w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Comprehensive
neuropsychological
evaluation
of
children
and
adolescents
with
sickle
cell
anemia:
a
hospital-based
sample
Samantha
Nunes
∗,
Nayara
Argollo,
Marivania
Mota,
Camilo
Vieira,
Eduardo
Pondé
de
Sena
UniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received14May2016 Accepted12September2016 Availableonline7October2016
Keywords:
Anemia,sicklecell Intelligencetests Neuropsychologicaltests Behavioraldisorders
Neurobehavioralmanifestations
a
b
s
t
r
a
c
t
Background:Individualswithsicklecellanemiamaysuffersymptomaticorsilentcerebral infarctsleadingtoneurocognitivecomplications.Thisstudyinvestigatedthecognitiveand intellectualperformanceofchildrenandadolescentswithsicklecellanemia.
Methods:Thesocioeconomicstatus,clinicalaspectsandbehavioralprofileof15young indi-vidualswithsicklecellanemiawereevaluated.TheWechslerIntelligenceScaleforChildren, theDevelopmentalNeuropsychologicalAssessmentTest,andtheChildBehaviorChecklist wereapplied.
Results:Participantswithahistoryofstrokehadlowerintelligencequotient(IQ)scores. Alterationswerefoundinattentionandexecutivefunctioning,language,verbalandvisual memory,visuospatialprocessingandsensorimotorskills.Thesealterationswerefoundboth inthechildrenandadolescentswhohadhadacerebralinfarctionandinthosewho appar-entlyhadnot.Inthemajorityofcases,therewerelearningdifficulties,ahistoryofrepeating schoolyearsandaneedforspecialisteducationalsupport.Themostcommonadditional diagnosesinaccordancewiththeDiagnosticandStatisticalManualofMentalDisorders IVweredepressivedisorder,anxietydisorderandsomaticdisorder,aswellasconditions associatedwithphysicalandpsychosocialrepercussionsofsicklecellanemia.
Conclusion:Assicklecellanemiaisconsideredaprogressivecerebralvasculopathy,itisa potentialriskfactorforneurocognitiveandpsychosocialdevelopment.Therefore,periodic neuropsychologicalandbehavioralevaluationsofchildrenandadolescentswithsicklecell anemiamayrepresentausefulmeasuretoreducelong-termbiopsychosocialrepercussions. ©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:ProgramadePós-Graduac¸ãoProcessosInterativosdosÓrgãoseSistemas,InstitutodeCiênciasdaSaúde, UniversidadeFederaldaBahia(UFBA),AvenidaReitorMiguelCalmon,S/N,ValedoCanela,40110-902Salvador,BA,Brazil.
E-mailaddress:[email protected](S.Nunes).
http://dx.doi.org/10.1016/j.bjhh.2016.09.004
revbrashematolhemoter.2 0 1 7;39(1):32–39
33
Introduction
Sicklecelldisease(SCD)comprisesagroupofinheritedblood disordersresultingfromageneticalterationinhemoglobin.It isthemostcommonmonogenichereditarydiseaseinBrazil.1
InthestateofBahia,thenumberofindividualswiththesickle celltraitisestimatedat5.5%ofthegeneralpopulationand 6.3%ofthepopulationofAfricandescent.Theincidenceof sicklecellanemia(SCA)inBahiaisthehighestinBrazil:1in 650livebirths.2
Ohene-Frempong etal. reportedthat 11% ofindividuals withSCAdevelopsymptomaticcerebralinfarctspriorto com-pleting20yearsofage. Thesequelaeoftheseeventsaffect differentaspectsofthepatient’slife.Overall,11–35%of chil-drenand adolescentswith SCDpresent withsilentstrokes identifiedonlybyimagingexamsandwithnoobservable clin-icalsymptoms.3
Theneurocognitivecomplicationsandtheirconsequences areprogressiveandoriginatefromastateofcerebral vascu-lopathy,negativelyaffectingchilddevelopmentandqualityof life.4
Theprincipalobjectiveofthisstudywastoevaluate cog-nitive function and the behavioral profile of children and adolescentswithsicklecellanemia.
Methods
TheInternalReviewBoardofthePlataformaBrasilofthe Profes-sorEdgardSantosTeachingHospital,UniversidadeFederalda Bahiaapprovedtheprotocolofthisdescriptive,observational, hospital-basedstudy(#314.636).
Fifteenchildrenandadolescentswithagesrangingfrom6 to16yearsandSCAdiagnosedbyhemoglobin electrophore-sisparticipatedinthisstudy.Childrenwithvisualorauditory deficits, epilepsy, a history of brain trauma, meningitis or intoxications,ahistoryofgestationalorneonatalanoxicbrain injury,prematurity, concomitant geneticsyndromesor any other conditionthat would preventthe psychometrictests frombeingconductedwereexcludedfromthestudy.
