REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologia www.sba.com.brSCIENTIFIC
ARTICLE
Analysis
of
the
prevalence
of
atelectasis
in
patients
undergoing
bariatric
surgery
夽
Letícia
Baltieri
a,
Fabiana
Sobral
Peixoto-Souza
b,
Irineu
Rasera-Junior
c,
Maria
Imaculada
de
Lima
Montebelo
d,
Dirceu
Costa
b,e,
Eli
Maria
Pazzianotto-Forti
d,∗aUniversidadeEstadualdeCampinas(Unicamp),ProgramadePós-Graduac¸ãoemCiênciasdaCirurgia,Campinas,SP,Brazil bUniversidadeNovedeJulho(Uninove),ProgramadePós-Graduac¸ãoemCiênciasdaReabilitac¸ão,SãoPaulo,SP,Brazil cClínicaBariátricadePiracicaba,Piracicaba,SP,Brazil
dUniversidadeMetodistadePiracicaba(Unimep),ProgramadePós-Graduac¸ãoemCiênciasdoMovimentoHumano,Piracicaba,SP,
Brazil
eUniversidadeFederaldeSãoCarlos(UFSCar),ProgramadePós-Graduac¸ãoemFisioterapia,SãoCarlos,SP,Brazil
Received14April2014;accepted26November2014 Availableonline25November2015
KEYWORDS
Morbidobesity;
Bariatricsurgery;
Pulmonary atelectasis; Physiotherapy specialty
Abstract
Backgroundandobjective: To observe the prevalence of atelectasis in patients undergoing bariatric surgery and the influence ofthe body mass index (BMI), gender and age on the prevalenceofatelectasis.
Method: Retrospectivestudy of407 patientsandreportsonchestX-rayscarried outbefore andafterbariatricsurgeryoveraperiodof14months.Onlypatientswhounderwentbariatric surgerybylaparotomywereincluded.
Results:Therewasanoverallprevalenceof37.84%ofatelectasis,withthehighestprevalence inthelungbasesandwithgreaterprevalenceinwomen(RR=1.48).Therewasaratioof30% fortheinfluenceofageforindividualsundertheageof36,andof45%forthoseolderthan36 (RR=0.68).TherewasnosignificantinfluenceofBMIontheprevalenceofatelectasis.
Conclusion: Theprevalenceofatelectasisinbariatricsurgeryis37%andthemainriskfactors arebeingfemaleandagedover36years.
©2015SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
夽 Institution:UniversidadeMetodistadePiracicaba(Unimep),Piracicaba,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](E.M.Pazzianotto-Forti).
http://dx.doi.org/10.1016/j.bjane.2014.11.016
PALAVRAS-CHAVE
Obesidademórbida;
Cirurgiabariatrica;
Atelectasia pulmonar; Especialidade
emFisioterapia
Análisedaprevalênciadeatelectasiaempacientessubmetidosàcirurgiabariátrica
Resumo
Justificativaeobjectivo:Observar aprevalência de atelectasiaem pacientessubmetidos à cirurgia bariátrica e a influênciado índice de massa corporal (IMC), sexo e idade sobre a prevalênciadeatelectasia.
Método: Estudoretrospectivode407pacienteselaudos deradiografias detórax realizadas anteseapósacirurgiabariátricaduranteumperíodode14meses.Apenasospacientes sub-metidosàcirurgiabariátricaporlaparotomiaforamincluídos.
Resultados: Houveumaprevalênciageraldeatelectasiade37,84%,commaiorprevalêncianas basespulmonareseemmulheres(RR=1,48).Houveumaproporc¸ãode30%paraainfluênciada idadenosindivíduoscomidadeinferiora36anosede45%naquelescomidadesuperiora36 anos(RR=0,68).NãohouveinfluênciasignificativadoIMCsobreaprevalênciadeatelectasia.
