w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Interventional
rheumatology:
the
competence
of
Brazilian
rheumatologists
Aline
Teixeira
de
Landa,
Jamil
Natour,
Rita
Nely
Vilar
Furtado
∗UniversidadeFederaldeSãoPaulo,EscolaPaulistadeMedicina,DisciplinadeReumatologia,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24August2016 Accepted11April2017 Availableonline19June2017
Keywords: Jointinjection Competence Rheumatologist Training
a
b
s
t
r
a
c
t
Objectives: DescribeBrazilianrheumatologists’scompetenceininterventional rheumato-logy;assesstheassociationbetweenthisabilityanddemographicandtrainingvariables. Methods:A cross-sectional study with 500 Brazilian rheumatologists. Participantswere assessedbyself-administeredquestionnaireconsistingofdemographics,training,practice inofficeandknowledgeininterventionalrheumatologydata.
Results:463participantshadtheirdataanalyzed.Themeanagewas40.2years(±11.2).70% hadperformedperiarticularinjectionsand78%hadperformedintra-articularinjections. Thesamplewasdividedintothreegroups:non-interventionist,littleinterventionistand veryinterventionist.Thenon-interventionistgroupshowed(p<0.001–0.04)highermeanage, lowerproportionofuniversitybond,lowertraininghistory,higherproportionofgraduates intheSoutheastcountry,andhigherproportionofgraduatesinthe1980sto1989.Thevery interventionistgroupshowedhigher(p<0.001–0.018)proportionofadultrheumatologists, higherproportionofuniversitybond,longertrainingtimewithgreaterpracticeof com-plexprocedures,andhigherproportionofgraduates,trainedandwithprivatepracticein theSouthcountry.Variablesmostassociatedwiththeveryinterventionistsubgroupare per-formingaxialintra-articularinjections(OR:7.4,p<0.001),synovialbiopsy(OR:5.75,p=0.043), image-guidedIAI(OR:4.16,p<0.001),viscosupplementation(OR=3.41,p<0.001),jointlavage (OR=3.22,p=0.019),salivaryglandbiopsy(OR=2.16,p=0.034)andover6-monthtraining (OR:2.16,p=0.008).
Conclusions: Performingmorecomplexinvasiveproceduresandover6-monthtrainingin interventionalrheumatologywerevariablesassociatedwithenhancedinterventional pro-file.
©2017PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](R.N.Furtado).
http://dx.doi.org/10.1016/j.rbre.2017.05.002
Reumatologia
intervencionista:
competência
dos
reumatologistas
brasileiros
Palavras-chave: Injec¸ãoarticular Competência Reumatologista Treinamento
r
e
s
u
m
o
Objetivos: Descreveracompetênciadosreumatologistasbrasileirosnareumatologia inter-vencionista(RI);avaliaraassociac¸ãoentreessacapacidadeevariáveisdemográficasede treinamento.
Métodos:Fez-seumestudotransversalcom500reumatologistasbrasileiros.Osparticipantes foramavaliadosporquestionárioautoadministrado,constituídopordadosdemográficos, treinamento,práticaemconsultórioeconhecimentoemdadosdeRI.
Resultados: Analisaram-seosdadosde463participantes.Amédiafoide40,2anos(±11,2). Desses,70%fizeraminjec¸õesperiarticulares(IPA)e78%intra-articulares(IAI).Aamostra foidivididaemtrêsgrupos:nãointervencionista,poucointervencionistaemuito interven-cionista.Ogruponãointervencionistaapresentou(p<0,001-0,04)maiormédiadeidade, menorproporc¸ãodevínculouniversitário,menorhistóriadetreinamento,maiorproporc¸ão degraduadosnaRegiãoSudestedopaísemaiorproporc¸ãodegraduadosnasdécadasde 1980a1989.Ogrupomuitointervencionistaapresentou(p<0,001-0,018)maiorproporc¸ão dereumatologiasqueatendempacientesadultos,maiorproporc¸ãodevínculouniversitário, maiortempodetreinamentodepráticadeprocedimentoscomplexos,maiorproporc¸ãode graduadosnosuldopaís,treinadosecomconsultórioparticularnessaregião.Asvariáveis maisfrequentementeassociadasaosubgrupomuitointervencionistaforamfeituradeIAI axial(OR:7,4,p<0,001),biópsiasinovial(OR:5,75,p=0,043),IAIguiadaporimagem(OR: 4,16,p<0,001),viscossuplementac¸ão(OR=3,41,p<0,001),lavagemarticular(OR=3,22,p= 0,019),biópsiadaglândulasalivar(OR=2,16,p=0,034)emaisdeseismesesdetreinamento (OR:2,16;p=0,008).
Conclusões: Fazerprocedimentosinvasivosmaiscomplexosetermaisdeseismesesde treinamentoemRIforamasvariáveisassociadasaummelhorperfilintervencionista.
