REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiology www.sba.com.brSCIENTIFIC
ARTICLE
The
incidence
of
emergence
delirium
and
risk
factors
following
sevoflurane
use
in
pediatric
patients
for
day
case
surgery,
Kingston,
Jamaica
Rachel
Gooden
a,b,
Ingrid
Tennant
b,∗,
Brian
James
a,
Richard
Augier
b,
Annette
Crawford-Sykes
b,
Kelvin
Ehikhametalor
b,
Georgiana
Gordon-Strachan
c,
Hyacinth
Harding-Goldson
baBustamanteHospitalforChildren,SouthEastRegionalHealthAuthority,Kingston,Jamaica
bDepartmentofSurgery,Radiology,AnaesthesiaandIntensiveCare,UniversityoftheWestIndies,Kingston,Jamaica cHealthResearchResourceUnit,Dean’sOffice,FacultyofMedicalSciences,UniversityoftheWestIndies,Kingston,Jamaica
Received31July2013;accepted24September2013 Availableonline11November2013
KEYWORDS
Emergencedelirium;
Agitation; Sevoflurane;
Pediatricanesthesia
Abstract
Backgroundandobjectives: Emergence delirium is a distressing complication of the use of sevofluraneforgeneralanesthesia.Thisstudysoughttodeterminetheincidenceofemergence deliriumandriskfactorsinpatientsataspecialistpediatrichospitalinKingston,Jamaica.
Methods:Thiswasacross-sectional,observationalstudyincludingpediatricpatientsaged3---10 years,ASAIandII,undergoinggeneralanesthesiawithsevofluraneforelectiveday-case pro-cedures.Datacollectedincludedpatients’levelofanxietypre-operativelyusingthemodified YalePreoperativeAnxietyScale,surgeryperformed,anestheticdurationandanalgesics adminis-tered.Postoperatively,patientswereassessedforemergencedelirium,definedasagitationwith non-purposefulmovement,restlessnessorthrashing;inconsolabilityandunresponsivenessto nursingand/orparentalpresence.Theneedforpharmacologicaltreatmentandpost-operative complicationsrelatedtoemergencedeliriumepisodeswerealsonoted.
Results:One hundredandforty-five(145)children wereincluded, withemergencedelirium occurring in28(19.3%). Emergencedelirium episodeshadameandurationof6.9±7.8min, required pharmacologicinterventionin19(67.8%)childrenandwereassociated witha pro-longedrecoverytime(49.4±11.9versus29.7±10.8minfornon-agitatedchildren;p<0.001). Factorspositivelyassociatedwithemergencedeliriumincludedyoungerage(p=0.01,OR3.3, 95%CI1.2---8.6)andmoderateandsevereanxietypriortoinduction(p<0.001,OR5.6,95%CI 2.3---13.0).Complicationsofemergencedeliriumincludedintravenouslineremoval(n=1),and surgicalsitebleeding(n=3).
∗Correspondingauthor.
E-mail:[email protected](I.Tennant).
0104-0014/$–seefrontmatter©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Conclusion:Childrenofyoungeragewithgreaterpreoperativeanxietyareatincreasedrisk ofdevelopingemergencedeliriumfollowinggeneralanesthesiawithsevoflurane.Theoverall incidenceofemergencedeliriumwas19%.
©2013SociedadeBrasileiradeAnestesiologia.PublishedbyElsevier EditoraLtda.Allrights reserved.
PALAVRAS-CHAVE
Delíriode
emergência; Agitac¸ão; Sevoflurano;
Anestesiapediátrica
Incidênciadedelírioaodespertarefatoresderiscoapósousodesevofluranoem pacientespediátricosparacirurgiaambulatorial,Kingston,Jamaica
Resumo
Justificativaeobjetivos: Delírioaodespertaréumacomplicac¸ãopreocupanteapósousode sevofluranoemanestesiageral.Esteestudoprocuroudeterminaraincidênciadedelírioao des-pertareosfatoresderiscoempacientesdeumhospitalpediátricoespecializado,emKingston, Jamaica.