Conclusão:Aprevalênciadeatelectasiaemcirurgiabariátricaéde37%,eosprincipaisfatores deriscosãosexofemininoeidadesuperiora36anos.
©2015SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Obesityhasreachedepidemicproportions,andin2008over 1.4billionadultswereoverweight.1,2Inadditiontothe co-morbiditiesthataccompanyobesesubjects,somechangesin therespiratorysystemandlungfunctioncanalsobefound, duetotheaccumulationoffataroundtheribs,diaphragm andabdomen,thuslimitingmovementoftheribcage.3
Obesity is achronic disease,3,4 and bariatricsurgery is indicatedfor patientswhodonotrespondtoconservative treatment.4
InastudybyChungetal.5itwasshownthatobesityis aforerunnerfortheappearanceofintraandpost-operative respiratory complications during or after surgery. Since gastroplasty, one of the bariatric surgery techniques, is upper abdominalsurgery, it presents changes inherent to this procedure, such as reduced lung volumes, increased respiratory rateand respiratory muscle dysfunction.6 The appearanceofatelectasisisfrequentamongst alltypesof patientduringgeneralanesthesia.7,8Onsubmittingpatients toelective upperabdominalsurgery,Pereiraetal.9 found a 32% incidence of pulmonary complications in patients whopresentedtherestrictivepulmonarysyndrome,as com-paredto6%ofcomplicationsinpatientswithoutrespiratory co-morbidities. Atelectasis appeared in 34% of the whole sample.
Thesituationisworseinobesepatientsinwhom atelec-tasismayappearandpersistforupto24hafterextubation, which does not occur in non-obese patients.10 Moreover, evenduring the surgical procedure, handling the abdom-inal cavity results in diaphragmatic elevation andfurther increasesthepossibilityofatelectasis.11
AccordingtoMartí-Valeri etal.,12 whostudiedpatients suffering from obstructive apnea sleep syndrome (OASS), aprevalenceof17%of atelectasiswasdiagnosedbychest radiographyafterbariatricsurgery.
However,thereisalackofdataintheliterature concern-ingthe prevalence of atelectasias afterbariatric surgery,
eventhoughitisknownthatthiscouldconstituteoneofthe causesof pulmonarydysfunctionandrespiratoryfailurein thesepatients.
To recognize and identify postoperative respiratory complications after upper abdominal surgery could con-tributetothedevelopmentofpreventivestrategies.
Thehypothesisofthisstudyisthatpatientswithmorbid obesity whoundergo surgery may have a higher index of atelectasisduetoincreasedabdominalfatandtheneedfor generalanesthesia.
The aim of this study was to observe the prevalence of atelectasis in obese and morbidly obese patients who undergogastroplastyusingtheRoux-YGastricBypass tech-nique(RYGB)bylaparotomy,evaluatingthechestX-rays48h aftersurgery,andalsoobservinganyinfluenceoftheBMI, genderorageontheprevalenceofatelectasis.
Methods
Thestudyfollowedethicalguidelinesandwasapprovedby theEthicsCommitteeoftheMethodistUniversityof Piraci-caba,SP,Brazil(protocolnumber09/08).Thisisa retrospec-tivestudyinwhichchestX-rayreportsmadeafterbariatric surgerywereanalyzedatthemomentofhospitaldischarge (48h after surgery). Data were collected for a period of 14 months. The reports were collected fromthe medical recordsofpatientswhohadundergonebariatricsurgery.
OnlypatientssubmittedtoRYGB-type bariatricsurgery by laparotomy, witha BMIabove 35kg/m2, nopulmonary
symptomsorlungdisease,normalpulmonary functiontest and normal preoperative chest X-ray, were included. All patientsweresubmittedtothepulmonaryfunctiontestand hadachestX-ray,butnolungdiseaseswereidentified. Dys-pneawasnotconsideredasarespiratoryco-morbidity,since itiscommoninpatientswithmorbidobesity.
oftheirhospitalstay,leadtoanincreasedriskofpulmonary complications,requirehospitalizationintheIntensiveCare Unit(ICU)ortheuseofcontinuouspressureairwaypressure (CPAP),bi-levelpositiveairwaypressure(BIPAP)therapyor additionaloxygen-therapyapartfromthestandardizedone duringpostoperativerecovery,orwhoshowedunstable post-operativeconditions.
