www.jped.com.br
ORIGINAL
ARTICLE
Frequency
of
and
factors
associated
with
vascular
complications
after
pediatric
liver
transplantation
夽
,
夽夽
Mariana
Orlandini
a,
Flávia
Heinz
Feier
b,∗,
Brunna
Jaeger
a,
Carlos
Kieling
c,
Sandra
Gonc
¸alves
Vieira
c,
Maria
Lucia
Zanotelli
baUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
bPediatricLiverTransplantationGroup,HospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
cPediatricHepatologyandLiverTransplantation,HospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
Received11March2013;accepted19August2013
Availableonline24December2013
KEYWORDS Thrombosis; Hepaticartery; Portalvein; Morbidity; Mortality
Abstract
Objective: toevaluatethefrequencyandfactorsassociatedwithvascularcomplicationsafter pediatriclivertransplantation.
Method: riskfactorswereevaluatedin99patientsunder18 yearsofagewithchronicliver diseasewhounderwentdeceaseddonorlivertransplantation(DDLT)betweenMarchof1995and Novemberof2009attheHospitaldeClínicasdePortoAlegre,Brazil.Thevariablesanalyzed includeddonorandrecipientage,gender,andweight;indicationfor transplant;PELD/MELD scores;technicalaspects;postoperativevascularcomplications;andsurvival.
Results: vascularcomplicationsoccurredin19patients(19%).Arterialeventsweremost com-mon,occurredearlierinthepostoperativeperiod,andwereassociatedwithhighgraftlossand mortalityrates.Inthemultivariateanalysis,thefollowingfactorswereidentified:portalvein diameter≤3mm,donor-to-recipientbodyweightratio(DRWR),prolongedischemictime,and
useofarterialgrafts.
Conclusion: thechoiceoftreatmentdependsonthetimingofdiagnosis;however,inthisstudy, surgicalrevisionorcorrectionproducedworseoutcomesthanpercutaneousangioplasty.The reductionofriskfactorsandearlydetectionofvascularcomplicationsarekeyelementstoa successfultransplantation.
©2013SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:OrlandiniM,FeierFH,JaegerB,KielingC,VieiraSG,ZanotelliML.Frequencyofandfactorsassociatedwith
vascularcomplicationsafterpediatriclivertransplantation.JPediatr(RioJ).2014;90:169---75.
夽夽StudyconductedatthePediatricLiverTransplantationGroup,HospitaldeClínicasdePortoAlegre,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.H.Feier).
PALAVRAS-CHAVE Trombose;
Artériahepática; Veiaporta; Morbidez; Mortalidade
Frequênciaefatoresrelacionadosacomplicac¸õesvascularesapóstransplante hepáticopediátrico
Resumo
Objetivo: Avaliarafrequênciaeosfatoresassociadosacomplicac¸õesvascularesapós trans-plantehepáticopediátrico.
Método: Osfatoresderiscoforamavaliadosem99pacientescommaisde18anosdeidadecom doenc¸ahepáticacrônicasubmetidosatransplantehepáticocadavérico(THC)entremarc¸ode 1995enovembrode2009noHospitaldeClínicasdePortoAlegre,Brasil.Asvariáveisanalisadas incluíram:idade,sexo epesodos doadoresereceptores;indicac¸ão detransplante;escores PELD/MELD;aspectostécnicos;complicac¸õesvascularespós-operatórias;esobrevida. Resultados: Ocorreramcomplicac¸õesvascularesem19pacientes(19%).Oseventosarteriais forammaiscomuns,tendoocorridoprecocementenopós-operatório,eforamassociadosaaltas taxasdeperdadoenxertoemortalidade.Emumaanálisemultivariada,foramidentificados osseguintesfatores:diâmetrodaveiaporta≤3mm,proporc¸ãodepesododoador/receptor
(DRWR),tempodeisquemiaprolongadoeusodeenxertosarteriais.