Métodos: Estudotransversaleobservacional,incluindopacientespediátricoscomidadesentre 3-10anos,estadofísicoASAI-II,submetidosàanestesiageralcomsevofluranopara procedi-mentoseletivosemregimeambulatorial.Osdadoscoletadosincluíramníveldeansiedadeno pré-operatóriomedido comaEscala deAnsiedadePré-operatóriadeYale modificada, cirur-giarealizada,durac¸ãodaanestesiaeanalgésicos administrados.Noperíodopós-operatório, ospacientesforamavaliadosparaverificaraincidênciadedelírioaodespertar,definidocomo agitac¸ãocommovimentosnão-intencionais,inquietac¸ãooudebatimento;inconsoláveleapático àpresenc¸ade enfermeiros e/oudos pais. Anecessidade detratamentofarmacológico eas complicac¸õespós-operatóriasrelacionadasaepisódiosdedelírioaodespertartambémforam registradas.
Resultados: 145crianc¸asforamincluídas,comincidênciadedelírioaodespertarem28(19,3%). Osepisódiosdedelírioaodespertarapresentaramumamédiadedurac¸ãode6,9±7,8min;a intervenc¸ão farmacológicafoinecessária em 19pacientes(67,8%)efoiassociada ao tempo de recuperac¸ão prolongado (49,4±11,9 versus 29,7±10,8min para crianc¸as não-agitadas;
p<0,001).Osfatorespositivamenteassociadosao delírioaodespertarincluíram idademais jovem(p=0,01,OR3,3,IC951,2-8,6)eansiedademoderadaegravepré-induc¸ão(p<0,001, OR5.6,IC952,3-13,0).Ascomplicac¸õesdodelírioaodespertarincluíramaremoc¸ãodalinha intravenosa(n=1)esangramentodosítiocirúrgico(n=3).
Conclusão:Ascrianc¸asmaisjovensqueapresentamansiedadesérianoperíodopré-operatório possuemmaiorriscodedesenvolverdelíriopós-anestesiageralcomsevoflurano.Aincidência globaldedelíriofoide19%.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
The introduction of inhaled anesthetic agents withlower
blood solubility (sevoflurane and desflurane) into clinical
practicehaspermittedfaster onset,moreprecise control
and more rapid recovery from anesthesia.1,2 Sevoflurane
ismost commonly usedinpediatric anesthesiafor inhala-tionalinductionandmaintenancebecauseofitsdecreased pungency,airwayirritationandcardiovasculardepression.3
However, its use has been associated with a greater incidence of excitatory emergence in the post-operative period.4
Emergencedelirium(ED)hasbeendescribedbyseveral authorsasaclinical stateduring emergencefromgeneral anesthesiainwhichpatientsareawakebuthaveanaltered mentalstatemanifestingasdisorientation,inconsolability, confusion,andviolentorharmfulphysicalbehavior.4,5These
patientsdonot appeartorecognizefamilymembers, dis-playnon-purposefulbehavioranddonotreactappropriately to external stimuli.6 Currently, there is no one accepted
definitionofEDandanumberofscoringsystemshavebeen usedtoaid inthediagnosis.6,7 Awiderangeof incidences
from 10 to 80%4 has been recorded in the literature and
this maybe inpart due todifferences in definitionsused for diagnosis. Itsunderlyingcauseremains unknown. Age, preoperative anxiety,anesthetictechniqueoragents, sur-gical procedure, pain and the use or not of adjunctive medication have all been suggested to play a role in its development.4,5,8,9ED usuallyoccursearlyinthe recovery
period(thefirst30min)andisshort-livedandself-limiting, lasting between 5 and 15min.4 However pharmacological
intervention maybe entertained, depending onthe dura-tionandseverityoftheeventandmayincludeanalgesics, benzodiazepines and hypnotics such asfentanyl, propofol andmidazolam.4
Restlessrecovery from anesthesiamay cause injury to the patient, including the surgical site, and accidental removalofintravenousaccess,drainsandsurgicaldressings. Extranursingcaremayoftenbenecessary.10Thismaythen
parentaldistressandoveralldissatisfactionwiththe anes-theticcare.4Thisstudywasthereforedesignedtoassessthe
incidenceofED attheonlydedicatedpediatrichospitalin Jamaicaandidentifypossiblecontributingfactors.