Thechildren’sparentsorguardians wereinterviewed at admission.Thechild’s birthregistrationcardwas reviewed toobtaindatarelatedtopregnancyandneonatalconditions. Theschoolreportwas usedto evaluateneuropsychomotor
development and educational history, data on the clinical characteristicsofSCDwereobtainedandthesocioeconomic criteriaoftheAssociac¸ãoBrasileiradeEmpresasdePesquisa (ABEP)wereapplied.5
AshortformoftheWechslerIntelligenceScaleforChildren (Third Edition–WISC-III) wasused toestimate the intelli-gencequotient(IQ).Thisinstrumentisusedasascreeningtool toevaluatetheintellectualperformanceofBrazilianchildren (Table1).6,7
Fifteensubtestsofthedevelopmentalneuropsychological assessmenttest(secondedition–NEPSY-II)8wereselectedto
investigatecognitivefunction.Thistooltakesabroadand flex-ible approachto neuropsychological evaluation.Percentiles wereusedtoclassifyperformanceinthisassessment(Table1). TheChildBehaviorChecklist(CBCL),aquestionnaire con-sistingof113items,developedtoevaluateindividualsinthe 6–18agerange,wasappliedtoparentsorguardians9(Table1).
Results
Ofthefifteencasesevaluated,nine(60%)weremale.Themean ageofthepatientswasnineyears(range:6–16years).Ofthe 15 patients, 12 (80%)were right-handed, whilethree (20%) becameleft-handedafterhavingsufferedalefthemisphere stroke.Inthesecases,thetrainedlefthandwasconsidered thedominanthand.
In nine (60%) cases, the family reported that the child needed specialisteducational supportdue todifficultiesat school.
TheIQtestwasfoundtobewithinthenormalrangefor ten(66.6%)participants,whilefour(26.6%)hadalowerthan averagescore,andone(6.6%)scoredaboveaverage.Ofthefour (26.6%)participantswhoscoredbelowaverage,three(20%)had aborderlinescore(70–79).ThemeanIQscorewas88.5.
Inthemajorityofcases,theindividual’sperformancewith respecttoimmediatememorywaspoorforvisual,spatialand verbalcontentaswellasinthesubtestsofattentionand exec-utivefunctioning,languageandsensorimotorskills(Table2). Overall,nine(60%)participantsperformedbelowaverageinat leastoneoftheNEPSY-IIsubtests(Table3).
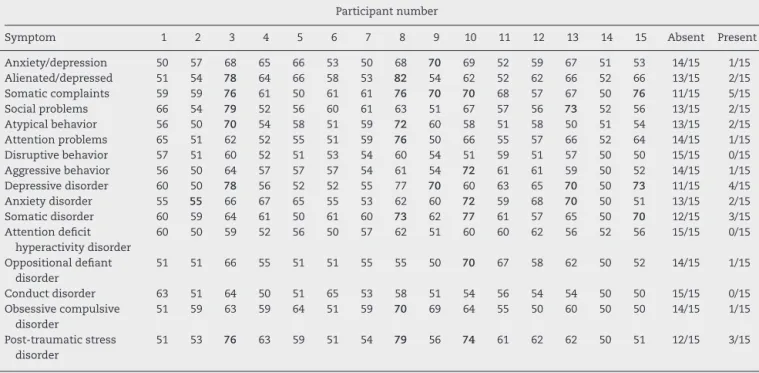
Thebehavioralprofileanddiagnosticcriteriabasedonthe DiagnosticandStatisticalManualofMentalDisorders(fourth Edition)aredescribedinTable4.
Table1–ClassificationofperformanceaccordingtotheWechslerIntelligenceScaleforChildren(ThirdEdition) intelligencequotient(IQ),DevelopmentalNeuropsychologicalAssessmentTest(secondedition)andChildBehavior Checklist.
EstimatedIQa NEPSY-IIb CBCLc
Index Classification Percentile Classification T-score Percentile Classification
≤79 Low ≤25th Low ≤64 ≤85th Normal
80–119 Average 26–75th Average 65–69 86–96th Borderline
≥120 High 76–99th High ≥70 ≥97th Clinical
a WISC-III:WechslerIntelligenceScaleforChildren.7
b NEPSY-II:adevelopmentalneuropsychologicalassessment.8
rev
bras
hema
tol
hemoter.
2
0
1
7;
3
9(1)
:32–39
Table2–PerformanceintheDevelopmentalNeuropsychologicalAssessmentTest(secondedition)subtests.
