Disponible en castellano/Disponível em língua portuguesa SciELO Brasil www.scielo.br/rlae 1 Paper extracted from the study funded by CAPES, Theme Project FAPESP (process No. 2003/08386-3), Integrated Project CNPq (process No. 500901/ 2003-1), Padct III millennium/Brazilian Tuberculosis Research Network – REDE-TB (process No. 62.005/01-4); 2 Ph.D. in Nursing and Public Health, Researcher; 3 Doctoral Student. University of São Paulo at Ribeirão Preto College of Nursing - WHO Collaborating Centre for Nursing Research Development, Brazil; 4 Full Professor, University of São Paulo at Ribeirão Preto Medical School, Deputy coordinator of the Brazilian Tuberculosis Research Network (REDE-TB); 5 Full Professor, University of São Paulo at Ribeirão Preto College of Nursing - WHO Collaborating Centre for Nursing Research Development, Brazil; Operational Research Coordinator of the Brazilian Tuberculosis Research Network, e-mail: [email protected]
PERFORMANCE INDICATORS OF DOT AT HOME FOR TUBERCULOSIS CONTROL IN A
LARGE CITY, SP, BRAZIL
1Roxana Isabel Cardozo Gonzáles2 Aline Aparecida Monroe3 Ricardo Alexandre Arcêncio3 Mayra Fernanda de Oliveira3 Antonio Ruffino Netto4 Tereza Cristina Scatena Villa5
Cardozo Gonzáles RI, Monroe AA, Arcêncio RA, Oliveira MF, Ruffino Netto A, Villa TCS. Performance indicators of DOT at home for tuberculosis control in a large city, SP, Brazil. Rev Latino-am Enfermagem 2008 janeiro-fevereiro; 16(1):95-100.
The study had the objective to analyze the performance of the health services that implement the Directly Observed Therapy at home for tuberculosis control. This study analyzed four Tuberculosis Control Programs, referred to as A, B, C, and D, using the following indicators: Resource use; Performance quickness; Monitoring medication administration; Time spent per home visit. Data were collected during visits to 47 patients receiving DOT at home. Resource use was higher in program B (91.3%); program A showed quicker performance (5.8) and more visits during which medication administration was monitored (77.4%); program C had the longest time spent per home visit (14.7 minutes) and program A the shortest (10.4 minutes). The best or worst performance numerically expresses how resources are being used and whether the observation of medication intake is being achieved.
DESCRIPTORS: health programs and plans/standards; directly observed therapy; tuberculosis/control & prevention
INDICADORES DE DESEMPEÑO DEL DOT EN DOMICILIO PARA EL CONTROL DE LA
TUBERCULOSIS EN UN MUNICIPIO DE GRAN COMPLEJIDAD, SP, BRASIL
La finalidad del estudio fue analizar el desempeño de los servicios de salud que brindan Tratamientos por observación en domicilio para el control de la tuberculosis. Se estudiaron cuatro Programas de Controle da Tuberculosis identificados como A, B, C y D a partir de los indicadores de Aprovechamiento de recursos; Agilidad en el desempeño; Supervisión de la administración del medicamento y Tiempo utilizado por visita domiciliaria. Los datos fueron recolectados durante la visita a 47 enfermos. Se observó que el aprovechamiento de recursos fue mayor en el programa B (91,3%); en el programa A fue observada mayor agilidad (5,8) y mayor porcentaje de visitas con supervisión en la administración del medicamento (77,4%); en el programa C fue mayor el tiempo utilizado por visita (14,7 minutos), siendo este menor para el programa A (10,4 minutos). El mayor o menor desempeño expresa numéricamente la forma cómo los recursos están siendo utilizados, así como el alcance de las metas al respecto de la observación durante la ingestión de medicamentos.
