w w w . r b o . o r g . b r
Original
Article
Giant-cell
tumor:
analysis
on
the
importance
of
early
diagnosis
and
the
epidemiological
profile
夽
Diego
Firmino
de
Carvalho
Diniz
Ferraz
∗,
César
Augusto
Torres
dos
Santos,
Victor
Hugo
Farias
Costa,
Antônio
Marcelo
Gonc¸alves
Souza,
Paulo
Rogerio
Gomes
Lima
ServiceofOrthopedicsandTraumatology,HospitalOtáviodeFreitas,Recife,PE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10October2014
Accepted5March2015
Availableonline5January2016
Keywords:
Giant-celltumors/diagnosis
Giant-celltumors/epidemiology
Giant-celltumors/therapy
a
b
s
t
r
a
c
t
Objective:Thisstudyaimedtoascertaintherelationshipbetweenearlydiagnosisof
giant-celltumors(GCT)andtheirprognosis,bycorrelatingthetimeofsymptomonsetwiththe
stagingoftheinjury(throughtheCampanacciclassificationatthetimeofdiagnosis),and
withthetypeoftreatment.Thesecondaryobjectiveofthestudywastooutlinethe
epi-demiologicalprofileofpatientswithGCTintheregionwherethedataweregathered,and
tocomparethemwithdataintheliterature.
Methods:Theauthorspresentanevaluationon61patientsdiagnosedwithboneGCT,with
regardtothesiteofinvolvement,age,initialsymptoms,timeofsymptomonset,
classi-ficationandtypeoftreatment,amongpatientsattendedbetweenMay1994andAugust
2009.
Results:ThethresholdindicatedasthelimitforCampanaccistageItumorstobethe
com-monestdiagnosis,witha98.2%chancethatthetreatmentwouldbenon-aggressive,was
2monthsaftersymptomonset.Thisfindingwasstatisticallysignificant(p=0.017).Every
additionalmonthincreasedthechancethatapatientwouldbediagnosedwithan
advanced-stagetumorby10.94%,inrelationtothechancesofhavingtheothertwostages ofthe
tumor.
Conclusion:Thestudyresultnotonlysuggeststhatthealternativehypothesisthattheearlier
thediagnosisofGCTis,thelessseverethelesionwillbe,hasbeenconfirmed;butalso
espe-ciallypredictstherelationshipbetweenthetimeofsymptomappearanceandtheseverity
ofthetumor.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.Allrightsreserved.
夽
WorkperformedintheHospitaldoCâncerdePernambuco,Recife,PE,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](D.F.deCarvalhoDinizFerraz).
http://dx.doi.org/10.1016/j.rboe.2015.12.012
Tumor
de
células
gigantes:
análise
sobre
importância
do
diagnóstico
precoce
e
perfil
epidemiológico
Palavras-chave:
Tumoresdecélulas
gigantes/diagnóstico
Tumoresdecélulas
gigantes/epidemiologia
Tumoresdecélulas
gigantes/terapia
r
e
s
u
m
o
Objetivo:Presumirarelac¸ãoentreodiagnósticoprecocedotumordecélulasgigantes(TCG)
eoseuprognóstico,relacionarotempodesurgimentodossintomascomoestadiamentoda
lesão,pormeiodaclassificac¸ãodeCampanaccinomomentododiagnóstico,ecomtipode
tratamento.Oobjetivosecundáriodoestudoétrac¸aroperfilepidemiológicodospacientes
comTCGdaregiãoondeforamcolhidososdadosecompará-locomdadosdaliteratura.
Métodos: Avaliac¸ãode61pacientesdiagnosticadoscomtumordecélulasgigantesósseo
quantoaolocaldeacometimento,idade,sintomatologiainicial,tempodosurgimentodos
sintomas,classificac¸ãoetipodetratamentoempacientesatendidosentremaiode1994e
agostode2009.
Resultado: Apontaomarcodedoismesesapósoiníciodasintomatologiacomodatalimite,
quandoseriamaiscomumodiagnósticodetumorestágioIdeCampanacciecom98,2%de
chancedesertratadodemodonãoagressivo,dadoscomrelevânciaestatística(p=0,017).A
cadaaumentodeummêsachancedeumpacienteserdiagnosticadocomtumoremestágio
avanc¸adoé10,94%maiordoqueemrelac¸ãoaosoutrosdoisestágiosdotumor.
