w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Assessment
of
prognosis
in
patients
with
stage
II
colon
cancer
Patrícia
Martins,
Sandra
Martins
∗LifeandHealthSciencesResearchInstitute(ICVS),SchoolofHealthSciences,UniversityofMinho,Braga,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14April2015 Accepted28August2015
Availableonline26September2015
Keywords:
Coloncancer
High-andlow-riskstageII Disease-freesurvival Disease-specificsurvival
a
b
s
t
r
a
c
t
Pathologic staging is currently the most important prognostic factor in colon cancer, althoughindividuallythisproceduredoesnotprovideacompleteclinicaloutcome.
Thisstudyaimedtodeterminethedisease-specificsurvivalofpatientswithcolon can-certreatedintheBragaHospitalfromJanuary2005toDecember2013,accordingtothe AmericanJointCommitteeonCancer,6thedition,andthedisease-freesurvivaland disease-specificsurvivalofhigh-andlow-riskstageIIpatients,whetherinuse,ornot,ofadjuvant chemotherapy.
Weobtainedatotalsampleof578patients,with145and65high-andlow-riskstage IIpatients,respectively.Weobserveda5-yeardisease-specificsurvivalrateof93%,27.4% and75%forstageIIA,IIBandIIIApatients,respectively,whereIIIAandIIBpresent statis-ticallysignificantdifferences(p=0.001).Inhigh-riskstageIIpatients,disease-freesurvival (p=0.107)anddisease-specificsurvival(p=0.037)werehigherinthegroupsubmittedto chemotherapy.Inlow-riskpatients,disease-freesurvivalwashigherinthegroupsubmitted tochemotherapy(p=0.494),whiledisease-specificsurvivalwaslower(p=0.426).
ThedifferencesobservedbetweenstageIIBandIIIAsurvivalcanbeexplainedbythe consensualuseofadjuvantchemotherapyinstageIIIA,andbyitscontroversialuseinstage IIB.Adjuvantchemotherapyshowedtobeeffectiveonlyinhigh-riskstageIIpatientsin termsofdisease-specificsurvival.
Inthefuture,othermarkers,namelymolecularones,maybeusedtostratifytheriskof stageIIpatientsanddeterminewhowillbenefitfromadjuvantchemotherapy.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Avaliac¸ão
o
prognóstico
de
pacientes
com
cancer
de
colon
no
estadio
II
Palavras-chave:
Câncerdecólon
EstadioIIdealtoriscoebaixorisco Sobrevivêncialivrededoenc¸a
r
e
s
u
m
o
Oestadiamentopatológicoé,atualmente,ofatordeprognósticomaisimportantedocâncer decólon,emboraindividualmentenãoprevejatotalmenteoresultadoclínico.
Nesteestudo,pretendeu-sedeterminarasobrevivênciaparaumadoenc¸aespecífica(SDE) dospacientescomcâncerdecólontratadosnoHospitaldeBragaentrejaneirode2005e
∗ Correspondingauthor.
E-mail:[email protected](S.Martins).
http://dx.doi.org/10.1016/j.jcol.2015.08.005
Sobrevivênciaparaumadoenc¸a específica
dezembrode2013,deacordocoma6a
edic¸ãodaAmericanJointCommitteeonCancerea SobrevivênciaLivredeDoenc¸a(SLD)eSDEdosdoentesemestadioII,classificadosemalto ebaixorisco,deacordocomarealizac¸ãoounãodequimioterapiaadjuvante.
Obtivemosumaamostratotalde578pacientes,dosquaisumaparcelapertenciaao esta-dioIIdealtooudebaixorisco(145e65pacientes,respetivamente).ObservamosSDEa5 anosde:93%,27,4%e75%paraosestadiosIIA,IIBeIIIA,respetivamente;IIIAeIIB apresen-taramdiferenc¸assignificativas(p=0,001).SLD(p=0,107)eSDE(p=0,037)paraoestadioII dealtoriscoforamsuperioresnogrupotratadocomquimioterapia.Nosdoentesdebaixo risco,SLDfoisuperiornogrupotratadocomquimioterapia(p=0,494),enquantoqueSDEfoi inferior(p=0,426).
