w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Postoperative
mortality
in
inflammatory
bowel
disease
patients
Renato
Vismara
Ropelato
∗,
Paulo
Gustavo
Kotze,
Ilário
Froehner
Junior,
Danieli
D.
Dadan,
Eron
Fábio
Miranda
PontifíciaUniversidadeCatólicadoParaná(PUCPR),HospitalUniversitárioCajuru(SeCoHUC),UnidadedeCirurgiaColorectal,Curitiba, PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received30November2016 Accepted16January2017 Availableonline3February2017
Keywords:
Mortality Crohn’sdisease Ulcerativecolitis Surgery
a
b
s
t
r
a
c
t
Introduction:Sincethe1960s,mortalityinCrohn’sdiseaseandUlcerativeColitispatientshad asignificantdecreaseduetoadvancesinmedicalandsurgicaltherapy.Animportant pro-portionofthesepatientsaresubmittedtosurgicalproceduresduringtheirdiseasecourse, withpostoperativemortalitybetween4and10%.
Methods:157inflammatoryboweldiseasepatientssubmittedtosurgicaltherapywere retro-spectivelyidentifiedandallocatedin2groups(Crohn’sandcolitis).Deathswereindividually discriminatedindetail.
Results:281surgicalprocedureswereperformed.Inthecolitisgroup,43operationswere performedin24patients;intheabdominalCrohn’ssubgroup,127proceduresin90patients andintheperinealCrohn’ssubgroup,115in64patients,respectively.Ninepostoperative deathswereobserved(3inthecolitisand6intheCrohn’sgroups).Overallpostoperative mortalitywas5.7%(4.5%forCrohn’s;6.6%inabdominalCrohn’sand12.5%forColitis).Most ofdeathswererelatedtoemergencyproceduresandprevioususeofcorticosteroids.The causeofdeathinallpatientswassepsis.
Conclusions:Overallpostoperativemortalityininflammatoryboweldiseasewas5.7%,andit wasattributedtotheseverityofthecasesreferred.
©2017SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.This isanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Mortalidade
em
portadores
de
doenc¸a
inflamatória
intestinal
submetidos
a
tratamento
cirúrgico
Palavras-chave:
Mortalidade Doenc¸adeCrohn
r
e
s
u
m
o
Introduc¸ão:Apartirdadécadade60,amortalidadedosportadoresdedoenc¸adeCrohn(DC)e aRetocoliteUlcerativaInespecífica(RCUI)tevedeclíniodevidoanovasterapêuticasclínicas ecirúrgicas.Importanteproporc¸ãodestespacientesésubmetidaaprocedimentoscirúrgicos nodecorrerdassuasvidas,comtaxasdemortalidadevariandoentre4e10%.
∗ Correspondingauthor.
E-mail:[email protected](R.V.Ropelato).
http://dx.doi.org/10.1016/j.jcol.2017.01.001
jcoloproctol(rioj).2017;37(2):116–122
117
Retocoliteulcerativa Cirurgia
Método:Foramidentificadosretrospectivamente157pacientesportadoresdedoenc¸as infla-matóriasintestinais(DII),submetidosaoperac¸õesabdominaisouperineais,divididosem doisgrupos(DCeRCUI).Oscasosdeóbitosforamdiscriminadoseavaliados individual-mente,deformadescritiva.
Resultados: 281operac¸õesforamrealizadas.NogrupoRCUIforamrealizadas43operac¸ões em24pacientes,nosubgrupoDCabdominal,127operac¸õesem90pacientesenosubgrupo DCperineal,115em64pacientes,respectivamente.Dototalde9óbitos,3ocorreramno grupoRCUIe6noDC.AmortalidadegeralnasDIIfoide5,7%.ParaaDC,4,5%.Nosubgrupo deoperac¸õesabdominaisfoide6,6%eparaaRCUI12,5%.Amaiorpartedosóbitosestavam relacionadosaprocedimentosdeurgência/emergência,comusopréviodecorticoterapia.A
causamortisemtodosospacientesfoisepse.