Conclusão:Oresultadodoestudosugerenãosomenteaconfirmac¸ãodahipóteseopcionalde
quequantomaisprecoceodiagnósticodeTCG,menosgraveéalesão,mas,principalmente,
predizarelac¸ãodotempodesurgimentodosintomacomagravidadedotumor.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Todososdireitosreservados.
Introduction
Bone giant-cell tumors (GCTs) are benign mesenchymal
neoplasmswith aggressivecharacteristics. Histologically,it
is known that GCTs were first described by Cooper apud
McCarthy1andwereconsideredtobe“fungalmedullary
exos-toses”.In1845,Lebertetal.apudMcCarthy1describedagroup
ofbonetumorswithgiantmultinucleatedcellsthatpresented
atendencytorecur,butwhichcouldbecuredthrough
ampu-tation.HistopathologicalevaluationsonGCTsrevealthatthey
are formed by vascularized tissue consisting of stroma of
fusiformorovoidcellsandbythepresenceofnumerous
mul-tinucleatedgiantcellsthatresembleosteoclasts.Theypresent
characteristicscommontomanydifferenttumoraland
pseu-dotumorallesions,andanalysistogetherwiththeclinicaland
imagingcharacteristicsisneededinordertoconfirmthe
diag-nosis.
Accordingto aseries attheMayo Clinic,2 these tumors
accountfor5%ofboneneoplasmsandareslightlymore
preva-lentinfemales.Theagegroupmostaffectedisbetweenthe
secondandfourthdecadesoflife.GCTsgenerallyaffecta
sin-glebone.Thecommonestsitesaffectedarethedistalfemur,
proximaltibiaanddistalradius.
The clinical condition consists of progressive pain and
increased joint volume, which may be associated with
joint symptoms such as mechanical blocking and
synovi-tis.These symptoms are often initially related to physical
activity and the pain only rarely becomes incapacitating.
A diagnosis of GCT is suspected when, in addition to the
abovementioned clinical condition, radiographic evaluation
reveals a tumorofosteolyticappearance that destroys the
entireepiphysisand mayreachasfarasthejointcartilage
(characteristicsofaggressivenessintheradiological
evalua-tion).Thediagnosis isconfirmedthroughhistopathological
analysis.
In1990,Campanaccietal.3presentedaradiographic
clas-sificationforGCTsthatdescribesthreedifferentgrades:stage
1–small,quiescentandintraosseouslesions;stage2–active
oraggressivetumors,withcompromisedbonecortex,but
pre-sentingintactperiosteum;stage3–aggressive,withinvasion
ofadjacentsoftissues.
Historically,thetreatmentconsistedofsimplecurettage,
but this method was shown to give rise to a high
recur-rencerate.Currently,thetechniquesmostusedarecurettage
withadjuvanttherapy,resectionoftheaffectedsegmentwith
fusion-likereconstructionorauto/homograftreplacementor
useofendoprostheses.
Nonspecific initial symptoms, lack of medical training
directedtowardprimarycareanddifficultyinaccessing
refer-ralhospitalsmakesithardertoachieveearlydiagnosisand
adequatetreatmentforGCTs.Thepresentstudyhadtheaims
ofevaluatingtherelationshipbetweenearlydiagnosisofGCT
and its prognosis and correlatingthe lengthoftime since
symptomsappearedwiththestagingofthelesion,bymeans
oftheCampanacciclassificationatthetimeofdiagnosis,and
withthetypeoftreatment.Thisstudyalsohadthe aimof
establishing time markers for early diagnosis of GCT that
would becapableofallowingthe assumptionoflow
sever-ity ofthe lesion,withthe needforless aggressivetypesof
treatment,andservingasaguideforpublicpoliciesfor
Material
and
method
In September 2014, a cross-sectional descriptive study
was conducted among patients at the Cancer Hospital of
Pernambuco.Allthemedicalfilesofpatientswhohadbeen
diagnosedwithGCTbetweenMay1994andAugust2009were
reviewed.Patientswithsoft-tissueGCT;patientshospitalized
duetotumorrecurrence;casesinwhichthetimethathad
elapsedbetweentheonset ofsymptomsand thediagnosis
recordswasnotmentioned;andrecordswithconflictingor
incompletedata,i.e.absenceofhistopathological
confirma-tion,illegibleinformation,incompleteadmissionformsand
non-explanatory surgicaldescriptions, were excluded from
thedata-gathering.