They were submitted to a pre-anesthetic of inhaled sevoflurane and intravenous propofol, with maintenance of the anesthetic by continuous infusion pumping of remifentanil. Neuromuscular blockers (rocuronium, pan-curonium)wereadministeredduringtheprocedureandalso morphine, the latter being administered until complete post-anesthetic recovery,as required. Dipirona and keto-profen were used as analgesics in the ward by way of a periferic catheter.Mechanical ventilation wascarried out usingtheDrägerFabiusGSequipmentinthecontrolled vol-umemodewithatidalvolumeof6---8mL/kg,PEEPof5cm H2Oandinhaledoxygenfractionbetween0.4and0.6.The
patientsremainedinthe hospitalfor threedaysandtheir pre-operative chestX-ray reports showednoparenchymal lungalterationsaccordingtothereportmadebythe radiol-ogist.
In the postoperative period,all patients received con-ventional respiratory physiotherapy twice a day, with deepbreathing,use ofincentivespirometry,resourcesfor bronchial hygiene if needed, active or assisted coughing andassisted walking(at least60m)during thesession. In addition,allpatientstookpartinafollow-uppreoperative multidisciplinary group (doctor,physiotherapist, dietician, psychologistandphysicaltrainer).
The radiological examinationswere carried out during thepostoperativeperiod,i.e.,48hafterbariatricsurgery, beforehospitaldischarge.Therewerefoursessionsof phys-iotherapybeforetakingthechestX-rays,withtwosessions onthefirstpostoperativedayandtwosessionsonthesecond postoperativeday.
The chestX-ray examinationswereevaluatedfromthe report issued by the hospital radiologist. The following criteria were used to detect the presence of atelectasis accordingtoWoodringandReed13:displacementof interlob-ularfissures,pulmonaryopacity,elevationofthediaphragm, displacementof thetrachea,heart, mediastinumand pul-monary hilum, compensatory hyperinflation of the lungs, coming together of the ribs and loss of alveolar volume. Data regarding age, gender, height, current body mass, ideal body weight, body mass excess and BMI were also collected.
The data were processedusing the Statistical Package for Social Sciences for Personal Computers(version 13.0) and the BioStat (version 5.3). The Shapiro---Wilktest was appliedtotestnormalityand,inthecaseofnormality;the data werepresented asthe mean andstandard deviation (SD).Thepatientsincludedwerecomputedinthedatabase alongwiththedemographicanddichotomizedinformation as‘‘yes’’or ‘‘no’’forthefollowing radiographicchanges: atelectasis,cardiacabnormalities,pneumoperitoneum, pul-monary congestion, pleural effusion and pneumonia. The statistical analysis was based on a study of the relation-ship betweenthe resultsof the atelectasisdetectiontest andthevariables:BMI, ageandgender, usingtherelative risk(RR)withaconfidenceintervalof95%.Inaddition,the
Table1 Characteristicsofthegroup:continuousvariables.
Mean±SD Range
Age(years) 36.96±10.16 18---68 Height(cm) 163.40±8.33 142---194 Bodymass(kg) 121.05±21.99 79.8---238.3 Excessbodyweight(kg)a 65.98±20.35 26---174.2 BMI(kg/m2) 45.16±6.33 35.46---74.37
BMI,bodymassindex.
a Based on the ideal body weight recommended by the
MetropolitanLifeFoundation.14
chi-square(G-test)wasusedtoanalyzethestatistical asso-ciationbetweengenderandatelectasis.FortheBMIandage data,cut-offpointswereestablishedfortheanalysis,based onthemedianofthedata.p-Values≤0.05wereconsidered statisticallysignificant.
