Francisco
Portela
a,∗,
Camila
C.
Dias
b,c,
Paulo
Caldeira
d,
Marilia
Cravo
e,
João
Deus
f,
Raquel
Gonc¸
alves
g,
Paula
Lago
h,
Henrique
Morna
i,
Paula
Peixe
j,
Jaime
Ramos
k,
Helena
Sousa
d,l,
Lurdes
Tavares
m,
Helena
Vasconcelos
n,
Fernando
Magro
o,p,q,
Paula
Ministro
raServic¸odeGastrenterologia,CentroHospitalarUniversitáriodeCoimbra,Coimbra,Portugal
bCIDES–DepartmentofHealthInformationandDecisionSciences,FacultyofMedicine,UniversityofPorto,Portugal cCINTESIS–CentreforHealthTechnologyandServicesResearch,Porto,Portugal
dGastroenterologyDepartment,CentroHospitalardoAlgarve,Portugal eServic¸odeGastrenterologia,HospitalBeatrizÂngelo,Loures,Portugal fServic¸odeGastrenterologia,HospitalFernandesdaFonseca,Amadora,Portugal gServic¸odeGastrenterologia,HospitaldeBraga,Braga,Portugal
hGastroenterologyDepartment,CentroHospitalarPorto-HospitalSantoAntónio,Portugal iServic¸odeGastrenterologia,HospitaldoFunchal,Funchal,Portugal
jServic¸odeGastrenterologia,CentroHospitalardeLisboaOcidental,Lisboa,Portugal kServic¸odeGastrenterologia,HospitaldosCapuchos,Lisboa,Portugal
lBiomedicalSciencesandMedicineDepartment,UniversityofAlgarve,Portugal mServic¸odeGastrenterologia,HospitaldeSantaMaria,Lisboa,Portugal nServic¸odeGastrenterologia,HospitaldeSantoAndré,Leria,Portugal oGastroenterologyDepartment,CentroHospitalarSãoJoão,Porto,Portugal
pDepartmentofPharmacologyandTherapeutics,FacultyofMedicine,UniversityofPorto,Portugal qMedInUP–CentreforDrugDiscoveryandInnovativeMedicines,UniversityofPorto,Portugal rServic¸oGastrenterologia,CentroHospitalardeTondela–Viseu,Viseu,Portugal
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:Received1December2016 Receivedinrevisedform 29December2016 Accepted30December2016 Availableonline6January2017 Keywords:
Complementaryandalternativemedicine (CAM)
Compliance
Inflammatoryboweldiseases(IBD)
a
b
s
t
r
a
c
t
Background:Theuseofcomplementaryandalternativemedicinesisincreasingamongchronicpatients,
particularlythoseafflictedwithinflammatoryboweldiseases.
Aim:Thisstudyaimedtoaddresstheprevalenceofcomplementaryandalternativemedicinesuseamong
Portugueseinflammatoryboweldiseases’patients.
Methods:Patientswereinvitedtofillananonymousquestionnaireconcerningtheuseofcomplementary
andalternativemedicines.
Results: Thirty-oneper cent of the patientsreported having used complementaryand alternative
medicinesin thepast, whereas12%wereusingthembythetimethequestionnairewas
adminis-tered.Fifty-ninepercentoftheusersdidnotsharethisinformationwiththeirphysician,whereas14%
and8%discontinuedtheirmedicationandperiodicalexamination,respectively.Steroidsprescription
(OR=2.880)andahigherinstructionlevel(OR=3.669)werepredictorsofcomplementaryandalternative
medicinesuseinthiscohort.
Conclusions:RoughlyathirdofPortugueseIBDpatientshadusedCAM.Steroidtreatmentandanacademic
degreeareassociatedwithCAMuse.Giventhepotentialsideeffectsandinteractions,patientinformation
aboutthebenefitsandlimitationsofconventionalandcomplementarytreatmentsshouldbereinforced.
©2017EditriceGastroenterologicaItalianaS.r.l.PublishedbyElsevierLtd.Allrightsreserved.
∗ Correspondingauthor.
E-mailaddress:[email protected](F.Portela).
1. Introduction
Inflammatoryboweldiseases(IBD),whichincludeCrohn’s dis-ease(CD)andulcerativecolitis(UC),arelifelongimmune-mediated disorders characterized by a relapse and remitting course, and http://dx.doi.org/10.1016/j.dld.2016.12.031
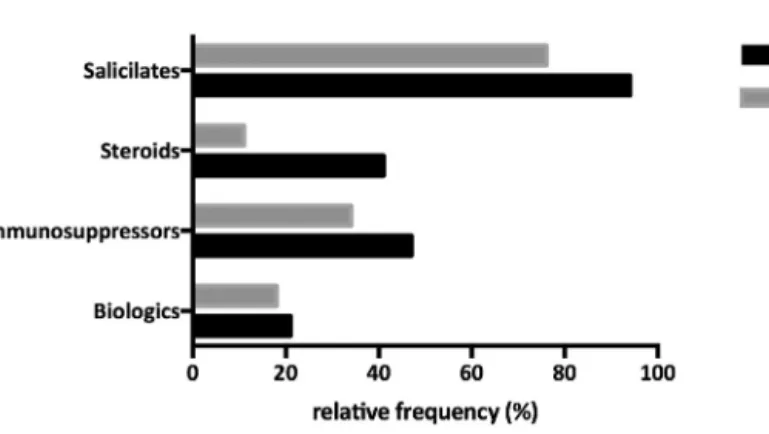
Fig1.RelativefrequencyofconventionaltherapiesusedamongthestudiedIBDpopulation.
particularlycommonindevelopedcountries[1,2].WhereasUCis limitedtotherectumandcolon,CDcanvirtuallyaffectanypart ofthegastrointestinaltract(GI),althoughbeingmorecommonly foundalongtheileumandinthebeginningofthecolon.Despitethis andotherdifferences,CDandUCshareacharacteristicheavy bur-denofsymptomatology:rectalbleeding,abdominalpain,diarrhea andfatiguearesomeofthemoreconspicuoussymptomsaffecting IBDpatients.Sofar,nocurativetherapieshavebeendevelopedfor UCorCD,andthereforethecurrentmanagementofthesediseases aimstocontrolthesymptomsandimprovepatients’health-related quality of life (HRQoL). Thismanagement relies onquite com-plextherapeuticlinesthatcanincludesteroids,anti-inflammatory drugs (such as 5-aminosalicylic acid[5-ASA]), immunomodula-tors (suchas azathioprine [AZA] oranti-tumournecrosis factor ␣[anti-TNF␣]),andbowelsurgery.Understandably,bothIBDand themedicationstakentocontroltheburdenofsymptomshavea highimpactonpatients’HRQoLandareassociatedwithahigher prevalenceofpsychologicaldisorders[3].
The awareness and interest in complementary and alterna-tivemedicines (CAM)hasbeenraisingamong IBDpatients.The EuropeanCrohn’sand Colitis Organisation(ECCO) defines com-plementaryand alternativetherapies accordingtotheirpattern ofuse:complementarytherapies arethosethatareused along-side withconventional medicine,whereas alternative therapies are those that are used in the place of conventional medicine [1,2].Theholisticandself-healingnatureofCAMis particularly attractivetochronicpatients,asitisthepopularnotionthatCAM hasno side effects. In thecontext of IBD, differenttechniques andproductsarecommonlyused,someofwhichhavebeenthe subjectof laboratorytestsand/orclinicaltrials:treatmentwith helminths[4],gut-directedhypnotherapy[5–8],herbalmedicines [8–12],acupuncture[8,13],nutritionalstrategies[8,14,15], exer-cise[16],andantioxidanttherapy[17] area fewofthem.Some of the results obtained in these trials are indeed promising – forinstance,theassociationofgut-directedhypnotherapywitha reducedIBD-relatedinflammationandanincreaseofHRQoL[6], orthedemonstrationthatBoswelliaserratagumresinandPlantago ovataseedsareaseffectiveas5-ASAinthetreatmentofUC[11]. However,theseresultsneedtobeinterpretedwithcaution,asthe lackofhigh-qualitydataremainsanissueinmostCAMstudies.The efficacyandsafetyofCAMneedtobeevaluatedbymulticentric anddoubleblindrandomizedcontrolledtrialswithlargesamples beforedefinitiveconclusionsaredrawn.
Theknowledge of CAM utilizationpatternsamong a certain communityis absolutely necessaryin ordertoprevent interac-tions with conventional medicine, potential side effects and a decreaseintherapeuticcompliance.Althoughsuchanissuehas beenapproachedin severalcountriesofNorth America, Europe
andAsia,thepictureinPortugalremainsunknown,andthestrong impactofregionalandculturalfactorsinCAMutilizationprevents theextrapolationoftheresultsfromotherEuropeancountries.As so,thisstudyaimedtoexploretheuseandattitudesofPortuguese IBDpatientstowardCAMbasedontheresultsofananonymous survey.
2. Materialandmethods
2.1. Studypopulation
IBDpatientswererecruitedfromAPDI(PortugueseIBDpatients’ association)andfrom13differentuniversityandcommunity hos-pitalsbetweenOctober2011andMarch2012.Patientsolderthan 18yearsandwithaconfirmeddiagnosisofUC,CDorunclassified colitiswereinvitedtoparticipateinthestudy.Thesepatientswere givenaquestionnairecontaining31yesornoandmultiplechoice questions focused on social-demographic aspects (gender, age, instructionlevelandprofessionalsector),clinicaldata,compliance, andCAMuseandattitudes.Allquestionnaireswereanonymous andself-administered,beingafterwardsreturnedbymail.Thelocal ethiccommitteehasapprovedthisstudy.
2.2. Statisticalanalysis
Categoricalvariables were describedusing absoluteand rel-ativefrequencies, whereas continuousvariables weredescribed using average, median, standard deviation, percentiles, and minimum/maximum values. The Pearson Chi-square test was used to test the independence of categorical variables. T and Mann–Whitneytestswereusedtotestthesimilarityofgroups, dependingonwhethertheirdistributionwasnormalornot nor-mal.Logisticregressionwasemployedtodeterminewhichfactors couldindependentlypredicttheuseofCAM.Alltestswere evalu-atedconsideringasignificancelevelof5%.Alldatawasarranged, processedandanalysedwithSPSS®v.19.0data(StatisticalPackage forSocialSciences),whereasgraphsweredesignedusingPrism7.
3. Results
3.1. Cohortcharacterization
Atotalof750questionnairesweredistributed,and442were returnedandconsideredvalid,whichcorrespondstoaresponse rateof59%.Ninequestionnaires(1.2%)wereconsideredinvaliddue toalackofanswers.Thesocio-demographicandclinical charac-teristicsofthestudypopulationaresummarizedinTable1.Most respondentswerefemale(57%),wereeducatedtoacollegedegree
Crohn’sdisease 299 65
Unclassified 8 2
Diseaseduration(median,P05–P95) 11 3–30
Hospitaladmissions(previous5years)(n,%)
None 253 56
1 90 20
2–5 94 21
>5 13 3
Bowel-relatedsurgeries(previous5years)
(n,%) 96 22
(median,P05–P95) 1 (1–3)
Conventionaltherapyprescription(n,%)
Yes 329 76
Disease-relatedcurrentwell-being(n,%)
Ok 182 40
So-so 213 47
Notok 54 12
Verybad 9 2
HaveyoueverusedalternativemedicinesbecauseofyourIBD?(n,%)
Yes 145 31
DoyoucurrentlyusealternativemedicinesbecauseofyourIBD?(n,%)
Yes 57 12
Howdidyoufeelregardingyourdiseasebythetimeyoudecidedtousealternativemedicines?(n,%)
Ok 14 10
So-so 36 25
Notok 49 34
Verybad 47 32
(39%)andworkedinthetertiarysector(79%).UCafflicted33%of
therespondents,whereas65%ofthemhadaCDdiagnosisand2%
hadunclassifiedcolitis.Themediantimeofdiseasedurationwas
11years,and22%ofallpatientshadundergoneatleastone
bowel-relatedsurgeryinthepreviousfiveyears.Duringthesametime
period,20and21%ofallpatientshadoneortwotofivehospital
admissions,respectively.Conventionaltherapieswereprescribed
toatotalof76%ofallrespondents,andthedistributionofthose
therapiesisdepictedonFig.1:salicylateswerethemostcommonly
prescribedmedications(94%of therespondentshad usedthem inthepastand76%wereusingthembythetime the question-naire wasadministered),followed byimmunosuppressors (47% inthepastand34%bythetimethequestionnairewas adminis-tered).Theprescriptionofsteroidswasrelativelycommoninthe fiveyearsprecedingthisstudy(41%ofpatientswereonsteroids), butbythetimethequestionnairewasadministeredonly11%ofthe respondersweremedicatedwiththesedrugs.Mostpatients(87%) reportedtheywerefeelingatleastpartiallywellinrelationtotheir IBD(Table1).
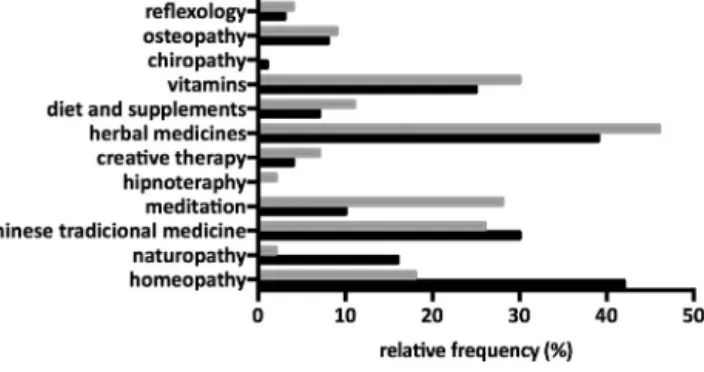
Atotalof145patients(31%)ofthiscohorthadusedsomekindof CAMtotreattheirIBDinthepast,and57(12%)werestilldoingsoby thetimethisquestionnairewasdistributed(Table1).Themajority ofthesepatients(66%)statedthattheywereeither“notok”or“very bad”inrelationtotheirIBDbythetimetheydecidedtoresortto CAM.ThetypesofCAMusedaredepictedinFig.2,alongsidewith theirrelativefrequencies.Herbalmedicinesandhomeopathywere theCAMtypesmorefrequentlyusedbythepatientsinthepast(39% and42%,respectively),butonlyherbalmedicinesremainedinthe
toppreferencesofthepatientsbythetimethequestionnairewas addressed(46%),followedbyvitaminsintake(30%).Homeopathy droppeddowntoarateofutilizationof18%.
3.2. AttitudesandreasonsleadingtoandfollowingCAM utilization
Theinabilityofconventionalmedicinetoimprovetheir condi-tionwasthemostcommonlyreportedreasonforpatientstoresort toCAM(33%),and 72%didsoafterreceivingadvicefroma col-league,friendoffamilymember(Fig.3).Atotalof67%ofallCAM usersreportedapositiveoutcomeoftheexperience(i.e.,theyfelt “better”or“muchbetter”afterCAMuse).Thecostsassociatedwith CAMwereconsiderablyhigh,with66%oftheCAMusers spend-ingover50D permonthinthesemedicines,and41%reportinga monthlycostover100D.Indeed,financialreasonswerethesecond mostcitedreasonforpatientstoabandonCAMafterexperiencing it(44%),surpassedonlybytheabsenceofpositiveoutcomes(51%). InwhatconcernsthepotentialeffectofCAMuseonconventional medicinecompliance,86% and92%oftherespondentsreported tohavemaintainedtheconventionaltherapy andtheperiodical examinationsandanalyses(respectively)duringthetimeperiod theywereusingCAM.Finally,59%oftheCAMusersconcealedthis informationfromtheirattendingphysician,and71%didsobecause theywereafraidofthephysicianreaction(Fig.3).Still,85%ofall IBDpatientswouldappreciatetheopportunitytodiscussCAMwith theirphysician.
Fig.2. RelativefrequencyofCAMtherapiesusedamongtheCAMusers.
Tertiary 102 (86) 194 (76)
IBD(n,%) 0.416
Ulcerativecolitis 41 (29) 109 (35)
Crohn’sdisease 99 (70) 199 (63)
Unclassified 2 (1) 6 (2)
Diseaseduration(median,P05–P95) 10(4–27) 11(3–30) 0.839***
Disease-relatedcurrentwell-being(n,%) 0.837
Ok 54 (39) 126 (40)
So-so 65 (46) 144 (46)
Notok 17 (12) 37 (12)
Verybad 4 (3) 5 (2)
Hospitaladmissions(previous5years)(n,%) 0.098
None 69 (50) 180 (59)
1 26 (19) 64 (21)
2–5 38 (28) 55 (18)
>5 5 (4) 7 (2)
Bowel-relatedsurgeries(previous5years) 0.601
(n,%) 32 (24) 63 (21)
(median,P05–P95) 2 (1–4) 1 (1–3) 0.318***
Conventionaltherapyprescription(n,%) 0.003
Yes 117 (85) 208 (71)
Conventionaltherapyduringthelast5years(n,%)
Biologics 0.088 Yes 36 (26) 57 (19) Immunossupressors 0.024 Yes 77 (55) 133 (43) Steroids 0.001 Yes 73 (53) 105 (36) Salicilates 0.053 Yes 113 (91) 279 (96)
Currentconventionaltherapy(n,%)
Biologics 0.043 Yes 30 (23) 45 (15) Immunossupressors 0.358 Yes 48 (38) 97 (33) Steroids 0.003 Yes 23 (18) 24 (8) Salicilates 0.078 Yes 90 (70) 231 (78)
Note:Boldmeanssignificant(p<0,05).
* PearsonChi-square.
** Ttestforindependentsamples. ***Mann–WhitneyTest.
3.3. ThetypicalprofileofaCAMuser-associatedvariablesand predictors
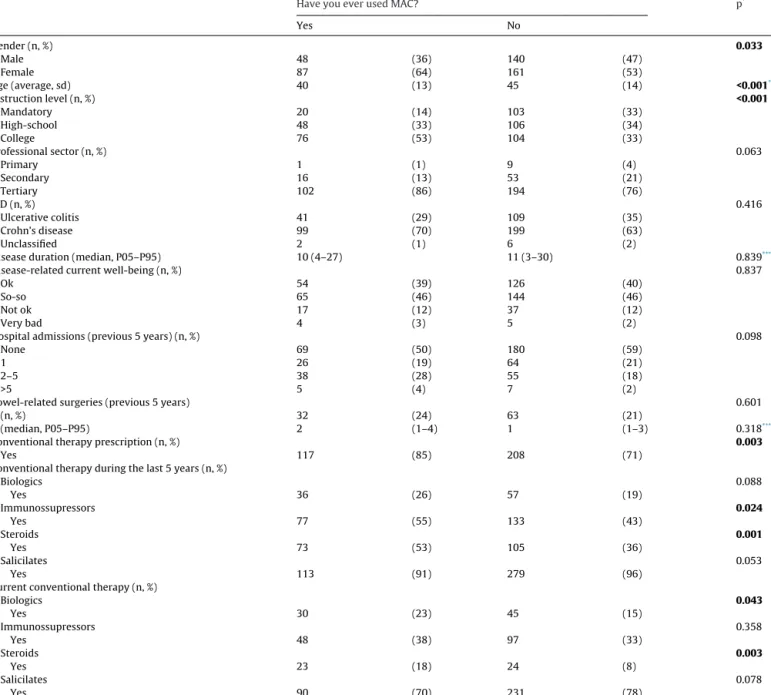
Table2liststhesocio-demographicandclinicalvariables inves-tigatedandtheirassociationwithCAMuse.Neitherdiseasetype nordiseasedurationnornumberofhospitaladmissionsandbowel surgeriesareassociatedtoCAMuseinasignificantfashion.Onthe otherhand,patientswhoareyounger(anaverageof40yearsold vs.45,p<0.001),females(64%ofallusers,p=0.033),andthathave acollegedegree(53%ofallusers,p<0.001)areparticularlyprone touseCAM.Moreover,CAMuseismorecommonamongpatients towhomconventionaltherapywasprescribed(p=0.003), partic-ularlythosethatwereonimmunosuppressorsorsteroidsinthe fiveyears precedingthequestionnaireadministration(p=0.024 andp=0.001,respectively),oronsteroidsor biologicalsbythe
timethequestionnairewasadministered(p=0.003andp=0.043, respectively).
Alogistic regression wasemployedtodiscernwhich factors werepredictiveofCAMuse(Table3).Althoughtherewerea num-berofsignificantvariablesontheunivariatemodel(gender,age, instructionlevel,hospitaladmissionsinthepreviousfiveyearsand prescriptionofconventionaltherapy,namelyimmunosuppressors, steroidsandbiologicals),onlytwoofthemretainedtheir signifi-canceinthemultivariatemodel:instructionlevelandsteroidsuse. IBDpatientseducatedtoacollegedegreeweremorethanthree timesmorelikelytouseCAMwhencomparedtothosewiththe mandatorylevelofinstruction(OR=3.669,95%CI:1.554,8.664), whereasthosethathadusedsteroidsatsometimeinthefiveyears preceding theadministration of thequestionnaire werealmost
Table3
MultivariateanalysisofvariablesassociatedwithCAMuse.
Univariatemodela Multivariatemodelb
OR CI95% p OR CI95% p
Gender
Male Ref
Female 1.576 1.037–2.396 0.033
Age,average(stdev) 0.972 0.957–0.988 <0.001 Instructionlevel
Mandatory Ref Ref
High-school 2.332 1.295–4.198 0.005 2.255 0.900–5.650 0.083 College 3.763 2.144–6.608 <0.001 3.669 1.554–8.664 0.003 Professionalsector Primary Ref Secondary 2.717 0.320–23.100 0.360 Tertiary 4.732 0.591–37.871 0.143 IBD
Unclassifiedcolitis Ref
Ulcerativecolitis 1.128 0.219–5.818 0.885
Crohn’sdisease 1.492 0.296–7.529 0.628
Diseaseduration 0.996 0.971–1.020 0.721
Disease-relatedcurrentwell-being
Ok Ref
So-so 1.053 0.683–1.624 0.814
Notok 1.072 0.556–2.068 0.835
Verybad 1.867 0.483–7.221 0.336
Hospitaladmissions(previous5years)
None Ref
1 1.060 0.622–1.807 0.831
2–5 1.802 1.095–2.966 0.020
>5 1.863 0.572–6.068 0.302
Bowel-relatedsurgeries(previous5years)
Yes 1.138 0.701–1.847 0.601
No Ref
Howmanysurgeries? 1.219 0.779–1.908 0.386
Conventionaltherapyprescription
Yes 0.450 0.265–0.764 0.003
No Ref
Conventionaltherapyduringthelast5years Biologics Yes 1.510 0.9.9–2.429 0.089 No Ref Immunosuppressors Yes 1.583 1.060–2.364 0.025 No Ref Steroids Yes 2.011 1.333–3.032 0.001 2.880 1.619–5.124 <0.001 No Ref Ref Salicilates Yes 0.442 0.189–1.030 0.059 No Ref
Currentconventionaltherapy Biologics Yes 1.701 1.013–2.854 0.044 No Ref Immunosuppressors Yes 1.225 0.795–1.887 0.358 No Ref Steroids Yes 2.473 1.338–4.574 0.004 No Ref Salicilates Yes 0.656 0.410–1.049 0.079 No Ref
Note:Boldmeanssignificant(p<0,05).
aDependentvariable:MACuse.
bDependentvariable:MACuse;independentvariables:allofthosethathadapvaluebelow0.20intheunivariatedmodelselectedbytheForwardmethod.
threetimesmorelikelytouseCAMthanthosewhohadnottaken anysteroidsinthattimeperiod(OR=2.880,95%CI:1.619,5.124).
4. Discussion
The utilization of CAM seems to be rising among chronic patients,particularlyamongthosethatsufferfromIBD.Butdespite
thecommonperceptionthatCAM issafe,someoftheproducts employedmayhavekidneyandlivertoxicity,and/ormayinteract withconventionaltherapeutics,decreasingtheireffect.The knowl-edgeonthepatternsofCAMuseisfundamentaltotackletheissues mentionedabove.Suchinformationwas,tothebestofour knowl-edge,unavailableinwhatconcernsPortugueseIBDpatients.This
theirprevalencevaluesreferto“everused”or“currentuse”ofCAM. Still,theCAMutilizationamong PortugueseIBD patientsseems tobesimilar tothat foundacrossother South European coun-tries(23.6%–28.2%inItaly[18,19]and23.1%inSpain[20]),Korea (29.5%–30%[21,22]),UK(26%[23])andHungary(30.9–31.7%[24]). Ontheotherhand,theprevalenceofCAMuseseemstobehigher amongIBD patientsfrom Germany(51.3%–52%[25,26]), France (65.6%[27]),Norway(30–49%[28,29]),Canada(21%–56%[30,31]), Australia(45.4%[32])andNewZealand(44.1%[33]).Ourresults arebased ona59% response ratewhich isless than whatwas achievedinsomepapers[18,28]butsimilartoothers [25].The factthatpatientswerefreetoanswerthequestionnairesathome andreturnedthembymailmayhavehadanegativeimpacton theresponseratebut,inouropinion,itwasimportanttolimitthe constraintsinherenttohospitalenvironment.
RegardingtheoutcomesofCAMuse,67%oftherespondentsin thisstudyreportedfeeling“better”or“muchbetter”.Thisvalue ishigherthanthatfoundamongotherstudiesthataddressedthis parameter,whichvariedbetween26%and55.6%[20,21,23].D’Inca etal.hasfurtheranalysedthespecificreasonsthatunderliethe patients’satisfactionwithCAM,andobservedthatwhether45.5%of CAMusersreportedageneralsenseofwell-beingbutwithout clini-caleffect,39.7%and21.8%actuallyexperiencedanimprovementin theirIBDsymptomsandareductioninthenumberofflares, respec-tively[18].ItisimportanttonoticethatthepositiveeffectsofCAM inthisandotherstudiesareself-reported,andarethereforethe resultofacomplexinteractionbetweenphysicalandpsychological factors,wheretheplaceboeffectcannotbedismissed.
Thepreferences interms of CAM type unveiledan interest-ingpattern:whereashomeopathy,herbalmedicineandChinese traditional medicine appear to have been popular in the time period that preceded the questionnaire administration, herbal medicine,vitamins,meditationandtraditionalChinesemedicine werethepreferredtherapiesbythetimethepatientsenteredthe study.Theseresultsarenotuncommon:homeopathyand/orherbal medicinestendtorankhighamongthepreferencesofEuropean CAMusers[18–20,23–26,29,34].Ontheotherhand,probioticstend tobethepreferredCAM inNorth America [30,31].Onceagain, thesedifferencesmayresultfromasimplemethodologicalbias: withafewexceptions,probioticsarenotconsideredtobeCAM amongEuropeanstudies(andthereforearenotanoptiononthe questionnaires).
Theabsenceofimprovement followingconventionaltherapy was the most cited reason for CAM users to try these thera-pies(33%),followedbythepossiblesideeffectsofconventional therapies(15%)andbytheinabilityofconventionalmedicineto curetheirdisease(14%).Thismotivational context issimilarto that observed in other studies in what concerns the so-called push-factors(i.e.,factorsthatpushapatientawayfrom conven-tionalmedicine)[19,26,30–32,34].Unfortunately,wehavefailedto includeinourquestionnairethepull-factors(i.e.,factorsthatpulla patienttowardCAM),suchasthepossibilitytohaveagreater
con-self-reported.Andif,ononehand,patientsarenotalwayswilling toadmittheydiscontinuedtheirmedication,ontheotherhand, thelackofadherencemayactuallybeunintended(andunnoticed bypatients).Indeed,Nguyenetal.haveshownthatCAMusewas associatedwithalessfavorableadherencetoconventionaltherapy, but97%ofnon-adherentsreportedthattheirattitudewas uninten-tional[31].Conversely,Weizmanetal.concludedthatCAMusewas notassociatedwithalackofadherencetoconventionaltherapies [30].Morestudiesareneededtoclarifythisissueandtodevelop compliance-enhancingstrategiesforIBDpatients,bothCAMusers andnon-users.
Doctor–patientcommunicationandmutualtrustisan unavoid-ablekeyaspectonehastoconsiderwhenaddressingCAMuse.In thisstudy,59%ofCAMusersdidnot disclosethefactthatthey wereusingCAMtotheirphysician,and71%ofthemclaimedthey didsobecausetheywereafraidoftheMDreaction.However,85% ofallIBD patientsin thiscohort wouldappreciatethe possibil-itytodiscussCAMwiththeirattendingphysician.Thisscenariois transversaltodifferentIBDpopulations:aconsiderableproportion ofCAMuserschoosenottodisclosethatinformationtotheir physi-cian[25,30,32].AqualitativestudybyLindbergetal.suggestedthat IBDpatientswouldliketodiscussCAMusewiththeirphysician, buttheydonotinitiateanyconversationonthissubjectforfear theywouldnotbetakenseriously[35].Incontrast, gastroenterol-ogistswereshowntohaveagenerallypositiveattituderegarding CAM:astudyfromGallingerandNguyenbasedonawebsurvey reportedthat68%ofgastroenterologistsbelievedthatCAMcould beagoodadjuvantinIBDtherapyand72%feltcomfortable dis-cussingit[36];aqualitativestudybyLindbergetal.reportedthat healthprofessionalsbelievedCAMbelongedwithinhealthcareand wasrelevanttoconventionaltherapeutics[37].Notwithstanding,a commoncomplaintamongallgastroenterologistsandotherhealth professionalswasthelackofformalknowledgeinthearea.Given theincreasingimportanceandprevalenceofCAMuse,the intro-ductionofCAM-relatedtopicsinmedicalschoolsandworkshops ofcontinuingmedicaleducationisabsolutelynecessary,andwill undoubtedlybeakeysteptofacilitatedoctor-patient communica-tioninthisparticularsubject.
Thefemalegender,youngerage,collegeeducation,previoususe ofimmunosuppressorsandsteroids,andcurrentuseofbiologicals andsteroidsweresignificantlyassociatedwithCAMuse.College instructionandprevioususeofsteroidswereactually indepen-dentpredictorfactorsofCAMuse,withORsof3.669and2.880, respectively. These relationships have been noticed before in severalstudiesand, oppositetowhat happens withotherCAM usefeatures,seemtobetransversalacrossdifferentgeographic locationsandIBDpopulations[18,19,22,24,26,28–30,32,33].Other factorsassociatedwithCAMusehavebeendepictedinother stud-ies,butthosewereeithernotexploredorfailedtobeassociated withCAMuseinthepresentstudy:evidenceforahealth-conscious lifestyle, number of hospital admissions and consultations, drug-sideeffectsandothercomplications,relapses,long-term
evo-lution of the disease,need for psychologicalsupport, presence ofextra-intestinalmanifestations,permanentemployment,higher incomeandpresenceofco-morbidities[18–20,22,26,28,32,33,38]. Conventional therapies have known side effects, the fear of whichmayleadpatientstoresorttoCAMinthesearchofwhat theybelievetobea more naturaland less toxicapproach. The factthat previoususeof steroidswasfoundasanindependent predictorofCAMusecanbe,atleastinpart,explainedbytheside effectsprofileofthesedrugs.Steroidscanalsobeconsidereda sur-rogatemarkofamoderateorseveredisease,whichhasbeenlinked toCAMuseinotherstudies[18,19,22,29].Ontheotherhand,the associationofCAMusetoahighlevelofinstructionisquite com-monandmayberelatedtothefactthatcollege-educatedpatients aremoreresourcefulandmorelikelytoexploretheirIBDdisease fromdifferentperspectives.Moreover,theuseofCAMgivesthema senseofcontrolovertheirdisease.Additionally,theyarealsomore likelytobeabletoaffordCAM:infact,andasshownbythisand otherstudies,CAMuseisratherexpensive[18,27].Theassociation ofCAMusewithpermanentemploymentandhigherincomeseen inotherstudiessupportsthishypothesis[22,32,33].Still,the rela-tionshipbetweencollegeeducationandtheuseoftherapiesmostly deprivedofscientificsupportmeritsfurtherstudies.
Thisstudywasbasedonananonymousquestionnairethatwas distributedacrosstheentirecountry(ruralandurbanareas)and includedpatientsindifferentstagesandwithdifferentseverityof thediseases(patientswererecruitednotonlyfrommedical consul-tationsbutalsofromthePortugueseassociationofIBDpatients).It has,however,afewlimitationsthatshouldbenoticed.Oneofthem isinherenttoallquestionnaire-basedCAMassessments–thelack ofconsistencybetweenthequestionnairesadministeredin differ-entcountriesmakestheircomparisonsdifficultorevenimpossible. Thedevelopmentandnational-validationofaninternationalCAM questionnairewithaprecisedefinitionofwhatshouldbe consid-eredCAM[39],aswellasthethroughoutcharacterizationofthe populationenrolled,arekeystepstosolvetheseissues.Another limitationreferstothefactthatthestudiedpatientswereinpart recruitedfromconventionalmedicinecarecenters:satisfiedusers ofCAMareunlikelytoattendthesecenters,whichintroducesa biasinthesamplingprocess.ThediseasestatusandCAM improve-mentswereself-reportedandnotobjectivelyevaluated–thisis anunavoidableconsequenceofkeepingthequestionnaires anony-mous;however,itdoespreventonetoidentifyplaceboeffectsand inflammatory bowelsyndrome-relatedworsening ofsymptoms. Finally,thequestionnairewasnotpreviouslyvalidated,itdidnot explorepositivemotivationalfactors,andwehadnoinformation onthepatients’psychologicalstateofmindandHRQoL.
Asa globalconclusion, theCAMusepatternsofIBDpatients inPortugalmatchthosepreviouslyfoundamongotherEuropean countries:thetypicaluserisayoungfemalewithacollege educa-tionandanhistoryofsteroidsprescription,whereasthepreferred CAMtypeisherbalism.Theprevalenceisratherhighandis intrin-sically linked with the perceived inability of the conventional medicinetoproducepositiveoutcomes.Patient-doctor communi-cationisanissue:patientswouldliketodiscussCAMwiththeir physicians,but theyfear theirreaction andend upnot disclos-ingCAMuse.Medicinefacultiesandcontinuingmedicaleducation shouldinvestin disseminating formalknowledge onCAM, and physicians should improve their empathy and understand the benefitsofanintegrativehealthcare,includingconventionaland non-conventionaltherapies.Thiswouldlikely enhancepatients’ complianceandsolvepossibleCAM-relatedadherenceissues.
Conflictofinterest
F.Portelareceivedapresentingfeefrom:AbbVie,Ferring,MSD, ViforPharma.FMagroreceivedapresentingfeefrom:AbbVie,
Fer-ring,Falk,Hospira,PharmaKern,MSD,Schering,Lab.Vitoria,Vifor, OmPharma.Allothersauthors:nonetodeclare.
Support
GEDII(PortugueseIBDStudyGroup).
Acknowledgments
TheauthorswouldliketoexpresstheirgratitudetoAbbviefor supportingmail-relatedexpenses,toSandraDiasforhersupportas thecoordinatorofthenationalIBDgroup(GEDII–GrupodeEstudo deDoenc¸asInflamatóriasIntestinais),andtoCatarinaL.Santosfor medicalwritingassistance.
References
[1]DignassA,EliakimR,MagroF,etal.SecondEuropeanevidence-basedconsensus onthediagnosisandmanagementofulcerativecolitispart1:definitionsand diagnosis.JournalofCrohn’s&Colitis2012;6:965–90.
[2]VanAsscheG,DignassA,PanesJ,etal.ThesecondEuropeanevidence-based consensusonthediagnosisandmanagementofCrohn’sdisease:definitions anddiagnosis.JournalofCrohn’s&Colitis2010;4:7–27.
[3]AlarhayemA,AchebeE,LogueAJ.Psychosocialsupportoftheinflammatory boweldiseasepatient.TheSurgicalClinicsofNorthAmerica2015;95:1281–93, vii–viii.
[4]SzkudlapskiD,LabuzekK,PokoraZ,etal.Theemeringroleofhelminthsin treatmentoftheinflammatoryboweldisorders.JournalofPhysiologyand Pharmacology2014;65:741–51.
[5]MoserG.Theroleofhypnotherapyforthetreatmentofinflammatorybowel diseases.ExpertReviewofGastroenterology&Hepatology2014;8:601–6. [6]SzigethyE.Hypnotherapyforinflammatoryboweldiseaseacrossthelifespan.
TheAmericanJournalofClinicalHypnosis2015;58:81–99.
[7]PetersSL,MuirJG,GibsonPR.Reviewarticle:gut-directedhypnotherapyinthe managementofirritablebowelsyndromeandinflammatoryboweldisease. AlimentaryPharmacology&Therapeutics2015;41:1104–15.
[8]JoosS.Reviewonefficacyandhealthservicesresearchstudiesof complemen-taryandalternativemedicineininflammatoryboweldisease.ChineseJournal ofIntegrativeMedicine2011;17:403–9.
[9]SalagaM,ZatorskiH,SobczakM,ChenC,FichnaJ.Chineseherbalmedicines inthetreatmentofIBDandcolorectalcancer:areview.CurrentTreatment OptionsinOncology2014;15:405–20.
[10]AlgieriF,Rodriguez-NogalesA,Rodriguez-CabezasME,RiscoS,OceteMA, GalvezJ.Botanicaldrugsasanemergingstrategyininflammatorybowel dis-ease:areview.MediatorsofInflammation2015;2015:179616.
[11]TriantafyllidiA,XanthosT,PapaloisA,TriantafillidisJK.Herbalandplant ther-apyinpatientswithinflammatoryboweldisease.AnnalsofGastroenterology 2015;28:210–20.
[12]GilardiD,FiorinoG,GenuaM,AlloccaM,DaneseS.Complementaryand alter-nativemedicineininflammatoryboweldiseases:whatisthefutureinthe fieldofherbalmedicine?ExpertReviewofGastroenterology&Hepatology 2014;8:835–46.
[13]JiJ,LuY,LiuH,etal.Acupunctureandmoxibustionforinflammatorybowel dis-eases:asystematicreviewandmeta-analysisofrandomizedcontrolledtrials. Evidence-BasedComplementaryandAlternativeMedicine2013;2013:158352. [14]ClarkeJO,MullinGE.Areviewofcomplementaryandalternativeapproaches
toimmunomodulation.NutritioninClinicalPractice2008;23:49–62. [15]NguyenDL,LimketkaiB,MediciV,SaireMendozaM,PalmerL,BechtoldM.
Nutritionalstrategiesinthemanagementofadultpatientswithinflammatory boweldisease:dietaryconsiderationsfromactivediseasetodiseaseremission. CurrentGastroenterologyReports2016;18:55.
[16]BilskiJ,Mazur-BialyA,BrzozowskiB,etal.Canexerciseaffectthecourseof inflammatoryboweldisease?Experimentalandclinicalevidence. Pharmaco-logicalReports2016;68:827–36.
[17]MouraFA,deAndradeKQ,dosSantosJC,AraujoOR,GoulartMO.Antioxidant therapyfortreatmentofinflammatoryboweldisease:doesitwork.Redox Biology2015;6:617–39.
[18]D’IncaR,GarribbaAT,VettoratoMG,etal.Useofalternativeand complemen-tarytherapiesbyinflammatoryboweldiseasepatientsinanItaliantertiary referralcentre.DigestiveandLiverDisease2007;39:524–9.
[19]BertomoroP,RennaS,CottoneM,etal.Regionalvariationsintheuseof com-plementaryandalternativemedicines(CAM)forinflammatoryboweldisease patientsinItaly:anIG-IBDstudy.JournalofCrohn’s&Colitis2010;4:291–300. [20]FernandezA,Barreiro-deAcostaM,VallejoN,etal.Complementaryand alter-nativemedicineininflammatoryboweldiseasepatients:frequencyandrisk factors.DigestiveandLiverDisease2012;44:904–8.
[21]KimSB,ParkSJ,ChungSH,etal.Vaccinationandcomplementaryand alterna-tivemedicineinpatientswithinflammatoryboweldisease.IntestinalResearch 2014;12:124–30.
[27]AbitbolV,LahmekP,BuissonA,etal.Impactofcomplementaryandalternative medicineonthequalityoflifeininflammatoryboweldisease:resultsfroma Frenchnationalsurvey.EuropeanJournalofGastroenterology&Hepatology 2014;26:288–94.
[28]OpheimR,BernklevT,FagermoenMS,CvancarovaM,MoumB.Useof com-plementaryandalternativemedicineinpatientswithinflammatorybowel disease:resultsofacross-sectionalstudyinNorway.ScandinavianJournalof Gastroenterology2012;47:1436–47.
[29]OpheimR,HoivikML,SolbergIC,MoumB,GroupIS.Complementaryand alter-nativemedicineinpatientswithinflammatoryboweldisease:theresultsofa population-basedinceptioncohortstudy(IBSEN).JournalofCrohn’s&Colitis 2012;6:345–53.
[30]WeizmanAV,AhnE,ThanabalanR,etal.Characterisationof complemen-taryandalternativemedicineuseanditsimpactonmedicationadherence ininflammatorybowel disease.AlimentaryPharmacology &Therapeutics 2012;35:342–9.
[36]GallingerZR,NguyenGC.Practicesandattitudestowardcomplementaryand alternativemedicineininflammatoryboweldisease:asurveyof gastroenterol-ogists.JournalofComplementary&IntegrativeMedicine2014;11:297–303. [37]LindbergA,EbbeskogB,KarlenP,OxelmarkL.Inflammatoryboweldisease
professionals’attitudestoandexperiencesofcomplementaryandalternative medicine.BMCComplementaryandAlternativeMedicine2013;13:349. [38]Sirois FM. Health-related self-perceptions over time and provider-based
complementaryandalternativemedicine(CAM)useinpeoplewith inflam-matory boweldisease orarthritis. ComplementaryTherapiesinMedicine 2014;22:701–9.
[39]QuandtSA,VerhoefMJ,ArcuryTA,etal.Developmentofaninternational questionnairetomeasureuseofcomplementaryandalternativemedicine (I-CAM-Q).JournalofAlternativeandComplementaryMedicine2009;15:331–9.