Conclusão: Aescolhadotratamentodependedomomentododiagnóstico;contudo,nessasérie, acirurgiaderevisão,oucorrec¸ãocirúrgica,produziuresultadospioresqueaangioplastia per-cutânea.Areduc¸ãodosfatoresderiscoeadetecc¸ãoprecocedecomplicac¸õesvascularessão fundamentaisparaumtransplantebem-sucedido.
©2013SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Livertransplantation is an accepted treatment option for childrenwithchronicliver disease,withactuarialsurvival rates of up to 80% in five and 75% in ten years.1 Early causesofgraftfailureandmortalityaremostlyrelatedto vascularcomplications,especiallyhepaticartery thrombo-sis (HAT) and portal vein thrombosis (PVT).2 There are a numberof recognizedriskfactors for thedevelopmentof thesecomplicationsinthepediatricpopulation,suchas dis-crepancybetween donorandrecipient arterial andportal diameter,surgicalskills,lowerrecipientweight,3andsmall portalveindiameter.4Therearenoconsistentdata regard-ingtheseriskfactorsinthepediatricpopulationofBrazil.
The aim of this study was to assess the frequency ofvascular complications inpediatric patients undergoing deceaseddonorliver transplantation (DDLT)at the Hospi-taldeClínicasdePortoAlegre, Brazil,andtoidentifythe factorsassociatedwiththesecomplicationsandmortality.
Methods
The charts of 99 first liver transplant recipients under 18 years of age who underwent DDLT at the Hospital de ClínicasdePortoAlegrebetweenMarchof1995and Novem-berof2009wereretrospectivelyreviewed.Thestudy was approvedbytheinstitution’sethicscommittee.
Duringthisperiod,128livertransplantswereperformed on 121 children and adolescents (range: 4 months to 18 years).Ofthese,29wereexcludedfromthesample:13who underwentemergencylivertransplantationduetofulminant hepatitis,six who received living donorgrafts, and three becausethepreservationsolutionwasn’ttheUniversityof Wisconsinsolution(UW).Theexclusioncriteriaweredefined
in order to avoid comparison bias based on immunologi-calor technicalfactorsinfluencingvascularcomplications. The patients were split into two groups for comparison: with vascular complications (n=19) and without vascular complications(n=88).Thesedatawereusedforunivariate andmultivariateanalysisinordertoidentifytheassociated factors.
Recipients were assessed for the following variables: age, gender, weight, transplant indication, PELD/MELD scores, type of allograft, type of anastomosis, vascular complications, management of these complications, and survival.Sincedataregardinggraftweightwasnotavailable for all patients, the donor weight/recipient weight ratio (DRWR)wasassessed.5
Thediagnosisofvascularcomplicationswasestablished by a minimum of two imaging modalities and/or surgi-cal confirmation. All transplants were performed by the samesurgicalteam,andthepiggybacktechniquewithvena cava preservation was the standard procedure. Vascular anastomosiswas performed under3.5 ×loupe magnifica-tions.APDSTM(Ethicon)(7-0polydioxanonemonofilament)
threadwasusedforarterialandportalsutures,anda non-absorbable5-0polypropylenemonofilamentwasusedonthe hepaticveins.Runningstitcheswereusedforvesselslarger than3mmindiameter,andsimpleinterruptedstitchesfor smallervessels.
abnormalities that justified testing. When DUS suggested a vascular complication, repeat ultrasound, angiography, computerizedtomography(CT)scanwithintravenous con-trast,and/or surgerywasperformed toconfirm ordiscard the diagnosis. Vascular complications were classified as arterial (hepatic artery) or venous (affecting the portal veinorsuprahepaticvenacava).Early complicationswere definedasthoseoccurringwithin30daysoftransplantation, whereaslatecomplicationswerethosethatoccurredafter thisperiod.
Statisticalanalysis
Quantitativedatawereexpressedasmedian,interquartile range,andminimumandmaximumvalues,andcategorical datawereexpressedascountsandpercentages.