Asdiferenc¸asdesobrevivênciaobservadasparaosestadiosIIBeIIIApodemsedeverao usocontroversodaquimioterapiaemIIBeaousoconsensualemIIIA.Ousodaquimioterapia adjuvantedemonstrouserefetivonosdoentesemestadioIIdealtoriscoemtermosdeSDE. Futuramente,outrosmarcadores,nomeadamentemoleculares,poderãoviraser uti-lizadosparaestratificaroriscodoestadioIIedefinirquemsebeneficiarácomotratamento adjuvante.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Theincidenceofneoplasmsandtheassociatedmortalityhave beenincreasingworldwide.1In2012,colorectalcancer(CRC)
wasratedthirdplaceamongneoplasiaswiththehighest inci-dence(1.4millioncases,9.7%)andwasrated4thplaceinterms ofmortality(8.5%)worldwide.2InPortugal,CRCisrated2nd
placeamongneoplasiaswithhighestincidenceand mortal-ityinbothmenandwomen,withanincidenceandmortality of14.8%and15.7%inmenand14.1%and15.9%inwomen, respectively.2In2008,innorthernPortugal,CRCwasthe
sec-ondmostfrequentneoplasia,bothinwomen(15.1%)andmen (18.7%).3
Currently,pathologicstagingisthemostimportant progno-sticfactor,althoughindividuallythisprocedurecannotfully predicttheclinicaloutcome,4–6andthestagingsystemmost
oftenusedistheTumor-Node-Metastasis(TNM)systemofthe AmericanJointCommitteeonCancer(AJCC).Asthestage pro-gressesfrom ItoIV,theoverallfive-yearsurvivalfallsfrom valuesgreaterthan90%(stageI)tolessthan10%(stageIV). StagesIIandIIIhaveoverallsurvivalsof70–85%and25–80%, respectively.7
In recent decades, the prognosis has been improving, thanksto factors suchas an earlierdiagnosis and staging andtreatmentadvances.8–10Morerecently,the6theditionof
AJCC11wasrevised,andits7thedition(2010)iscurrentlyin
use.12
Thus, staging procedures are useful for proposing the prognosis;however,T3-4N0 (stageII)patientshaveaworse Disease-SpecificSurvival(DSS) (87.5%, 79.6%,58.4%)versus T1-2N1a(stageIII)patients(90.7%).13Thissuggeststhatother
factorscontributetothe prognosisofthe patients,namely, thepresenceofperforation orintestinal obstructionatthe timeofdiagnosis,preoperativeincreaseincarcinoembryonic antigen,lowhistologicaldifferentiation,presenceof lympho-vascularandperineuralinvasion,andresectionoflessthan 12 lymph nodes together with the surgical specimen.14,15
ThehigherDSSofT1-2N1apatientswithrespecttostageII can alsobejustifiedbythe factthat, forstageIII patients, the benefitsofadjuvant chemotherapy are established; on the other hand, the use of this therapy still remains con-troversial forstage IIpatients.16,17 This controversyis well
documentedinaliteraturereviewconductedbyAndréetal.,18
inwhich severalstudiesdocumentabsence ofbenefitwith adjuvantchemotherapyforoverallanddisease-freesurvival instageIIpatients,includingthestudyInternational Multi-centrePooledAnalysisofB2ofCancerTrials(IMPACTB2),19the
meta-analysisbyFigueiredoetal.20andameta-analysis
pub-lishedbytheMayoClinic.21Ontheotherhand,theanalysisof
theNationalSurgicalAdjuvantBreastandBowelProject Adju-vantStudies(NSABP)(21),aJapanesemeta-analysis22andthe
studyQuickandSimpleandReliableStudy(QUASAR)23found
benefitsinitsuse,andNSABPnotedthatadjuvant chemother-apyreducesextensivelytheriskofrecurrence.21Thegroup
AdjuvantRectalCancerEndpoints(ACCENT)alsofound bene-fitwiththeuseofadjuvantchemotherapyinstageIIpatients, intermsofsurvival.24
AccordingtotheNationalCancerInstitute,thedecisionto introduceadjuvantchemotherapyforstageIIpatientsmust bemadeindividually;presently,thisprocedureisnotsuitable formostpatients,unlesstheyareincludedinclinicaltrials.25
According to the European Consensus of 2014 for the EuropeanRegistrationofCancerCare(EURECCA),oneshould considertheuseofadjuvantchemotherapyinhigh-riskstage II patients,including those withT4tumors,withless than 10lymphnodesexamined,presentingvenousandlymphatic invasion, with poor tumordifferentiation, and withtumor perforation.26 The same criteriaare usedby the American
Theliteratureisverycontroversialontheroleofadjuvant chemotherapyinstageIIpatients;thus,theaimofthisstudy istocarryoutanassessmentonthistopicinpatientstreated attheBragaHospital.