Participantnumber
NEPSY-IIsubtests 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Low Mean
Auditoryattentiontotalcorrect <2 2 75 26 26 5 <2 50 50 25 75 26 <2 25 26 7/15 8/15 Auditoryattentioncommissionerrors <2 50 50 50 50 <2 <2 50 50 25 50 50 75 50 50 4/15 11/15 Auditoryattentionomissionerrors <2 25 50 50 50 <2 <2 50 50 50 50 50 <2 25 50 6/15 9/15 Auditoryattentioninhibitionerrors 10 50 50 50 50 50 <2 50 50 50 50 50 50 50 50 2/15 13/15 Auditoryresponsesettotalcorrect <2 25 2 10 10 25 <2 75 50 25 25 10 NC 50 50 10/14 4/14 Auditoryresponsesettotalcommissionerrors 5 50 75 <2 25 10 <2 50 50 5 50 25 NC 50 50 7/14 7/14 Auditoryresponsesettotalomissionerrors <2 25 <2 <2 25 5 <2 75 50 25 25 25 NC 75 75 10/14 4/14 Auditoryresponsesettotalinhibitionerrors 10 50 50 25 75 50 25 75 50 25 75 50 NC 25 50 5/14 9/14
Designfluency 5 2 NC 5 5 50 NC NC NC 10 75 5 <2 <2 10 9/11 2/11
Inhibitiontotalerrors <2 10 25 50 5 <2 IN 75 75 <2 75 <2 <2 <2 5 10/14 4/14 Narrativememoryfreeandcuedrecall <2 <2 10 50 75 25 5 2 75 5 50 75 25 5 10 10/15 5/15 Narrativememoryfreerecall 25 10 5 50 50 25 10 <2 75 10 50 75 5 25 25 10/15 5/15
Memoryforfaces NC NC NC 75 75 75 NC NC NC 5 25 50 75 25 10 4/9 5/9
Memoryfordesignscontent 10 25 10 50 75 25 <2 25 50 10 25 5 <2 2 10 12/15 3/15 Memoryfordesignsspatial 10 10 50 25 50 10 <2 75 10 25 25 2 5 <2 75 11/15 4/15 Memoryfordesignstotal 5 25 10 50 50 25 <2 25 25 25 25 5 <2 <2 10 13/1 2/15 Memoryfordesignsdelayedcontent <2 50 25 P 75 25 <2 25 75 P 25 15 NC 10 25 9/12 3/12 Memoryfordesignsdelayedspatial <2 50 10 25 75 25 2 75 75 P 25 10 25 10 75 9/14 5/14 Memoryfordesignsdelayedtotal <2 75 10 10 75 10 <2 25 75 NC 10 10 10 25 75 10/14 4/14 Listmemoryandlistmemorydelayed 10 5 NC 25 25 25 NC NC NC 25 25 75 NC 50 75 7/10 3/10 Comprehensionofinstructions 10 10 2 10 25 19 <2 5 75 5 75 25 2 25 25 13/15 2/15 Phonologicalprocessing 10 <2 25 25 10 5 IN 2 50 5 50 <2 5 24 25 12/14 2/14 Speedednamingcorrect 10 5 2 <2 25 2 IN 50 50 <2 75 2 NC <2 5 9/13 4/13 Speedednamingtime 5 <2 25 <2 75 <2 IN 25 75 <2 50 <2 NC 50 75 8/13 5/13 Speedednamingerrors 50 25 50 25 50 <2 IN 50 50 50 25 25 NC 25 50 6/13 7/13 Wordgenerationsemantic 2 75 25 10 50 2 <2 25 50 10 75 50 5 50 75 9/15 6/15 Wordgenerationinitialletter <2 25 10 25 75 2 <2 75 25 <2 50 <2 NC 10 25 11/14 3/14
Arrows <2 25 25 17 50 10 <2 25 10 25 50 50 <2 <2 50 11/15 4/15
Geometricpuzzles 2 10 10 50 75 10 5 25 2 50 2 50 25 <2 25 11/15 4/15
Imitatinghandpositions <2 50 NC 25 50 2 NC NC NC 50 10 10 <2 <2 75 7/11 4/11 Imitatinghandpositions(dominanthand) 75 25 NC 10 50 50 NC NC NC 50 10 5 <2 <2 75 6/11 5/11 Imitatinghandpositions(non-dominanthand) <2 75 NC 50 75 <2 NC NC NC 50 25 25 <2 2 75 6/11 5/11 Visuomotorprecisiontime 75 <2 NC <2 50 25 NC NC NC 25 50 10 75 25 25 7/11 4/11 Visuomotorprecisionerrors <2 75 NC 75 75 <2 NC NC NC 75 50 25 <2 <2 50 5/11 6/11
NC:testnotcarriedoutforage;IN:inabilitytoanswertest.
revbrashematolhemoter.2 0 1 7;39(1):32–39
35
Table3–Socioeconomicandclinicalclassificationofthechildrenandadolescentswithsicklecellanemia.
Participantnumber
Characteristics 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Gender F F M F M M M M F M F M M F M
Age(years–mean: 10)
12 12 13 8 10 8 15 16 14 7 7 10 6 7 10
Right-handed Yes Yes Yes Yes Yes No No Yes Yes Yes Yes Yes No Yes Yes Typeofschool Pub Priv Pub Priv Priv Pub Pub Pub Priv Priv Priv Pub Priv Priv Priv Appropriateclassfor
age
No No No Yes Yes Yes No Yes Yes No Yes No No Yes Yes
Learningdifficulty Yes Yes Yes Yes Yes No Yes No No Yes No Yes Yes No Yes Mother’syearsof
schooling
Miss 4 12 16 12 8 12 12 14 4 12 8 6 10 12
Socioeconomiclevel B B B A B C C B A B B B B B C
Ageatdiagnosis (months–mean: 5)
36 4 0 4 0 0 9 4 12 0 0 0 0 0 1
Ageatbeginningof treatment (months–mean: 7)
36 9 0 15 1 0 11 4 12 6 1 2 6 0 2
Admissionsto hospital
>10 >10 >10 >10 4 >10 3 >10 >10 >10 4 4 >10 >10 >10
Bloodtransfusions >30 >30 >30 0 4 >30 >30 5 6 5 7 7 >30 >30 2 Hydroxyurea Yes Yes No Yes Yes Yes Yes No Yes Yes No Yes Yes No No Ischemicstrokes Yes Yes No No No Yes Yes No No No No No Yes Yes No Hemisphereaffected
bystrokes
Right Right None None None Left Left None None None None None Left Right None
Numberofstrokes 1 1 0 0 0 2 1 0 0 0 0 0 5 2 0
Silentinfarcts No No No No No No No No Yes No No No No No No EstimatedIQ(mean:
88.5)
77 77 91 94 100 71 56 91 103 85 123 91 80 83 106
M:male;F:female;Miss:missingdata;Pub:public;Priv:private;m:mean(range);f:frequency.
Table4–BehavioralprofileandStatisticalManualofMentalDisorders4thEditiondiagnosesfromtheChildBehavior Checklistevaluation.
Participantnumber
Symptom 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Absent Present
Anxiety/depression 50 57 68 65 66 53 50 68 70 69 52 59 67 51 53 14/15 1/15 Alienated/depressed 51 54 78 64 66 58 53 82 54 62 52 62 66 52 66 13/15 2/15 Somaticcomplaints 59 59 76 61 50 61 61 76 70 70 68 57 67 50 76 11/15 5/15 Socialproblems 66 54 79 52 56 60 61 63 51 67 57 56 73 52 56 13/15 2/15 Atypicalbehavior 56 50 70 54 58 51 59 72 60 58 51 58 50 51 54 13/15 2/15 Attentionproblems 65 51 62 52 55 51 59 76 50 66 55 57 66 52 64 14/15 1/15 Disruptivebehavior 57 51 60 52 51 53 54 60 54 51 59 51 57 50 50 15/15 0/15 Aggressivebehavior 56 50 64 57 57 57 54 61 54 72 61 61 59 50 52 14/15 1/15 Depressivedisorder 60 50 78 56 52 52 55 77 70 60 63 65 70 50 73 11/15 4/15 Anxietydisorder 55 55 66 67 65 55 53 62 60 72 59 68 70 50 51 13/15 2/15 Somaticdisorder 60 59 64 61 50 61 60 73 62 77 61 57 65 50 70 12/15 3/15 Attentiondeficit
hyperactivitydisorder
60 50 59 52 56 50 57 62 51 60 60 62 56 52 56 15/15 0/15
Oppositionaldefiant disorder
51 51 66 55 51 51 55 55 50 70 67 58 62 50 52 14/15 1/15
Conductdisorder 63 51 64 50 51 65 53 58 51 54 56 54 54 50 50 15/15 0/15 Obsessivecompulsive
disorder
51 59 63 59 64 51 59 70 69 64 55 50 60 50 50 14/15 1/15
Post-traumaticstress disorder
51 53 76 63 59 51 54 79 56 74 61 62 62 50 51 12/15 3/15
Discussion
Theparticipants’socioeconomiclevelsweresimilar.Mostof the children studied in private schools near their homes, wherethe pedagogical methodology usedand the require-mentsaresimilartothoseinpublicschools.
ThecommonsymptomsofSCAwerepresentinallcases andalltheparticipantswereundergoingspecialisttreatment, asrequiredbytheMinistryofHealthunderregulation#55 pub-lishedin2010.2Incompliancewithaclinicalprotocol,mostof
theindividualsweretakinghydroxyurea10andwerereceiving
bloodtransfusions,treatmentsthatarebasedonclinicaland scientificconsensus.2,11
Performanceinintelligencetestsisgenerally associated with academic achievement and both have proven useful measuresformonitoring achild’scognitive development.12
Theindividualsinthisstudywhohadhadastrokehadlower IQscoresandweretheonlyparticipantswhoscoredpoorlyin theWISC-IIIsubtestsofvocabularyandblockdesign.Twoof thesixindividualswithahistoryofstrokehadanIQscore within the normal range; nevertheless, these scores were lowerthanthoseobtainedbytheparticipantswhohadnothad strokes.Patientswhohadsufferedstrokesperformedpoorlyin allthefunctionsevaluated.Indeed,havinghadastroke predis-posestheindividualtomoreseverealterationsinintellectual andcognitivedevelopment,asshowninpreviousstudies.13
Althoughthisfindingisnotsurprising,itemphasizesthefact thatevenonestrokemaydefineachild’slife,reducinghis/her potentialinacademicdevelopmentandreducingemployment opportunitiesinadultlife.Inchildhood,thecostof perform-ingpoorly atschoolisobviouslyreflectedinareductionof formallearningandadecreaseincognitivereserve.Frequent hospitaladmissionstogether withpoorschoolperformance constitute the principal causes ofschool dropout in these children.14
Ingeneral,insofarastheneuropsychologicalevaluationis concernedchildrenwithSCAperformedpoorly.Noneofthe childrenfitthenormalprofileofatypicalchildinanyofthe testsusedinthis study.Ofthe tenchildrenwhose IQwas withinthenormalrange,sixhadlearningdifficulties. There-fore,eventhechildrenwithanaverageIQmayhavelearning difficultiesduetounderlyingcognitiveimpairment.
The NEPSY-II cognitive domain attention and executive functioningismorecloselyrelatedtoacademicachievement thantheIQ.15Thirteen(86.6%)participantsscoredbelow
aver-age in auditory selective, sustained and divided attention, cognitiveflexibility,workingmemoryandinhibitorycontrol. Thenumberofomissionerrorswasgreaterinthemore com-plex activities, as seen in the performance of ten of the participants.Attentionandexecutivefunctioningisreported tobethemostcommonlyaffecteddomaininindividualswith SCD,bothinthosewho havehadacerebralinfarctionand inthosewhohavenot.11Childrenwithattentionalterations
tendtoperformpoorlyinschoolactivitiesandneedmoretime toperformtasksthatrequirerationalthoughtand concen-trationsuchasreading,writing andarithmetic.They often need teacher mediation during class since they are easily distractedbyexternalstimuli.Becauseoftheirdifficulty in concentrating,theyfailtoabsorbaconsiderableamountof
thecontentprovidedinclass.Theirdifficultyinapplyingnew strategiestoresolveproblems,inadaptingtonewrulesandin theircapacitytoinhibitimpulsiveresponsesalsomeansthat thesechildrenrequiremoretimeforlearning.These charac-teristicsreflectimmaturityinthedevelopmentofbehavioral self-regulationandpersonalmanagement,whichalsoaffects theirpersonalperformance,sincedeficitsinthesefunctions resultinrelationshipsofgreaterdependencywithcaregivers toperformroutineactivities.13
The Memoryand Learningdomain reflects the acquisi-tionandconsolidationofinformation.11Resultswerefound
tobebelowaverageforverbalmemory,visuospatialmemory andimmediateanddelayedrecall,withapoorerperformance in visuospatial memory compared to narrative memory. Somestudieshavereportedalterationsindifferentmemory systems.16,17Ingeneral,lessimpairmentwasfoundin
narra-tivememorywithrespecttoimmediaterecognition.Academic adaptations thatuse this memorytoolcould beappliedto facilitatelearningatschool.
Fourteen (93.3%) patients had difficulties in the lan-guagefunctions:comprehensionofinstructions,phonological processing, and word generation within specific semantic andinitiallettercategories.Thepoorestperformancewasin verbalcomprehension.Theseandotheraspectsoflanguage developmentaredirectlyrelatedtolearningcapacityandto the developmentoftheprocessesofreadingand writing.18
Onestudyevaluatedimpairmentinthesemantic,syntaxand phonologicalfunctionsoflanguageinindividualswithSCD and suggestedthattheywereassociatedwithanalteration inshort-termmemoryprocesses,specificallywithadeficitin workingmemory.19 Inmostcases,therewasimpairmentin
bothfunctions,whichhamperedtheacademicperformanceof childrenwithSCAevenfurther,since,inadditiontothe alter-ationinexecutivefunctioning,therewereimportantdeficits inbasiclanguagefunctions.
Mostoftheparticipantshadsomedegreeofimpairment invisuospatialorientationandanalysisandintheircapacity formentalrotation.Inthetestsusedtoevaluate sensorim-otor ability,writing accuracy waswithin thenormal range in themajority ofcasesbut therewas difficulty inwriting speed,motorplanningandkinestheticfeedbackwhen perfor-mancewasevaluatedinbothhands.Somereviewarticleshave reportedsimilardeficits.11,13Theparticipantshadgreater
dif-ficultywithactivitiesthatdemandedmentalplanning,which isrequiredinschoolworkinvolvinggeometricand mechan-icalreasoningsuchastheexactsciences,possiblyexertinga negativeeffectontheirresults.Thespeedofmotorresponse wasalsofoundtobeimpaired,whichmayaffectnotetaking duringclass.Alternativessuchastheuseofconcretematerial andaudioorvideorecordingsofclassesmayhelpthese stu-dentswithspatialorganizationandmotorspeed.Oneofthe participants(Case#6),forcedtousehisnon-dominanthand, testedwithinthenormalrangewiththelefthandinmotor planningandkinestheticfeedback,leadingtoahypothesisof adaptationbasedonneuroplasticity.
revbrashematolhemoter.2 0 1 7;39(1):32–39
37
thelearningabilityofchildrenwithSCA,afindingthathasalso beenreportedinanotherstudy.20
The inherent complications of SCA, together with the individual’s socioeconomic difficulties and their alienation from social and school life, explains the finding that the behavioral profile of individuals with SCD often includes symptomssuchasanxiety/depression,alienation/depression and somaticcomplaints.SinceSCA isachronic disease,it representsariskfactorinpsychicdevelopmentandthe conse-quentappearanceofpsychopathologies.IndividualswithSCA sufferphysicalsymptomsofthediseaseandhavetocopewith itsnumerouslimitationsthatincluderestrictedphysicaland socialactivities,neurologicalsequelae,treatmentprocedures and constant hospital admissions in addition to cognitive difficulties and poor academic performance. All these fac-torspredispose childrenand their parentstohigher levels ofanxiety and depression, as shown in this and in other studies.20–22
The somatic complaints presented in seven cases may berelatedtochronicpain,sincepainfulcrisesarecommon in SCA as a consequence of inflammation and infections. ThesymptomsofSCAexplainthesomaticcomplaintsfound here.Similarresultswerereportedinanotherstudy,inwhich significantdifferences werefoundbetweenthenumbers of somaticcomplaintsinchildrenwithSCAcomparedto unaf-fectedchildren.20
Therewere fewercasesofproblemsrelatedtothesocial sphereandtoattention.Theparentsoffour(26.6%)children hadalreadyidentifiedattentionproblems;however,thirteen childrenactuallyhadabnormalities.Thebehavioral evalua-tion ofattention performed bythe parentsshowed results thatwerecompatiblewithcognitiveevaluationinonlythree (23%)ofthe13cases,suggestingthatbothinstrumentsneed tobeusedtoimproveunderstanding ofthecognitive func-tionstobeevaluated.Disagreementwiththeobjectivefinding ofdifficultiesintheattentiondomainmayindicatethat par-ents/guardiansfailtoperceivecognitivedeficitsintheirchild. Furthermore,duetothe intrinsiccharacteristicsofthe dis-ease,parentsareoftenrelativelyundemandinginsofarastheir child’slearningisconcernedorindeedmayallowthechildto abstaincompletelyfromschoolactivities.Thisfact empha-sizes the need to provide guidance on the importance of activitiesaimedatstimulatingbrainfunctionthatultimately improveself-esteemandincreasecognitivereserve.
ThemostcommondiagnosesbasedonDiagnosticand Sta-tisticalManual ofMental Disorders 4th Edition(DSM-IV)23
weredepressivedisorder,somaticdisorderand anxiety dis-order.Inaprevious study,depressionwasfoundin13% of childrenwithSCD.24Theriskofthediseasebecomingmore
severeandtheriskofdeath,aswellasadmissionstohospital andneurologicalsequelae,exposechildrenandtheirfamilies tocontinuousstress,increasingtheriskofpsychiatric disor-derssuchaspost-traumaticstressdisorder,identifiedinthree casesinthisstudy.25Thesedataindicatetheneedto
inves-tigateemotionalissuesandreferpatientsfortreatment.In addition,thefamilyneedsguidancetobeabletoprovide sup-portfortheirchild,ameasurethatmayhelpreducedepressive symptomsandimprovethequalityoflifeofthesechildren.24
Based on the CBCL, none of the children fulfilled the criteria for attention deficit hyperactivity disorder (ADHD).
Two studiesreportedsimilarCBCLresultsforchildrenwith
SCD.21,26 However,oneofthesestudiesidentifiedsymptoms
ofADHDinchildrenandadolescentswithSCDusingascale basedontheDSM-IV.
A similar study conducted with SCA children in the 7–12 age range found significant impairment in intellec-tualperformance,executivefunctioning,language,memory andvisuospatialskillscomparedtohealthychildren.27This
study reported adifferenceof13–14points inthe IQscore betweenchildrenwithSCAandcontrols.Inaddition, those with SCAwere more likelytofall behindat schooland to havetorepeatschoolyearsasaconsequenceoftheir learn-ingdifficulties.Behavioralandemotionalproblemswerealso reported.
There was no association inthis study between abnor-malities in any given type of cognitive function and any specificdisorder,sincemostoftheparticipant’simpairment waspresentinallthecognitivedomainsirrespectiveofthe presenceofapsychopathologicaldiagnosis.
Thehigher mean age ofthe patientsin this study may haveplayedarole inthe identificationofgreater cognitive impairment,sincestudiessuggestanincreaseinimpairment withincreasedageduetothegreaterpredispositionto neu-rologicaleventsandotherfactorsrelatedtothedisease.19,27
Fromapathophysiologicalviewpoint,SCAevolvesasvascular dementia.Withtime,thenumberofsilentinfarctsincreases andaseverestrokeoftenoccurs,leadingtofurther deteriora-tioninthechild’scognition.Addedtothis,absenteeismfrom schoolorevenschooldropoutatanearlyagereducescognitive stimulation.
When analyzed individually, Case #7 had the poorest overall performance. The patient had had a left ischemic stroke with noticeable motor (right hemiplegia) and lan-guageimpairment.Neuropsychologicalevaluationidentified reducedintellectualability(lowIQ)anddeficitsinallthe cog-nitivevariablesevaluated.
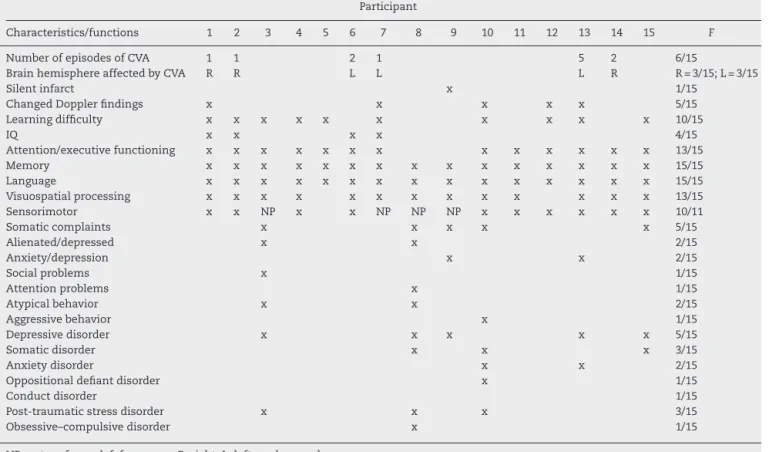
Itisinterestingtonotethatinthetwocases(#8and#9) inwhichattentionandexecutivefunctioningwaspreserved, therewasnohistoryoflearningdifficulties,althoughCase#9 had hadadocumentedsilentinfarctinthepast. Thismay reflectgreatercognitivereserveandadequatematernal stim-ulation,sincethemotherinthiscasewasattendinguniversity. Inthecase-by-casedataanalysissummarizedinTable5, findings show that despite family follow-up and special-ist medical treatment, the cognitive performance of most oftheparticipantswaspoorinallthe functionsevaluated, emphasizing the role ofSCA as a potential risk factor for neurocognitive and psychosocial development. Nine cases presentedsignificant cognitivedeficits,eventhose patients whohadnothadastrokeandthosewithnoabnormalityin maximummeanbloodflowvelocity(MFV).Thisfinding sug-geststhatinadditiontotheriskfactorsmentionedhere,other riskfactorsinherenttothediseaseitselfsuchasanemiaper seandrecurrentpainmaycontributetopoorcognitive perfor-mance.Inaddition,itraisesthehypothesisoftheexistence ofundiagnosedsilentinfarctsonlyfoundfollowing neuropsy-chologicalevaluations.13,27,28
Table5–Summaryoftheresultswithrespecttotheintellectual,cognitiveandbehavioralperformanceoftheindividuals withsicklecellanemiaandtheirclinicaldata.