Univariate analysis was performed on Kaplan-Meier curvescomparedbythelog-ranktest,yieldinghazardratios, 95%confidenceintervals,andtheirsignificance.A multivari-ateCoxmodelincludingsignificantvariables(p<0.20)was constructedandusedtoadjustforconfounders.Abackward selectionprocedure wasperformed,andallvariableswith p≥0.10wereremoved.Datawereanalyzedandprocessed
usingtheStatisticalPackageforSocialSciences(SPSS), ver-sion17.0.
Results
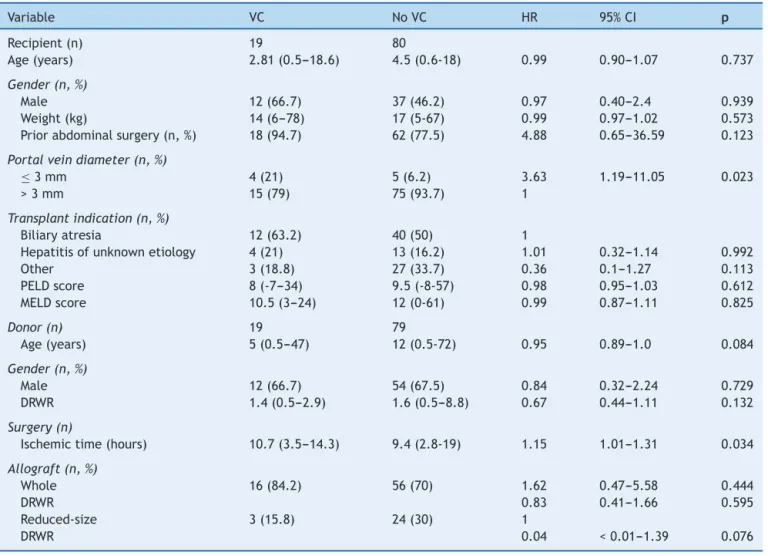
The main indication for transplant was biliary atresia (52.5%),followedbyhepatitisofunknownetiology(17.2%) andautoimmunehepatitis(7%).Medianrecipientweightwas 17.0kg (range: 5.0---78.0kg), and the median PELD score was 9.0 (range: 8.0---57.0). A total of 99 patients were included in the study; 72(72.7%) receivedan entire liver and27 (27.3%)receiveda reducedor splitgraft. Vascular complicationsoccurredin19(19.2%)patients.Medianage, weight,andDRWRinthecomplicationgroupwere2.1years (range:0.5---18.6 years),14.0kg(range:6.0---78.0kg), and 1.4(range:0.44---2.88),respectively(Table1).
Of the 19 patients with vascular complications, 16 received whole-liver transplants and three received reduced-sizegrafts(twoleftlobes andoneright lobeand segment).4Nopatientswithvascularcomplicationsreceived split grafts. Vascular malformations were found in five patients(26.3%),andreducedportalveindiameter(≤3mm) in four(21%). Venousgraftswere notused inthese cases becausethe graft wasn’t alwaysavailable or because the intraoperative evaluation concluded that the blood flow wasgood.Two patients (10.5%)needed grafts for arterial revascularization; in both cases, an autologous infrarenal aorticgraftwasused.Onlyonepatienthadneverundergone abdominalsurgerypriortotransplantation.
The most common complication was HAT (7%). Five patients(5%)developedPVT,three(3%)hadhepaticartery stenosis,andtwo(2%)hadportalveinstenosis.Onepatient had a mycotic aneurysm of the hepatic artery, and one developedstenosis ofthesuprahepatic-cavalanastomosis. Earlyvascularcomplicationsweremostfrequent,occurring in11patients(57.9%),withamortalityof81.8%.Vascular complication-freesurvivalisshowninFig.1A.
Inallpatients,adiagnosisofvascularcomplicationwas suggestedbyDUS.Thedefinitivediagnosiswasestablished byrepeatedDUS inthreepatients(15.8%),angiographyin eight (42.1%), CT scan with intravenous contrast in four (21%),andreoperationinseven(36.8%).
Clinical management with intravenous heparin (Liquemine®) and oral acetylsalicylic acid were admin-istered in six patients, with a mortality rate of 33.3%. Percutaneous treatment was indicated in four patients: threeunderwentangioplastyandtworeceivedstents.The primarypercutaneousmanagementwaswithballoon dilata-tion; the stent was inserted when the balloon dilatation alonewasinsufficient.Inonecase,thestentwasindicated becauseofarterialkinking.Allpercutaneousinterventions weresuccessful,andallfourpatientswerealiveattheend of follow-up. Seven patients were submitted to surgery, five of whom (71.4%) underwent thrombectomy with reanastomosis.All died,includingtwowho wereawaiting transplantation. In the remaining two patients (28.6%), re-transplantation(rLT) wastheinitialsurgical treatment, butneithersurvived.
The outcomes are listed in Table 2. One patient in whomrLT wasindicated died beforeanytreatment could be administered. Overall mortality in patients with vas-cular complication was 57.9%, and seven deaths (36.8%) weredirectlycorrelatedtothevascularcomplication.Other causesofdeathweresepsis,renalfailure,pneumonia, pneu-mothorax,tuberculosis,intracranialbleeding, andchronic rejection.
Intheunivariateanalysis,portalveindiameter≤3mm andprolongedischemictimeweresignificantriskfactorsfor vascularcomplications(p<0.05).Apriorhistoryof abdomi-nalsurgeryalsohadsignificanceasariskfactor(p<0.20,HR 4.88).TheresultsofunivariateanalysisareshowninTable1. Stratificationbygrafttypedemonstratedthatincreased DRWRwasaprotectionfactoragainstvascularcomplications inpatientsreceivingreducedgrafts.Afteradjustingfor con-founders with Cox multivariate analysis, portal diameter ≤3mm (p=0.026;HR4.51;Fig.1B), DRWR(p=0.072; HR 0.61),prolongedischemictime(p=0.06;HR1.26),andthe useofarterialgrafts(p=0.025;HR7.82)remainedashighly significantriskfactorsforvascularcomplications(Table3). Thesurvivalofpediatriclivertransplantrecipientswho developed vascular complications was significantly lower (Fig.1B).
Discussion
Livertransplantationin thepediatric settingistechnically challengingduetothereducedsizeofthevasculatureand biliarytree.Discrepanciesinportalveinandhepaticarterial diameterbetween thedonorandrecipientareexpected.1 Theincidenceofvascularcomplicationsreportedinthe lit-eraturevarieswidely amongcenters,butis alwayshigher thaninadultsamples.6,7
Table1 Samplecharacteristicsandunivariateanalysis.
Variable VC NoVC HR 95%CI p
Recipient(n) 19 80
Age(years) 2.81(0.5---18.6) 4.5(0.6-18) 0.99 0.90---1.07 0.737
Gender(n,%)
Male 12(66.7) 37(46.2) 0.97 0.40---2.4 0.939
Weight(kg) 14(6---78) 17(5-67) 0.99 0.97---1.02 0.573
Priorabdominalsurgery(n,%) 18(94.7) 62(77.5) 4.88 0.65---36.59 0.123
Portalveindiameter(n,%)
≤3mm 4(21) 5(6.2) 3.63 1.19---11.05 0.023
>3mm 15(79) 75(93.7) 1
Transplantindication(n,%)
Biliaryatresia 12(63.2) 40(50) 1
Hepatitisofunknownetiology 4(21) 13(16.2) 1.01 0.32---1.14 0.992
Other 3(18.8) 27(33.7) 0.36 0.1---1.27 0.113
PELDscore 8(-7---34) 9.5(-8-57) 0.98 0.95---1.03 0.612
MELDscore 10.5(3---24) 12(0-61) 0.99 0.87---1.11 0.825
Donor(n) 19 79
Age(years) 5(0.5---47) 12(0.5-72) 0.95 0.89---1.0 0.084
Gender(n,%)
Male 12(66.7) 54(67.5) 0.84 0.32---2.24 0.729
DRWR 1.4(0.5---2.9) 1.6(0.5---8.8) 0.67 0.44---1.11 0.132
Surgery(n)
Ischemictime(hours) 10.7(3.5---14.3) 9.4(2.8-19) 1.15 1.01---1.31 0.034
Allograft(n,%)
Whole 16(84.2) 56(70) 1.62 0.47---5.58 0.444
DRWR 0.83 0.41---1.66 0.595
Reduced-size 3(15.8) 24(30) 1
DRWR 0.04 <0.01---1.39 0.076
Dataexpressedas‘‘median(interquartilerange)[range]’’oras‘‘number(%).’’
CI,confidenceinterval;DRWR,donortorecipientweightratio;HR,hazardratio;MELD,modelforend-stageliverdisease;p,p-value;
PELD,pediatricmodelforend-stageliverdisease;VC,vascularcomplication.
Duffyetal.reportedHATrates of8% versus3.9%in pedi-atricandadultpatients,respectively,inasampleof4,234 transplantsperformedon3,558patientsattheUniversityof California,LosAngeles,intheUnitedStates.7Uchidaetal. reportedanincidenceofHATof6.7%afterLDLTinthe pedi-atricpopulation, withaten-yearsurvivalof78%.3Theuse ofmicrovascular techniques in arterialreconstructionhas diminishedthiscomplication,especiallyinchildren.
Patientswith HAT areat a higher risk of allograftloss (53%),morbidity,andmortality(33%).10,12,13Allevents are moresevereinearlycomplications.6,9,14 Thefactthatonly
one of the patients withHAT survivedmay be associated withlatediagnosisandthelack ofavailablegraftsintime forrLT.
Venous complications are less frequent than arterial complications,andthemost commonis PVT.11 These find-ings were not different in the present patients. Unlike arterial complications, venous events occur later. Ueda etal.reporteda 9%rateofportalveincomplications ina review of 521 pediatric patients whounderwent LDLT. Of the 47 patients in the portal event group, 38 were diag-nosedwithacomplication3monthsaftertransplant.15Moon
Table2 Managementofvascularcomplications.
Treatment Arterial
(n=10)
Portal (n=5)
Hepaticvein (n=2)
Anticoagulation(n,%);SR 3(30);1/3 3(43);3/3
Percutaneous(n,%);SR 2(20);2/2 2(29);2/2
Surgicalrevision(n,%);SR 4(40);0/4 1(14);0/1
PrimaryrLT(n,%);SR 1(10);0/1 1(14);0/1
1.0
0.8
0.6
0.4
0.2
0.0
1.0
0.8
0.6
0.4
0.2
0.0
0.00 30.00 60.00 90.00 PV≤3mm
P=0.023 PV>3mm
Follow-up (months)
Follow-up (months)
With VC
Without VC
Sur
viv
al
Propor
tion of v
ascular
complication-free patients
82 79 75 75 75 75 75
5 5 5
5 5
5 6
120.00 150.00 180.00
0.00 30.00 60.00 90.00 120.00 150.00 180.00 No. at risk
PV>3mm PV≤3mm
A
B
Fig.1 A,Kaplan-Meier curveofvascularcomplicationsafterorthotopic livertransplantationinpatients withportalvein(PV) diameter>3mmvs.≤3mm.B,Kaplan-Meiercurvesofsurvivalinorthotopiclivertransplantrecipientswithorwithoutvascular
complications(VC).
etal.reportedan11.2%incidenceofportalcomplications in another sample of patients undergoing LDLT (n=96). Once again, most complications occurred 3 months after transplantation.16Kawanoetal.alsoreportedanincidence of9%oflateportalveinstenosisfollowingLDLT;allpatients
Table 3 Factors associated with vascular complications inpatientsundergoingorthotopiclivertransplantation.Cox multivariateregressionanalysis.
Variable HR 95%CI p
Recipient
Portalveindiameter
<3mm 4.51 1.20---16.95 0.026
>3mm 1
DRWR 0.61 0.36---1.04 0.072
Surgery
Ischemictime(hours) 1.26 1.07---1.49 0.006 Arterialgraft 7.82 1.29---47.29 0.025
CI,confidenceinterval;DRWR,donortorecipientweightratio;
HR,adjustedhazardratio;p=p-value.
weretreated by interventional radiology.17 Stillregarding livingdonation,anotherstudyreportedanincidenceof15% ofportalcomplications inthe pediatricgroup,associating withadiscrepancyinportalveindiameter.11,18
Venousgrafts were not used in thesecases because por-talflowwaspresentandconsideredadequateafterFogarty balloonportalveindilation.
Intheir studyof HAT,Stewartetal. foundan ischemic timeof12hoursormoretobeasignificantriskfactorfor vas-cularcomplications(p<0.001).20Inthepresentsample,four outofsixpatientswithprolongedischemictimedeveloped HAT.Lowerbodyweightandhighergrafttorecipientweight ratio(GRWR)werealsoinflictedasriskfactorsforHATinthe pediatricpopulation.3GRWRcouldnotbeassessedbecause graftweightwasn’tavailablein mostcases.Thisdatahas only been routinely collectedin the last 5 years.Lack of appropriatedataisalimitationofretrospectivestudies.
In ordertotry toevaluate theimpactof graft size on vascularcomplications,DRWRwasassessed.Ohetal.also assessedDRWR,andnotedthat patientswhoreceive allo-graftsfromsmalldonorshavesignificantlyhigherHATrates (p=0.002).5In thepresent study,ahighDRWR wasa pro-tective factor afterstratification by graft type(wholevs. partial).Inpatientswithreduced-sizegrafts,thehigherthe DRWR,thelowerthepotentialfor vascularcomplications. Thisphenomenonisbelievedtobeduetothelargervessel diameter.
Theuseofarterialgraftsforvascularreconstructionhas also been debated as a risk factor. In the present study, multivariateanalysisdemonstratedthat patientsrequiring arterial grafts had higher rates of vascular complications (p=0.025). A meta-analysis conducted by Bekker et al. foundfourstudiesassessing theuseofarterial graftsasa riskfactorforvascularcomplications.Inthreeofthese stud-ies,twoof which employedmultivariateanalysis,arterial graftswereindeedfoundtobeariskfactor.5,10,21 Arecent publicationbyBackesetal.reportedtheirexperiencewith arterialgraftsin58recipients,38duringprimaryliver trans-plantationand20rLT.TheincidenceofearlyHATwas6.8% inprimarylivertransplantationrecipients,andnoneinthe rLT.Iliacarterygraftwithinfrarenalaorticanastomosiswas thetechniqueofchoice;however,thestudywasn’t fitfor theevaluationofriskfactors.22
Atleastthreemodalitiesareavailableforthetreatment ofvascularcomplications:revascularization,rLT,orclinical management.Thechoicedependsonthetimingof diagno-sis.rLT providesthe best outcomes and is the treatment ofchoiceinmostgroups;however,itisseverelylimitedby thescarcityofdonors.10,23Inearlyvascularcomplications, attemptsat emergencyrevascularizationthrough percuta-neousintervention(angioplasty)orsurgicalre-explorationis thefirststepinmanagement,particularlyinHAT.24,25Inthe eventofirreversiblecelldamage,rOLTistheonlyoption.26 Revascularization success rates are approximately 50%.10 Thrombectomyisnotindicated inlate-onsetHAT,whichis usuallycomplicatedbyischemiaandbiliarytractinjury,and isthusbesttreatedbyrLT.27Patientswithlate-onsetPVTand portalhypertensionbutnoliverfunctioncompromisemay benefit from splenorenal shunting. If intra-hepatic portal veinsarepermeable, ameso-Rexshuntmaybeperformed rLTismandatoryinearly-onsetPVTwithgraftdysfunction.28 Inthepresentstudy,highmortalityrateswereobserved in patients undergoing revision of anastomosis with thrombectomy;patientsmanagedwithpercutaneous inter-vention (angioplasty) had better outcomes. Few patients underwent rLT, but several died while awaiting the
procedure, as reported elsewhere.29 In the present sam-ple,thetimetorLT limitedtheresults,sincethescarcity of donors delayed the rescue procedure. Outcomes are encouraging in asymptomatic patients treated with early revascularization after incidental diagnosis of vascular complicationsonDUS.24,25 Graftsurvivalratesafter revas-cularization are substantially higher in this group than in symptomaticpatients(81.8%vs.40%).24
Conclusion
Despitetechnicalprogressinpediatriclivertransplantation, vascularcomplicationsarestillasignificantdeterminantof allograftloss,increasingpostoperativemorbidityand mor-tality.