Results
The mean surgery time was 132±12min. The patients remainedinthepost-anesthesiarecoveryroomforan aver-age of 3h and received a 28% oxygen supply during this period.Whennecessary,theyreceivedanalgesicsaccording toamedicalprescription andrespiratoryphysical therapy twiceadayduringthepost-operativeperiod,including exer-ciseswithdeepandfractionatedinspiration,coughing,use ofarespiratoryencourageranddeambulation.
Ofthe patientswithnormalpreoperative chestX-rays, 413patientswereselected,and theirpostoperativechest X-rays (one per patient) were collected for analysis. Of these,sixpatientsandtheirpostoperativechestX-rayswere excludedbecausetheyweretakenintheexpirationphases, hamperingtheanalysis.Thus407patientsandtheirexams wereanalyzed.Tables1and2summarizethecharacteristics ofthegroup,anditcanbeseenthatwomenmadeupthe majorityofthesample,82.8%.
Table 2 Characteristics of the group: categorical variables.
n %
Gender
Female 337 82.8
Male 70 17.2
BMI
<40 92 22.6
40---49 224 55.04
≥50 84 20.64
Smoker
Yes 32 7.86
No 346 85.01
Ex-smoker
Yes 29 7.13
No 317 77.89
180
154 (37.8%)
80 (19.6%)
39 (9.58%)
23 (5.65%)
14 (3.44%)
8 (1.97%) 160
140
120
100
80
60
40
20
0
Atelectasis Cardiac abnormality Pneumoperitoneum Pulmonary congestion
Pleural effusion
Pneumonia
Figure1 Prevalenceofradiographicalterations.
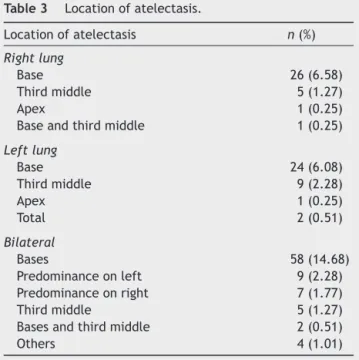
Table3 Locationofatelectasis.
Locationofatelectasis n(%)
Rightlung
Base 26(6.58)
Thirdmiddle 5(1.27)
Apex 1(0.25)
Baseandthirdmiddle 1(0.25)
Leftlung
Base 24(6.08)
Thirdmiddle 9(2.28)
Apex 1(0.25)
Total 2(0.51)
Bilateral
Bases 58(14.68)
Predominanceonleft 9(2.28)
Predominanceonright 7(1.77)
Thirdmiddle 5(1.27)
Basesandthirdmiddle 2(0.51)
Others 4(1.01)
Onanalyzingtheradiologyreportsaprevalenceof37.84%
ofatelectasiswasobservedinthesample(Fig.1),located
mainlyinthelungbases,ascanbeseeninTable3. Itcanbe seenin Table3thatsome patientspresented atelectasisinmorethanone regionofthelung. However, itisworthmentioningthatnoneofthepatientsdiagnosed withatelectasisshowedanyclinicalrepercussions.
Astatisticallysignificantdifferencewasfoundbetween thegendersfortheprevalenceofatelectasis,withgreater prevalenceinwomen(p=0.043).By analyzingtherelative riskaRRof1.48(95%CI0.98---2.21,p=0.02)wasobserved andaratioof40%forwomenand27%formen.When ana-lyzingtheinfluenceofageontheprevalenceofatelectasis anRRof0.68(95%CI0.52---0.88,p=0.001)wasfoundanda ratioof30%forindividualsundertheageof36yearsand45% forindividualsovertheageof36years.TheRRoftheBMI fortheprevalenceofatelectasiswas0.94(95%CI0.73---1.21,
p=0.35)withaprevalence of36%for individualswithBMI below44kg/m2versus38%forindividualswithaBMIabove
44kg/m2.