©2017PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatologyisconsideredonlyaclinicalspecialtybymany. But in fact, the practice involves a series of interventions thatassistthe physicianinthe diagnosisand treatmentof rheumatic diseases.Interventional rheumatology has been partoftheexpertiseforoverhalfacentury,whenthepractice of intra-articular injection (IIA) with corticosteroids (CSs) began.1Thisremainsthemostcommonprocedureperformed
by rheumatologists nowadays. The periarticular injections (PIs) withCSs canbe usedforthe treatmentof inflamma-torysofttissueasthefirstchoiceoreveninrefractorycases. Theuseofimagetechniquescanimprovetheeffectivenessof jointinjection,bothintra-andperiarticular.Otherprocedures relatedtopatientdiagnosisincludesynovial,bone,muscle, andsalivaryglandbiopsies.2–5
Therearefewstudiesevaluatingtheintervention’s com-petence ofrheumatologists throughoutthe world.6–8 Some
studies focus on rheumatologist’s competence to perform musculoskeletalultrasound(MU)fordiagnosticpurposesor forguidingprocedures.9–13
Therearenopublishedstudiesevaluatingthetheoretical competenceininterventionalrheumatologyamongBrazilian rheumatologists. Itisbelieved thatthere isalarge hetero-geneity intraining toperform osteoarticular procedures in Brazil.
Theaimsofthis studyweretodescribethecompetence ofBrazilianrheumatologistsininterventionalrheumatology, assesstheassociationbetweentheircompetenceand demo-graphic variables, and between their educational training in order to try to identify variables associated with more interventionalrheumatologists.
Methods
Thiswasacross-sectionalstudyreviewedandapprovedby the Ethics Committee of the Universidade Federal de São Paulo, São Paulo,Brazil.Five hundred Brazilian rheumatol-ogists were randomly selected and assigned toparticipate in the study. Participants were selected during the most importantannualRheumatologymeetingofthe Rheumato-logy BrazilianSocietyconductedinthe southeastregionof Brazil.
Assessment
Participantswereassessedthroughself-administered ques-tionnaire.Thequestionnaireconsistedoftwoparts:thefirst related to the demographic characteristics and training in interventionalrheumatologyand the second relatedtothe competenceininterventionalrheumatology.
Thefirstpartofthequestionnaireconsistedofthe follow-ingitems:age; venueand yearofgraduation;institutionof residency/specializationinrheumatology;titleofspecialistin rheumatology,mastersorPhDdegrees;universitybondand privatepractice.
The second part of the questionnaire comprised the following items related to practice in interventional rheu-matology: training in invasive procedures during medical residency/specialization; practice in invasive procedures; practiceinPIandinjectedstructures;practicein appendic-ularIAI,injectedjointsandindicationfortheprocedure;axial IAIpracticeandinjectedjoints;CSusedinPIandreasonfor choice;CSusedinIAIand reasonforchoice; practiceinPI andIAIimage-guidedinjectionsandimagetechniqueusedto guidetheprocedure;practiceinviscosupplementation,joint lavage,epiduralinjectionwithCSandsynovial,salivarygland, boneandmusclebiopsies.
The questions that addressed the joints injected (PI or appendicular IAI)wereanalyzednot onlydescriptively, but alsocategorizedaseasyordifficulttoperformaccordingtothe opinionoftwo(2)rheumatologistswithextensiveexperience ininterventionalrheumatologyasfollows:
PI:Easytoperform:subacromial,lateralepicondyle,medial epicondyle,trochantericbursa,ischialbursa,anserinebursa andplantarfascia;Difficulttoperform:peritendonofshort extensor/longabductorofthethumb(deQuervain tendini-tis), carpal tunnel, peritendon of flexor tendon of finger (stenosing tendonitis or trigger tendonitis), Baker cyst, perienthesites/bursitis ofthe Achilles tendon, in synovial sheathoftheperonealtendonsandtheposteriortibial ten-don.
IAI:Easytoperform:knee;wrist;ankleand metacarpopha-langeal;Difficulttoperform:temporomandibular; acromio-clavicular;glenohumeral;radiohumeral;1st metacarpopha-langeal, proximal interphalangeal and distal interpha-langeal;hip;subtalar;intertarsalandmetatarsophalangeal.
Participantswereinitiallydividedintotwogroups: “non-interventionalgroup”,formedbyRheumatologistswhodonot performanyprocedure, and“interventionalgroup”,formed byRheumatologistswhodidatleastonetypeofprocedure. Later, they were then divided into two groups: (1) “many interventionsgroup”whodidatleast50%ofPIsconsidered easy,20%ofPIsconsidereddifficult,50%ofIAIsconsidered easyand20%ofIAIsconsidereddifficult;(2)“few interven-tionsgroup”whodidsomeinvasiveprocedures,butdidnot reach the pre-set limit to compose the first subgroup, as well as rheumatologists who did not perform any type of procedure.
RegardingthequestiononthemosteffectiveCSfor intra-articularuse,accordingtoscientificevidence,thebestoption wasconsideredtriamcinolonehexacetonide.14
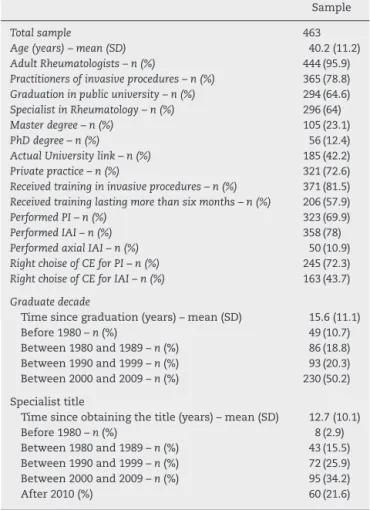
Table1–Demographiccharacteristicsofthesample.