Arterial complications are more common, occur early in the postoperativeperiod,and areassociatedwith high ratesofgraftlossandpatientmortality.Conversely,venous complicationsarelessfrequent,occurlateinthe postoper-ativeperiod,andhavenosignificanteffectongraftlossor mortalityrates.
Strategies for identification and mitigation of risk fac-tors, preventionoftechnicalcomplications, andprotocols forearlydetectionofvascularcomplicationsmayreducethe needforrLT,thusproducingalong-termpositiveeffecton treatmentofpatientswithend-stageliverdisease. Develop-mentofthesestrategiesisachallengeyettobeovercome.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.JaraP, Hierro L. Childhood liver transplantation.Long term results.GastroenterolHepatol.2010;33:398---410.
2.HuangTL,ChengYF,ChenTY,TsangLL,OuHY,YuCY,et al. Doppler ultrasound evaluation of postoperative portal vein stenosisinadultlivingdonorlivertransplantation.Transplant Proc.2010;42:879---81.
3.UchidaY,SakamotoS, EgawaH,OgawaK, OguraY,Taira K, etal.Theimpactofmeticulousmanagementforhepaticartery thrombosisonlong-termoutcomeafterpediatriclivingdonor livertransplantation.ClinTransplant.2009;23:392---9.
4.SuzukiL, deOliveiraIR,WidmanA,GibeliNE,CarnevaleFC, MaksoudJG, etal.Real-timeand DopplerUS afterpediatric segmentallivertransplantation:I.portalveinstenosis.Pediatr Radiol.2008;38:403---8.
5.OhCK,PelletierSJ,SawyerRG,DacusAR,McCulloughCS,Pruett TL,etal.Uni-andmulti-variateanalysisofriskfactorsforearly andlatehepaticarterythrombosisafterlivertransplantation. Transplantation.2001;71:767---72.
6.HardikarW, Poddar U, Chamberlain J, Teo S, Bhat R, Jones B, et al. Evaluation of a post-operative thrombin inhibitor replacementprotocoltoreducehaemorrhagicandthrombotic complications afterpaediatric liver transplantation. Thromb Res.2010;126:191---214.
7.DuffyJP,HongJC,FarmerDG,GhobrialRM,YersizH,HiattJR, etal. Vascularcomplications oforthotopicliver transplanta-tion:experienceinmorethan4,200patients.JAmCollSurg. 2009;208:896---903.
Aggressivemanagementofthearterialcomplicationsofliver transplantation.Impactuponsurvivalandbiliarycomplications. CirEsp.2010;87:155---8.
9.ZanotelliML,VieiraS,AlencastroR,KielingC,LeipnitzI, Fer-reiraC, et al. Management of vascular complications after pediatriclivertransplantation.TransplantProc.2004;36:945---6.
10.Bekker J, PloemS, de Jong KP.Early hepaticartery throm-bosis after liver transplantation: a systematic review of the incidence, outcome and risk factors. Am J Transplant. 2009;9:746---57.
11.TakahashiY,NishimotoY,MatsuuraT,HayashidaM,TajiriT, Soe-jimaY, et al. Surgicalcomplications after livingdonor liver transplantation in patients with biliary atresia: a relatively highincidenceofportalveincomplications. PediatrSurgInt. 2009;25:745---51.
12.Jean-Bernard O. Approach to avoid and to manage vascular thrombosisandstenosisinpediatriclivertransplantation. Pedi-atrTransplant.2007;11:124---6.