Conclusões: AtaxademortalidadecirúrgicanasDIIfoide5,7%,atribuidaspelaseveridade doscasos.
©2017SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Introduction
Crohn’sdisease(CD)andUlcerativeColitis(UC)presentanot homogeneousandincreasingglobalincidenceovertheyears. Due to the heterogeneous demographic character among countries,the incidenceofUCvaries between8–14/100,000 and120–200/100,000people;ontheotherhand,theincidence ofCDvariesbetween6–15/100,000and50–200/100,000.1
From the1960s onwards,the mortalityofpatients with thesediseases,mainlyUC,showedasignificantdeclinedue totheuseofnewclinicalandsurgicaltherapeuticmeasures.2
InthecaseofCD,thereisalowrisk,but theriskofdeath ishigherversusgeneralpopulation (consideringindividuals ofthe sameageand gender).Ameta-analysispointed toa downwardtrendinmortalityratesoverthelast30years,but withoutstatisticalsignificance.3InUC,anothermeta-analysis
showedthatthetotalmortalityofpatientsdidnotdifferfrom thegeneralpopulation,althoughinsubgroupsofpatientswith amoresevereandextensivedisease(andthatconsequently madeuseofimmunosuppressivemedication)theriskofdeath washigher.4
A significant proportion of patients with inflammatory boweldisease(IBD)willundergosurgicalprocedures through-outtheirlives.InCD,bowelsurgeryisneededinabout70–80% ofcases after 20 years of illness. Of these patients, about 30%willrequireasecondsurgeryafter10years.1Inpatients
withUC,colectomiesare requiredinapproximately20–30% ofpatientsafter25yearsofdisease.1Consideringthewhole
rangeofoperativeprocedures,intestinalresectionsinpatients withIBDperformedonanemergencybasisareassociatedwith highermortalityrates.Inadditiontotheincreasedriskdue totheurgencyrequiredperse,atthetimeofsurgery,many patientsaremalnourished andinthe useofdrugssuchas corticosteroids,immunosuppressantsandbiologicalagents, whichmayhaveanimpactonmorbidityandmortality.5
The use of tumor necrosis factor alpha (anti-TNF␣)
inhibitorshasalteredthe naturalhistoryofthe disease.In randomizedstudies,the reductionofcomplicationsand of theneedforsurgeryhasalreadybeendemonstrated.Onthe other hand,in populationalstudies, this has notyet been documented.5
Theprimaryobjectiveofthisstudywastodeterminethe mortalityrateamongpatientswithIBDinareferralservicefor themanagementofCNandNSUCpatientsundergoing surgi-calprocedures.Thesecondaryobjectivesweretodescribethe demographiccharacteristicsofthispopulation,aswellasto makeadetailedevaluationofthecasesofdeath,relatingthem topossibleriskfactors.
Method
ThisstudywasapprovedbytheResearchEthicsCommitteeof theBioethicsNucleusofthePontifíciaUniversidadeCatólica doParaná(PUC-PR),accordingtothePresentationCertificate forEthicalAppreciation(CAAE)number58325916.6.0000.0020, providedbythePlataformaBrasilwebsite..
Thiswasaretrospective,analyticalandlongitudinalstudy ofaseriesofcases.157patientssubmittedtosurgical proce-duresrelatedtoIBDfromJanuary2004toDecember2014ina referralservicewereidentified.Thesepatientsweredivided into groups according to the diagnosis (UC and CD). The CD group wasfurtherdivided into twosubgroups: abdom-inal procedures and perineal procedures. After reviewing the patient’s medicalrecords, the followingvariables were analyzed: age,gender,indicationofsurgery,procedure per-formed,thesystemofdesignationoftheprocedure(electiveor urgent)anddeathinthepostoperativeperiod.Previous treat-ments(clinicaland surgicalones)andinparticularthe use ofcorticosteroidsandanti-TNF␣ agentswere analyzed.The
occurrenceofmalnutrition(definedasaserumalbuminvalue below 3.0mg/dL), use oftotal parenteral nutrition, anemia (definedasahemoglobinemia[Hb]<8g/dL),andtheneedfor bloodtransfusionwereequallychecked.Thetypeofsurgery performed and thepre-operativehospitalization timewere alsoanalyzed.Thecasesofdeathwereindividually discrimi-natedandevaluated.SurgicalproceduresnotrelatedtoIBDs wereexcludedfromtheanalysis.