Materials
and
methods
Thetargetpopulationforthestudyconsistedofpatientswith colonadenocarcinomatreatedattheBragaHospitalbetween January1,2005,andDecember31,2013.Asampleof conve-nience,consistingof578patients,waselaboratedbasedon thefollowinginclusion/exclusioncriteria.
Inclusion criteria: Postoperative histological diagnosis of colonadenocarcinomainpatients whounderwent curative surgicalresectionattheBragaHospitalbetweenJanuary1, 2005,andDecember31,2013.
Exclusion criteria: Patients with a different histological diagnosis from the mentioned above; patients with rec-taladenocarcinoma; patients whodied inthe first 30days after surgery; patients who underwent primary therapy; patients with a personal history of CRC and hereditary syndromes.
Methodology
AprospectiveanalysisoftheColoproctologyUnitdatabaseat theBragaHospitalwasheld,consistingofclinical, patholog-icalandfollow-updata.Subsequently,stageIIpatientswere dividedintotwogroups:oflow-andhigh-risk,basedoncriteria definedbytheEURECCAconsensus.26
Thisproject was approvedbythe Ethics Committee for Healthandbythe EthicsSubcommitteeforLifeandHealth SciencesoftheBragaHospital.
Statisticalanalysis
ThecollecteddatawereanalyzedusingtheStatisticalPackage forSocialSciences (SPSS)software, version19.0 (SPSS Inc., Chicago,IL,USA).
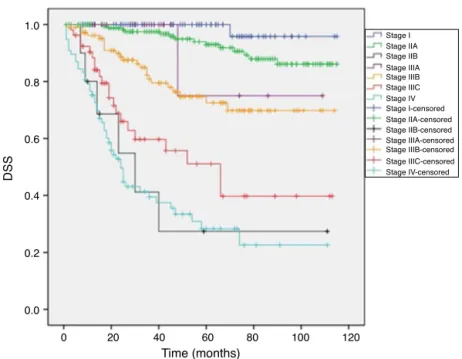
Forthetotalsampleofpatients,adescriptiveanalysisof variableswasperformed.Next,Kaplan–MeiercurvesforDSS andforthedifferentstagesofAJCC(6thedition)wereobtained. TheLog-Ranktest(Mantel–Cox),withasignificancesetin0.05, wasappliedtodetectdifferencesofDSSbetweengroups. Five-yearDSSwasdeterminedforallgroups.
Kaplan–Meiercurves forDFSandDSS wereobtainedfor high-andlow-riskstageIIpatients,accordingtotheuseor non-useofadjuvantchemotherapy.
TheLog-Ranktest(Mantel–Cox),withasignificancesetin 0.05,wasappliedtodetectdifferencesofDSSandDFSamong thegrouptreatedwithadjuvantchemotherapyversus non-treatedgroup.Five-yearDSSandDFSweredeterminedforall groups.
DFSisdefinedastheperiodfromsurgerytorecurrenceof disease,andDSSastheperiodfromsurgeryuntilthepatient’s diedfromthedisease.
Results
Samplecharacterization
The study population consists of 578 individuals; 61.9% (n=358)malesand38.1%(n=220)females.Themeanageat thetimeofsurgerywas67.9years.
As regards to the pathological staging, the study popu-lation had thefollowing characteristics:47.8% (n=276) had nodalmetastasesand14.4%(n=83)werealreadywithdistant metastases.