Discussion
It can be seen that women made up the majority of the sampleinthisstudy,inagreementwiththestudyofOgden etal.15inwhichahigherprevalenceofobesitywasobserved inwomen.
Inbariatricsurgery, several studies have reportedthat obesity isan independentriskfactor for thedevelopment of postoperative complications,5,16,17 and during general anesthesia,pulmonarycomplicationsoftenarise,including atelectasis.7,18Howevertheresultsofthisstudyshowedno increaseintheriskofatelectasisduetotheincreaseinBMI. AccordingtoWoodringandReed,13themorbidlyobesecan show compression atelectasis of the lung parenchyma as a resultofthe abdominalcontents movingthediaphragm in a cephalic direction, which can be aggravated in the supineposition.Duringgeneralanesthesia,atelectasiscan develop,eveninhealthyindividuals,andisassociatedwith anincreasedintra-operativeshunt,leadingtogasexchange impairment.19 Perhapsthe best explanationfor its occur-rence is a dysfunction of the diaphragm by way of an inhibitionofthephrenicnervereflexduringsurgical manipu-lation,withconsequentdiaphragmaticparesis.20Atelectasis appearswithinminutesaftertheinductionofanesthesiaat 85%---90%, and its adverse effects persist in the postoper-ativeperiod,affectingrecoveryofthepatient.10,19,21Such effectsofgeneralanesthesiaaremorepronouncedinobese individuals.
InastudycarriedoutbyEichenbergeretal.10obeseand eutrophicindividualswereaccompaniedbychestcomputed tomography,carriedoutintheperiodsbeforetheinduction ofanesthesia,afterextubationand24haftersurgery.They observedthatatelectasisappearedinbothpatientprofiles aftertheinductionofanesthesia,butintheeutrophic indi-vidualsitwasresolvedinafewhours,whereasitpersisted for up to 24h after surgery in the obeseindividuals. The resultspresentedinthisstudyshowedahighprevalenceof atelectasis(37.84%)inthepopulationofpatientsundergoing bariatricsurgery.Althoughdealingwithlaminaratelectasis, thepresenceofthischangecangenerategreaterimpactin the morbidly obese,who alreadyhave alterations in lung functionandrespiratorymusclemechanics.3,22,23
second day after surgery, or approximately 48h after surgery. The study of Eichenberger et al.10 stopped the assessments24hafterextubation,butthepresentstudystill observed a high prevalence of atelectasis even48h after surgery.
The presenceofatelectasisinthepostoperativeperiod may result in the very frequent complaint of dyspnea in morbidlyobesepatients.24Mostoftheatelectasisobserved inthepresent studywaslocated inthelungbase regions. AccordingtoSood25 theobeseindividualhasincreased air-wayclosureinthedependentregionsofthelungandthereis cephalicdisplacementofthediaphragmduetothe compres-sion of the abdominal contents. In these patients, these alterations are more pronounced after bariatric surgery, adding other factors such as pain, the fear of breathing deeply and suppression of thee cough mechanism, either becauseofpainordecreasedmucociliaryclearancedueto intubation,anesthesiaandanalgesia,causingthe accumu-lationofpulmonarysecretionsandfavoringtheemergence ofatelectasis.26
The hypotheses of this study included the possibilities ofincreasingatelectasiswithincreasingageandBMI.This hypothesis was only confirmed for the age variable, for which,byadoptingthemedianvalueof36years,ahigher prevalenceofatelectasiswasobservedintheoldergroup. The factthat norelationship wasfound betweenBMI and the prevalence of atelectasis can be explained by the sample being composed only of morbidly obese patients, thosemostat riskfordevelopingatelectasis.10 Ifthe sam-ple had been constituted of eutrophic individuals in the samepostoperative clinical conditionsandsurgical proce-dure, maybe the risk observed would have been higher in the morbidly obese patients. As for the female gen-der as a risk factor for the development of atelectasis, one hypothesis which may explain this, at least in part, was the presence of excessively large breasts in these morbidly obese volunteers. According to Cunha et al.,27 big and bulky breasts can have a restrictive effect on thechest,interferingwithrespiratorydynamics,andthey observed an increase in total lung capacity (TLC) and residualvolume(RV) in volunteerssubjected toreductive mastoplasty. The decrease in TLC and RV prior to breast reduction may favor the appearance of pulmonary alter-ations.