13.NetoJS,PuglieseR,FonsecaE,VincenziR,PuglieseV,Candido H,etal.Fourhundredthirtyconsecutivepediatriclivingdonor liver transplants: variables associated with post transplant patientandgraftsurvival.LiverTransplant.2012;18:577---84.
14.MorayG,BoyvatF,SevmS,KarakayaliF,AyvazI,Dalgic¸A,etal. Vascularcomplicationsafterlivertransplantationinpediatric patients.TransplantProc.2005;37:3200---2.
15.Ueda M, Oike F, Kasahara M, Ogura Y, Ogawa K, Haga H, et al. Portal vein complications in pediatric living donor livertransplantation using left-side grafts. Am J Transplant. 2008;8:2097---105.
16.MoonJI, JungGO,ChoiGS, KimJM,ShimM,Kim EY,etal.
Riskfactors forportal vein complicationsafterpediatric liv-ingdonorlivertransplantationwithleft-sidedgrafts.Transplant Proc.2010;42:871---5.
17.KawanoY,MizutaK,SugawaraY,EgamiS,HisikawaS,Sanada Y,etal.Diagnosisandtreatmentofportalveinstenosisafter livingdonorlivertransplantation.TransplInt.2009;22:1151---8.
18.ShibasakiS,TaniguchiM,ShimamuraT,SuzukiT,YamashitaK, WakayamaK,etal.Riskfactorsforportalveincomplications inpediatriclivingdonorlivertransplantation.ClinTransplant. 2010;24:550---6.
19.Broniszczak D,SzymczakM,Kaminski A, ChyzynskaA, Ismail H, Drewniak T, et al. Vascular complications after pediatric livertransplantationfrom thelivingdonors.TransplantProc. 2006;38:1456---8.
20.StewartZA,LockeJE,SegevDL,DagherNN,SingerAL, Mont-gomeryRA,etal.Increasedriskofgraftlossfromhepaticartery thrombosisafterlivertransplantationwitholderdonors.Liver Transpl.2009;15:1688---95.
21.Silva MA,JambulingamPS, GunsonBK, MayerD, BuckesJA, MirzaDF,etal.Hepaticarterythrombosisfollowingorthotopic livertransplantation:a10-yearexperiencefromasinglecentre intheUnitedKingdom.LiverTranspl.2006;12:146---51.
22.BackesAN,GibelliNE,TannuriAC,SantosMM,Pinho-Apezzato ML,AndradeAC,etal.Hepaticarterygraftinpediatricliver transplantation:single-centerexperiencewith58cases. Trans-plantProc.2011;43:177---80.
23.ParejaE,CortesM,NavarroR,SanjuanF,LopezR,MirJ. Vascu-larcomplicationsafterorthotopiclivertransplantation:hepatic arterythrombosis.TransplantProc.2010;42:2970---2.
24.SheinerPA,VarmaCV,GuarreraJV,CooperJ,GarattiM,EmreS, etal.Selectiverevascularizationofhepaticarterythromboses afterlivertransplantationimprovespatientandgraftsurvival. Transplantation.1997;64:1295---9.
25.KimBW,WonJH,LeeBM,KoBH,WangHJ,KimMW.Intraarterial thrombolytictreatmentforhepaticarterythrombosis immedi-atelyafterlivingdonorlivertransplantation.TransplantProc. 2006;38:3128---31.
26.CoelhoJC,MatiasJE, ParolinMB,MartinsEL,SalvallagioPR, Gonc¸alves CG.Complicac¸õesvasculares pós-transplante hep-ático.RevColBrasCir.2000;27:378---82.
27.Jain A, Costa G, Marsh W, Fontes P, Devera M, Mazarie-gos G, et al. Thrombotic and nonthrombotic hepatic artery complications in adults and children following primary liver transplantationwithlong-termfollow-upin1000consecutive patients.TransplInt.2006;19:27---37.
28.AlvarezF.Portalveincomplicationsafterpediatricliver trans-plantation.CurrGastroenterolRep.2012;14:270---4.