Asfortheadministrationofadjuvantchemotherapy,this procedurewasperformedin54.7%(n=316)ofpatients,while 34.4% (n=199) were not treated. During follow-up, 75.8% (n=375)showednorecurrence ofthe disease;ontheother hand,in18.4%(n=91)therewasarecurrence.Overall,19.9% (n=115)diedfromthedisease.
DSSanalysis,accordingtoAJCC(6thedition)
The mean DSS was calculated for the different stages, as follows:StageI, 113.1months(95%confidenceinterval[CI]: 109.5–116.7); stage IIA, 107.2 months (95% CI: 103.3–111.1); stage IIB, 46.4 months (95% CI: 17.9–74.9); stage IIIA, 93.8 months(95%CI:67.9–119.6);stageIIIB,89.7months(95%CI: 81.2–98.2);stageIIIC,63.3months(95%CI:48.5–78.1);andstage IV, 43.7 months (95% CI:33.3–54.1). Themean DSS of this sampleis90.6months(95%CI:86.7–94.5).Inpaired compar-isonsbetweenstages,statisticallysignificantdifferencesfor DSShavebeenfoundinmostcases,wheretheLog-Ranktest obtainedap-valuelowerthan0.05,exceptbetweenstagesI andIIA(Log-Rank=2.896;p=0089);IandIIIA(Log-Rank=3.658;
p=0.056); IIA and IIIA (Log-Rank=0.109; p=0741); IIB and IIIC(Log-Rank=1.232;p=0.267);IIBandIV(Log-Rank=0.036;
p=0.850);andIIIAandIIIB(Log-Rank=1.749;p=0.186). With regard to the five-yearDSS by stage,we observed 100%forstageI;93%(95%CI:88.5–97.5%)forstageIIA;27.4% (95% CI:0–59.2%)forstageIIB; 75%(95% CI:32.5–100%)for stageIIIA;72.5%(95%CI:62.3–82.7%)forstageIIIB;51.1%(95% CI:33.9–68.3%)forstageIIIC;and28.3%(95%CI:16.3–40.2%) for stage IV. The five-year DSS sample is 75.4% (95% CI: 71.1–79.7%).ThesurvivalcurvesareshowninFig.1.
Low-riskstageIIpatients’groupassessment
Thelow-riskgroup consistedof65individuals,60% (n=39) maleand40%(n=26)female.Themeanageatdiagnosiswas 69.9years.
Asfortheadministrationofadjuvantchemotherapy,this procedurewasperformedin44.6%(n=29)ofpatients,while 40%(n=26)werenotthustreated.
Duringthefollow-up,13.8%(n=9)presentedrecurrenceof thediseaseand3.1%(n=2)diedfromthedisease.Allpatients who died belonged to the group that underwent adjuvant chemotherapy.
DSS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
20 40 60 80 100 120
Stage I
Stage I-censored Stage IIA
Stage IIA-censored Stage IIB
Stage IIB-censored Stage IIIB
Stage IIIB-censored Stage IIIC
Stage IIIC-censored Stage IV
Stage IV-censored Stage IIIA
Stage IIIA-censored
Fig.1– DSSforeachstageofAJCC(6thedition).
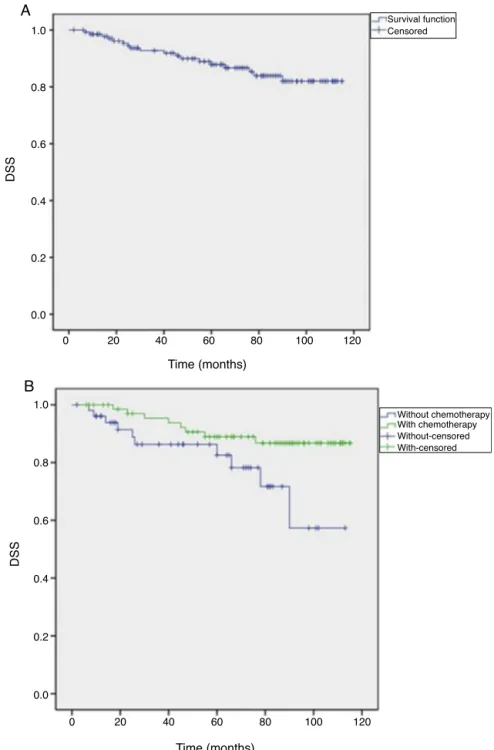
who underwent adjuvant chemotherapy was 82.4 months (95%CI:68.1–96.7),and forthegroup notthus treated,the meanDFSwas59.2months(95%CI:54.1–64.3).TheDFS differ-encesbetweenthetwogroupsarenotstatisticallysignificant (Log-Rank=0.468;p=0.494).
