www.revportcardiol.org
Revista
Portuguesa
de
Cardiologia
Portuguese
Journal
of
Cardiology
ORIGINAL
ARTICLE
Combined
MitraClip
implantation
and
left
atrial
appendage
occlusion
using
the
Watchman
device:
A
case
series
from
a
referral
center
Ana
Rita
G.
Francisco
a,∗,
Eduardo
Infante
de
Oliveira
a,
Miguel
Nobre
Menezes
a,
Pedro
Carrilho
Ferreira
a,
Pedro
Canas
da
Silva
a,
Ângelo
Nobre
b,
Fausto
J.
Pinto
aaCardiologyDepartment,SantaMariaUniversityHospital,CHLN,CAML,CCUL,FacultyofMedicine,UniversityofLisbon,Lisbon,
Portugal
bCardiothoracicSurgeryDepartment,SantaMariaUniversityHospital,CHLN,CAML,CCUL,FacultyofMedicine,Universityof
Lisbon,Portugal
Received2August2016;accepted11November2016 Availableonline30June2017
KEYWORDS Mitralregurgitation; MitraClip;
Leftatrialappendage occlusion;
Watchman
Abstract
Introduction:Patientsreferredfor percutaneoustranscathetermitralvalverepairusing the MitraClip® systemfrequentlyhaveatrialfibrillation,whichimposesadditionalchallengesdue totheneedfororalanticoagulation.Leftatrialappendageocclusioniscurrentlyregardedasa non-inferioralternativetoanticoagulationinpatientswithnon-valvularatrialfibrillationand bothhighthromboembolicandbleedingrisk.ConsideringthatbothMitraClipimplantationand leftatrialappendageocclusionarepercutaneoustechniquesthatrequiretransseptalpuncture, itistechnicallyattractivetoconsidertheirconcomitantuse.
Objectives:WeaimtoevaluatethefeasibilityofacombinedapproachwithMitraClip implan-tationandleftatrialappendageocclusioninasingleprocedure.
Methods:Wereportthefirstcaseseriesregardingthisissue,discussingthespecificadvantages, pitfallsandtechnicalaspectsofcombiningthesetwoprocedures.
Results:FivepatientsunderwentleftatrialappendageocclusionwiththeWatchman® device followedbyMitraClipimplantationinthesameprocedure.Allpatientsexperiencedsignificant reductioninmitralvalveregurgitationofatleasttwogrades,optimaloccluderposition,no associatedcomplicationsandsignificantclinicalimprovementassessedbyNYHAfunctionalclass (reductionofatleastonefunctionalclass,withfourpatientsinclassIatone-monthfollow-up).
∗Correspondingauthor.
E-mailaddress:ana.r.francisco@gmail.com(A.R.G.Francisco).
http://dx.doi.org/10.1016/j.repc.2016.11.012
0870-2551/©2017SociedadePortuguesadeCardiologia.PublishedbyElsevierEspa˜na,S.L.U.Allrightsreserved.
Conclusion:In selectedpatientsrejectedforsurgicalmitralvalverepair,withatrial fibrilla-tionandincreasedriskofbleedingandembolicevents,acombinedapproachwithMitraClip implantationandleft atrialappendageocclusioninasingleprocedureisfeasible, safe and effective.
©2017SociedadePortuguesade Cardiologia.Publishedby ElsevierEspa˜na,S.L.U.Allrights reserved.
PALAVRAS-CHAVE Regurgitac¸ãomitral;
MitraClip;
Encerramentodo apêndiceauricular esquerdo;
Watchman
Implantac¸ãosimultâneadeMitraClipeencerramentodoapêndiceauricular esquerdocomWatchman:aexperiênciadeumcentrodereferência
Resumo
Introduc¸ão: Osdoentesreferenciadosparareparac¸ãomitralpercutânea,usandoosistema Mitr-aClip,têmfrequentementefibrilhac¸ãoauricular,comdesafiosadicionaisdevidoànecessidade deanticoagulac¸ão.Oencerramentopercutâneodoapêndiceauricularesquerdoé,atualmente, umaalternativanãoinferioràanticoagulac¸ãoemdoentescomfibrilhac¸ãoauricularnãovalvular, comelevadoriscoquertromboembólicoquerhemorrágico.Considerandoqueestasduas técni-cas(MitraClipeencerramentopercutâneodoapêndiceauricularesquerdo)requerempunc¸ão transeptal,étecnicamenteatrativoconsideraroseuusoconcomitante.
Objectivos: Avaliaraexequibilidadedeefectuarnomesmoprocedimentoimplantac¸ãode Mitr-aClipeencerramentopercutâneodoapêndiceauricularesquerdo.
Métodos: Descric¸ãodaprimeirasériedecasossobreaaplicac¸ãodestasduastécnicasnumsó procedimento,comanálisedasvantagens,dificuldadeseaspetostécnicos.
Resultados: Cincodoentesforamsubmetidosaencerramentopercutâneodoapêndiceauricular esquerdocomdispositivoWatchman,seguidodeimplantac¸ãodeMitraClipnomesmo proced-imento.Emtodososdoentesverificou-sereduc¸ãosignificativadograudaregurgitac¸ãomitral empelomenosdoisgraus,posic¸ãoótimadosistemadeoclusãodoapêndice,semcomplicac¸ões associadasecommelhoriaclínicasignificativaavaliadapelaclassefuncionaldeNYHA(reduc¸ão de pelomenos umaclassefuncional, comquatro doentes em classefuncionalInofinaldo primeiromêsdeseguimento).
Conclusão:Em doentesselecionados,recusadosparareparac¸ãocirúrgicadavalvularmitral, comfibrilhac¸ãoauriculareriscoelevadodeeventoshemorrágicoseembólicos,umaabordagem combinadacomimplantac¸ãodeMitraClipeencerramentopercutâneodoapêndiceauricular esquerdonumsóprocedimentoéviável,seguraeeficaz.
©2017SociedadePortuguesadeCardiologia.PublicadoporElsevierEspa˜na,S.L.U.Todosos direitosreservados.
ACC AmericanCollegeofCardiology AF atrialfibrillation
AHA AmericanHeartAssociation ESC EuropeanSocietyofCardiology
KDOQI KidneyDiseaseOutcomesQualityInitiative LAA leftatrialappendage
LSPV leftsuperiorpulmonaryvein LVEF leftventricularejectionfraction MR mitralregurgitation
MVR mitralvalverepair
NYHA NewYorkHeartAssociation OAC oralanticoagulation
TEE transesophagealechocardiography
Introduction
Percutaneoustranscathetermitralvalverepair(MVR)using the MitraClip® system is an emerging approach to treat selectedcasesofdegenerativeandfunctionalmitral regur-gitation(MR).Itssafetyandefficacyinhighrisk-patientshas been consistentlydemonstrated,bothinclinicaltrialsand in real-world settings.1---3 The procedure has been
recom-mendedbytheEuropeanSocietyofCardiology(ESC)andthe European Association for Cardio-Thoracic Surgery (EACTS) since 2012 for patients with both primary and secondary severeMR athighsurgicalrisk(classIIb,levelofevidence C).4FollowingapprovalbytheUSFoodandDrug
Administra-tion(FDA)in2013,theMitraClipwasalsorecommendedin the 2014 AmericanCollege of Cardiology (ACC)/American Heart Association (AHA) guidelines for degenerative MR (classIIb,levelofevidenceB).5
Patientsreferred for MitraClip implantation frequently have concomitant atrial fibrillation (AF). These patients present highsurgicalriskduetotheassociationofvarious comorbidities, as well asa frailty profile that represents increased risk of thromboembolic and bleeding events. Thesecharacteristicsposeadditionalchallengesduetothe needforchronicoralanticoagulation(OAC).
Left atrial appendage (LAA) occlusion, either percuta-neouslyorsurgically,iscurrentlyregardedasanalternative to OACin patients withnon-valvular AF.6 Similarly tothe
MitraClip, this wasasa resultof twotrials7,8 and several
registries.9---12 The ESCguidelinesissued aclassIIb
recom-mendationregardingthisprocedure,13 anditobtainedFDA
approvalin2015.
ThefrequentassociationofMRandAFhasoftenled sur-geonstoexcisetheLAAduringheartsurgery.14Considering
thatbothMitraClipimplantationandLAAocclusionare per-cutaneoustechniquesthatrequiretransseptalpunctureand accesstotheleftatrium,itistechnicallyattractiveto con-sideremulatingthesurgicalapproachpercutaneously.With theexceptionoftwosinglecasereports,therearenoother publisheddataregardingthefeasibility,safetyandefficacy ofacombinedprocedure.15,16 Inthisarticle,wereportthe
first case series regarding this issue, discussing the spe-cificadvantages,pitfallsandtechnicalaspectsofcombining thesetwoprocedures.
Methods
Weperformedaretrospectivesingle-centerstudyof consec-utivepatientswithsevereMRandAFundergoingMitraClip deviceimplantationplusLAAocclusionwiththeWatchman® device.Baselineclinical,echocardiographic,hemodynamic andproceduraldatawererecordedretrospectivelythrough reviewsofhospitalrecords.Echocardiographic assessment was repeated after the procedure, on the same day and atone-monthfollow-up.Acuteandone-monthresultswere analyzed.
Results
Fivepatients withsevere MR andAF rejectedfor surgical MVR were referred for percutaneous MVR. After assess-mentbytheinterventionalcardiologyteam,theywerealso selectedforLAAocclusiononthebasisofhigh thromboem-bolicrisk combinedwithhighbleedingrisk.Table1shows thebaselinepatientcharacteristics.
Patient1 wasa 57-year-oldmanwithalcoholicdilated cardiomyopathy, severely compromised left ventricular ejectionfraction(LVEF)andseverefunctionalMR.Cardiac resynchronization therapy and atrioventricularnode abla-tion had already been performed. Concomitantly he had permanent AF,liver cirrhosis (Child-Pugh classB)without esophageal varices (with continued alcohol abuse), pre-vious ischemic stroke under OAC, chronic renal disease (KidneyDisease OutcomesQualityInitiative [KDOQI]stage 3b),pulmonaryandsystemichypertension,dyslipidemiaand previousresectionofcoloncancer.
Patient2 wasa 72-year-oldmanwithischemic dilated cardiomyopathyandmoderatelydepressedLVEF,witha car-diacdefibrillatorsystem implantedforprimaryprevention
andseverefunctionalMRwithepisodesofflashedema.He hadpreviouslyundergonetriplecoronaryarterybypassgraft surgery.OthercomorbiditieswerepermanentAF,pulmonary andsystemichypertension,dyslipidemia,chronickidney dis-ease(KDOQIstage3a),chronicirondeficiencyanemiawith intestinalangiodysplasiaandprevioussmoking.
Patient 3 wasa 76-year-old woman withnon-ischemic dilatedcardiomyopathy,severelydepressedLVEFandsevere functional MR,who hadalready undergone cardiac resyn-chronizationtherapy.ShealsohadpermanentAFwithlabile INR under warfarin (TTR <60%), pulmonary and systemic hypertension,dyslipidemiaandchronickidney dysfunction (KDOQI stage 3a), and chronic use of non-steroidal anti-inflammatorydrugsduetoosteoarticulardisease.
Patient 4 was a 78-year-old man with non-ischemic dilatedcardiomyopathy,severelydepressedLVEFandsevere functionalMR.Concomitantcomorbiditieswerepermanent AFwithlabileINRunderwarfarin(TTR<60%),pulmonaryand systemichypertension, chronickidney dysfunction (KDOQI stage3b)anddyslipidemia.
Patient 5was a71-year-old manwithischemic dilated cardiomyopathy, severely depressed LVEF and severe functional MR. Concomitant comorbidities were previous ischemic stroke, permanent AF, systemic hypertension, chronic kidneydysfunction (KDOQIstage3a) and dyslipid-emia.
Overall,thepatientshadsignificantcomorbidities,LVEF <35% and severe functional MR, and were severely symp-tomatic(NYHAclassIIIorIV).Theyhadahighriskofboth thromboembolicandbleedingevents,withmean CHA2DS2-VAScscoreof4.5±0.6andmeanHAS-BLEDscoreof3.5±0.6. ThemeanannualstokeriskpredictedbyCHA2DS2-VAScwas 6.0±1.4%,withahigherannualriskofmajorbleedingevents predictedbyHAS-BLED(6.2±2.9%).
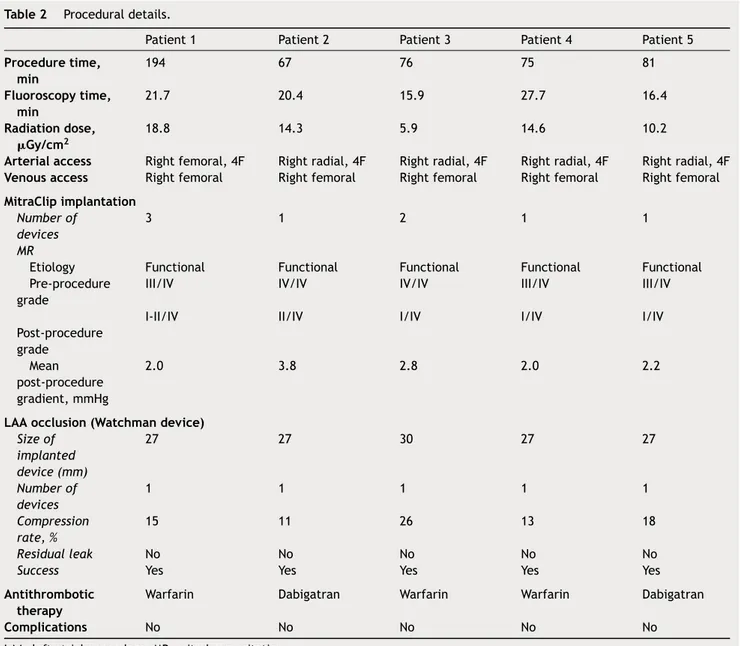
Proceduraldetails
The procedure was performed under general anes-thesia in the cardiac catheterization laboratory, with three-dimensionaltransesophagealechocardiography(TEE) guidance for MitraClip deployment and fluoroscopic guid-ance. In all cases LAA occlusion was performed first. ProceduraldetailsaredisplayedinTable2.
Vascularaccess
By protocol, right radial arterial access (4F sheath) was establishedforinvasiveblood pressuremonitoring, except foronecaseinwhichaccesswasviatherightfemoralartery (4Fsheath)duetoinabilitytoobtainradialaccess.Venous accesswasviatherightfemoralvein(6Fsheath)inallcases. Afterestablishmentofarterialandvenousaccess,an intra-venousunfractionatedheparinboluswasadministered(50% ofthetotalrecommendeddose---100U/kg).
Transseptalpuncture
Transseptal puncture, guided by TEE, was performed through an 8F SL1 sheath (St. Jude Medical) with a BRK transseptal needle (St. Jude Medical). The puncture was
Table1 Baselinepatientcharacteristics.
Patient1 Patient2 Patient3 Patient4 Patient5
Age,years 57 72 76 78 71
Gender Male Male Female Female Male
AFclassification Permanent Permanent Permanent Permanent Permanent
LVEF,% 24 35 20 30 23
NYHAclass III/IV III/IV III/IV II/IV III/IV
Cardiomyopathyetiology Alcoholic
dilated Ischemic dilated Non-ischemic dilated Non-ischemic dilated Ischemic dilated Comorbidities
Hypertension Yes Yes Yes Yes Yes
Pulmonaryhypertension Yes Yes Yes Yes Yes
Diabetes No Yes No No No
Previousstroke Yes No No No Yes
Renaldisease,KDOQIstage 3b 3a 3a 3b 3a
Previousopenheartsurgery No Yes No No Yes
Chronicliverdisease Yes No No No No
Chronicanemia No Yes No No No
Malignancy Yes No No No No
CHADS2score 4 3 3 3 4
Annualstrokerisk,%15 8.5 5.9 5.9 5.9 8.5
CHA2DS2-VAScscore 4 5 5 4 6
Annualstrokerisk,%17 4 6.7 6.7 4 9.7
PreviousemboliceventunderOAC Yes No No No Yes
HAS-BLEDscore 4 3 3 3 3
Annualbleedingrisk,%18 8.9 5.8 5.8 5.8 5.8
Age>65years No Yes Yes Yes Yes
Previousstroke Yes No No No Yes
Priorbleedingorpredisposition No Yes No No No
Renaldysfunction(Cr>2.36mg/dl) Yes No No Yes No
Liverdysfunction(cirrhosis) Yes No No No No
LabileINR(TTR<60%) No No Yes Yes No
Drugspredisposingtobleeding Yes No No No Yes
Alcoholabuse Yes No No No No
PreviousbleedingeventunderOAC No No No No No
AF:atrialfibrillation;Cr:serumcreatinine;INR:internationalnormalizedratio;KDOQI:KidneyDiseaseOutcomesQualityInitiative;LVEF: leftventricularejectionfraction;NYHA:NewYorkHeartAssociation;OAC:oralanticoagulation;TTR:timeintherapeuticrange.
performed aiming for the optimal position for MitraClip implantation.