Results
Table1–Distributionofpatientsinrelationtogenderanddisease,withnumbersofpatientsoperatedbygroup.
Crohn’sdisease(CD) Ulcerativecolitis(UC) Total
Male Female Male Female
Patients(n) 75 58 15 9 157
Surgicalprocedures(n) 135 104 27 16 281
Meanage 34.2(12–65) 41.5(15–82) 37.7(19–76) 40.6(14–64) 36.2(12–82)
CD)wereanalyzed.Themeanagewas36.2years.Thesedata aredetailedinTable1.
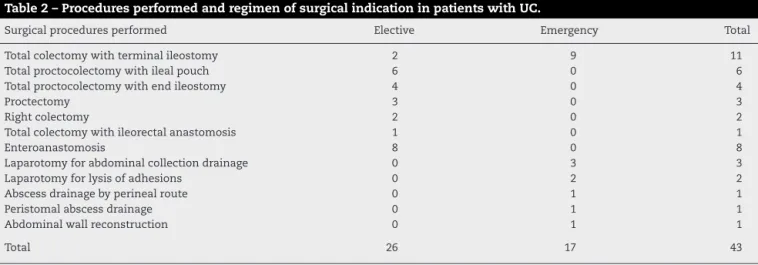
In the UC group, 43 operations were performed in 24 patients.Themeannumberofsurgicalproceduresperpatient was1.79(1–4).Thetypesofoperationsandtheirindications arelistedinTable2.Asobserved,amongtheprocedures,17 wereperformedonanemergencybasis.Theelectivesurgical indicationswere:refractorydisease,intestinaltransit recon-struction, dysplasia-associated lesion or mass (DALM),and stenosis. The surgical indications of emergency were: dis-easerefractorytomedicaltreatment,abdominalabscessor collection,toxicmegacolon,intestinalobstruction,and evis-ceration. The mostcommon surgical indication– both for electivesurgeryandforemergencysurgery–was refractori-nesstomedicaltreatment.Inthisgroup,3deathsoccurred. Still,inthisgroup,themortalityrateoftotalcolectomywith endileostomyintheemergencyroomreached30%.
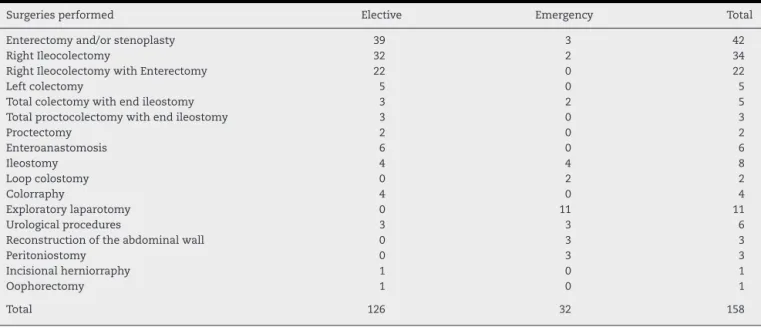
InthegroupofpatientswithCD,238operationswere car-riedoutin133patients(meanageof35.6years;Table3).In 7cases,abdominalandperinealprocedureswereperformed duringthesamesurgicaltime.Themeannumberof surger-iesperpatientwas1.4(1–5).IntheabdominalCDsubgroup, 32operationswerecarriedoutonanemergencybasis. Sur-gical indications in patients with CD were, among others: localizedileocolicdisease,stenoses,fistulas,refractorinessto medicaltreatment, perineal disease,intestinal obstruction, anabdominalcollectionoranastomoticdehiscence, intesti-nal perforation, evisceration, stoma necrosis, hemorrhage, abdominalwall/peristomalabscess,andbladderfistula.The mostcommon indicationinelectiveprocedureswas steno-sis;ontheotherhand,intheemergencysurgeries,themost common indication was abdominal collection/anastomotic
dehiscence (Table 3). There were 6 related deaths in the abdominalCDsubgroup.