Due to the greatrisk of pulmonary complications that patients are exposed to in the post-operative period, it wouldbehelpfultothinkofeffectivemethodstominimize thesecomplications.
One way of preventing the pulmonary complications related to bariatric surgery and other upper abdominal surgeryistheearlyonsetofrespiratorytherapy,with mon-itoringateverystageofinpatientandoutpatientsessions, includingtheuseofincentivespirometryandpositive pres-sure, whichpromotes rapid recovery oflung function and preventstheformationofatelectasis.26,28---32
Thusit wasconcludedthat48hafterbariatricsurgery, theprevalenceofatelectasisinthepopulationinquestion was37%, whichcanbeconsideredrelevant.The atelecta-siswaspredominantlyinthelungbases,andthemainrisk factorsforitsdevelopmentweretobefemaleandover36 yearsofage.
Limitations
of
the
study
Thelimitationofthisstudyisrelatedtothefactthatthere was no group of eutrophic individuals undergoing upper abdominalsurgeryinparallelwiththeobesegroup,inorder tocomparetheprevalenceofatelectasisinthesetwo pop-ulationsandtoestablishtherelativeriskinpatientswitha widerrangeofBMI.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.World Health Organization. Media centre: obesity and over-weight.Genebra:WHO;2012.Available at:http://www.who. int/mediacentre/factsheets/fs311/en/
2.Yurcisin BM, Gaddor MM, DeMaria EJ. Obesity and bariatric surgery.ClinChestMed.2009;30:539---53.
3.McCallisterJW,AdkinsEJ,O’BrienJM.Obesityandacutelung injury.ClinChestMed.2009;30:495---508.
4.Coutinho WF. Consenso latino-americano de obesidade: federac¸ãolatino-americanade sociedadesdeobesidade. Arq BrasEndocrinolMetab.1999;43:21---67.
5.ChungF,MezeiG, TongD.Pre-existingmedicalconditionsas predictorsofadverseeventsinday---casesurgery.BrJAnaesth. 1999;83:262---70.
6.Barbalho-MoulimMC,MiguelGPS,FortiEMP,etal.Silicone-ring roux-en-y gastricbypassinthetreatmentofobesity:effects oflaparoscopicversuslaparotomicsurgeryonrespiration.Obes Surg.2011;21:194---9.
7.CoussaM,ProiettiS,SchnyderP,etal.Preventionof atelec-tasisformationduringtheinductionofgeneral anesthesiain morbidlyobesepatients.AnesthAnalg.2004;98:1491---5.
8.TokicsL,HedenstiernaG,SvenssonL,etal.V/Qdistributionand correlationtoatelectasisinanesthetizedparalyzedhumans.J ApplPhysiol.1996;81:1822---33.
9.Pereira EDB, Farensin SM, Fernandes ALG. Morbidade respi-ratórianospacientescomesemsíndromepulmonarobstrutiva submetidos a cirurgia abdominal alta. Rev Assoc Med Bras. 2000;46:15---22.
10.EichenbergerAS,ProiettiS,WickyS,etal.Morbidobesityand postoperativepulmonaryatelectasis:anunderestimated prob-lem.AnesthAnalg.2002;95:1788---92.