The remainingdose ofintravenous unfractionated hep-arinwasthenadministeredandanactivatedclotting time of250-300swasmaintainedthroughouttheprocedure.
Once access to the left atrium was achieved, an Amplatzer stiff wire was advanced into the left superior pulmonaryvein(LSPV).
Leftatrialappendageocclusion
For LAA occlusion, a Watchman 14F double curve access sheathwasusedfollowedby angiographyof theLAAwith apigtailcatheter.TheLAAclosuredevicesizewasselected afterassessing the following LAAfeatures byTEE: ostium sizeandshape,andnumberoflobesandlengthinatleast fourTEEviews(0◦,45◦,90◦and135◦).Thesemeasurements werecomplementedbyangiographyoftheLAA.Thedevice
was implanted under angiographicand echocardiographic (TEE)guidanceusingthestandardtechnique.Criteriaof suc-cesswereachievedinallfivepatients.Onlyonedeviceper patient was used,with appropriatestability, compression andsealing.Noresidualleaksorimmediatecomplications werenoted.
MitraClipprocedure
TheWatchman14Fdoublecurvesheathwasexchangedfor a24FMitraClipGuideCatheter,overanAmplatzersupport wirepositionedintheLSPV.Astandardtechniquewasused, underangiographicandTEEguidance.
TheprocedurestepsaresummarizedinFigure1. Threepatients received only oneclip, while the other tworequiredtwoandthreeclips,respectively.Allpatients showedsignificantimprovementinMR,threeofthemwith residual grade I/IV regurgitation and the other two with
Table2 Proceduraldetails.
Patient1 Patient2 Patient3 Patient4 Patient5
Proceduretime, min 194 67 76 75 81 Fluoroscopytime, min 21.7 20.4 15.9 27.7 16.4 Radiationdose, Gy/cm2 18.8 14.3 5.9 14.6 10.2
Arterialaccess Rightfemoral,4F Rightradial,4F Rightradial,4F Rightradial,4F Rightradial,4F Venousaccess Rightfemoral Rightfemoral Rightfemoral Rightfemoral Rightfemoral MitraClipimplantation
Numberof
devices
3 1 2 1 1
MR
Etiology Functional Functional Functional Functional Functional
Pre-procedure grade
III/IV IV/IV IV/IV III/IV III/IV
Post-procedure grade
I-II/IV II/IV I/IV I/IV I/IV
Mean post-procedure gradient,mmHg
2.0 3.8 2.8 2.0 2.2
LAAocclusion(Watchmandevice)
Sizeof implanted device(mm) 27 27 30 27 27 Numberof devices 1 1 1 1 1 Compression rate,% 15 11 26 13 18 Residualleak No No No No No
Success Yes Yes Yes Yes Yes
Antithrombotic therapy
Warfarin Dabigatran Warfarin Warfarin Dabigatran
Complications No No No No No
LAA:leftatrialappendage;MR:mitralregurgitation.
gradeII/IV.Thisgoalwasachievedwithoutsignificant steno-sis,meanfinaltransvalvulargradientbeing2.7±0.9mmHg. Nocomplicationsoccurred.Ofnote,therewasno interfer-ence of theMitraClip delivery system withthe implanted Watchmandevice.
Hemostasis
In allpatients,thePerclose Proglidesuture-mediated clo-sure system (Abbott Vascular) was used for hemostasis of the femoral vein access site (two systems were pre-deployed, before insertion of the transseptal puncture sheath). Hemostasis of the arterial access site was per-formedbymanualcompression.