Materials
and
methods
The Bustamante Hospital for Children (BHC), Kingston, Jamaicais a283-bed hospital,includinga 5bedIntensive CareUnit.Itistheonlyspecialistchildren’shospitalinthe EnglishspeakingCaribbeanprovidingcaretopatientsfrom birthto12years.
All AmericanSociety of Anesthesiologist (ASA) physical status I and II elective patients, between 3 and 10 years thatpresentedforelectivepediatricday-casesurgeryatthe BHCbetweenJuly18andNovember23,2011andinwhom sevofluranewasnotcontraindicatedforinductionand main-tenance of anesthesia, wereeligibleto participatein the study.Informedwrittenconsentwasobtainedfromthe par-entorguardianofthechild.Otherexclusioncriteriawere:
1. Pre-existingneurologicaldysfunctionandagitation(e.g. Down’sSyndrome,autism).
2. ENT surgeries associated with the feeling of ‘‘suffocation’’ such as adenoidectomies and tonsil-lectomies.
3. Ophthalmicprocedureswherepostoperativeeyepatches would be applied, which could possibly contribute to patientdisorientationduringemergence.
4. Patientswhoarevisuallyorhearingimpairedthatwould possiblyresultinpostoperativedisorientation.
5. Majorproceduressuchascardiacandneurosurgical pro-cedures.
Pre-operative assessment was done and preoperative medicationsadministeredwererecorded.
Anxietyassessmentwasdoneonthewardbytheresearch anesthetist just before transfer to the operating theater (OT) and then in the OT after separation from parents, priortoinduction.Thepatient’sanxietylevelwasassessed usingthe modified Yale PreoperativeAnxiety Scale.11 The
mYPASconsistsof22itemsinfivecategories(activity, emo-tionalexpressivity,state of arousal, vocalization, anduse ofparents).The highestbehaviorallevelobservedineach ofthefivemYPAScategoriesisthescoreforthatcategory. The highestpossible scorethat canbeachieved(extreme
agitation)is22.Thescorehasgoodinter-andintra-observer reliability,has been validated in the pediatric population andcanbecompletedin lessthanaminute.11 The scores
werecategorizedintomild (5---10),moderate (11---15)and severe(16---22)anxiety.
Standardmonitoringofelectrocardiography(ECG), non-invasivebloodpressure(NIBP)andoxygensaturation(SpO2) wasapplied.Atotalfreshgasflowofthreetimesthe esti-matedminutevolumeofthepatient(50%oxygeninnitrous oxide)with8%sevofluranewasusedwithaMaplesonF cir-cuit,flushedfor2minpriortoinductionofanesthesia.The anestheticmask wasthen appliedat theend of anormal expiration.Aftertheeyelashreflexwaslost,andthepatient was at an adequate depth of anesthesia, an intravenous catheter was inserted. Any complications at induction or under anesthesia including coughing, breath-holding, laryngospasm, bronchospasm, arrhythmias, hypotension, hypertension and abnormal movements were recorded. The airway technique chosen was at the discretion of theanesthetist.Childrenrequiringendotrachealintubation received intermittent positive pressure ventilation, while thoserequiringaLMAorfacemaskwereallowedtobreathe spontaneously,exceptforthosehavingumbilicaland supra-umbilical herniorraphies. Anesthesia wasthen maintained withsevoflurane(concentrationadjustedasneededbythe attendinganesthetist)in50%oxygenwithnitrousoxide.Any analgesicsadministeredintra-operativelywerealsonoted, suchaspethidine,diclofenac,acetaminophenorlocal anes-thetics.
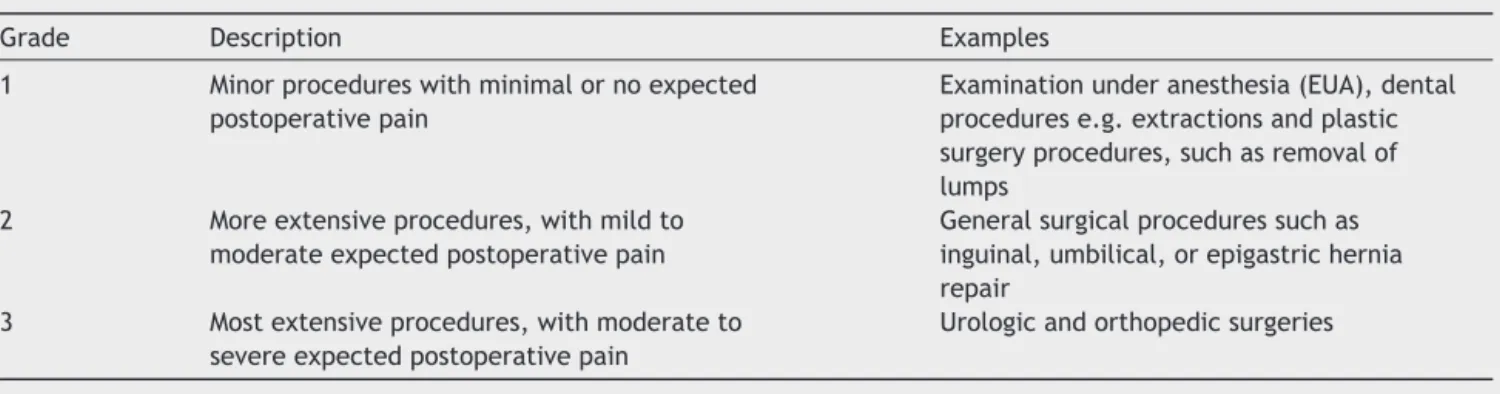
Thesurgicalprocedureperformedwasdocumented,and categorizedintooneof the3 groups basedonthe extent oftheoperationaswell asthe expectedseverityof post-operative pain, as outlined in Table 1. At the conclusion of the procedure, sevoflurane was discontinued and the patient was transferred to the Post-Anesthesia Care Unit (PACU)providedrespirationwaswellestablished,saturation onroom air was satisfactory,and there was cardiovascu-larstability.Lengthofanesthesiawasdefinedastimefrom inductionuntiltimeofdiscontinuationofsevoflurane.The emergencetimewasalso noted,fromtimeof discontinu-ationofsevoflurane totimeof eye openingor purposeful limb movement (the first to appear). During recovery, a trained observer (PACU nurse or researcher) blinded to the pre-operative anxiety score, recorded all emergence behaviorsusingCravero’s5-pointagitationscaleevery5min (Table2)untilthepatientwasawake,calmanddischarged.7
The presence and duration of ED were documented. ED
Table1 Descriptionofsurgicalgradecategories.