Sample
Totalsample 463
Age(years)–mean(SD) 40.2(11.2)
AdultRheumatologists–n(%) 444(95.9)
Practitionersofinvasiveprocedures–n(%) 365(78.8)
Graduationinpublicuniversity–n(%) 294(64.6)
SpecialistinRheumatology–n(%) 296(64)
Masterdegree–n(%) 105(23.1)
PhDdegree–n(%) 56(12.4)
ActualUniversitylink–n(%) 185(42.2)
Privatepractice–n(%) 321(72.6)
Receivedtrainingininvasiveprocedures–n(%) 371(81.5)
Receivedtraininglastingmorethansixmonths–n(%) 206(57.9)
PerformedPI–n(%) 323(69.9)
PerformedIAI–n(%) 358(78)
PerformedaxialIAI–n(%) 50(10.9)
RightchoiseofCEforPI–n(%) 245(72.3)
RightchoiseofCEforIAI–n(%) 163(43.7)
Graduatedecade
Timesincegraduation(years)–mean(SD) 15.6(11.1) Before1980–n(%) 49(10.7) Between1980and1989–n(%) 86(18.8) Between1990and1999–n(%) 93(20.3) Between2000and2009–n(%) 230(50.2) Specialisttitle
Timesinceobtainingthetitle(years)–mean(SD) 12.7(10.1) Before1980–n(%) 8(2.9) Between1980and1989–n(%) 43(15.5) Between1990and1999–n(%) 72(25.9) Between2000and2009–n(%) 95(34.2) After2010(%) 60(21.6) SD,standarddeviation;PI,periarticularinjection;IAI,intra-articular injection.
Regarding more complex procedures in interventional rheumatology(guidedprocedures,biopsies,jointlavageand epiduralinjectionwithCS),Rheumatologistshadtodescribe theircompetencetoperformit,andwheretheyobtained tech-nicaltraining.
Statisticalanalysis
Descriptive analysis (mean, standard deviation [SD], fre-quencyandpercentage)wasusedforthecharacterizationof thesample.
AfterthecompetencedescriptionofBrazilian rheumatol-ogistsininterventionalrheumatology,thefollowinganalyzes wereperformed:assessmentoftheassociationbetween com-petenceanddemographicvariablesandtrainingvariablesand comparing the“non-interventional”/“interventional”groups and“manyinterventions”/“fewinterventions”groups. More-over, an analysis was carried out to identify predictor factorsofparticipantsbelongingtothe“manyinterventions” group.
7.8
53.4
0 10 20 30 40 50 60 70 80 90 100
51.8 36.6
48.2
67.6 47.4
38 44.6 13.6
99.4 58.4
18.8 14.1
27.7
87.6 84.4 78.7 77.7 70.4 66.9 66.6 63.4 53.8 43.9 39.8 28.3 24.5 23.9
Temporomandibular Trapeziometacarpal Proximal interphalangeal Distal interphalangeal Metacarpophalangeal Wrist Elbow Acromioclavicular Glenohumeral Hip Knee Ankle Subtalar Midfoot Metatarsophalangeal Lateral epicondylitis Trochanteric bursitis Medial epicondylitis Trigger finger Subacromial tendinitis Anserine bursitis Carpal tunnel syndrome De quervain tendinitis Plantar fasciitis Baker cyst Calcaneus tendinitis Ischiatic bursitis Posterior tibial tendinitis Fibular tendinitis
PI IAI
Fig.1–Percentageofparticipantswhoperformperiarticularinjection(PI)andintra-articularinjection(IAI)perjointor structure.
Themultivariatelogisticregressionusingbackward con-ditionalmethodwasalsoperformedtoidentifyfactorsthat couldpredicttheparticipant’sprobabilityofbelongingtothe “manyinterventions”group.
TheSPSSsoftwareversion17.0(Chicago,IL)wasusedand thelevelofstatisticalsignificancewas5%.
Results
Fourhundredeighty-sevenquestionnaireswerecompleted,of which463mettheinclusioncriteria.Twenty-fourparticipants wereexcludedbecausetheywerenotrheumatologists.
Thedemographiccharacteristicsofthesampleareshown inTable1.Majorityofparticipants(81.5%)declaredtohave receivedtrainingininterventionalrheumatologyduring resi-dency/specialization.Approximately70%performedPI,while 78%performedIAI.ThesoutheastregionofBrazilwastheone thatobtainedthehighestnumberofparticipantsinthestudy –graduated(58.3%),trainedinrheumatology(77.2%),holding master’s(74.8%)orPhD(78.8%)degreesandcurrentlyworking inprivatepractice(62.8%).