InthegroupofpatientsoperatedonforCD,115perineal operations wereperformedin64patients(perinealCD sub-group): 39 men(mean age36 years) and 25women (mean age31.9years).Themeannumberofproceduresperpatient was1.79(1–8proceduresperpatient).101fistulotomiesand 19 other procedures (drainage of abscess, anal dilatation, debridement,andfissurectomy)werecarriedout.Therewere nodeathsinthissubgroup.
Amongthepatientsanalyzed,9deathswereidentified,3 (1maleand 2female)intheUCgroupand6(4maleand2 females)intheCDgroup.Themeanageofthecasesofdeath was 37.3(14–77) years.Theoverall mortalityratewas5.7% (9/157patients).FortheCDgroup,themortalityratewas4.5% (6/133patients);inthesubgroupofabdominaloperationsthe mortalityratewas6.6%(6/90patientsoperated),andintheUC group,12.5%(3/24patientsoperated).Thesedataaredetailed inTable4.
The9patientswhodiedhadundergone27operations(1–6 procedures).Inonlytwocases,onlyoneoperationwas per-formedduringhospitalization.Amongthesesurgeries,asa mainprocedure6colectomies(withorwithoutenterectomy), threeenterectomies,threeperinealprocedures,and15 proce-duresofothertypeswereperformed(Table5).
In the 3 UC-related deaths, the disease had a pancoli-tispresentation.Allofthesepatientsunderwentintravenous (IV)corticosteroidtherapy,oneofthemhadbeentakingoral mesalazineforlessthanaweek,anotherhadused azathio-prine,andthethirdhadundergoneasingle-doseinfusionof infliximab twodays beforesurgery. Noneof thesepatients hadanyprevioussurgeryrelatedtoIBD.Allweresubmitted
Table2–ProceduresperformedandregimenofsurgicalindicationinpatientswithUC.
Surgicalproceduresperformed Elective Emergency Total
Totalcolectomywithterminalileostomy 2 9 11
Totalproctocolectomywithilealpouch 6 0 6
Totalproctocolectomywithendileostomy 4 0 4
Proctectomy 3 0 3
Rightcolectomy 2 0 2
Totalcolectomywithileorectalanastomosis 1 0 1
Enteroanastomosis 8 0 8
Laparotomyforabdominalcollectiondrainage 0 3 3
Laparotomyforlysisofadhesions 0 2 2
Abscessdrainagebyperinealroute 0 1 1
Peristomalabscessdrainage 0 1 1
Abdominalwallreconstruction 0 1 1
jcoloproctol(rioj).2017;37(2):116–122
119
Table3–ProceduresperformedandregimenofsurgicalindicationforsurgeriesinpatientswithCD(abdominal subgroup).
Surgeriesperformed Elective Emergency Total
Enterectomyand/orstenoplasty 39 3 42
RightIleocolectomy 32 2 34
RightIleocolectomywithEnterectomy 22 0 22
Leftcolectomy 5 0 5
Totalcolectomywithendileostomy 3 2 5
Totalproctocolectomywithendileostomy 3 0 3
Proctectomy 2 0 2
Enteroanastomosis 6 0 6
Ileostomy 4 4 8
Loopcolostomy 0 2 2
Colorraphy 4 0 4
Exploratorylaparotomy 0 11 11
Urologicalprocedures 3 3 6
Reconstructionoftheabdominalwall 0 3 3
Peritoniostomy 0 3 3
Incisionalherniorraphy 1 0 1
Oophorectomy 1 0 1
Total 126 32 158
Table4–Mortalityrateinrelationtothenumberofpatientsandoperationsperformedinthedifferentgroups.
Patients Operations Deaths Mortality(%)
Patients Operations
General 157 281 9 5.7 3.2
Crohn’s(abdominalsubgroup) 90 127 6 6.6 4.7
Crohn’s(perinealsubgroup) 64 115 0 0 0
UC 24 43 3 12.5 6.9
toanemergencysurgery.Thethreecaseshadasanindication oftheprocedureatoxicmegacolon,andinonecasecolonic perforationwaspresent.
BetweenCD-relateddeaths,thedisease waslocalizedto thesmallintestineintwocases(oneofwhichhadan asso-ciated perineal disease); two other patients suffered from colonicandperinealdisease;inoneofthecases,thedisease waslocatedinthesmallbowel,colon,andperineum;andin thelattercaseonlyanileocolicdiseasewasdiagnosed.Only onepatientwasnotoperatedonanemergencybasis.Onlytwo patientswerenotinuseofpreoperativecorticosteroids.
Onepatienthad beentreatedwithintravenous corticos-teroidtherapy and underwent aperianal abscessdrainage procedure under diagnostic suspicionof CD onlyfivedays beforea totalcolectomy with emergency ileostomydue to colonic perforation and a low digestive hemorrhage. Only one patient was in use of biological drugs before surgery: adalimumab,alreadyinlong-termuse,associatedwith aza-thioprineandoralcorticosteroidtherapy,alsoforalongtime. Inthispatient,theindicationforsurgerywasdueto multi-pleenterocutaneous(peri-ileostomic)fistulas,inanelective procedure.
Inallthedeathsabloodtransfusion wasindicated(one patientunderwenttransfusionreaction,withthesuspension ofthetransfusion),withthepresenceofmalnutritionatsome timeofthehospitalization.Inonlyonecasethepatientdid notreceivetotalparenteralnutrition.
Inallpatients,thecauseofdeathwassepsis,fourof pul-monaryorigin andtwocasesofcentralvenouscatheter, in
additiontooneofabdominalfocus,fungalsystemic, anda progressionofFournier’ssyndrome,respectively(Table5).
Discussion
Among patients with CD, intestinal surgery is required in about 70–80%ofcasesafter20 years ofillness.In patients withUC,colectomiesarerequiredinapproximately20–30% ofpatientsafter25yearsofdisease.1Frolkisetal.,ina
meta-analysisofpopulationstudies,haveidentifiedthat therisk ofsurgeryat1,5,and10yearsafterthediagnosisofCDand between1and10yearsafterthediagnosisofUChasdecreased significantlyoverthelastsixdecades.6
A Danish study observed increased mortality in cases ofUC in patientsolder than 50 years,duringthe first two yearsafterdiagnosis,andinpatientswithanextensive col-itis.Suchdeathsusuallyoccurintheperioperativeperiodin patientswithseveredisease.7Kaplanetal.assessedthe
post-colectomymortalityinpatientswithUC,andalsoidentified theoccurrenceofhighermortalityinpatientsover60yearsof age.8Inthepresentstudy,alldeathsrelatedtoUChadarecent
diagnosisofdisease(<2years)andsufferedfrompancolitis. OnlyoneofthedeathsrelatedtoUCoccurredamongpatients agedover60,but proportionatelythisincreaseinmortality wasalsoidentified.
j
coloproctol
(rio
j).
2
0
1
7;
3
7(2)
:116–122
Table5–Detailedanalysisofcasesofdeath.
Previoustreatments
Gender Age AZA MSZ CTC Anti-TNF-␣ Surgeries Malnutrition/ TPN
Anemia/ Transfusion
Surgeryperformed (initial)
Indication Emergency POHT (days)
Surgeries (n)