Grade Description Examples 1 Minorprocedureswithminimalornoexpected
postoperativepain
Examinationunderanesthesia(EUA),dental procedurese.g.extractionsandplastic surgeryprocedures,suchasremovalof lumps
2 Moreextensiveprocedures,withmildto moderateexpectedpostoperativepain
Generalsurgicalproceduressuchas inguinal,umbilical,orepigastrichernia repair
3 Mostextensiveprocedures,withmoderateto severeexpectedpostoperativepain
Table2 Cravero’sAgitationScale.7
Scale Description
1 Obtunded,notresponsivetostimulation
2 Asleep,butresponsivetomovementor
otherstimulation
3 Awakeandappropriatelyresponsive
4 Cryinganddifficulttoconsole
5 Wildthrashingbehaviorneedingrestraint
wasdefinedas: agitationwithnon-purposeful movement, restlessness,orthrashing;incoherence;inconsolabilityand unresponsivenesstonursingandsubsequentparental pres-ence.ChildrenwerenotconsideredtohaveEDiftherewas clinicalevidencesuggestiveofpainsuchaslocalizationand apparentinadequateanalgesia.Insuchcases,analgesiawas administered and the patient was reassessed. Vital signs (heart rate,SpO2 andrespiratory rate) were documented at5minintervals.Allpharmacologicandnon-pharmacologic interventions(decidedonbythePACUnurseandanesthetist assignedtothelist)andadverseeventswerealsorecorded. Recoverytimewasdefined asthetimefromadmission to thePACUuntilthepatientwasfullyawake, appropriately responsiveandcooperative,withaGrade 3orless onthe CraveroAgitationScale. Discharge criteriawere in accor-dancewithroutinepracticeandincludedanawake,oriented patientwhohadoptimalanalgesiaandstablevitalsigns.
The sample size wascalculated using a single propor-tionmethod.Thiscalculationwasbasedonapresumed30% incidence(basedontheliteraturereview)andtodetecta 10%differencebetween populations.Asample population of145 wasrequired to yield apower of 80% and a confi-dence intervalof 95%. The data wereanalyzed usingthe Statistical Package for the Social Sciences (SPSS) version 12.0(IBM,Chicago,IL).Parametricdatawerepresentedas mean±standard deviation (sd) and were compared using unpaired Student’s t-tests. Chi-square and Fisher’s exact testswereusedtocomparenon-parametricdata.p values of<0.05wereconsidered significant.Ethical approvalwas obtainedfromthe UWIFaculty ofMedical SciencesEthics CommitteeandthelocalHealthAuthority.
Results
Demographics
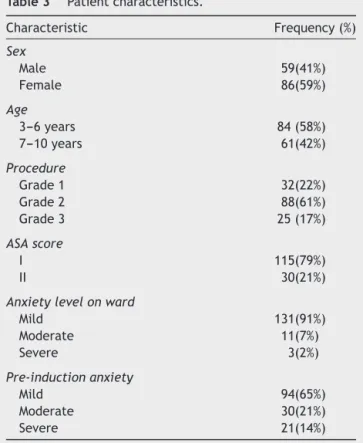
A total of 145 patients were studied, 86 (59%) of whom were females. Their mean age was 6.3±2.3 years, with bothmedian andmodeof 6.0andIQRof4 years(Fig.1). Surgicalproceduresperformedincludedinguinal herniorrha-phies, reduction and fixation of fractures, orchidopexies, cyst removal, examinations under anesthesia and dental extractions. Most (61%) procedures were general surgical proceduressuch as herniorrhaphies,classified as Grade 2 (Table 3). There were 115 ASA 1 patients (79%) and 30 ASA2patients(21%).Chronicillnesseswereuncommonand includedasthma,sicklecelldiseasetrait(HbAS)and sinus-itis.
0
3 4 5 6 7 8 9 10
5 10 15 20 25 30
Number
of
patients
Age in years
Figure1 Distributionofageinyears.
Pre-operative
Most patients (98%) in the study were not premedicated. Only one patient received midazolam and 2 patients receivedpromethazine (Phenergan). The mYPASscores on the wardweresignificantly lowerthanthosejust priorto induction of anesthesia. Mildanxiety (scoreof 5---10) was seen in 91%of patients preoperativelyonthe ward, com-paredto65%priortoinductionofanesthesia.Severeanxiety (mYPAS16---22)wasseeninonly2%ofpatientsontheward, whichincreasedto14%justpriortoinduction(Table3).