Fig. 1shows the frequencyof PIsand IAIs. Lateral epi-condylitis,trochantericbursitisandmedialepicondylitiswere the periarticular diseases most injected. The appendicular
jointsmostinjectedweretheknee,wristandankle.The indi-cationsforIAIwerethepresenceofsynovitis(91.2%),followed byjointswelling(64.9%)andjointpain(27.3%).Jointinstability wasidentifiedasanindicationforIAIinonly1.7%of partici-pants.Fifty(10.9%)participantsperformedaxialIAI.Theaxial jointmostinjectedwasthesternoclavicular,beinginjectedby 76.6%ofparticipants.
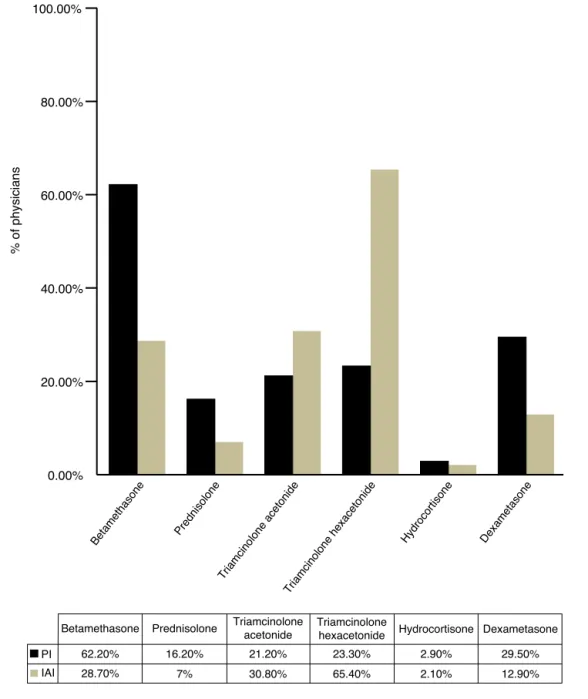
Fig.2showstheCSscommonlyusedinIAIsandPIs.For bothtypesofinjections(IAIsandPIs),thepresenceof scien-tificevidencehasbeenthemainreasonforchoosingtheCS, beingindicatedby53.8%oftheparticipantstoPIand67.5% forIAI.Mostrheumatologists(67.3%)indicatedcorrectlythat triamcinolonehexacetonidewasasthemosteffectiveCSfor IAIs.
GuidedIAIswereperformedbyonly14%ofparticipants, withtheankle(75.8%),hip(54.8%)andglenohumeral(53.2%) beingthemostguidedinjectedjoints.Themostwidelyused methodtoguidetheIAIwasultrasonography,whichwasused by88.7%.
Regarding the practice of viscosupplementation, it was observedthat38.2%ofrheumatologistsreportedhavingdone thisprocedureintheirmedicalpractice.Themostsubmitted jointtoviscosupplementationwastheknee(100%ofcases).
0.00% 20.00%
% of physicians
40.00% 60.00% 80.00% 100.00%
Betamethasone Prednisolone
Triamcinolone acetonide
Triamcinolone hexacetonide
Hydrocortisone Dexametaso ne
Betamethasone
62.20% PI
IAI
16.20% 21.20% 23.30% 2.90% 29.50%
28.70% 7% 30.80% 65.40% 2.10% 12.90%
Prednisolone Triamcinolone
acetonide
Triamcinolone
hexacetonide Hydrocortisone Dexametasone
Fig.2–Corticosteroidchoiceforperiarticularinjections(PI)andintra-articularinjection(IAI).
invasiveprocedures,residencywasthevenuewheremost par-ticipantsreceivedacademictraining.
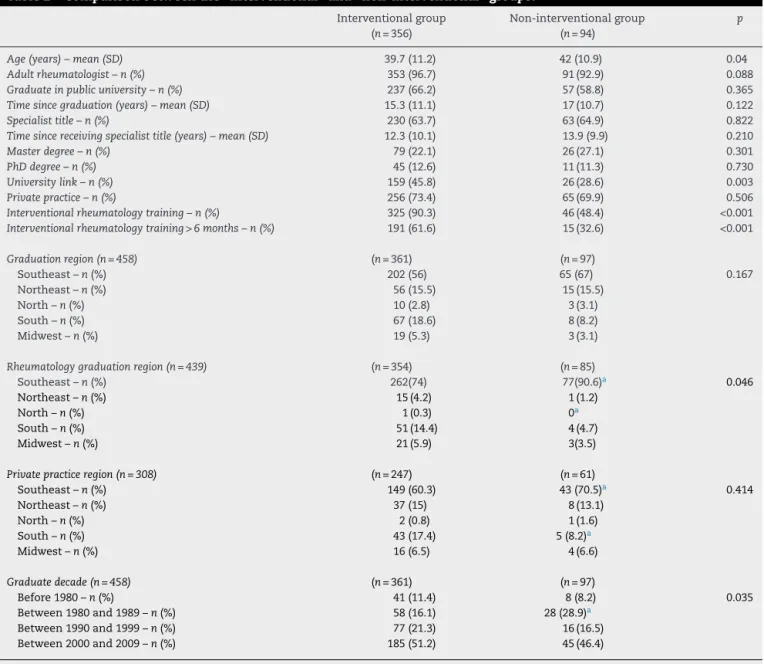
Table2shows thecomparisonofdemographicdataand academic training between the “non-interventional” and “interventional”groups.Itwasobservedthattheaverageage of the “non-interventional” group was significantly higher thanthe“interventional”group.Inthe“interventional”group, therewasahigherproportionofrheumatologistsconnected withuniversityandtrained ininterventionalrheumatology formorethansixmonthsduringresidency/medical special-ization.The “non-interventional” group had a significantly higher proportion of individuals with training in rheuma-tology in the southeastern region of Brazil and graduated between 1980 and 1989. The “interventional” group had rheumatologistswithahigherproportionoftrainingin rheu-matologyinthesouthernregionofBrazil.