11.TorringtonKG,SorensonDE,SherwoodLM.Postoperativechest percussionwithposturaldrainageinobesepatientsfollowing gastricstapling.Chest.1984;86:891---5.
12.Martí-Valeri C, Sabaté A, Masdevall C, et al. Improve-ment of associated respiratory problems in morbidly obese patients after open Roux-en-Y gastric bypass. Obes Surg. 2007;17:1102---10.
13.WoodringJH, Reed JC. Types and mechanismsof pulmonary atelectasis.JThoracImaging.1996;11:92---108.
14.MetropolitanLifeFoundation.Metropolitanheightandweight tables.StatBull.1983;64:2---9.
15.OgdenCL,YanovskiSZ,CarrollMD,etal.Theepidemiologyof obesity.Gastroenterology.2007;132:2087---102.
17.Rose K, Cohen MM, Wigglesworth DF,et al. Critical respira-tory events in the postanesthesia care unit. Anesthesiology. 1994;81:410---8.
18.PerilliV,SollazziL,BozzaP,etal.Theeffectsofthereverse trendelenburg position on respiratory mechanics and blood gasesinmorbidlyobesepatientsduringbariatricsurgery.Anesth Analg.2000;91:1520---5.
19.LundquistH,HedenstiernaG,StrandbergA, etal.CT assess-ment of dependent lung densities in man during general anaesthesia.ActaRadiol.1995;36:626---32.
20.RamosGC,PereiraE,Gabriel-NetoS,etal.Aspectoshistóricos da pressão arterial de oxigênio e espirometria relaciona-dos à operac¸ão abdominal. ABCD Arq BrasCir Dig. 2009;22: 50---6.
21.DugganM,KavanaghBP.Pulmonary atelectasis:apathogenic perioperativeentity.Anesthesiology.2005;102:838---54.
22.DumontL,MattysM,MardirosoffC,etal.Changesinpulmonary mechanicsduringlaparoscopicgastroplastyinmorbidlyobese patients.ActaAnaesthesiolScand.1997;41:408---13.
23.PelosiP,CrociM,CalappiE,etal.Pronepositioningimproves pulmonaryfunctioninobesepatientsduringgeneralanesthesia. AnesthAnalg.1996;83:578---83.
24.Remístico PPJ, Araújo S, Figueiredo LC, et al. Impact of alveolar recruitment maneuver in the postoperative period of videolaparoscopic bariatric surgery. Rev Bras Anestesiol. 2011;61:163---8.
25.SoodA.Alteredrestingandexerciserespiratoryphysiologyin obesity.ClinChestMed.2009;30:445---54.
26.Smith MCL, Ellis ER. Is retained mucus a risk factor for thedevelopmentofpostoperativeatelectasisandpneumonia? Implicationsforthephysiotherapist.PhysiotherTheoryPract. 2000;16:69---80.
27.CunhaMS,SantosLL,VianaAA,etal.Avaliac¸ãodafunc¸ão pul-monarempacientessubmetidasàmastoplastiaredutora.Rev ColBrasCir.2011;38:11---4.
28.Ebeo CT, Benotti PN, Byrd RP, et al. The effect of bi-level positive airway pressure on postoperative pulmonary function following gastric surgery for obesity. Respir Med. 2002;96:672---6.
29.Jaber S, Delay JM, Chanques G, et al. Outcomes of patientswithacuterespiratoryfailureafterabdominalsurgery treatedwithnoninvasivepositivepressureventilation.Chest. 2005;128:2688---95.
30.ZorembaM,DetteF,GerlachL.Short-Termrespiratoryphysical therapytreatmentinthepacuandinfluenceonpostoperative lungfunctioninobeseadults.ObesSurg.2009;19:1346---54.
31.Forti EMP,IkeD, Barbalho-MoulimM,et al. Effects ofchest physiotherapyontherespiratoryfunctionofpostoperative gas-troplastypatients.Clinics.2009;64:683---9.