Causamortis
CD
1 M 38 Yes No No No Enterectomy Yes/Yes Yes/Yes Enterorraphiesand ileostomy
Enterocutaneous fistulas
Yes 11 4 Abdominalsepsis
2 M 31 Yes No Yes No No Yes/Yes Yes/No Debridement Fournier’sSd. Yes 0 6 Fournier’sSd.
3 F 77 Yes Yes No No No Yes/Yes Yes/Yes Rightileocolectomy andenterectomy
Enterocutaneous fistulas
Yes 4 2 Pulmonarysepsis
4 M 44 Yes No Yes No Right
ileocolectomy
Yes/Yes Yes/Yes Rightileocolectomy Intestinal occlusion
Yes 1 2 Pulmonarysepsis
5 M 18 No No Yes No Perianalabscess drainage
Yes/Yes Yes/Yes Totalcolectomywith endileostomy
Colon
perforation+LDH
Yes 0 6 Centralvenous cathetersepsis 6 F 20 Yes No Yes Yes(ADA) Two-stagetotal
colectomyand fistulotomy
Yes/Yes Yes/Yes Two-stageenterectomy andfistulotomy
Enterocutaneous fistulas
Yes 2 3 Centralvenous cathetersepsis
NSUC
7 F 18 Yes Yes Yes No No Yes/Yes Yes/Yes Totalcolectomywith endileostomy
Intractability– hemorrhage
Yes 17 1 Fungalsepsis
8 F 14 Yes Yes Yes Yes(IFX) No Yes/Yes Yes/Yes Totalcolectomywith endileostomy
Intractability– perforation
Yes 3 2 Pulmonarysepsis
9 M 76 No No Yes No No Yes/No Yes/Yes Totalcolectomywith
endileostomy
Intractability– toxicmegacolon
Yes 1 1 Pulmonarysepsis
jcoloproctol(rioj).2017;37(2):116–122
121
colectomywithendileostomyandtheclosure oftherectal stump,respectively).8Inthepresentstudy,weidentifiedinthe
UCgroupageneralmortalityof12.5%,butthatreached30% inthosepatientssubmittedtothissameprocedurealsoonan emergencybasis.Still,accordingtothesameauthors,ahigher mortalityratewasalsoobservedinpatientsoperatedafter6 daysofhospitaladmission.8Thesedatawerealsoregistered
inanotherCanadianstudy,wheretheauthorsnotedthatthe complicationrateandmortalitywerehigherinpatients sub-mittedtoemergencycolectomies,incaseswherethesurgery wasperformed14daysafterhospitalization(incomparison topatientswiththeirsurgeryperformedbetween3and14 days).9
Another factor to consider is the number of colec-tomies/year for UC treatment, considered as of small (<4 colectomies/year), medium (4–11) and large (>11 colec-tomies/year)volume.Mortalitywashigherinhospitalswith asmall volumeofsurgeries.8 Our study presentedasmall
volume(1.4)ofannualcolectomiesintheinitialstudyperiod (2004–2010),butthatreachedamediumvolume(4)initsfinal period(2011–2014). Therefore, the UC management experi-ence isdirectly linkedtocomplications and deathsinthis difficultpatientpopulation.
UndertakingacolectomyinisolationinpatientswithUC isnotausualtreatment.However,inthepresentstudy,this scenariooccurred ontwo occasions: ina caseofapatient alreadysubmittedtoaleftcolectomy,withatransversecolon stomaandclosureofrectalstumpinanemergencybasisdue tohemorrhage,andinanotherpatienttowhomthesurgical indicationwasduetoadysplasticlesionintherightcolon, withtherefusalofthepatienttoperformawidercolectomy.
InCD,thesurgicalmortalityreportedinsomeseriesranges from0.5%to5%,10,11anumbersimilartoour4.5%foundinthe
groupofCrohn’spatientsoperatedoninoursample. Duetoitspotentialimmunosuppressiveeffect,theuseof biologicaldrugshasalwaysbeenmuchquestionedregarding theincreaseofpostoperativecomplications,especiallythose oftheinfectioustype.Inthissense,severalpublicationsdealt withthetheme.Inameta-analysisandsystematicreview,a slightincreaseinpostoperativecomplicationsassociatedwith theirusewasobserved,particularlyinCDpatients.12Onthe
otherhand,anotherDanishstudyfoundthattheuseof inflix-imabinthe preoperativeperioddidnotincrease morbidity andmortalityrates,13whichwasalsoconfirmedintwoother
relevantprospectivestudies.14,15Inthepresentseries,only2
patientswhodiedhadbeenmedicatedwithbiologicalagents inthepreoperativeperiod(1inCDand1inUC),bothwiththe associateduseofcorticosteroids.