Throughexcludingthegroupscitedabovefromthe
data-gathering,61patientswereselected.Thesecaseshadmedical
filesthathadbeenfilledoutlegibly,withtheabovementioned
information complete and non-conflicting. The following
informationwassoughtinthesemedicalfiles:timeelapsed
between the onset of symptoms and the tumor diagnosis
at the referral oncological hospital; site of tumor
involve-ment;patient’sage;patient’splaceoforigin;typeoftreatment
implemented;Campanacci classificationonadmission;and
symptomspresentedduringtheattendance.Theprocessof
clinicalinvestigation,lesionclassificationandtreatmentwas
implementedbyqualifiedprofessionalswhoweremembers
oftheBrazilianSocietyofOncologicalOrthopedics.
Thesamplewasclassifiedinaccordance withthe
Cam-panaccisystemandwasdividedintotwogroupsrelatingto
thetreatment required.Thepatientswith GCTsthatcould
beresected through curettagewith adjuvant therapy were
groupedas“non-advanced”cases,whilethosewhorequired
interventionsthatweremore“aggressive”wereconsideredto
be“advanced”cases.
Thisstudywassubmittedtotheethicscommitteeofthe
healthcareinstitutionindicatedthroughtheBrazilplatform,
forauthorization.
Statistical
analysis
Theresultsfromthequantitativevariableswereexpressedas
meansand standarddeviations, whilethe resultsfromthe
qualitativevariableswereexpressedasabsoluteandrelative
frequencies.TheKruskal–Wallis testwas usedtoascertain
possibledifferencesinmeantimetakenfortreatmentandin
patientage,inrelationtotumorstage.Alogisticregression
modelwasusedtocorrelatethetimetakenfortreatmentand
thetumorstage.
Results
ThemeanageamongthepatientswithatumorinCampanacci
stageIwas38.3± 13.7years,whilethoseinstageIIpresented
ameanof29.5± 10.6years.PatientswithastageIIItumor
pre-sentedameanof34.1± 13.9years.Itwasseenthattherewas
nostatisticallysignificantdifferenceinmeanageinrelation
totumorstage(p=0.311)(Table1).
Table1–Comparisonofmeanagesandlengthsof follow-upinrelationtotumorstage.
Tumorstage(mean±SD) p-value
I II III
Age(years) 38.3±13.7 29.5±10.6 34.1±13.9 0.311 Time(months) 1.5±0.5 6.4±0.8 10.4±2.1 0.017a
a Statisticallysignificant.
ThepatientswithstageItumorspresentedameantime
takenuntilthediagnosisof1.5± 0.5months.Thosewithstage
IItumorspresentedameanof6.4± 0.8monthsandthosewith
stageIIItumors,10.4± 2.1months.Itwasobservedthatthere
weresignificantdifferencesinthetimetakenuntilthe
diag-nosis, inrelationtothetumorstage(p=0.017),i.e.patients
attheinitialstagepresentedshortertimestakentomakethe
diagnosisthanthoseatadvancedstagesofthetumor(Table1).
ItwasseenthatpatientsinstageIpresentedshortertimes
tomakethediagnosisthanthoseinstagesIIandIII:p<0.0001
and<0.0001,respectively(Fig.1).
Itwasseenthatthetimetakentomakethediagnosisfor
patientswithstageIIItumorswaslongerthan thetimefor
patientswithstageII:p=0.013(Fig.1).
Through logistic regression analysis (Eq. (1)), it was
observed that forevery 1-month increase, the chancethat
apatientwouldbediagnosedwithatumorattheadvanced
stagewas10.94%greaterthanattheothertwotumorstages.
log(− log(1− ˘(x)))= −1.64+ 0.1 tempo (1)
where˘(x)istheprobabilitythatapatientwouldbeclassified
ashavinganadvancedstageofthetumor.
Itwas seenfrom Table 2thatpatients withatimeof1
monthtakentomakethediagnosispresentedaprobability
of0.5%ofbeingclassifiedashavinganadvancestageofthe
tumor,whileifthissamepatientweretobediagnosedonly
in the fifthmonth, this probability would be13.7%. If this
samepatientweretobediagnosedonlyafter12months,this
probabilitywouldbe81.5%.
Initial 35
30
25
20
15
10
5
0
Length of follow-up (months)
Intermediate Advanced
Tumor stage
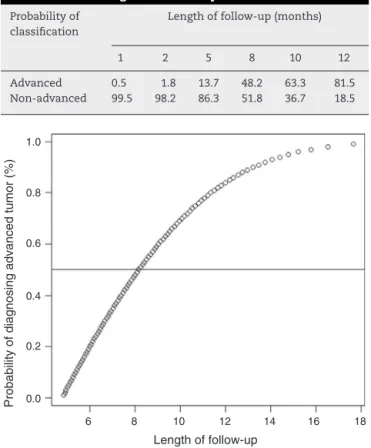
Table2–Probabilityoftumorstageclassification,in relationtothelengthoffollow-up.
Probabilityof classification
Lengthoffollow-up(months)
1 2 5 8 10 12
Advanced 0.5 1.8 13.7 48.2 63.3 81.5 Non-advanced 99.5 98.2 86.3 51.8 36.7 18.5
Length of follow-up
Probability of diagnosing advanced tumor (%)
6 0.0 0.2 0.4 0.6 0.8 1.0
8 10 12 14 16 18
Fig.2–Probabilityoftumorclassificationinanadvanced stage,inrelationtothetimetakentomakethediagnosis.
ItwasseeninFig.2thatapproximately20%ofthepatients
wereclassifiedwaspresentinganadvancedstageofthetumor
inthe sixth month. Inthe eighth monthofthe follow-up,
approximately 50%ofthe patients presentedtumorsatan
advancestage,while80%ofthepatients wereclassified as
presentinganadvancedstageofthediseasearoundthe11th
month.
Table3presentstheprevalencesofsymptomsamongthe
patientsstudied.Itshowsthatpainalonewasthecommonest
symptomandtumorformationwasthecommonestclinical
sign.
TheincidenceofGCTsaccordingtotheirlocation inthe
skeletonispresentedinTable4,whichshowsthattheyaffect
theepiphysesoflongbones,mostcommonlyattheknee.In
Table3–Prevalenceofsymptoms.
Symptoms N %
Pain 28 46.7
Tumorformation 17 28.3
Painandtumorformation 4 6.7
Increasedvolume 4 6.7
Painandincreasedvolume 2 3.3 Pathologicalfracture 2 3.3 Painandpathologicalfracture 2 3.3
Edemaandpain 1 1.7
Table4–IncidenceofGCTaccordingtolocationin skeleton.
Siteofinvolvement No.ofpatients Percentage
Distalfemur 20 32.78%
Proximal 7 11.47%
Distaltibia 6 9.83%
Distalradius 6 9.83%
Phalanges 5 8.19%
Others 17 27.86%
additiontotheseregions,GCTshavealsobeenfoundinthe calcaneus,proximalhumerus,ulna,hopandproximalradius.
Discussion
Theresultsfromthisstudysuggestnotonlythatithas pro-videdconfirmationoftheoptionalhypothesisthattheearlier thediagnosis ofGCTismade,thelowertheseverityofthe lesionwillbe,butalsoespecially,thatthispredictsthe rela-tionshipbetweenthetimeofsymptomonsetandtheseverity ofthetumor.Forexample,inpatientswhoarediagnosed1 monthaftersymptomsfirstappear,theirchanceofpresenting alesionthatcanbetreatedthroughcurettageplusadjuvant treatment99.5%,whichhasbenefitsbothforthepatientand forthepublichealthcaresystem,incomparisonwithsurgical proceduresthataremoreaggressive.
GCTs were found in our series of 61 patients mostly betweentheirthirdandfourthdecadesoflife,andthisfinding isinlinewiththedataintheliterature.3–5Unlikeastudy6in
which31%ofthepatientswerediagnosedwithpathological
fractures,wefoundinourseriesthatonly3.3%ofourpatients
hadsuchlesions.
Theobservationthat onlyonepatientinourstudy
pre-sented metastasis (1.6%)is concordantwith theworldwide
literature,2,7 inwhichithasbeenestimatedthattheriskof
metastasisfromGCTisbetween1and3%.AccordingtoRenard
etal.,8theexplanationforthemetastaticfociliesinthefact
thattumorcellsmaybefoundinperipheralvesselsofthebone
siteaffected.
ComparingtheincidenceofGCTsregardingtheirlocation
intheskeletonwithwhatwasdemonstratedbyJesus-Garcia
etal.,6weobtainedsimilardata,ascanbeseeninTable4.The
kneeisthelocationofhighestincidenceandaccountsfor44%
ofthecases.
Withtheaimofestablishingtimemarkersforearly
diag-nosisincasesofGCT,the objectivethatwastaken onwas
toidentifylesionsclassifiedasCampanaccistageIorIIthat
itwouldbepossibletotreatthroughcurettageplusadjuvant
therapy,whichwere groupedasnon-advancedcasesinthe
statistical analysisofthis study.Theresultsshowed thata
timemarkerof2monthsaftertheonsetofsymptomswasthe
timelimitfortheperiodinwhichthecommonestdiagnosis
wouldbeaCampanaccistageItumor,witha98.2%chanceof
beingcapableofnon-aggressivetreatment.Thisfindingwas
statisticallysignificant(p=0.017).
In ordertoreach thetime markerdemonstrated inthis
study, improvements in public healthcare policies will be
needed.Investmentinhumanandstructuralresourceswithin
regularizationofrapidpassagebetweenprimarycareand
spe-cialistunitsforoncologicaltreatmentarewaysofmakingthe
publichealthcaresystemcapableoftimelydiagnosisforGCT
cases.
Thepresentstudy foundthattherewashighprevalence
of generic signs and symptoms, which caused difficulty
regardingclinicalsuspicionandearlydiagnosis.Thepresence
ofjointpainand/ortumorformationwasshowntobeasign
ofsuspicionforinvestigatingpossibleGCTs.
Fromanalysisontheresultobtainedregardingmeanage
inrelationtolesionseverityatthetimeofdiagnosis,itwas
concluded that there was no statistical significance.Thus,
symptoms thatare highly prevalent amongolder patients,
suchasjointpain,needtobebetterinvestigated.Likewise,in
attendingyoungerpatients,tumoretiologyneedstobenoted,
giventhatthedataobtainedinseveralstudieshave
demon-strateditsimportanceforearlydiagnosis.
Conclusion
Thisstudy demonstrated that the mark of2months after
symptomonsetwasthetimelimitfortheperiodinwhicha
diagnosisofCampanaccistageItumorswouldbemore
com-mon, with a98.2% chanceof onlyneeding non-aggressive
treatment.Thisfindingwasstatisticallysignificant(p=0.017).
Withevery1-monthincrease,thechancethatapatientwould
bediagnosedwithatumoratanadvanced stageis10.94%
greaterthaninrelationtotheother twotumorstages.The
epidemiologicalprofileofpatientswithGCTinthisregionis
concordant withthe datainthe worldwideliterature,with
regardtoage,riskofmetastasisandsiteaffected.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.McCarthyEF.Giant-celltumorofbone:anhistorical
perspective.ClinOrthopRelatRes.1980;(153):14–25.
2.CanaleST.CirurgiaortopédicadeCampbell.10thed.SãoPaulo:
Manole;2006.
3.CampanacciM,BaldiniN,BorianiS,SudaneseA.Giant-cell
tumorofbone.JBoneJointSurgAm.1987;69(1):106–14.
4.López-BareaF,Rodríguez-PeraltoJL,García-GirónJ,
Guemes-GordoF.Benignmetastasizinggiant-celltumorofthe
hand.Reportofacaseandreviewoftheliterature.ClinOrthop
RelatRes.1992;(274):270–4.
5.EckardtJJ,GroganTJ.Giantcelltumorofbone.ClinOrthop
RelatRes.1986;(204):45–58.
6.GarciaFilhoRJ,WajchenbergM,JustinoMAF,KorukianM,
IshiharaHY,PonteFM.Tumordecélulasgigantes.Análiseda
invasãoarticular,fraturapatológica,recidivalocalemetástase
paraopulmão.RevBrasOrtop.1997;32(11):849–56.
7.GarciaFilhoRJ.Diagnósticoetratamentodetumoresósseos.
RiodeJaneiro:Elsevier;2005.
8.RenardAJ,VethRP,PruszczynskiM,WobbesT,LemmensJA,
vanHornJR.Giantcelltumorofbone:oncologicand