Themeanfive-yearDFSforthelow-riskgroupwas71.3% (95%CI:52.1–90.5%);forthegroupthatunderwent chemother-apy, the mean five-year DFSwas 71.8% (95% CI:51.6–92%) versus63.8%(95%CI:12.4–100%)forthegroupnotthustreated. ThesurvivalcurvesareshowninFig.2(AandB).
Themean DSS forthe low-risk stage IIgroup was 98.9 months(95%CI:90.9–106.9).ThedifferencesofDSSbetween thegroupthatunderwentchemotherapyversusthegroupnot thustreatedwasnotstatisticallysignificant(Log-Rank=0634,
p=0.426).
Themeanfive-yearDSS forthe low-riskgroupwas96% (95%CI:88.4–100%);93.8%(95%CI:81.8–100%)forthegroup thatunderwentchemotherapyversus100%forthegroupnot thustreated.ThesurvivalcurvesareshowninFig.3(AandB).
High-riskgroup
Thehigh-riskgroupconsistedof145subjects, 62.1%(n=90) malesand37.9%(n=55)females.Themeanageatdiagnosis was70.9years.
Asfortheadministrationofadjuvantchemotherapy,this wascarriedoutin49%(n=71)ofpatients,while35.9%(n=52) didnotundergothisprocedure.
Duringthefollow-up,17.2%(n=25)ofpatientshaddisease recurrenceand12.4%(n=18)diedfromthedisease.
Theprognosisforhigh-riskpatientswhounderwent adju-vantchemotherapywascomparedtothatforthosewhowere notthustreated.ThemeanDFSforthehigh-riskstageIIgroup was96.5months(95%CI:89.9–103).Inthegroupthat under-went chemotherapy, the mean DFS was 98.8 months(95%
CI: 90.3–107.2) versus 85 months (95%CI: 72.1–97.9) in the groupnotthustreated.ThedifferencesinDFSbetweenthe twogroupsarenotstatisticallysignificant(Log-Rank=2.598;
p=0.107).
Thefive-yearDFSforhigh-riskstageIIgroupwas80.5% (95%CI:73.4–87.6%),with83.4%(95%CI:74.4–92.4%)forthose patients who underwent chemotherapyand68.8% (95%CI: 54.1–83.5%)forthosenotthustreated.Thesurvivalcurvesare showninFig.4(AandB).
ThemeanDSSforhigh-riskstageIIgroupwas102.8months (95% CI: 97.5–108). Patients who underwent chemotherapy presentedameanDSSof105.5months(95%CI:99.3–111.8) and those whose procedure was notcarried out the mean DSSwas90.3months(95%CI:78.4–102.2).Thedifferencesin DSSbetweenthetwogroupsarestatisticallysignificant (Log-Rank=4.337;p=0.037).
Themeanfive-yearDSSinhigh-riskstageIIpatientswas 87.9%(95%CI:81.8–94%);inpatientsundergoing chemother-apythisvaluewas88.9%(95%CI:81.1–96.7%);andinpatients notsubmittedtochemotherapythisvaluewas82.5%(95%CI: 70.3–94.7%).
ThesurvivalcurvesareshowninFig.5(AandB).
Discussion
DFS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
A
Survival FunctionCensored
20 40 60 80 100 120
DFS
Time (months)
B
0.0 0.2 0.4 0.6 0.8 1.0
Without chemotherapy With chemotherapy Without-censored With-censored
0 20 40 60 80 100 120
Fig.2–(A)DFSoflow-riskstageIIpatients;(B)DFSaccordingtotheadministrationofchemotherapy,forlow-riskstageII patients.
similar values are also observed.17 The insufficient
num-ber ofindividuals inour sample for each stage may have beenonefactorresponsibleforthedifferencesbetweenour resultsandtheliteraturefindings,andalsobytheabsence ofstatisticallysignificant differencesinDSS betweensome stages.
Inourstudy,asinotherstudiesreviewed,DSSforIIIAis higherthantoDSSforIIB(p=0.001).17Althoughcareshouldbe
takenininterpretingthisdata(inthefaceofthelownumberof patientswithstageIIB),thisfactmaybeduetotheconsensual useofadjuvantchemotherapyinpatientsinstageIII,and,on theotherhand,tothecontroversialuseofthisprocedurein patientswithstageII.16,17
Reviewing the literature, we note that the use of adju-vantchemotherapyinpatientsinstageIIisnotconsensual,16
as several studies documenting the lack of benefit were published,18–21whileotherstudiesshowevidenceofgainwith
thisprocedure,21–24stressingthatonlysmallabsolute
bene-fitswillbeobtainedinthefaceoftheriskofovertreatment, includingtoxicity.23Thus,theuseofadjuvantchemotherapy
inpatientswithstageIIwillbeonlyrecommendedfor high-riskpatients.26,27
Time (months)
DSS
0 0.0 0.2 0.4 0.6 0.8 1.0
A
B
Survival function Censored
20 40 60 80 100 120
Time (months)
DSS
0 0.0 0.2 0.4 0.6 0.8 1.0
Without chemotherapy With chemotherapy Without-censored With-censored
20 40 60 80 100 120
Fig.3–(A)DSSoflow-riskstageIIpatients;(B)DSSaccordingtotheadministrationofchemotherapy,forlow-riskstageII patients.
DFS and DSS were also higher in the group that under-wentadjuvantchemotherapy(83.4%and88.9%,respectively) compared with the non-treated group (68.8% and 82.5%, respectively).DFSvaluesyieldednotstatisticallysignificant results(p=0.107);ontheotherhand,theresultsobtainedfor DSS were statisticallysignificant (p=0.037).These data are consistent withseveral studies showingthe benefit ofthe adjuvantchemotherapyintermsofoverallsurvivalandDFS. Grandeet al.28 studiedhigh-risk stageIIA patients, having
foundhigheroverallsurvivalsandfive-yearDFSinpatients receivingadjuvantchemotherapy,comparedtopatients sub-mittedonlytosurgery. Inthe MOSAICstudy, theirauthors
demonstratedthattheuseofFOLFOX4reducedtherelative riskofrelapsein28%ofhigh-riskstageIIpatients.29NSABP21
showedsomebenefitwiththeuseofchemotherapyintermsof survivalforstageIIpatientswithapoorprognosis(T4tumors, obstruction,perforation).InthestudybyKumaretal.,30these
authorsfoundstatisticallysignificantbenefitsoftheadjuvant chemotherapyintermsofDFSandDSSonlyforpatientswith T4tumors.
DFS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
A
B
Survival Function Censored
20 40 60 80 100 120
DFS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
Without chemotherapy With chemotherapy Without-censored With-censored
20 40 60 80 100 120
Fig.4–(A)DFSofhigh-riskstageIIpatients;(B)DFSaccordingtotheadministrationofchemotherapy,forhigh-riskstageII patients.
thedifferencesbetweengroupswerenotstatistically signif-icant (p=0.494). Thefive-year DSS was 100%forthe group thatdidnotreceive chemotherapy,and93.8%forthegroup thus treated; but caution is needed in interpreting these data,takingintoaccountthesmall numberofevents(two) inthis patientgroup.Thedifferencesbetweengroupswere notstatisticallysignificant (p=0.426). Grandeetal.28 found
statistically significant differences in favor of the use of chemotherapyintermsofoverallsurvivalandoffive-yearDFS, howeverKumaretal.30foundthattheuseofchemotherapy
wasassociatedwithworseDFSandDSS.
DSS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
Survival function Censored
A
20 40 60 80 100 120
DSS
Time (months)
0 0.0 0.2 0.4 0.6 0.8 1.0
Without chemotherapy With chemotherapy Without-censored With-censored
B
20 40 60 80 100 120
Fig.5–(A)DSSofhigh-riskstageIIpatients;(B)DSSaccordingtotheadministrationofchemotherapy,forhigh-riskstageII patients.
Conclusion
Pathologicstagingis currentlythe mainindicator ofcolon cancerprognosis,althoughindividuallythisprocedurecannot fullypredictclinicaloutcome.Accordingtotheliterature,we foundinoursamplethatstageIIIApatientspresenthigher DSSversusstageIIBpatients(p=0.001),althoughonemust bearinmindthesmallnumberofpatientsinthesetwostages, and this can also justify why the absolute values of five-yearDSS differfrom those described inthe literature.One canjustifythissituationwiththeconsensualuseofadjuvant
chemotherapyinstageIIIpatients,anditscontroversialuse instageIIpatients.Fortheremainingstages,thevaluesare closetothosedescribedintheliterature.
In our study, the use of adjuvant chemotherapy was effectiveforDSSonlyinhigh-riskstageIIpatients.For the remainingparametersevaluated,theresultswere controver-sialandnotstatisticallysignificant,whichcouldberelatedto thesmallnumberofpatients,tocensorshipandtotheabsence ofrandomizedstudygroups.
usedtostratifythestageIIriskandtodefinewhowillbenefit fromadjuvanttherapy.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. StewartBW,WildCP.InternationalAgencyforResearchon Cancer.WorldCancerReport;2014.Availablefrom:http:// www.iarc.fr/en/media-centre/pr/2014/pdfs/pr224E.pdf
[accessed18.06.14].
2. GLOBOCANFactsheet.Availablefrom:http://globocan.iarc.fr/ Pages/factsheetscancer.aspx[accessed18.06.14].
3. Top10-Roreno-RegistoOncológicodoNorte(Internet). Availablefrom:http://www.roreno.com.pt/pt/estatisticas. html[accessed18.06.14].
4. BarozziC,RavaioliM,D’ErricoA,GraziGL,PoggioliG,Cavrini G,etal.Relevanceofbiologicmarkersincolorectalcarcinoma: acomparativestudyofabroadpanel.Cancer.2002;94:647–57.
5. SaadRS,LiuYL,NathanG,CelebrezzeJ,MedichD,Silverman JF.Endoglin(CD105)andvascularendothelialgrowthfactoras prognosticmarkersincolorectalcancer.ModPathol. 2004;17:197–203.
6. Gómez-DomínguezE,Trapero-MarugánM,delPozoAJ, CanteroJ,GisbertJP,MatéJ.Thecolorectalcarcinoma prognosisfactors.Significanceofdiagnosisdelay.RevEsp EnfermDig.2006;98:322–9.
7. MeyerhardtJA,MayerRJ.Systemictherapyforcolorectal cancer.NEnglJMed.2005;352:476–87.
8. AbdallaEK,VautheyJN,EllisLM,EllisV,PollockR,BroglioKR, etal.Recurrenceandoutcomesfollowinghepaticresection, radiofrequencyablation,andcombinedresection/ablationfor colorectallivermetastases.AnnSurg.2004;239:818–25, discussion825–27.
9. LangK,KornJR,LeeDW,LinesLM,EarleCC,MenzinJ.Factors associatedwithimprovedsurvivalamongoldercolorectal cancerpatientsintheUS:apopulation-basedanalysis.BMC Cancer.2009;9:227.
10.BrennerH,HoffmeisterM,ArndtV,HaugU.Gender differencesincolorectalcancer:implicationsforageat initiationofscreening.BrJCancer.2007;96:828–31.
11.GreeneF,BalchCM,FlemingID,etal.,editors.AJCCcancer stagingmanual.6thed.Springer;2002.
12.EdgeS,ByrdDR,ComptonCC,FritzAG,GreeneFL,TrottiA. AJCCcancerstagingmanual.7thed.Springer;2010.
13.GundersonLL,JessupJM,SargentDJ,GreeneFL,StewartAK. RevisedTNcategorizationforcoloncancerbasedonnational survivaloutcomesdata.JClinOncol.2010;28:264–71.