Table2–Comparisonbetweenthe“interventional”and“non-interventional”groups.
Interventionalgroup (n=356)
Non-interventionalgroup (n=94)
p
Age(years)–mean(SD) 39.7(11.2) 42(10.9) 0.04
Adultrheumatologist–n(%) 353(96.7) 91(92.9) 0.088
Graduateinpublicuniversity–n(%) 237(66.2) 57(58.8) 0.365
Timesincegraduation(years)–mean(SD) 15.3(11.1) 17(10.7) 0.122
Specialisttitle–n(%) 230(63.7) 63(64.9) 0.822
Timesincereceivingspecialisttitle(years)–mean(SD) 12.3(10.1) 13.9(9.9) 0.210
Masterdegree–n(%) 79(22.1) 26(27.1) 0.301
PhDdegree–n(%) 45(12.6) 11(11.3) 0.730
Universitylink–n(%) 159(45.8) 26(28.6) 0.003
Privatepractice–n(%) 256(73.4) 65(69.9) 0.506
Interventionalrheumatologytraining–n(%) 325(90.3) 46(48.4) <0.001
Interventionalrheumatologytraining>6months–n(%) 191(61.6) 15(32.6) <0.001
Graduationregion(n=458) (n=361) (n=97)
Southeast–n(%) 202(56) 65(67) 0.167 Northeast–n(%) 56(15.5) 15(15.5)
North–n(%) 10(2.8) 3(3.1) South–n(%) 67(18.6) 8(8.2) Midwest–n(%) 19(5.3) 3(3.1)
Rheumatologygraduationregion(n=439) (n=354) (n=85)
Southeast–n(%) 262(74) 77(90.6)a 0.046
Northeast–n(%) 15(4.2) 1(1.2)
North–n(%) 1(0.3) 0a
South–n(%) 51(14.4) 4(4.7)
Midwest–n(%) 21(5.9) 3(3.5)
Privatepracticeregion(n=308) (n=247) (n=61)
Southeast–n(%) 149(60.3) 43(70.5)a 0.414
Northeast–n(%) 37(15) 8(13.1)
North–n(%) 2(0.8) 1(1.6)
South–n(%) 43(17.4) 5(8.2)a
Midwest–n(%) 16(6.5) 4(6.6)
Graduatedecade(n=458) (n=361) (n=97)
Before1980–n(%) 41(11.4) 8(8.2) 0.035
Between1980and1989–n(%) 58(16.1) 28(28.9)a
Between1990and1999–n(%) 77(21.3) 16(16.5)
Between2000and2009–n(%) 185(51.2) 45(46.4)
SD,standarddeviation.
Mann–Whitneytestwasusedforcategoricaldata;chi-squaretestwasusedfornumericaldata.
a Statisticaldifferencewhencomparedto“interventional”group.
withamedicaldegreeandrheumatologytraininginthe south-ernregionofBrazil.
Using the backward conditional method, a multivariate logisticregression was performedto identifyand calculate theoddsratio(OR)ofvariablesthatweremostassociatedto the“manyinterventions”group.Thevariablesfoundwerethe following:practiceinaxial IAI, viscosupplementation,joint lavage,synovialbiopsy,salivaryglandbiopsy,IAIguidedby imageandtrainingininterventionalrheumatologyforlonger thansixmonths.
The most strongly associated variable was axial IAI practice, withan OR of7.4 (95%CI 2.7–20.1, p<0.001), fol-lowedbysynovialbiopsy(ORof5.7[95%CI,1.05–31.32]p<0.05) and image-guided injections (OR of4.1 [IC 95%, from 1.88 to 9.2] p<0.0010. The data for these and other variables
identified by multivariate logistic regression are shown in
Table4.