Follow-up
All patients were discharged 24-36 hours after the pro-cedure. They started anticoagulation with warfarin or
non-vitaminKantagonistoralanticoagulants,accordingto thechoiceoftheattendingcardiologist,withlater transi-tiontoantiplatelettherapy afterTEEfollow-up(PROTECT AFstrategy).10
Patientsunderwentclinicalandechocardiographic(TEE) follow-up one month after the procedure. Results were excellentinallpatients,withclinicalsymptomatic improve-ment(NYHAclassI-II/IV),significantMRreduction(without significant stenosis), optimaloccluder position,no throm-busandnoclinicalevents. The interatrialseptum showed asmall,nothemodynamicallyrelevant,left-to-rightshunt. DetailsareshowninTable3.Inameanclinicalfollow-upof 243±70.7days, the symptomatic improvement was main-tained,withoutadverseevents.
Discussion
and
limitations
In thiscase series, we demonstrate thesafety and effec-tivenessofcombiningpercutaneousMVRusingtheMitraClip
Figure1 Proceduresteps:(1)transseptalpunctureguidedbytransesophagealechocardiography(TEE)(1a)andfluoroscopy(1b); (2)theWatchman14FdoublecurvesheathisadvancedoveranAmplatzerstiffwirepositionedintheleftsuperiorpulmonaryvein; (3)theleftatrialappendageismeasuredbyangiography(3a)andTEE(3b);(4)theWatchmanisimplantedguidedbyfluoroscopy (4a)andgoodappositionandabsenceofleaksandcomplicationsareconfirmedbyTEE(4b);(5)theWatchman14Fdoublecurve sheathisexchangedfora24FMitraClipguidecatheter,overanAmplatzersupportwire;(6)theclipdeliverysystemisdirected tothemidscallopsoftheanteriorandposteriormitralvalveleaflets,andguidedbythree-dimensionalTEE,theclipispositioned abovetheoriginofthemitralregurgitation(MR)jet;(7)leafletinsertion,MRreduction,andabsenceofsignificantmitralvalve stenosisareconfirmedbyTEE(7aand7b);(8)additionalclipsaredeployedifnecessary.
Table3 Resultsatone-monthfollow-up.
Patient1 Patient2 Patient3 Patient4 Patient5
NYHAclass I/IV II/IV I/IV I/IV I/IV
Embolicevents No No No No No
Bleedingevents No No No No No
Mitralvalve
MRgrade I/IV II/IV I/IV I/IV II/IV
Meangradient,mmHg 1.0 4.6 1.7 1.6 2.1
LAAocclusion---Watchmandevice
Leaks No No No No No
Thrombus No No No No No
LAA:leftatrialappendage;MR:mitralregurgitation;NYHA:NewYorkHeartAssociation.
device and LAA occlusion with the Watchman device. It is shouldbe noted thatthis approachproduced excellent immediateand short-termresults despite the severe car-diac and non-cardiac comorbidities of this cohort. These
resultsareinagreementwiththefewpublishedsinglecase reports.15,16
SurgeonshavelongperformedthecombinationofMVR, mazeoperationandLAAexclusioninpatientswithMRand
AF,andLAAocclusionisrecommendedinpatientswithAF whoundergoheartsurgery.13TheLAAiseasilyaccessibleto
thesurgeon,theocclusionprocedureisreasonablysafeand itisbelievedtodecreaseembolicriskeveninthepresence of valvularAF.However,variability in surgical approaches meansthatremnantsoftheLAAareoftenleftbehind,which mightexplainthepoorlong-termresultsofthisapproach.14
DuringMitraClipimplantation,theLAAisalsoeasily acces-sible to the interventional cardiologist and the etiology of AF is non-rheumatic. In summary, the patient is anes-thetized,thetransseptalpuncturehasbeenperformedand theLAAis easily accessibletocathetertreatment. Percu-taneousLAAocclusionhasasolidscientificbasisandgood long-termresultsregardingbothsafetyandefficacy. There-fore, combining MitraClip implantation and percutaneous LAAocclusionseemsatleastasappealingascombining sur-gicalMVRandLAAexcision.
Fromaclinicalstandpoint,patientsreferredforMitraClip implantation frequentlypresent a profile suitablefor LAA occlusion(AF withhighthromboembolicand bleedingrisk duetothecomorbiditiesthatexcludedthemfromsurgical MVR).Exposingthesepatients totwoseparateprocedures wouldpresent severaldisadvantages.Itis wellrecognized that transseptal puncture carries a small but important risk of significant complications.19 Furthermore, the use
of large sheaths in two different locations may increase the risk of significant residual septal shunting. A single procedure involves a single transseptalpuncture, thereby minimizing bothrisks.Also,both proceduresrequirelarge sheaths placed in femoral veins. Combining the two pro-cedures streamlines vascular access and reduces the risk of complications.Finally, overall fluoroscopytimemaybe reducedcomparedtotwoindividualprocedures,duetothe commoninitialpathwayofbothtechniques.