14.DotanE,CohenSJ.ChallengesinthemanagementofstageII coloncancer.SeminOncol.2011;38:511–20.
15.WolpinBM,MayerRJ.Systemictreatmentofcolorectal cancer.Gastroenterology.2008;134:1296–310.
16.GillS,LoprinziCL,SargentDJ,ThoméSD,AlbertsSR,Haller DG,etal.Pooledanalysisoffluorouracil-basedadjuvant
therapyforstageIIandIIIcoloncancer:whobenefitsandby howmuch?JClinOncol.2004;22:1797–806.
17.O ´ConnellJB,MaggardMA,KoCY.ColonCancerSurvivalrates withthenewAmericanJointCommitteeonCancersixth editionstaging.JNatlCancerInst.2004;96:1420–5.
18.AndréT,AfchainP,BarrierA,BlanchardP,LarsenAK, TournigandC,etal.Currentstatusofadjuvanttherapyfor coloncancer.GastrointestCancerRes.2007;1.
19.IMPACTB2investigators.Efficacyofadjuvantfluorouraciland folinicacidinB2coloncancer.JClinOncol.1999;17:1356–63.
20.FigueiredoA,CharretteM,MarounJ,BrouwersMC,ZurawL. AdjuvanttherapyforstageIIcoloncancer:asystematic reviewfromtheCancerCareOntarioProgramin
Evidence-BasedCare’sGastrointestinalCancerDiseaseSite Group.JClinOncol.2004;22:3395–407.
21.MamounasE,WieandS,WolmarkN,BearHD,AtkinsJN,Song K,etal.Comparativeefficacyofadjuvantchemotherapyin patientswithDukes’BvsDukes’Ccoloncancer:resultsfrom fourNationalSurgicalAdjuvantBreastandBowelProject AdjuvantStudies(C-01,C-02,C-03eC-04).JClinOncol. 1999;17:1349–55.
22.SakamotoJ,OhashiY,HamadaC,BuyseM,BurzykowskiT, PiedboisP,Meta-AnalysisGroupoftheJapaneseSocietyfor CanceroftheColonandRectum;Meta-AnalysisGroupin Cancer.EfficacyofOralAdjuvantTherapyAfterResectionof ColorectalCancer:5-YearResultsFromThreeRandomized Trials.JClinOncol.2004;22:484–92.
23.QUASARstudy–QUASARCollaborativeGroup.Adjuvant chemotherapyversusobservationinpatientswithcolorectal cancer:arandomizedstudy.Lancet.2007;370:2020–9.
24.SargentDJ,SobreroA,GrotheyA,etal.Evidenceforcureby adjuvantchemotherapyincoloncancer:observationsbased onindividualpatientdatafrom20898patientson18 randomizedtrials.JClinOncol.2009;27:872–7.
25.NationalCancerInstitute–StageIIColonCancerTreatment (Internet).Availablefrom:http://www.cancer.gov/
cancertopics/pdq/treatment/colon/HealthProfessional/page7
[accessed11.09.14].
26.VandeVeldeCJ,BoelensPG,BorrasJM,CoeberghJW, CervantesA,BlomqvistL,etal.EURECCAcolorectal:
multidisciplinarymanagement:Europeanconsensus
conferencecolon&rectum.EurJCancer.2014;50,1.e1–1.e34.
27.BensonAB3rd,SchragD,SomerfieldMR,CohenAM, FigueredoAT,FlynnPJ,etal.AmericanSocietyofClinical
Oncologyrecommendationsonadjuvantchemotherapyfor
stageIIcoloncancer.JClinOncol.2004;22:3408–19.
28.GrandeR,CorsiD,ManciniR,GemmaD,CiancolaF,Sperduti I,etal.Evaluationofrelapse-freesurvivalinT3N0colon cancer:theroleofchemotherapy,amulticentricretrospective analysis.PLoSOne.2013;8:e80188.
29.HickishT,BoniC,NavarroM,TaberneroJ,TophamC,Bonetti A,etal.FOLFOX4asadjuvanttreatmentforstageIIcolon cancer:subpopulationdatafromtheMOSAICtrial.2004ASCO AnnualMeetingProceedings.JClinOncol.2004;22,abstr 3619.