Participant
Characteristics/functions 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 F
NumberofepisodesofCVA 1 1 2 1 5 2 6/15
BrainhemisphereaffectedbyCVA R R L L L R R=3/15;L=3/15
Silentinfarct x 1/15
ChangedDopplerfindings x x x x x 5/15
Learningdifficulty x x x x x x x x x x 10/15
IQ x x x x 4/15
Attention/executivefunctioning x x x x x x x x x x x x x 13/15
Memory x x x x x x x x x x x x x x x 15/15
Language x x x x x x x x x x x x x x x 15/15
Visuospatialprocessing x x x x x x x x x x x x x 13/15
Sensorimotor x x NP x x NP NP NP x x x x x x 10/11
Somaticcomplaints x x x x x 5/15
Alienated/depressed x x 2/15
Anxiety/depression x x 2/15
Socialproblems x 1/15
Attentionproblems x 1/15
Atypicalbehavior x x 2/15
Aggressivebehavior x 1/15
Depressivedisorder x x x x x 5/15
Somaticdisorder x x x 3/15
Anxietydisorder x x 2/15
Oppositionaldefiantdisorder x 1/15
Conductdisorder 1/15
Post-traumaticstressdisorder x x x 3/15
Obsessive–compulsivedisorder x 1/15
NP:notperformed;f:frequency;R:right;L:left;x:abnormal.
National Health System (SUS), and their high cost in the private healthsystem. Thus, importantneuroimaging data wasnotaddedtotheneuropsychologicalevaluationsofthe participantsinthisstudy.Thisfactmightexplainthelower prevalenceofsilentischemicstrokesinthisstudywhen com-pared with the literature.3 Silent brain infarcts may have
been underdiagnosed due to the impossibility of carrying out MRI and MRA brain scans in this sample. However, the low performance in neuropsychological assessment of patients with no apparent neurological impairment draws attentiontothepossibilityofundiagnosedbrainchangesdue totheinaccessibilityofadvancedexamsinthehealthsystem andreinforcestheimportanceoftheavailabilityofperiodic imaging.
One of the limitations of the present study was the small,heterogeneoussample,whichwastheresultofmissed appointmentsanddiscontinuationsduetohospitalizations, aswellasotherdifficultiescitedbythefamilies.Thismadeit impossibletorandomizethesample,makinganyinferences orgeneralizationoftheresultsimpossible.
Gaps remain in the information available on the cog-nition of children with SCD. Studies continue on the risk factors,predictive factors and on patients’ neuropsycholo-gical profile in an attempt to establish consensuses. New fields ofresearch maybeopened usingneuropsychological investigation,including the possibility ofdesigningstudies toanalyzewhetherthedeclineincognitiveand/oracademic performancemaybeusefulasamarkerofoutcome during treatment.
Conclusion
Thefindingsofthepresentstudyshowthatindividualswith SCDandahistoryofstrokehavepoorerIQscoresand abnor-malities in attention and executive functioning, language, verbalandvisualmemory,visuospatialprocessingand sensor-imotorabilityirrespectiveofwhetherornottheyhadhada confirmedstroke.
This study provides considerable food for thought on the cognition ofchildrenwith SCD, since findings showed significant cognitive impairment inSCA irrespective ofthe presence of known risk factors, emphasizing the need to investigate patients with SCD with no apparent risk fac-tors.Fewstudieshavetargetedtheemotionalandpsychiatric aspects of individuals with SCD and further research is needed on these issues in order to guarantee treatment forpatients,reducingpossibledamagetotheirpsychosocial development.
Periodicneuropsychologicalandbehavioralevaluationsof children and young adults with SCA are useful measures to reduce long-term biopsychosocial repercussions, and to stimulateparticipationinrehabilitationandeducational pro-grams,thusimprovingpatients’psychosocialdevelopment.
Conflicts
of
interest
revbrashematolhemoter.2 0 1 7;39(1):32–39
39
Acknowledgements
Theauthorsdedicatethispapertothepatientsandtheir fam-ilies.
r
e
f
e
r
e
n
c
e
s
1. SillaLM.Doenc¸afalciforme:umgraveedesconhecido problemadesaúdepúblicanoBrasil.JPediatr(RioJ). 1999;75(3):145–6.
2. Brasil.MinistériodaSaúdePortarian◦55,de29dejaneirode
2010.ProtocoloClínicoeDiretrizesTerapêuticas–Doenc¸a Falciforme.Brasília,DF:SenadoFederal;2010.
3. Ohene-FrempongK,WeinerSJ,SleeperLA,MillerST,Embury S,MoohrJW,etal.Cerebrovascularaccidentsinsicklecell disease:ratesandriskfactors.Blood.1998;91(1):288–94.