Our results seem to confirm these advantages, as there were nocomplications regarding any of the above-mentioned issuesandtotalfluoroscopytimeandradiation dosageswereacceptable.
Ontheotherhand,theoreticallytherearepotential dis-advantages. First, the high transseptal puncture for the MitraClip is less well suited for LAA occlusion. Second, overall procedure time maybe prolonged, withan added risk ofvolume overloador hemodynamic instability, espe-cially considering theseverely depressedsystolicfunction of many ofthese patients.We experienced nodifficulties witheitherissue, andoverallprocedure timewas accept-able(103.0±60.8min). Nonetheless,acknowledgingthese pitfallsisessentialforavoidingcomplications.
Anotheraspect ofthe technique thatis the subjectof debate is the appropriatesequence of procedures in this combined approach. Our team decided to perform LAA occlusionbeforeMitraClipimplantationbasedonthe ratio-naleofusingsheathswithsequentiallyincreasingdiameters. We consideredthat thisstrategy wouldreduce therisk of bleedingattheaccesssiteandwouldimposelesstraumaon theatrialseptum.Reversingtheorderoftheproceduresmay havetheadvantageofeliminatingtheriskofinterferenceof theMitraClipdeliverysystemwiththeimplantedWatchman device.However,wefoundthatthepresenceofthe Watch-mandeviceservedasausefulanatomicalreferenceduring manipulation ofthe MitraClipdelivery system. Performing theMitraClipimplantationfirstwouldrequireanexchange
for a shorter sheath compatible with the 14F Watchman delivery sheath, to avoid massive bleeding at the access site.Alternatively,the24Fcouldbeexchangeddirectlyfor the 14F usingthe pre-deployed Perclose Proglide systems toclosetheorificearoundthesheath.This approachmay compromisefinalaccessocclusionsuccess.
Conclusion
InselectedpatientsathighriskforMRsurgerywho concomi-tantlypresentAFandanincreasedriskofbothbleedingand embolic events, a combined approachwith MitraClip and WatchmanOccluder implantation in a single procedure is feasible,safeandeffective,inboth immediateand short-termfollow-up,whenundertakenbyanexperiencedteam.
Ethical
disclosures
Protection of human and animal subjects.The authors declarethatnoexperimentswereperformedonhumansor animalsforthisstudy.
Confidentialityofdata.Theauthorsdeclarethattheyhave followedtheprotocolsoftheirworkcenteronthe publica-tionofpatientdata.
Righttoprivacyandinformed consent.Theauthorshave obtained thewritten informedconsentof the patients or subjectsmentionedinthearticle.Thecorrespondingauthor isinpossessionofthisdocument.
Funding
Nospecificfundinggrantswereusedregardingthisstudy.
Conflicts
of
interest
AnaRitaG.Franciscohasnoconflictsofinteresttodeclare; Eduardo Infante deOliveira has receivedspeaker/proctor honoraria and research grants from Boston Scientific and speaker honoraria from Abbott Vascular; Miguel Nobre Menezeshasnoconflictsofinteresttodeclare;Pedro Car-rilhoFerreirahasreceivedspeakerhonorariaandresearch grants from Boston Scientific; Pedro Canas da Silva has receivedspeakerhonorariaandresearchgrantsfromBoston ScientificandAbbottVascular.
References
1.MauriL,GargP,MassaroJM,etal.TheEVERESTIItrial:design andrationaleforarandomizedstudyoftheE-ValveMitraClip systemcomparedwithmitralvalvesurgeryformitral regurgi-tation.AmHeartJ.2010;160:23---9.
2.Mauri L,Foster E,GlowerDD, etal.4-Yearresultsofa ran-domizedcontrolledtrialofpercutaneousrepairversussurgery formitralregurgitationcomparedwithmitralvalvesurgeryfor mitralregurgitation.JAmCollCardiol.2013;62:317---28.