Intra-operativecourse
The majority of patients (90%) had a laryngeal mask airway (LMA), 7 (5%) required endotracheal intubation and 8 (5%) had a face mask only. The most frequent
Table3 Patientcharacteristics.
Characteristic Frequency(%)
Sex
Male 59(41%) Female 86(59%)
Age
3---6years 84(58%) 7---10years 61(42%)
Procedure
Grade1 32(22%) Grade2 88(61%) Grade3 25(17%)
ASAscore
I 115(79%)
II 30(21%)
Anxietylevelonward
Mild 131(91%) Moderate 11(7%) Severe 3(2%)
Pre-inductionanxiety
Table4 Frequencyofcomplicationsduringanesthesia. Complications Frequency(%) Breathholding 13(9%) Coughing 18(6%) Laryngospasm 4(3%) Hypotension 3(2%) Wheals 2(1%) Emesisandabnormalmovement 1(1%)
complicationobservedwasbreathholding,whichoccurred
in 9% of patients, followed by coughing in 6% of patients
(Table4).The lengthofanesthesiarangedbetween 6and 185min (trimmed mean 40.0±17.1, median 37min, IQR 19min).Timetoemergencerangedfrom1to50min(mean 19.5±11.7min,median19min,IQR20min).Foranalgesia, rectalacetaminophenwasadministeredto86%ofpatients, intravenous pethidine (meperidine) wasgiven to 96% and 72%receivedlocalinfiltrationwith0.25%bupivacaine.
RecoveryperiodandED
Recovery time ranged from 5 to 76min (mean 33.5±13.4min). ED was seen in 28 (19.3%) patients and ranged from 1 to 37min (mean 6.9±7.8min). Most cases of ED lasted 5min or less (64%). Thirteen (46%) of the patients with ED required pharmacological treatment withpethidine (meperidine); and midazolam or ketamine wasaddedin5ofthosepatients.EpisodesofEDwere asso-ciatedwitha prolongedrecovery timeof 49.4±11.9min, compared with 29.7±10.8min for non-agitated children (p<0.001).IntheED group,onechild (4%)removedan IV line,3(11%)experiencedincreasedbleedingatthesurgical siteand1(4%)removedasurgicaldressing.
Factorsassociatedwithemergenceagitation
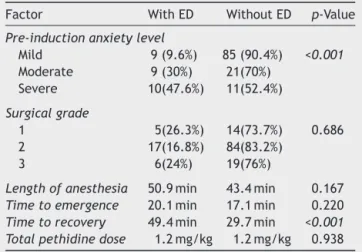
There wasa significant relationship between age and the developmentof ED: 26% of patients aged3---6 years were foundtobeagitated,comparedto10%ofpatientsaged7---10 years(p=0.01,OR3.3,95%CI1.2---8.6).Themeanageofthe patientswhodevelopedEDwas4.8±1.5yearscomparedto ameanageof6.7±2.3yearsforthosepatientswhodidnot (p<0.001).
Patientswhohadmoderateandsevereanxietyjustprior toinductionweremorelikelytodevelopEDinthe postop-erativeperiod(p<0.001,OR5.6,95%CI2.3---13.0).Only10% ofpatientswithmildanxietydevelopedED,comparedwith 37%ofpatientswithmoderateorsevereanxiety.This asso-ciationwasnotseenwithmYPASscores doneontheward preoperatively.
There was no association between gender (p=1.0), lengthofanesthesia(p=0.167),emergencetime(p=0.220), grade of surgical procedure (p=0.686), chronic illness (p=0.105),doseofopioidanalgesiagivenintra-operatively (p=0.938),oruseofwoundinfiltration(p=0.613)(Table5).