DESCRIPTORES: planes y programas de salud/normas; terapia por observación directa; tuberculosis/controle & prevención
INDICADORES DE DESEMPENHO DO DOT NO DOMICÍLIO PARA O CONTROLE DA
TUBERCULOSE EM MUNICÍPIO DE GRANDE PORTE, SP, BRASIL
O estudo teve como objetivo analisar o desempenho dos serviços de saúde que executam a Terapia Diretamente Observada (DOT) no domicílio para o controle da tuberculose. Foram estudados quatro Programas de Controle da Tuberculose nomeados como A, B, C e D a partir dos seguintes indicadores: aproveitamento dos recursos; agilidade do desempenho; monitoração da administração da medicação; tempo gasto por visita domiciliar. Os dados foram coletados durante a visita a 47 doentes em DOT no domicílio. Observou-se que o aproveitamento dos recursos foi maior no programa B (91,3%); maior agilidade (5,8) e maior porcentagem de visitas com monitoração da administração da medicação (77,4%) no programa A; maior tempo gasto por visita no programa C (14,7 minutos) e menor no programa A (10,4 minutos). O maior ou menor desempenho expressa numericamente a forma como os recursos estão sendo utilizados e se a observação da ingestão medicamentosa está sendo alcançada.
INTRODUCTION
T
he World Health Organization (WHO) haswidely supported the implementation of the Directly
Observed Treatment (DOT) as part of the DOTS
strategy (Directly Observed Therapy - Short-course),
which aims to favor patient compliance, and to
guarantee treatment completion. These two aspects
are still the greatest barriers to an effective
tuberculosis (TB) management and the cause of
increased multidrug resistance(1).
The DOT strategy in Brazil started in 1998
and has been successfully implemented in distinct
situations(2-4). The DOT is generally carried out at the
patient’s home or at the health service.
The DOT or supervised treatment (ST), as a
technology to manage tuberculosis control, consists
of a group of activities focused on planning the
treatment of the patient with tuberculosis and his or
her family, which is carried out by a health team. It
comprises the following activities: evaluating the
patient’s sociocultural and economic profile and his
or her participation in the therapeutic plan and
treatment compliance, observation of medication
intake by the health professional or the responsible
person , psychological support to the patient and his
or her family, search for respiratory symptoms,
delivery of incentives, monitoring the patient’s health
condition through the data registered in the health
information system, and other activities.
Choosing the location to carry out the DOT
depends on the agreement established between the
health service and the patient and his or her family;
it can occur at home, at the health service, or in other
locations.
It is important to state that it is impossible to
provide DOT at home without a minimum health
service structure that allows for the development of
activities inherent to the treatment of the patient with
tuberculosis.
Studies about the provision of DOT at home
in different countries have shown that the strategy
has contributed significantly to treatment compliance
and completion,, This was observed in Botswana and
Thailand, where cure rates increased with the TB
supervision treatment at home(5).
In Brazil, a study shows that TB treatment
compliance depends on the connection and welcoming
that health professionals offer to the patient during
the ST(6).
Some studies(7-8) attribute that the TB patients’
failure to comply with treatment is associated with
the fact that the patients have to go to the health
service to receive the medication.
It should be stressed that, in addition to its
contribution to treatment compliance and completion,
providing DOT at home also helps to re-organize the
health service and introduces new ways of managing
material and human resources, as well as the
registration and information system.
OBJECTIVE
Due to the need to understand some aspects
regarding the administration and organization of health
services that use the DOT strategy for TB control,
this study had the objective to:
- analyze health service performance in the
TB control through indicators regarding coverage,
resource use, performance quickness, monitoring
medicine administration, and time spent per home
visit in the Tuberculosis Control Programs that perform
the DOTS/ST.
METHODOLOGY
This is an exploratory study carried out in a
large city (505.012 inhabitants) in the State of São
Paulo - Brazil, using indicators to evaluate the
performance of the health services that perform the
DOT at the patient’s home. The Tuberculosis Control
Program is managed by a specialized team in each
district, and works in reference units. All programs
that carry out DOT at home were studied. The city
uses specific criteria to include patients in DOT. The
health service establishes an agreement with the
patient/family regarding the location where
supervision will take place, and the choice is usually
the patient’s home. The frequency of supervision varies
and occurs according to the patient’s profile,
availability of human and material resources, and
even the proximity between patient’s home and the
health service.
With the objective of collecting and analyzing
the data, the Tuberculosis Control Programs were
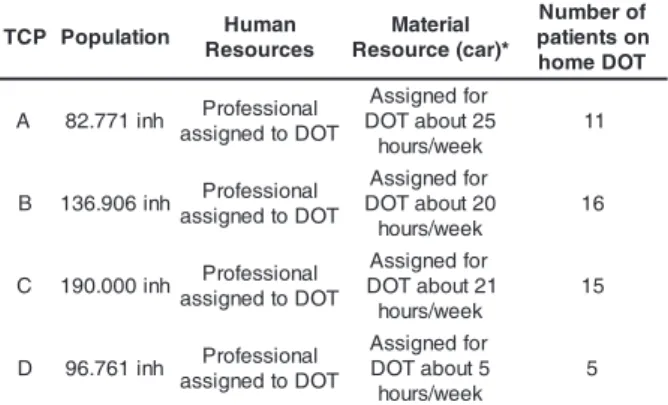
named A, B, C, D and characterized according to
population, availability of human/material resources,
Table 1 - Characterization of the Tuberculosis Control
Programs in the city of Ribeirão Preto, SP
important to emphasize that the home visits in the
DOT are generally carried out for MIO, however, some
visits are carried out to complement patient/family
care.
The time spent per home visit included the
transportation time of the health care professional to
the patient’s home and the time used during the visit
for treatment supervision.
The data collection was carried out during July
2003, using the Systematic Observation Technique
through the follow up of the home visits carried out
by the health care professional responsible for
supervising the TB patient’s home treatment in the
four health districts.
This study followed 47 patients from the four
health districts who received DOT at home. Of these,
28 were males and 19 were females; 91.49% were
pulmonary and 74.47% received treatment for the
first time.
In order to comply with the ethical and legal
aspects of research involving human beings,
determined by Resolution 196/96 of the National Health
Council, this research was approved by the Ribeirão
Preto College of Nursing Research Ethics Committee.
RESULTS AND DISCUSSION
The performance of the Tuberculosis Control
Program in each district that provides DOT at home
was analyzed through the indicators created in the
study. Considering the importance of human (health
care professional supervisor and driver) and material
resources (car) to provide DOT at home, the results
obtained regarding the indicator resource use in each
program are presented.
Table 2 - Resource time utilization of DOT/ST at home
by each Tuberculosis Control Program, 2003 P
C
T Population Human s e c r u o s e R l a i r e t a M * ) r a c ( e c r u o s e R f o r e b m u N n o s t n e i t a p T O D e m o h
A 82.771inh Professional T O D o t d e n g i s s a r o f d e n g i s s A 5 2 t u o b a T O D k e e w / s r u o h 1 1
B 136.906inh Professional T O D o t d e n g i s s a r o f d e n g i s s A 0 2 t u o b a T O D k e e w / s r u o h 6 1
C 190.000inh Professional T O D o t d e n g i s s a r o f d e n g i s s A 1 2 t u o b a T O D k e e w / s r u o h 5 1
D 96.761inh Professional T O D o t d e n g i s s a r o f d e n g i s s A 5 t u o b a T O D k e e w / s r u o h 5
*The time available for the material resources varies according to the organization of the health service, therefore the average week time was calculated.
The basic focuses used to evaluate medical
care quality - Structure-Process-Result(9-11) - were
used as the methodological-theoretical approach.
Performance indicators were determined
considering the optimization of material and human
resources, and the effective observation of medicine
intake in the studied programs. Thus, some indicators
correspondent to the material and human resources
were created to make it possible for the Tuberculosis
Control Program of each District unit to execute the
DOT. These include facilities, transportation (car), and
human resources (driver and health care professional
responsible for the DOT in the program), in addition
to the essential DOT activity (home visit for Medicine
Intake Observation).
The developed TCP performance indicators
were: Resource use (resource time spent/resource
available time); Performance quickness (number of
home visits carried out per hour available for the DOT
resources); Monitoring medication administration
(number of home visits with Medicine Intake
Observation (MIO)/number of home visits for MIO);
and Time spent per home visit (Time spent for the
DOT resources (min)/Total of home visits).
The time available was considered from the
moment the car arrived with the driver at the health
service to carry out the supervision home visits; and
the resource time spent corresponded to the time from
the moment the health care professional left the unit
until returning to the service. The visits for Medicine
Intake Observation (MIO) were those which had as
the main objective the observation itself, and home
visits with Medicine Intake Observation where those
in which the patient ingested the medicine in the
presence of the health care professional. It is
s m a r g o r P / e c i v r e S h t l a e
H Resourcetime
t n e p s e m i t e c r u o s e R / e l b a l i a v a ) A
( 88.5%
) B
( 91.3%
) C
( 75.0%
) D
( 89.6%
Program B shower the best utilization
(91.3%), followed by D (89.6%), A (88.5%), and C
(75.0%).
This means that program B had better
utilization of the resource time available, both material
The highest and lowest resource-use times by
the Tuberculosis Control Programs are due to their availability of human and material resources. Programs
A, B, and C have a health care professional assigned for
the development of the DOT at home activities, while
program D has only one professional who has the
responsibility to carry out other activities inside and
outside the health service in addition to the home supervisions. This demanded more time, and made it
impossible to carry out visits to the patients at home within the programmed time. Besides, this program does
not have a car and a driver assigned only for the execution
of the DOT, hence the need for the professional to constantly negotiate the use of such resources with the
managerial teams of other programs. It is worth stressing that the health care professionals assigned for the DOT
are also responsible for some activities due to the health service needs. Furthermore, sometimes some programs
take over the responsibility to carry out the DOT of
patients who belong to the city area covered in situations such as vacations, employee leave, or patient’s choice
to carry out the treatment at a determined health service. This occurred in program C.
The internal service organization itself can also affect resource use, since it lacks a systematic planning
of the number of patients to be supervised for daily MIO. Other factors affecting appropriate resource use
includes delays in the professionals’ departure from the health service or the car arriving to the service late,
and the lack of a professional specifically assigned to carry out the DOT at the time planned. Carrying out the
DOT demands reorganizing the service’s internal
activities, both due to the need of a minimum structure (car, driver and assigned health professional supervisor)
to develop the activities related to TB patient home treatment, and to guarantee the continuation of activities
performed within the health service. This reorganization takes place through the availability of human and
material resources available in the health service and the patient’s and family’s needs.
Both the lack of resources to perform the DOT and the non-systematization of activities related to
the DOT cause delays in the professional’s departure
from the health service to visit the patient’s home. Therefore, there is a reduction in the time to carry
out DOT activities, which can affect the quality of the care provided to the TB patient.
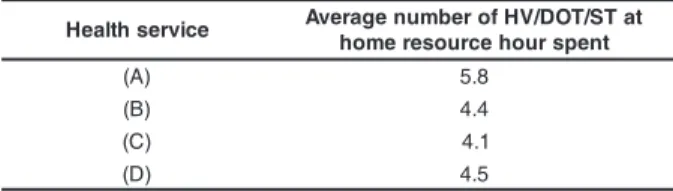
Regarding the indicator performance
quickness, the study found that, of the four programs,
program A presented a higher average number of
home visits (5.8), as observed in the following table.
Table 3 - Average number of home visits per health
unit according to DOT/ST resource hour spent
e c i v r e s h t l a e
H AveragenumberofHV/DOT/STat t n e p s r u o h e c r u o s e r e m o h )
A
( 5.8
) B
( 4.4
) C
( 4.1
) D
( 4.5
Program C had the smallest number of home
visits (4.1). This is likely due to the large territory
dimension of the health unit covered by the program.
This situation demands more transportation time to
supervise patients living in distant neighborhoods, and
implies that the program’s health team sometimes
performs the supervision of patients belonging to other
areas.
Program A covered the smallest territory.
This explains the greater number of home visits
observed in the program, compared to the other
programs, since the houses were located in the same
neighborhood or blocks, or patients lived in the same
household (three families). Thus, it is observed that
facilitators regarding the supervision of a greater
number of patients could be the size of the territory
and the proximity of the health service to the homes.
It is also important to state longer resource
utilization times represent a longer period for the
health professional to visit patient homes. Therefore,
the lack of performance quickness in program C can
also be attributed to the shorter time of resource
utilization in this program.
Other factors affecting performance quickness
can be related to DOT coverage and frequency.
Therefore, the program with the greatest number of
patients in DOT at home with daily supervision will
also have the greatest number of visits.
Regarding the monitoring of medication
administration, program A reached a greater
percentage of visits with medicine intake observation
(77.4%), as observed in the following chart:
Table 4 - Percentage of home visits with medicine
intake observation by Tuberculosis Control Program
in the city of Ribeirão Preto, SP, 2003
e c i v r e S h t l a e
H NumberofHVwithMIO/numberofHV O
I M r o f
) A
( 77.4%
) B
( 54.8%
) C
( 66.0%
) D
The low percentage of visits with MIO found
is due to the absence of the patient at the moment of
the home visit. In program A, 39.9% of patients were
absent during the visit, in program B: 40.0%; C:
56.4%; D: 100.0%. It is important to note that it is
considered a visit with MIO only when the professional
effectively observed the patient ingesting the
medicine.
The failures to find the patients at the moment
of the visits can be related to the limited visiting time,
the house supervision planning which does not take
into account the preferences/needs of the patient and
his or her social-cultural environment. Health care
must consider the needs and preferences of the
patients to facilitate the access and treatment
compliance(12).
A study carried out in a large city in the State
of São Paulo, regarding the patient’s perception about
the DOT at home, showed the dependence on the
visiting schedule for MIO of the health professional
as a weakness of DOT. This situation could be
improved if other social entities were included in the
therapeutic process (patient’s family, cured patients,
members of the community, and others(13)).
It is important to state that the monitoring of
medicine intake, in the studied city, privileges the MIO.
However, other complementary activities are carried
(delivery of incentives, health surveillance, request
of baciloscopy control, contact evaluation,
psychosocial support, and others). These activities
are fundamental for the patient’s compliance within
the family context, once home supervision involves
the interaction with a bio-psycho-social reality,
including the cultural repertory and magical-religious
beliefs of each family member(14). This interaction
usually determines and limits the degree of
co-responsibility of the patient and his or her family with
health care. It is necessary for health care
professionals, administrators and educators to change
their way of thinking and acting aiming to provide
comprehensive and humanistic care.
It is fundamental to advance to an
inter-disciplinary approach and to explore psychological and
social-cultural determinants of the disease. This would
help to develop appropriate and effective
interventions to detect cases and treatment, looking
at the patient within the community’s context and
making them motivated to solve the health problems,
instead of being concerned exclusively with the search
for better ways to control medicine intake(15) .
The current health models for the control of
infectious diseases, including TB, are specifically and
vertically directed to the disease, focusing only on
the short term results (cure rates) as opposed to health
promotion. Disease control remains a priority
exclusive to the health field. Other political and social
sectors are not necessarily deemed relevant to the
control of infectious diseases(16).
Regarding the indicator time spent per home
visit in the programs. It was observed that the time
was longer in program C (14.7 minutes), and shorter
in program A (10.4 minutes). The longer time spent
per home visit in program C may have happened due
to the longer resource time available in this program.
The shorter time spent observed in program A can
be explained by the smallest resource utilization time
(88.5%) of this program.
Human and material resource time available
is an important factor to perform the DOT at the
patient’s home, considering the need to establish a
connection and co-responsibility between the health
care professional and the patient/family. This allows
for a different approach to other problems and/or
needs that go beyond the therapeutic plan. It is
important to state that the success of these activities
can be related to the time within which they are
operated. Having more time to carry out home visits
can provide better conditions for the planning and
development of activities in the DOT, including the
patient’s, family’s and community’s education itself.
Thus, they can become multipliers of knowledge for
an active participation in the development of health
actions to control the disease.
CONCLUSIONS
The study enabled the creation and use of
some specific indicators related to resource use,
performance quickness, monitoring medication
administration, and time spent per home visit. It
enabled a closer analysis of the performance of the
Tuberculosis Control Programs that carried out the
DOT at home, as well as to understand some aspects
of the management and organization of the health
care services that use the DOT strategy in TB control.
The results show that program B had a better
performance regarding resource use; program A
achieved better performance in quickness and
per home visit, program C showed the longest time.
Note that higher and lower performance do not
necessarily mean better or worse quality in the service
provided, rather it is the numerical expression of the
way resources are being used and if home visits are
reaching their goal.
The availability of human and material
resources in the health service affected their
optimization, as well as the effectiveness of the
activities to follow the patient’s treatment. As a result,
the performance of the Tuberculosis Control Programs
that use the DOT at home were also affected.
Supervision activities are still mainly focused
on the observation of medicine intake. However, it is
important to emphasize that during the development
of this action (it was observed that other activities
were carried out) it is possible to perform
complementary interventions such as epidemic
surveillance actions (search for contacts and
individuals with respiratory symptoms), social support
activities, and others.
Therefore, it is considered relevant to review
the health care practice in the development of this
strategy in order to promote comprehensive care,
emphasizing not only MIO, but also preventive actions
and health protection.
Providing DOT at home requires permanent
qualification and supervision of the professionals
involved in TB patient and family care. In addition,
new knowledge should be obtained for planning and
executing health actions and articulating health care
between the health service and the patient and family.
It is necessary to review the resource
management and health care action plans to provide
DOT at home with the objective of using the available
resources in a rational fashion, and assure access to
different levels and services of the health system that
meet the social, cultural and economic needs of the
TB patient/family.
Finally, the adoption of the DOT at home must
consider the location of the service, the work organization
of the team responsible for the treatment, planning,
systemizing supervision activities, and administrating the
service needed to assure the optimization of human and
material resources in the program as well as the fulfillment
of the supervision activities.
REFERENCES
1. Davies PD. The role of DOTS in tuberculosis treatment and control. Am J Respir Med 2003; 2(3):203-9.
2. Morrone N, Solha MS, Cruvinel MC, Morrono N Junior, Freire J AS, Barbosa ZLM. Tuberculose: tratamento supervisionado “versus” tratamento auto-administrado. J Pneumol 1999; 25(4):198-206.
3. Muniz JN, Villa TCS. O impacto epidemiológico do tratamento supervisionado no controle da tuberculose em Ribeirão Preto (1998-2000). Bol Pneumol Sanit 2002; 10(1):49-54. 4. Hino P, Santos CB, Villa TCS, Muniz JN, Monroe AA. Tuberculosis patients submitted to supervised supervised treatment. Rev Latino-am Enferm 2005 janeiro-fevereiro; 13(1):27-31. 5. Kamolratanakul P, Sawert H, Lertmaharit S, Kasetjaroen Y, Akksilp S, Tulaporn C, et al. Randomized controlled trial of directly observed treatment (DOT) for patients with pulmonary tuberculosis in Thailand. Trans R Soc Trop Med Hyg 1999 September-October; 93(5):552-7.
6. Bertollozi MR. A adesão ao tratamento da tuberculose na perspectiva da estratégia do tratamento diretamente observado (DOTS) no município de São Paulo-SP. Tese (livre docência). São Paulo: Escola de Enfermagem/USP; 2005. 7. Kaona FAD, Tuba M, Siziya S, Sikaona L. An assessment of factor contribuing to treatment adherence and knowledge of TB transmission among patients on TB treatment. BMC Public Health 2004 December; 4:68.
8. SinghV, Jaiswal A, Porter JDH, Ogden JA, Sarin R, Sharma PP, et al. TB control, poverty, and vulnerabilitity in Delhi, India. Trop Med Int Health 2002 August; 7(8):693-700. 9. Donabedian A. The definition of quality and approaches to its assessment. Michigan: Health Administration Press; 1980. 10. Tanaka O, Melo C. Avaliação de Programas de Saúde do Adolescente: um modo de fazer. São Paulo(SP): Edusp; 2001. 11. Starfield B. Atenção Primaria: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: Ministério da Saúde, Unesco; 2002.
12. Volmink J, Matchaba P, Gamer P. Directly observed therapy and treatment adherence. Lancet 2000 April; 355(9212):1345-50.
13. Vendramini SHF, Villa TCS, Palha PF, Monroe AA. Tratamento supervisionado no controle da tuberculose em uma unidade de saúde de Ribeirão Preto: a percepção do doente. Bol Pneumol Sanit 2002 janeiro-junho; 10(1):5-12. 14. Monroe AA, Cardozo-Gonzales RI, Sassaki CM, Ruffino-Netto A, Villa TCS. Gerenciamento de caso ao doente/família com tuberculose: uma estratégia de sistematização do cuidado no domicílio. J Bras Pneumol 2005 janeiro-fevereiro; 31(1):91-2. 15. Lienhartdt C, Ogden JA. Tuberculosis control in resource - poor countries: have we reached the limits of the universal paradigm? Trop Med Int Health 2004 July; 9(7):833-41. 16. Porter J, Ogden J, Pronyk P. Infectious disease policy: towards the production of healh. Health Policy Plan 1999 December; 14(4):322-8.