3.MaisanoF,FranzenO,BaldusS,etal.Percutaneousmitralvalve interventionsintherealworld:earlyand1-yearresultsfrom the ACCESS-EU, a prospective, multicenter, nonrandomized
post-approval studyoftheMitraCliptherapyinEurope.JAm CollCardiol.2013;62:1052---61.
4.Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Joint Task Forceon the Managementof ValvularHeart Disease of the European Society of Cardiology (ESC); European Asso-ciation for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2012;33:2451---96.
5.NishimuraRA,OttoCM,BonowRO,etal.2014AHA/ACC Guide-linefortheManagementofPatientsWithValvularHeartDisease: ExecutiveSummary:areportoftheAmericanCollegeof Car-diology/American Heart Association Task Force on Practice Guidelines.Circulation.2014;129:2440---92.
6.Tzikas A, Sievert H, Holmes DR Jr. Percutaneous left atrial appendage occlusion in 2016. EuroIntervention. 2016;11:e1576---8.
7.HolmesDR,ReddyVY,TuriZG,etal.,PROTECTAF Investiga-tors.Percutaneousclosureoftheleftatrialappendageversus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferioritytrial. Lancet. 2009;374:534---42.
8.Holmes DR Jr, Kar S, Price MJ, et al. Prospective ran-domized evaluation ofthe WatchmanLeft Atrial Appendage Closuredeviceinpatientswithatrialfibrillationversus long-term warfarintherapy:thePREVAIL trial.JAmCollCardiol. 2014;64:1---12.
9.Boersma LV,SchmidtB, BettsTR,et al.Implantsuccess and safety of left atrial appendage closure with theWATCHMAN device: peri-procedural outcomes from the EWOLUTION reg-istry.EurHeartJ.2016:ehv730.
10.ReddyVY,HolmesD,DoshiSK,etal.Safetyofpercutaneousleft atrialappendageclosure:resultsfromtheWatchmanLeftAtrial AppendageSystemforEmbolicProtectioninPatientswithAF (PROTECTAF)clinicaltrialandtheContinuedAccessRegistry. Circulation.2011;123:417---24.
11.Urena M, Rodés-Cabau J, Freixa X, et al. Percutaneous left atrial appendage closure with the AMPLATZER cardiac plug deviceinpatientswithnonvalvularatrialfibrillationand con-traindicationsto anticoagulation therapy.J AmColl Cardiol. 2013;62:96---102.
12.TzikasA,ShakirS,GafoorS,etal.Leftatrialappendage occlu-sion for stroke prevention in atrial fibrillation: multicentre experiencewiththeAMPLATZERCardiacPlug.EuroIntervention. 2015;10.
13.KirchhofP,BenussiS,KotechaD,etal.2016ESCGuidelinesfor themanagementofatrialfibrillationdevelopedincollaboration withEACTS.EurJCardiothoracSurg.2016;50:e1---88.
14.CullenMW,StulakJM,LiZ,etal.Leftatrialappendagepatency atcardioversionaftersurgicalleftatrialappendage interven-tion.AnnThoracSurg.2016;101:675---81.
15.Schade A, Kerber S, Hamm K. Two in a single procedure: combinedapproach forMitraClip implantationand leftatrial appendage occlusionusing the Watchman device. JInvasive Cardiol.2014;26:E32---4.
16.PulsM,SeipeltR,SchillingerW.Completeinterventionalheart repairofmultipleconcomitantcardiacpathologiesinastaged approach.CatheterCardiovascInterv.2013;81:896---900.
17.LipGY,NieuwlaatR,PistersR,etal.Refiningclinicalrisk strat-ificationforpredicting strokeand thromboembolisminatrial fibrillationusinganovelriskfactor-basedapproach:theeuro heartsurveyonatrialfibrillation.Chest.2010;137:263---72.
18.LipGY,FrisonL,HalperinJL,etal.Comparativevalidationof anovelriskscoreforpredictingbleedingriskinanticoagulated patientswithatrialfibrillation: theHAS-BLED(Hypertension, AbnormalRenal/LiverFunction,Stroke,BleedingHistoryor Pre-disposition,Labile INR, Elderly,Drug/Alcohol Concomitantly) score.JAmCollCardiol.2011;57:173---80.
19.KatritsisGD,SiontisGC,GiazitzoglouE,etal. Complications oftransseptalcatheterizationfordifferentcardiacprocedures. IntJCardiol.2013;168:5352---4.