Discussion
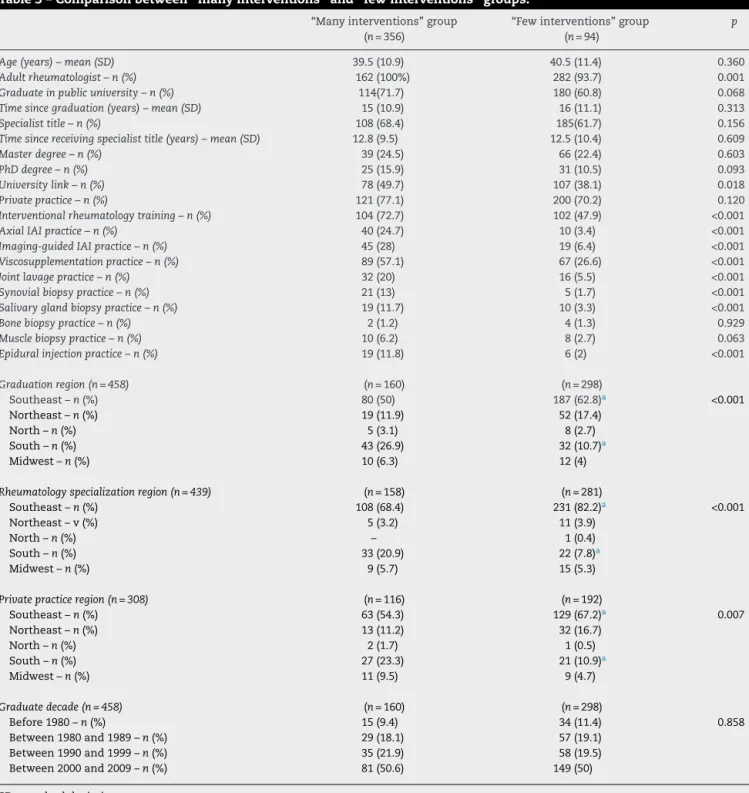
Table3–Comparisonbetween“manyinterventions”and“fewinterventions”groups.
“Manyinterventions”group (n=356)
“Fewinterventions”group (n=94)
p
Age(years)–mean(SD) 39.5(10.9) 40.5(11.4) 0.360
Adultrheumatologist–n(%) 162(100%) 282(93.7) 0.001
Graduateinpublicuniversity–n(%) 114(71.7) 180(60.8) 0.068
Timesincegraduation(years)–mean(SD) 15(10.9) 16(11.1) 0.313
Specialisttitle–n(%) 108(68.4) 185(61.7) 0.156
Timesincereceivingspecialisttitle(years)–mean(SD) 12.8(9.5) 12.5(10.4) 0.609
Masterdegree–n(%) 39(24.5) 66(22.4) 0.603
PhDdegree–n(%) 25(15.9) 31(10.5) 0.093
Universitylink–n(%) 78(49.7) 107(38.1) 0.018
Privatepractice–n(%) 121(77.1) 200(70.2) 0.120
Interventionalrheumatologytraining–n(%) 104(72.7) 102(47.9) <0.001
AxialIAIpractice–n(%) 40(24.7) 10(3.4) <0.001
Imaging-guidedIAIpractice–n(%) 45(28) 19(6.4) <0.001
Viscosupplementationpractice–n(%) 89(57.1) 67(26.6) <0.001
Jointlavagepractice–n(%) 32(20) 16(5.5) <0.001
Synovialbiopsypractice–n(%) 21(13) 5(1.7) <0.001
Salivaryglandbiopsypractice–n(%) 19(11.7) 10(3.3) <0.001
Bonebiopsypractice–n(%) 2(1.2) 4(1.3) 0.929
Musclebiopsypractice–n(%) 10(6.2) 8(2.7) 0.063
Epiduralinjectionpractice–n(%) 19(11.8) 6(2) <0.001
Graduationregion(n=458) (n=160) (n=298)
Southeast–n(%) 80(50) 187(62.8)a <0.001
Northeast–n(%) 19(11.9) 52(17.4)
North–n(%) 5(3.1) 8(2.7)
South–n(%) 43(26.9) 32(10.7)a
Midwest–n(%) 10(6.3) 12(4)
Rheumatologyspecializationregion(n=439) (n=158) (n=281)
Southeast–n(%) 108(68.4) 231(82.2)a <0.001
Northeast–v(%) 5(3.2) 11(3.9)
North–n(%) – 1(0.4)
South–n(%) 33(20.9) 22(7.8)a
Midwest–n(%) 9(5.7) 15(5.3)
Privatepracticeregion(n=308) (n=116) (n=192)
Southeast–n(%) 63(54.3) 129(67.2)a 0.007
Northeast–n(%) 13(11.2) 32(16.7)
North–n(%) 2(1.7) 1(0.5)
South–n(%) 27(23.3) 21(10.9)a
Midwest–n(%) 11(9.5) 9(4.7)
Graduatedecade(n=458) (n=160) (n=298)
Before1980–n(%) 15(9.4) 34(11.4) 0.858
Between1980and1989–n(%) 29(18.1) 57(19.1)
Between1990and1999–n(%) 35(21.9) 58(19.5)
Between2000and2009–n(%) 81(50.6) 149(50)
SD,standarddeviation.
Mann–Whitneytestwasusedforcategoricaldata;chi-squaretestwasusedfornumericaldata.
a Statisticaldifferencewhencomparedto“interventional”group.
AccordingtotheBrazilianMinistryofEducationand Cul-ture(MEC),arthrocentesis,IAIandPIareskillsthatmustbe acquiredthroughoutresidencyinrheumatology,aspartofthe officialprogramofthespecialtytraining.Proceduressuchas biopsies(bone,skin,minorsalivarygland,muscleand subcu-taneous),MU,nerveregionalblockingandepiduralinjection areconsideredoptional,evenifrecommended.15Despitethe
existenceofthistheoreticalprogram,itisknownthat hetero-geneityamongprogramsishuge.