Table5 Factorsassociatedwithemergencedelirium. Factor WithED WithoutED p-Value
Pre-inductionanxietylevel
Mild 9(9.6%) 85(90.4%) <0.001
Moderate 9(30%) 21(70%) Severe 10(47.6%) 11(52.4%)
Surgicalgrade
1 5(26.3%) 14(73.7%) 0.686 2 17(16.8%) 84(83.2%)
3 6(24%) 19(76%)
Lengthofanesthesia 50.9min 43.4min 0.167
Timetoemergence 20.1min 17.1min 0.220
Timetorecovery 49.4min 29.7min <0.001 Totalpethidinedose 1.2mg/kg 1.2mg/kg 0.938
Theitalicshighlightthestatisticallysignificantfindings.
Discussion
This study documented an ED incidence of 19.3% in the
pediatricsurgicalpopulation(3---10 years)undergoing
gen-eral anesthesia with sevoflurane at the BHC, Jamaica
withyoungerageandpre-operativeanxiety afterparental
separation being significant indicators. Reports from the
international literature show incidences of ED ranging
between10and80%4inchildrenwhoreceivedsevoflurane
anesthesia;however,variationsinprotocolsandinthe def-initionofEDinthesestudiesmakeabsolutecomparisonof resultsdifficult.Astudyofchildrenages3---7yearswhohad sevofluraneanesthesiaandthatalsousedasimilardefinition asinthisstudyreportedanincidenceof18%.8
Other studies have alsobeen in keepingwithour find-ingofhigherincidencesinyoungerchildren.Patientsaged 3---5 years undergoingsevoflurane anesthesia had an inci-denceofEDof40%,comparedto11.5%inthose6---10years andanoverallincidenceof26.7%.12Inastudycarriedoutin
Thailand13theincidenceofEDwassignificantlyhigherinthe
2---5yearagegroupthanthe6---9yeargroup(66.7%versus 45.8%,p=0.002). Aftercategorizingour patients into dif-ferentagegroups,wefoundthat26%ofchildrenaged3---6 yearsexperiencedED,comparedto10%inthosewhowere 7---10years.
The perioperativeperiodis oftenextremely distressing for children and we observed a definite increase in anxi-etyfollowingparentalseparation.Therelationshipbetween preoperative anxiety and ED seen was also observed in otherstudies.The oddsof havingmarkedsymptomsof ED increasedbyapproximately10%whenthemYPASincreased by 10 points.14 Preoperative anxiety was found to be
higherinchildren whodevelopedsevere ED thatrequired pharmacologic treatment (p=0.032).15 ED occurred more
frequently in children who exhibited difficult parental-separationbehaviorthaninthosewhodidnot(44.4%versus 18.3%).13
thatadequateanalgesiamayreduce theincidenceofED.4
TheincidenceofEDfoundinthisstudyamongpatients3---6 yearsiscomparabletostudiesinvolvingpainlessprocedures (MRI)orusingadequateregionalanesthesia.12,15---17However,
painisdifficulttodifferentiatefromtrueEDasthesignsare verysimilar,especiallyinyoungerpatients.18Weattempted
toexcludethepresenceoflocalizedpainwhenmakingthe diagnosisofED.
Thetimetorecoverywasdelayedinthosepatientswho developed ED, similartoother studies.8,12,15,16,19 The
pro-longedrecovery timemost likelyresulted fromadditional sedative pharmacologic treatment and other supportive therapies necessary to manage this phenomenon. The observedprolongedrecoveryprocessanddelayeddischarge couldalsohavebeeninfluencedbycomplicationsresulting from the period of agitation such as increased bleeding, dislodgedintravenouslinesanddrains.8
Limitations of this study included a lack of standard-ization of the concentration of sevoflurane used, doses andtimingofadjunctivemedicationsandthesecouldhave impactedontheincidenceofED.Theremayalsohavebeen observer bias, as the observers, although blinded to the levels of pre-operative anxiety, were not blinded to the anesthetictechniqueandsurgicalprocedure.
