacksstudiesonBISmonitoring inpediatricpatientswithcongenitalbraindiseaseundergoinggeneralanesthesia.
Clinicalfeatures:A13-year-oldchildweighing32kg,sufferingfromlobarholoprosencephaly, underwentsurgeryinwhichthebispectralindex(BIS)monitoringthedepthofanesthesiashowed anabnormalresponse.DetailedanalysisofthetrendsofBISvaluesinthedifferent observa-tiontimesdemonstratedsuddenfallsandrepetitivevaluesofBISlikelyrelatedtorepetitive epileptiformelectricalactivitycausedbysevoflurane.
Conclusion: TheBISisaveryusefulmonitoringtoolforassessingthedegreeofdepthof anesthe-siaandtoanalyzetheelectroencephalographicvariationsofanesthetics.Particularattention shouldbegiventopatientswithcongenitaldisordersofthecentralnervoussysteminwhich theBISmaygiveabnormalresponsesthatdonotreflectanaccurateassessmentofthedepth ofanesthesia.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mail:[email protected](D.Galante). http://dx.doi.org/10.1016/j.bjane.2014.07.003
PALAVRAS-CHAVE
Holoprosencefalia;
Índicebispectral;
Sevoflurano; Convulsões
Correlac¸ãoentremonitorac¸ãodoíndicebispectral(BIS)econcentrac¸ãoexpiradade sevofluranoempacientecomholoprosencefalialobar
Resumo
Objetivo:Oíndice bispectral(BIS) éum parâmetroderivadopor eletroencefalografia(EEG) queforneceumamedidadiretadosefeitosdesedativoseanestésicosnocérebroeorientac¸ão sobreaadequac¸ãodaanestesia.Aliteraturacarecedeestudossobreamonitorac¸ãodoBISem pacientespediátricoscomdoenc¸acerebralcongênitasubmetidosàanestesiageral.
Característicasclínicas: Crianc¸a de13anosdeidade,pesando32kg,comholoprosencefalia lobar,foisubmetidaàcirurgiaemqueamonitorac¸ãodaprofundidadedaanestesiacomouso doBISmostrouumarespostaanormal.AanálisedetalhadadastendênciasdosvaloresdoBISnos diferentestemposdeobservac¸ãomostrouquedassúbitasevaloresrepetitivosdoBIS, provavel-menterelacionadosàatividadeelétricaepileptiformerepetitivacausadaporsevoflurano. Conclusão:OBISéumaferramentademonitorac¸ãomuitoútilparaavaliarograude profundi-dadedaanestesiaeasvariac¸õeseletroencefalográficasdosanestésicos.Atenc¸ãoespecialdeve serdedicadaaospacientescomdoenc¸ascongênitasdosistemanervosocentralnosquaisoBIS podeapresentarrespostasanormaisquenãorefletemaavaliac¸ãoprecisadaprofundidadeda anestesia.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Holoprosencephaly
Holoprosencephaly(HPE)is acomplexbrain malformation
inwhichthereisanincompleteseparationoftheforebrain
betweenthe18thand28thdayofintrauterinelife,affecting
boththe forebrainandtheface,causing neurologicaland
facialdefectsofvaryingseverity.1
Ithasaprevelanceof1in250duringearlyembryo devel-opment,and1in10,000to1in20,000atterm.
Three classic forms of progressive severity have been described, classified according to their anatomical fea-tures:HPElobar,semi-lobar,andalobar.Amildersubtype, knownasmiddle interhemisphericvariant (MIH), wasalso identified. The HPE phenotype also includes aprosence-falia/atelencefalia(the most severe sign),schizencephaly andsepto-preopticHPE.The lesssevereformsaredefined microforms,characterizedbydefectsinthemidline,inthe absenceofbrainmalformationtypicalofHPE.However,the diseaseischaracterizedbyacontinuousspectrumof abnor-malseparation of thecerebral hemispheres ratherthana distinctsubdivisionoftheseformswhichpresent,however, significantinclinicalinter-andintra-familialvariability.In manycases,thereisacorrelationbetweentheseverityof facialabnormalitiesandbrainanomaly(withtheexception of mutationcases in the ZIC2 gene). In descending order of severity the main facial features are cyclopia, a pro-boscis,premaxillaryagenesis,acleftlip,coloboma,retinal dysplasia,choanalstenosis, stenosisofthepyriformsinus, hypotelorism, asingle median maxillary incisor,and even anormalface.Severeforms(especiallyinthepresenceof achromosomalabnormality)areoften fatalandmortality is associated withthe severity of the brain malformation and associated defects. In children who survive, a broad
spectrumofrelatedsignshasbeendescribed: developmen-tal delay,hydrocephalus, motordeficits, eatingproblems, motordysfunction,epilepsy,andhypothalamicdysfunction. Endocrine disorders from pituitary abnormalities, such as centraldiabetes,arecommon.