Table4–Multivariatelogisticregressionforpredictionofbelongingtothe“manyinterventions”group.
p OR(95%CI)
AxialIAIpractice <0.001 7.422(2.740–20.105) Synovialbiopsypractice 0.043 5.758(1.059–31.321) Imaging-guidedIAIpractice <0.001 4.169(1.888–9.204) Salivaryglandbiopsypractice 0.034 3.445(1.098–10.810) Viscosupplementationpractice <0.001 3417(1.928–6.056) Jointlavagepractice 0.019 3221(1.213–8.550) Interventionalrheumatologytraining>6months–n(%) 0.008 2164(1.219–3.841) OR,oddsratio;CI,confidenceinterval.
StudiespublishedbyGormleyetal.(2003)andLiddelletal. (2005)addressedthepracticeofIAIandPIamongUnited King-domgeneral practitioners. Both studies reported shoulder, knee and lateral epicondylitis injectionsas the most com-monlyperfomed.Amongthefactors,those thatinfluenced theexpertiseinIAIandPIweremalegender,practiceinrural regionandformaltraininginthoseprocedures.7,8
Oursampleconsistedof463participantswithameanage of40.2 years and the vast majority (95.9%)was composed byrheumatologistsseeingonlyadultpatients.The percent-ageofappendicularIAIpractitioners(78%)washigherthanPI practitioners(69.9%),andamuchsmallerpercentagereported performingaxialIAI(10.9%).
AmongthePIs,themostinjectedwaslateralepicondyle (87.6%),inwhichwassimilartostudiesconductedbyGormley in 2003 and Liddell in 2005. Among the joints most com-monlyinjected, theknee stoodoutwith99.4%.Thisfactis probablyduetothewidevarietyofrheumaticand orthope-dicdiseasesthataffectthisjoint.Inaddition,itisthelargest jointofthelocomotorsystemanditisrelativelysuperficial, which favorsthe possibility of performingsafe procedures blindly.
AmongthemostcommonlyCSusedinPIs,themostused in this study was betamethasone (62.2%). However, it was observedthat23.3% ofparticipantsreportedusing triamci-nolonehexacetonideforthisprocedure,whichisapotentially dangerous practice for the patient due to its atrophying characteristic.14
Forthe IAI,themostusedCSwastriamcinolone hexac-etonide (65.4%),also considered the mosteffective(67.3%). Comparing these data with those found by Centeno and colleagues in 1994, we observed that among American rheumatologists,methylprednisolonewasthemostusedCS for knee IAI, while in Brazil the most used was triamci-nolonehexacetonide.6However,triamcinolonehexacetonide
wasconsideredtheeffectiveCSbybothAmericanand Brazil-ianrheumatologists.
Regarding the performanceof image-guidedjoint injec-tions, we found that 14% of participants in this study performed this procedure, especiallyin the ankle, hip and glenohumeraljoint.TheMUwas themostusedmethodto guidejointinjections.Weobservedthat11.9%oftheassessed rheumatologists used joint injections guided by MU. This resultissimilartotwostudiesshowingthatinmostEULAR countries(84.9%ofthecountries)lessthan10%of rheuma-tologistsperformedthisprocedure.11InJapan,10.8%didit.13
Countries such as of the United Kingdom and the United
Stateshaveahigherpercentageofrheumatologistspracticing MU,33%and21%,respectively.9,12
In oursample,few rheumatologistswere skilledforthe practiceofthemostinvasiveandcomplexprocedures(joint lavage;synovial,salivarygland,boneandmuscularbiopsies; andepiduralinjection).Theirtrainingoccurredin rheumato-logyresidency.
Whencomparedtothe“interventional”group,the “non-interventional” group had a lower proportion ofuniversity link and shorter training (less than six months) duration in interventional rheumatology.These findings once again corroboratethegreatimportanceofpropertrainingin inter-ventionrheumatology.Inthe“interventional”group,ahigher proportionofgraduatesinthesouthernregionofBrazilwas found. Interestingly,the Southeastregion ofBrazil showed thehighestproportionofparticipantsinthe“few interven-tions”group.Thiswasasurprisingfindingduetothehigher concentrationofrheumatologistsinthesoutheastBrazilian region.
Interestingly,instudiesconductedbyGormleyandLiddell, itwasalsofoundthatgeneralpractitionersworkinginareas withlowconcentrationofexperts,citedinthestudyasrural ormixedregion,weremorelikelytoperformlocomotor sys-tem injections.7,8 Wealsofoundthat the“no intervention”
grouphadahigherproportionofgraduatesinthedecadefrom 1980to1989comparedtothe“interventional”group.The lat-ter resultcaninferthat physiciansgraduated after1990or youngerphysiciansaremoreinterventional,currently. How-ever,therewasnosignificantdifferencebetweengroupsinthe numbersofyears(mean–DP)aftergraduation.