Conclusions
OurfindingsindicatethatsevofluraneassociatedEDoccurs inchildrenattheBHCatsimilarratesanddurationstothose observedinother studies.We identifiedyoungerage(3---6 years)andmoderate tosevere preoperative anxietyafter parentalseparation,aspositivepredictorsofED.AttheBHC, asinother hospitalsinJamaica,earlyparentalseparation continuestobepracticed.Achangeinthispolicymayhavea significantimpactontheincidenceofEDinoursetting.The mYPASscorecouldbeavaluabletoolforidentifyingchildren whoareatriskfordevelopingED.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Eger 2nd EI. New inhaled anesthetics. Anesthesiology. 1994;80:906---22.
2.WallinRF,ReganBM,NapoliMD,etal.Sevoflurane:anew inhala-tionalanestheticagent.AnesthAnalg.1975;54:758---66.
3.SmithI,NathansonM,WhitePF.Sevoflurane----along-awaited volatileanaesthetic.BrJAnaesth.1996;76:435---45.
4.VlajkovicGP,SindjelicRP.Emergencedeliriuminchildren:many questions,fewanswers.AnesthAnalg.2007;104:84---91.
5.VeyckemansF.Excitationanddeliriumduringsevoflurane anes-thesiainpediatricpatients.MinervaAnestesiol.2002;68:402---5.
6.MalarbiS,StargattR,HowardK,etal.Characterizingthe behav-iorofchildrenemergingwithdeliriumfromgeneralanesthesia. PaediatrAnaesth.2011;21:942---50.
7.BajwaSA,CostiD,CynaAM.Acomparisonofemergence delir-iumscalesfollowinggeneral anesthesia inchildren.Paediatr Anaesth.2010;20:704---11.
8.Voepel-LewisT,MalviyaS,TaitAR.Aprospectivecohortstudyof emergenceagitationinthepediatricpostanesthesiacareunit. AnesthAnalg.2003;96:1625---30.
9.EckenhoffJE,KnealeDH,DrippsRD.Theincidenceandetiology ofpostanestheticexcitement.Aclinicalsurvey.Anesthesiology. 1961;22:667---73.
10.HudekK.Emergencedelirium:anursingperspective.AORNJ. 2009;89:509---16.
11.KainZN,MayesLC,CicchettiDV,etal.TheYalePreoperative AnxietyScale:howdoes itcompare witha‘‘goldstandard’’? AnesthAnalg.1997;85:783---8.
12.AonoJ,UedaW,MamiyaK,etal.Greaterincidenceofdelirium duringrecoveryfromsevofluraneanesthesiainpreschoolboys. Anesthesiology.1997;87:1298---300.
13.Saringcarinkul A, Manchupong S, Punjasawadwong Y. Inci-dence and risk factors of emergence agitation in pediatric patientsaftergeneralanesthesia.JMedAssocThai.2008;91: 1226---31.
14.KainZN,Caldwell-AndrewsAA,MaranetsI,etal.Preoperative anxietyandemergencedeliriumandpostoperativemaladaptive behaviors.AnesthAnalg.2004;99:1648---54.
15.WeldonBC,BellM,CraddockT.Theeffectofcaudal analge-siaonemergenceagitationinchildrenaftersevofluraneversus halothaneanesthesia.AnesthAnalg.2004;98:321---6.
16.Abu-Shahwan I. Effect of propofol on emergence behavior in children after sevoflurane general anesthesia. Paediatr Anaesth.2008;18:55---9.
17.CraveroJ,SurgenorS,WhalenK.Emergenceagitationin pae-diatricpatientsaftersevofluraneanaesthesiaandnosurgery:a comparisonwithhalothane.PaediatrAnaesth.2000;10:419---24.
18.ManworrenRC,PaulosCL,Pop R.Treatingchildrenfor acute agitationinthePACU:differentiatingpainandemergence delir-ium.JPerianesthNurs.2004;19:183---93.