Corticosteroidtherapyhasalsobeenextensivelystudied. Despiteitsundeniablebeneficialeffectsinthetreatmentof IBDs,especiallyinthe acutephase,itspostoperative reper-cussionisnegative.TREAT15andENCORE16studiesidentified
apotentialriskforinfectiouspostoperativecomplicationsand deathsinassociationwithcorticosteroiduse. Anotherlarge Canadianstudyalsofoundthisassociation,withanincrease inpostoperativecomplicationsbutnotinmortality.17Inthis
series,weidentifiedthisriskfactorinallUC-relateddeaths andin2/3ofCD-relateddeaths.
Anemiawasalsoanimportantfactoridentifiedincases ofdeath.AllpatientshadlevelsofHb<8g/dLatsometime
duringhospitalization.AKoreanstudycitesahematocrit(HT) <30%asariskfactorforearlypostoperativecomplications.18
Inaretrospectivestudyonpost-bowelresectionmorbidityin CDcases,Brueweretal.foundthatpatientswithHb<10g/dL showed a significant association with postoperative septic complications,comparedwithpatientswithHb>10g/dL,in aproportionof20%versus6%,respectively(p<0.05).19
Anotherdeterminantriskfactorforpostoperative morbid-ity andmortalityisthe nutritionalstatusofthe patient.In a series comparing anastomosis withmanual or mechani-calsuture,Smedhetal.observedthatthecomplicationrates were lower inthegrouppreviouslytreatedwithan enteral diet before the procedures.20 In addition, a Korean study
foundthatserumalbuminlevelsbelow3g/dLarepredictorsof increasesincomplicationsandthatitspreoperativecorrection decreasesmorbidityrates.18Yamamotoetal.alsoidentified
hypoalbuminemia(<3g/dL)asariskfactorforpostoperative abdominalsepticcomplicationsincasesofCD.11Thisrisk
fac-torwasdetectedevenmoreseverely(albumin<2mg/dL)inall deathsstudiedinthisseries.
Ourstudypresentssignificantlimitations,whichmustbe takenintoaccountintheanalysisoftheresults.Firstly,thisisa seriesofretrospective,descriptivecases,withoutcomparison amonggroupsandwithoutstatisticalanalysis,andwhichhad thesimpleobjectiveofservingasanalertfortheseriousness ofthesurgicaltreatmentofIBDinourcountry.Inaddition,the highnumberofmortalitycasesdemonstratestheclearbiasof areferralcenterinthemanagementofthesediseases,which receivesevere,oftenlate,cases–whichincreases complica-tions.Despiteitslimitations,itshouldbenotedthatthisis thefirstdescriptiveanalysisonmortalityinIBDcasesinour country.
Insummary,theoverallmortalityratefoundinthepresent studywas5.7%ofthepatients.Thepresenceofseveralrisk factors acting simultaneously and in a complex way con-tributedtothepostoperativemortalityincasesofIBDinthe groupofdeathsevaluatedhere.Amongthemainriskfactors found,thereistheemergencyandurgencyregimen,multiple operations,malnutrition,anemia,andpreviouscorticosteroid therapy.Studieswithagreaternumberofpatientsareneeded, inorder toobtainadeeper understandingofpostoperative mortalityinthemanagementofIBDsinourscenario.
Conflicts
of
interest
PGK:Abbvie,Ferring,Janssen,Pfizer,andTakeda;EFM:Abbvie andJanssen.Theotherauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.CosnesJ,Gower-RousseauC,SeksikP,CortotA.Epidemiology andnaturalhistoryofinflammatoryboweldiseases. Gastroenterology.2011;140:1785–94.
2.SonnenbergA.TimetrendsofmortalityfromCrohn’sdisease andulcerativecolitis.IntJEpidemiol.2007;36:890–9.
3.CanavanC,AbramsKR,MayberryJF.Meta-analysis:mortality inCrohn’sdisease.AlimentPharmacolTher.2007;25:861–70.
5. vanOverstraetenAB,WolthuisA,D’hooreA.Surgeryfor Crohn’sdiseaseintheeraofbiologicals:areducedneedor delayedverdict?WorldJGastroenterol.2012;18:3828–32.
6. FrolkisAD,DykemanJ,NegrónME,DebruynJ,JetteN,Fiest KM,etal.Riskofsurgeryforinflammatoryboweldiseaseshas decreasedovertime:asystematicreviewandmeta-analysis ofpopulation-basedstudies.Gastroenterology.
2013;145:996–1006.
7. WintherKV,JessT,LangholzE,MunkholmP,BinderV. Survivalandcause-specificmortalityinulcerativecolitis: follow-upofapopulation-basedcohortinCopenhagen County.Gastroenterology.2003;125:1576–82.
8. KaplanGG,MccarthyEP,AyanianJZ,KorzenikJ,HodinR, SandsnBE.Impactofhospitalvolumeonpostoperative morbidityandmortalityfollowingacolectomyforulcerative colitis.Gastroenterology.2008;134:680–7.
9. SilvaS,MaC,ProulxMC,CrespinM,KaplanBS,HubbardJ, etal.Postoperativecomplicationsandmortalityfollowing colectomyforulcerativecolitis.ClinGastroenterolHepatol. 2011;9:972–80.
10.PostS,BetzlerM,vonDitfurthB,SchurmannG,KuppersP, HerfarthC.RisksofintestinalanastomosesinCrohn’s disease.AnnSurg.1991;1:37–42.
11.YamamotoT,AllanRN,KeighleyMR.Riskfactorsfor intra-abdominalsepsisaftersurgeryinCrohn’sdisease.Dis ColonRectum.2000;43:1141–5.
12.YangZP,HongL,WuQ,WuKC,FanDM.Preoperative infliximabuseandpostoperativecomplicationsinCrohn’s disease:asystematicreviewandmeta-analysis.IntJSurg. 2014;12:224–30.
13.BregnbakD,MortensenC,BendtsenF.Infliximaband complicationsaftercolectomyinpatientswithulcerative colitis.JCrohn’sColitis.2012;6:281–6.
14.LichtensteinGR,FeaganBG,CohenRD,SalzbergBA,Diamond RH,ChenDM,etal.Seriousinfectionsandmortalityin associationwiththerapiesforCrohn’sdisease:TREAT registry.ClinGastroenterolHepatol.2006;4:621–30.
15.LichtensteinGR,FeaganBG,CohenRD,SalzbergBA,Diamond RH,PriceS,etal.Seriousinfectionandmortalityinpatients withCrohn’sdisease:morethan5yearsoffollow-upinthe TREATTMregistry.AmJGastroenterol.2012;107:1409–22.
16.D’HaensG,ColombelJF,HommesDW,PanesJ,RutgeertsPJ, EkbomA,etal.Corticosteroidsposeanincreasedriskfor seriousinfection:aninterimsafetyanalysisoftheENCORE Registry.Gastroenterology.2008:134–40.
17.NguyenGC,ElnahasA,JacksonTD.Theimpactof
preoperativesteroiduseonshort-termoutcomesfollowing surgeryforinflammatoryboweldisease.JCrohn’sColitis. 2014;8:1661–7.
18.YangSS,YuCS,YoonYS,YoonSN,LimSB,KimJC.Riskfactors forcomplicationsafterbowelsurgeryinKoreanpatientswith Crohn’sdisease.JKoreanSurgSoc.2012;83:141–8.
19.BruewerM,UtechM,RijckenEJ,AnthoniC,LaukoetterMG, KerstingS,etal.Preoperativesteroidadministration:effect onmorbidityamongpatientsundergoingintestinalbowel resectionforCrohnsdisease.WorldJSurg.2003;27:1306–10.