4. AnguloIL.Acidentevascularcerebraleoutrascomplicac¸ões dosistemanervosocentralnasdoenc¸asfalciformes.RevBras HematolHemoter.2007;29(3):262–7.
5. CritérioBrasildeClassificac¸ãosocioeconômicadesenvolvido pelaABA–Associac¸ãoBrasileiradeanuncianteseABIPEME– Associac¸ãoBrasileiradeInstitutosdePesquisasdeMercado; 2012.
6. WechslerD.WISC-III:Wechslerintelligencescaleforchildren: Manual.PsychologicalCorporation;1991,294pp.
7. MelloCB,ArgolloN,ShayerBP,AbreuN,GodinhoK,DuránP, etal.VersãoabreviadadoWISC-III:correlac¸ãoentreQI estimadoeQItotalemcrianc¸asbrasileiras.Psicologia:Teoria ePesquisa.2011;27(2):149–55.
8. KorkmanM,KempS,KirkU.NEPSY-II.SanAntonio,TX: Pearson;2007.
9. BordinI,MariJ,CaeiroM.Validac¸ãodaversãobrasileirado ChildBehaviorChecklist(CBCL),Inventariode
ComportamentosdaInfanciaeAdolescencia.RevABP-APAL. 1995;2(17):55–66.
10.Canc¸adoRD,LoboC,AnguloIL,AraújoPIC,JesusJA.Protocolo clínicoediretrizesterapêuticasparausodehidroxiureiana doenc¸afalciforme.RevBrasHematolHemoter.
2009;31(5):361–6.
11.WangWC.Centralnervoussystemcomplicationsofsickle celldiseaseinchildren:anoverview.ChildNeuropsychol. 2007;13(2):103–19.
12.ShayerB,CarvalhoC,MotaM,AbreuN,BuenoOF,ArgolloN. Desempenhodeescolaresematenc¸ãoefunc¸õesexecutivas noNepsyeinteligência.RevistaPsicologia-TeoriaePrática. 2015;17(1):120–35.
13.BerkelhammerLD,WilliamsonAL,SanfordSD,DirksenCL, SharpWG,MarguliesAS,etal.Neurocognitivesequelaeof pediatricsicklecelldisease:areviewoftheliterature.Child Neuropsychol.2007;13(2):120–31.
14.AlvesAL.Estudodamortalidadeporanemiafalciforme.Inf epidemiolSUS.1996;5(4):45–53.
15.DiamondA.Executivefunctions.AnnuRevPsychol. 2013;64:135–68.
16.HijmansCT,GrootenhuisMA,OosterlaanJ,HeijboerH,Peters M,FijnvandraatK.Neurocognitivedeficitsinchildrenwith sicklecelldiseaseareassociatedwiththeseverityofanemia. PediatrBloodCancer.2011;57(2):297–302.
17.CapovillaAG,CapovillaFC,SoaresJV.Consciênciasintática noensinofundamental:correlac¸õescomconsciência fonológica,vocabulário,leituraeescrita.Psico-USF. 2004;9:39–47.
18.SanchezCE,SchatzJ,RobertsCW.Cerebralbloodflowvelocity andlanguagefunctioninginpediatricsicklecelldisease.JInt NeuropsycholSoc.2010;16(2):326–34.
19.KralMC,BrownRT,HyndGW.Neuropsychologicalaspectsof pediatricsicklecelldisease.NeuropsycholRev.
2001;11(4):179–96.
20.BakriMH,IsmailEA,ElsedfyGO,AmrMA,IbrahimA. Behavioralimpactofsicklecelldiseaseinyoung childrenwithrepeatedhospitalization.SaudiJAnaesth. 2014;8(4):504–9.
21.CrosbyLE,JoffeNE,ReynoldsN,PeughJL,ManegoldE,PaiAL. Psychometricpropertiesofthepsychosocialassessment tool-generalinadolescentsandyoungadultswithsicklecell disease.JPediatrPsychol.2016;41(4):397–405.
22.SilS,CohenLL,DampierC.Psychosocialandfunctional outcomesinyouthwithchronicsicklecellpain.ClinJPain. 2016;32(6):527–33.
23.AmericanPsychiatricAssociation.Diagnosticandstatistical manualofmentaldisorders:DSM-IV.4thed.Washington,DC: AmericanPsychiatricAssociation;1994,866pp.
24.SehloMG,KamfarHZ.Depressionandqualityoflifein childrenwithsicklecelldisease:theeffectofsocialsupport. BMCPsychiatry.2015;15:78.
25.KatzmanMA,BleauP,BlierP,ChokkaP,KjernistedK,Van AmeringenM,etal.Canadianclinicalpracticeguidelinesfor themanagementofanxiety,posttraumaticstressand obsessive–compulsivedisorders.BMCPsychiatry.2014;14 Suppl.1:S1.
26.EkinciO,CelikT,UnalS,OzerC.Psychiatricproblemsin childrenandadolescentswithsicklecelldisease,basedon parentandteacherreports.TurkJHaematol.
2012;29(3):259–64.
27.AbreuKdC[dissertac¸ão]Perfilneuropsicológicoe
comportamentaldecrianc¸ascomdoenc¸afalciforme.Ribeirão Preto:UniversidadedeSãoPaulo,FaculdadedeFilosofia, CiênciaeLetras;2013.Availablefrom:http://www.teses.usp. br/teses/disponiveis/59/59137/tde-29072013-180153/pt-br.php
[cited2016-08-04].