Lobar holoprosencephaly is the milder classic form of holoprosencephaly. It is characterized by the separation between the leftand right cerebral hemispheres and lat-eralventricleswithajunctionalongthefrontalneocortex, particularly rostrally and ventrally. Approximately 19% of patientswithlobarHPEhavetheshape.
Thebispectralindex
the optimal quantity of drugs for each patient so as to maintaintheBISvaluewithinarangethatguaranteesa non-verbalresponsetostimuliandthelowprobabilityofexplicit memory. Prospective studieshave shown that a BIS main-tained between 40 and 60 ensures an adequate hypnotic stateduringanesthesia.
The reliabilityandaccuracy ofBISmonitoringfor pedi-atricpatientsisstillbeingstudied,especiallyinveryyoung children, neonates, andinfants. In addition,thereareno studiesontheuseoftheBISinpediatricsubjectssuffering from rare congenital diseases of the central nervous sys-tem.AwidevariabilityintheBISvalueshasbeenobserved inmanychildrenwithrespecttothedosagesofanesthetics used.
Case
report
One13-year-oldchildweighing 32kg, sufferingfromlobar holoprosencephaly,wasbroughttoourattentionfor orchi-dopexysurgery.Thechildwasindrugtreatmentwithsodium valproate,clorazepam,levothyroxinesodium,somatropin, anddesmopressin.The inductionwasmadeviainhalation, without premedication, through a mixture of air, oxygen, andsevoflurane ata concentrationof 6%andFiO2 of 0.4,
immediately after a peripheral vein wascannulated, fol-lowed by the administration of 2g/kg of fentanyl and
cisatracurium 0.15mg/kg. Then a ProSeal laryngeal mask airway (PLMA) size 2.5 wasinserted. The child was then connectedtomechanicalventilationwithamixtureofair, oxygenandend-tidalconcentrationofsevoflurane3%with FiO2of0.4andsubsequentlyreducedto2%,asaresultofthe
evaluationwithbispectralindex,allowing perfect adapta-tiontoartificialventilation.Allroutinehemodynamic and respiratory monitoring systems were applied: blood pres-sure,ECG,ETCO2andSpO2.Fromthemomentofinduction
adhesive front sensors were applied for the detection of thebispectralindex(BISVistaMonitoringSystemTM,Aspect
MedicalSystem,USA),recordingthetrendsfortheduration ofthesurgeryuntiltheawakeningofthechild.TheBIS val-ues were recordedat thefollowing times:Ti (induction), Tsis (surgical incision of the skin), T5 (5min after incision
oftheskin),Tsevo2 (afterreductionoftheconcentrationof
end-tidalsevoflurane2%),andTrecovery(thecessationofthe
administrationofsevofluraneanduponwaking).
Duringtheinductionphasewithsevofluraneat6%(Ti)the
BISrecordedamedianvalueof27.5±3.5DS(Fig.1).Atthe timeofthesurgicalincisionoftheskin,withaconcentration ofend-tidalsevolfuraneat3%(Tsis)amedianof41.5±4.3
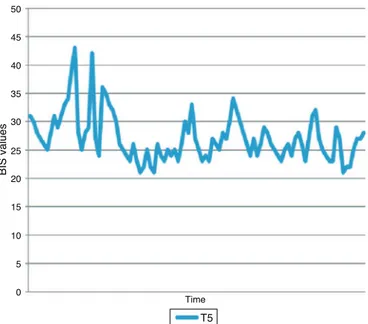
DS(Fig.1),and5min aftertheskinincision(T5)amedian
of26.0±4.2DS(Fig.2).Having consideredthe aboveBIS valuestoolowcomparedtothe40---60standardrelativeto an appropriate anesthesiaplan,it was decidedtoreduce the end-tidal concentration of sevoflurane to 2% (Tsevo2).
During this time we recorded BIS values of 26.5±5.3 SD (Fig.3).Attheendofthesurgery,about75minafter induc-tion,westoppedtheadministrationofsevoflurane(Trecovery)
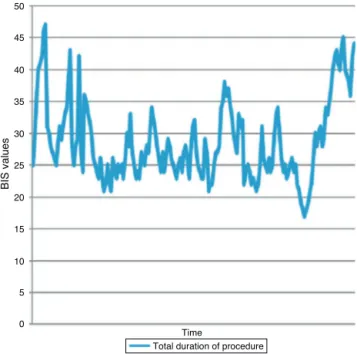
until the child woke up. The median BIS values recorded were29.5±8.1DSwitha maximumof47 andaminimum of17(Fig.4).ThetotalBISvaluesrecordedrelatedtothe wholedurationoftheoperationshowedanexcessivedepth ofanesthesiawithmedianvaluesof27±6.3SD(Fig.5).
50
45
40
35
30
25
20
15
10
5
0
Time
Tsis Ti
BIS values
Figure1 BISvaluesatthetimeofinduction(Ti,27.5±3.5 DS)andsurgicalincisionoftheskin(Tsis,41.5±4.3DS).
Theawakeningtookplacewithoutcomplicationsandin theabsenceofagitationorseizures.Throughoutthe dura-tionofthesurgeryrespiratoryandhemodynamicparameters wereallwithinthenormalrange:heartrate81.3±3.3SD, systolicbloodpressure101.3±2.0SD,diastolicblood pres-sure 52.0±2.3 SD, mean arterial pressure 68.5±1.8 SD (Fig. 6).Duringthe time(Tsevo2),an
electroencephalogra-phywasrecorded(EEG)thatdemonstratedanepileptiform EEGactivitywithspikes(Fig.7).
50
45
40
35
30
25
20
15
10
5
0
Time
T5
BIS values
40
35
30
25
20
15
10
5
0
Time
Tsevo2
BIS values
Figure 3 BIS values with 2% end-tidal sevoflurane (Tsevo2, 26.5±5.3SD).
50
45
40
35
30
25
20
15
10
5
0
Time Trecovery
BIS values
Figure 4 BIS values during the recovery of the patient (Trecovery,29.5±8.1DS).
Discussion
Theliterature lacksstudies onBISmonitoringin pediatric patientswithcongenital braindisease undergoinggeneral anesthesiafor surgery. Consequentlyit is very difficult to interpret the mechanisms by which such monitoring may besubjecttochangeor alterationunderanesthesia.5 The BISexpressesthedepthofanesthesiawithanumericvalue ranging from0 (deepanesthesia) to100 (awake patient), while values between 40 and 60 are considered ideal for anadequate surgical anesthesia. Inprinciple, theBIS val-uesrecordedinthepediatricageareinverselyproportional totheconcentrationofend-tidalsevofluraneandcorrelate
50
45
40
35
30
25
20
15
10
5
0
BIS values
Time
Total duration of procedure
Figure5 BISvaluesduringallthetimeofsurgicalprocedure (27±6.3SD).
120
100
80
60
40
20
0
mmHg/HR
HR SBP DBP MAP
Time
Figure6 Hemodynamic parametersrecordedduringallthe timeofsurgicalprocedure(HR,heartrate;SAP,systolicarterial pressure;DAP,diastolicarterialpressure;MAP,middlearterial pressure).HR81.3±3.3SD,SBP101.3±2.0SD,DBP52.0±2.3 SD,MAP68.5±1.8SD.
muchbetterwithchangesinbloodpressureandheartrate. Inaddition,theend-tidalconcentrationofsevofluranewhich correspondstoaBISof50(95%)ishigherinchildrenunder two years comparedto those who are older (1:55 versus 1:25%).IntherecoveryphasechangesintheBISaremore progressiveinolderchildrencomparedtothesmallerones whichshowinsteadanon---offprofile.6
Inourcase,despitehavingusedhigherend-tidal sevoflu-rane concentrations compared to those indicated above, fromthetimeofinductiontotheawakeningstage,thetotal BISvalues recordedrelated totheduration of the opera-tionshowedanexcessivedepthofanesthesiawithmedian valuesof27±6.3SD.Thisdatacanbeunderstandable dur-ing theearly stages of anesthesia, induction inparticular (Ti27.5±3.5DS),whentheconcentrationsof sevoflurane
needtobehigher.Insubsequentstages,especiallyatTsevo2
time,wewouldhaveexpectedanincreaseintheBISvalues afterreducing theend-tidalconcentrationof sevoflurane. In contrast,theBIS recordedmedian valuesparadoxically lower(Tsevo226.5±5.3DS).Similarly,duringtheawakening,
BISvalueswereratherlow (Trecovery29.5±8.1 DS)instead
of nearing60 which normallyindicates the resumptionof patientconsciousness.TherelativelyhigherBISvalue,and thus closer tothe rangeof 40---60, wasfound onlyat the moment of the incision of the skin (Tsis 41.5±4.3 DS)
although the BIS has no specificity in the prediction of responsetonociceptivestimuliasitisavaluemoreorless insensitivetonarcoticswhilereflectingthehypnoticstate. The mechanism and the possible causes of this abnor-mal response can be demonstrated, in our opinion, in a detailedanalysisof thetrends of BISvaluesinthe differ-entobservationtimes.Inparticular,inT5,Tsevo2,andTrecovery
(Figs.2---4)weexperiencedrapidvariabilitywithsuddenfalls andrepetitivevaluesofBIS.Therewasnotartifacts,andthe patientwasotherwisewell curarized:signal qualityindex (SQI),electromyograph(EMG),suppressionratiovalue(SRV) showedagoodqualityofsignal.
This fact brings us to another published case report, although onan adult patient,in whichsevoflurane deter-mined repetitive epileptiform electrical activity with suddenandrapidfalloftheBISvalues,whichwereresolved byadministeringantiepilepticdrugsduringsurgery.7
It is well-documented that sevolfurane can stimulate epileptogenic activity8---10 and the electroencephalogra-phy recorded during the time Tsevo2 demonstrated us an
epileptiformEEGactivitywithspikes;inourcaselobar holo-prosencephalyisadiseasethatisaccompaniedbyepilepsy. Althoughthechildwasalreadybeingtreatedwith medica-tionsforanunderlying disease,wemustassumethatthey werenotabletolimittherapidchangesobservedwiththe BISandsevofluranehasplayedanimportantrole.Wehave notusedanti-epilepticdrugsthatwouldbeusefulasex adiu-vantibuscriteriontodemonstratethenatureofthechanges inBISvalues.Inreality,fromaclinicalstandpointno con-vulsionswereobserved duringtheoperationor duringthe awakeningphase.Itislikelythattheepilepticactivitywas
aneuroelectricmanifestationdetectedbytheBIS.Finally, thegoodhemodynamic stability throughout theoperation confirmsthattheconcentrations ofsevofluranearebetter relatedtotheBISthanthevariationsofbloodpressureand heartrateinthepediatricpatient.
Conclusions
The BIS is a very useful monitoring tool for assessing the degree of depth of anesthesia and to analyze the elec-troencephalographic variations of anesthetics. Particular attentionshould begiventopatients withcongenital dis-ordersofthecentralnervoussystem inwhichtheBISmay give abnormal responses that do not reflect an accurate assessmentofthedepthofanesthesia. Thisisparticularly importantinthecaseofhighconcentrationsofsevoflurane thatmayresultinepileptogenicaction.Inthesecasesthe choiceofadifferentanesthetictechniqueshouldbetaken intoseriousconsideration.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.Bellone S, De Rienzo F, Prodam F, et al. Etiopathogenetic advancesandmanagementofholoprosencephaly:frombench tobedside.PanminervaMed.2010;52:345---54.
2.Sury M. Brain monitoring in children. Anesthesiol Clin. 2014;32:115---32.
3.KimJK,KimDK,LeeMJ.Relationshipofbispectralindexto min-imumalveolar concentrationduringisoflurane,sevofluraneor desfluraneanaesthesia.JIntMedRes.2014;42:130---7. 4.Nishiyama T. Composite-, plain-auditory evoked potentials
indexandbispectralindextomeasuretheeffectsof sevoflu-rane.JClinMonitComput.2013;27:335---9.
5.Rodriguez RA,Hall LE,DugganS, etal. Thebispectralindex doesnotcorrelatewithclinicalsignsofinhalational anesthe-siaduringsevofluraneinductionandarousalinchildren.CanJ Anaesth.2004;51:472---80.
6.DenmanWT,SwansonEL,RosowD,etal.Pediatricevaluation ofthebispectralindex(BIS)monitorandcorrelationofBISwith end-tidal sevoflurane concentration in infants and children. AnesthAnalg.2000;90:872---7.
7.ChinzeiM,SawamuraS,HayashidaM,etal.Changeinbispectral index during epileptiform electrical activity under sevoflu-rane anesthesia in a patient with epilepsy. Anesth Analg. 2004;98:1734---6.
8.Constant I,SeemanR, MuratI.Sevoflurane andepileptiform EEGchanges.PaediatrAnaesth.2005;15:266---74.
9.Särkelä MO,Ermes MJ, vanGils MJ,et al. Quantificationof epileptiformelectroencephalographicactivity during sevoflu-ranemaskinduction.Anesthesiology.2007;107:928---38. 10.SchultzA,SchultzB,GrouvenU,etal.Epileptiformactivityin