Regardingthecomparisonbetween“manyinterventions” and“fewinterventions”groups,itwasfoundthatthe“many interventions”grouphadahigherproportionofadult rheuma-tologists, university-related professionals and those with trainingtimeininterventionalrheumatologygreaterthan6 months.The“manyinterventions”groupalsohadahigher proportionofaxialIAIpractitioners,aswellasthose perform-ingimage-guidedinjections,viscosupplementationandmore complexinvasiveprocedures.Thesefindingsaremostlikely relatedtolongertraining,andalsorevealthemost interven-tionalprofileofthisgroup.
timeininterventionalrheumatologygreaterthan6months”, whichonceagainreaffirmstheneedforformalandadequate training, especially during the residency in interventional rheumatology, for greater employability of various types of diagnostic or therapeutic procedures, including those considered morecomplex inthe practice ofrheumatology. ThisfindingissimilartothoseofGormleyetal.(2003),who similarly found that physicians who have received formal trainingweremorelikelytocarryoutjointinjection.7
The absence of the variable “gender” between covered demographicscouldbeconsideredalimitationofthisstudy. Other limitations are the fact that the questionnaire was self-administered and would have enabled more easily to provideinappropriateinformation.Thestudypopulationwas recruitedataneventheldinthesoutheastregionofBrazil. Thismayhaveincreasedthepercentageofparticipantsinthis regionattheexpenseofothers.
The great practical applicability of this study is that it reaffirms the importance of systematic training in inter-ventional rheumatology for prolonged periods during the formative years of the rheumatologist, preferably during medicalresidency.
Conclusion
Inconclusion,thisstudyidentifiedthatthevariablesrelated toamoreinterventionalprofileamongBrazilian rheumatolo-gistswerethefollowing:workingwithadultspatientsandin university;didgraduationandhavingaprivateclinicinthe southernregionofBrazil;and,mainly,havinghad an inter-ventionalrheumatologytrainingtimelongerthansixmonths andinmorecomplexosteoarticularprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. HollanderJL,BrownEMJr,JessarRA,BrownCY.
Hydrocortisoneandcortisoneinjectedintoarthriticjoints; comparativeeffectsofanduseofhydrocortisoneasalocal antiarthriticagent.JAmMedAssoc.1951;147:1629–35.
2.VordenbaumenS,JoostenLA,FriemannJ,SchneiderM, OstendorfB.Utilityofsynovialbiopsy.ArthritisResTher. 2009;11:256.
3.RalstonSH.Bonedensitometryandbonebiopsy.BestPract ResClinRheumatol.2005;19:487–501.
4.HarrisBT,MohilaCA.Essentialmusclepathologyforthe rheumatologist.RheumDisClinNorthAm.2011;37:289–308, vii.
5.ChisholmDM,MasonDK.Labialsalivaryglandbiopsyin Sjögren’sdisease.JClinPathol.1968;21:656–60.
6.CentenoLM,MooreME.Preferredintraarticular
corticosteroidsandassociatedpractice:asurveyofmembers oftheAmericanCollegeofRheumatology.ArthritisCareRes. 1994;7:151–5.
7.GormleyGJ,CorriganM,SteeleWK,StevensonM,TaggartAJ. Jointandsofttissueinjectionsinthecommunity:
questionnairesurveyofgeneralpractitioners’experiences andattitudes.AnnRheumDis.2003;62:61–4.
8.LiddellWG,CarmichaelCR,McHughNJ.Jointandsofttissue injections:asurveyofgeneralpractitioners.Rheumatology (Oxford).2005;44:1043–6.
9.CunningtonJ,PlattP,RafteryG,KaneD.AttitudesofUnited Kingdomrheumatologiststomusculoskeletalultrasound practiceandtraining.AnnRheumDis.2007;66:1381–3.
10.DuftnerC,Schuller-WeidekammC,MandlP,NothnaglT, SchirmerM,KainbergerF,etal.Clinicalimplementationof musculoskeletalultrasoundinrheumatologyinAustria. RheumatolInt.2014;34:1111–5.
11.MandlP,NaredoE,ConaghanPG,D’AgostinoM-A,Wakefield RJ,BachtaA,etal.Practiceofultrasound-guided
arthrocentesisandjointinjection,includingtrainingand implementationinEurope:resultsofasurveyofexpertsand scientificsocieties.Rheumatology(Oxford).2012;51:184–90.
12.SamuelsJ,AbramsonSB,KaeleyGS.Theuseof
musculoskeletalultrasoundbyrheumatologistsintheUnited States.BullNYUHospJtDis.2010;68:292–8.
13.TakaseK,OhnoS,IdeguchiH,TakenoM,ShiraiA,Ishigatsubo Y.UseofmusculoskeletalultrasoundinJapan:asurveyof practicingrheumatologists.ModRheumatol.2010;20:376–80.
14.FurtadoR,NatourJ.Infiltrac¸õesnoaparelholocomotor.Porto Alegre:Artmed;2011.p.180.
15.GiorgiRDN,LaurindoIMM.Requisitosmínimosdoprograma deresidênciamédicaemreumatologia(R1eR2).SãoPaulo: Sociedadebrasileiradereumatologia;2010.Availablefrom: