rev bras hematol hemoter. 2017;39(1):28–31
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Cholelithiasis
and
its
complications
in
sickle
cell
disease
in
a
university
hospital
Raquel
Alves
Martins
∗,
Renato
Santos
Soares,
Fernanda
Bernadelli
De
Vito,
Valdirene
de
Fátima
Barbosa,
Sheila
Soares
Silva,
Helio
Moraes-Souza,
Paulo
Roberto
Juliano
Martins
UniversidadeFederaldoTriânguloMineiro(UFTM),Uberaba,MG,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17April2016 Accepted9September2016 Availableonline20October2016
Keywords:
Sicklecelldisease Chronichemolysis Cholelithiasis Treatment
a
b
s
t
r
a
c
t
Introduction:Theclinicalmanifestationsofsicklecelldiseasearerelatedtothe polymer-izationofhemoglobinS.Thechronichemolysiscausedbythisconditionoftencausesthe formationofgallstonesthatcanmigrateandblockthecommonbileductleadingtoacute abdomen.
Objective:Thisstudyaimedtoevaluatetheprofileofpatientswithsicklecelldiseaseand cholelithiasis.
Methods:Patientswithsicklecelldiseasewereseparatedintogroupsaccordingtothe pres-enceorabsenceofcholelithiasis.Socioepidemiologicalandclinicalcharacteristics,such asgender,age,useofhydroxyureaandthepresenceofotherhemoglobinopathieswere researchedinthemedicalrecordsofpatients.
Results:Ahundredandsevenpatientswithsicklecellanemiaweretreatedattheinstitution. Ofthese,27(25.2%)hadcholelithiasis.Thepresenceofcholelithiasiswashigherinthe11–29 agegroupthaninyoungerthan11yearsandover29years.Noassociationwasfoundfor thepresenceofcholelithiasiswithgender,useofhydroxyureaortypeofhemoglobinopathy (hemoglobinSS,hemoglobinSCorsicklebeta-thalassemia).Sixteenofthepatientshadto besubmittedtocholecystectomywith14ofthesurgeriesbeingperformedbylaparoscopy. Complicationswereobservedinthreepatientsandonepatientdiedforreasonsunrelated tothesurgery.
Conclusion:Aquarterofpatientswithsicklecelldiseasehadgallstones,morecommonly inthe11-to29-yearagerange.Patientsshouldbemonitoredfromchildhoodtoprevent cholelithiasiswithpreoperative, intra-operativeandpostoperative carebeing crucialto reducetheriskofcomplicationsinthesepatients.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthorat:Av.GetulioGuarita,250,BairroAbadia,38025-440Uberaba,MG,Brazil.
E-mailaddress:[email protected](R.A.Martins).
http://dx.doi.org/10.1016/j.bjhh.2016.09.009
revbrashematolhemoter.2 0 1 7;39(1):28–31
29
Introduction
Sicklecellanemiaiscausedbyamutationinchromosome11 thatresultsinthereplacementofglutamicacidwithvaline atposition6oftheN-terminusoftheglobinchain.The clini-calmanifestationsofsicklecelldiseasearedirectlyassociated withconformationchangesinhemoglobin(Hb).In deoxygen-ationevents(hypoxia,dehydration,stress,lowtemperature, acidosis, infection),because of the sickle shape ofthe red bloodcells(hencethename),HbSbecomesrelatively insolu-bleandaggregatesintolongpolymers.1–4
Approximately3500peopleareestimatedtobebornwith sickle cell disease in Brazil every year, with an estimated 25,000–30,000peoplehavingsickle cellanemiaand atleast 7,200,000peoplecarryingthesicklecelltrait.Theprevalence ofcarriersofsicklecell traitrangesfrom 2%inthegeneral populationto6–12%inAfricandescents.5
Asthecells are abnormal,theyhaveashorterlifethan normalredbloodcells.Chronichemolysisleadsto continu-ousproductionofbilirubin,whichisconjugatedintheliver andexcretedinthefecesasurobilinogen;inlargequantities, itmayformcalciumbilirubinategallstones.Cholelithiasiscan bedetectedeveninunderfive-year-oldchildren,butitismore commoninadolescents andadultswithsicklecellanemia. Gallstone migrationcan blockthe common bile duct lead-ingtoacuteabdomen.Becauseofthepotentialcomplications andseverityofthiscondition,earlydiagnosisisofparamount importance.Diagnosticimagingmethodsplay amajorrole whenmanagingpatientswithsicklecellanemia,particularly whenevaluatingcomplications.Earlydiagnosisand appropri-atetreatmentincreasesurvivalandimprovethequalityoflife ofpatientswithsicklecellanemia.6–8
Thisstudyaimedtoevaluatetheprofileofpatientswith sicklecelldiseaseandcholelithiasis,theincidenceofcasesat theFundac¸ãoHemominasinUberaba(FHU)andthe Hospi-taldasClínicasofUniversidadeFederaldoTriânguloMineiro (HC/UFTM)andtheimportanceofearlydiagnosisforproper treatment.
Methods
This is a retrospective descriptive study. A computerized databasewas usedtoanalyze patientswithsickle cell dis-easereferredtotheFHUandtothe HC/UFTMfrom1995to 2014.Diagnosisofcholelithiasiswasperformedby abdomi-nalultrasoundandtwogroupsofpatientswereformed:with andwithoutcholelithiasis.Thefollowingabsoluteand rela-tivedataregardingsomesocioepidemiologicalcharacteristics werecollected:gender(male,female),age(youngerthan10 years,between10and29years,andolderthan29years),type ofhemoglobinopathy(HbSS,HbS/beta-thal,andHbSC)and useofhydroxyurea.Theclassificationofthe hemoglobinopa-thywasperformedbyelectrophoresisoncelluloseacetateat alkalinepH.
Thedatawasfirstsubmittedtoananalysisofabsolute fre-quenciesandpercentages,andwereorganizedintables.An OddsRatiowascalculatedinordertostudytheassociation betweenthecharacteristics ofinterest.Thelevelof signifi-canceforalltestswassetat5%,andthedatawereanalyzed
usingthe statisticalsoftwareInStat3.0(GraphPadSoftware Inc,LaJolla,CA,USA).
Results
Onehundredandsevenpatientswithsicklecelldiseasewere followedupintheHematology/HemotherapyServicesofthe HC/UFTM and FHU during the study period. Twentyseven (25.2%)ofthepatientshadcholelithiasis.
Ameanprevalenceof25.2%wasobservedforthediagnoses ofcholelithiasis.Ofthe27cases,17wereinvestigatedbecause ofclinicalsymptoms,whereas tenpatientswerediagnosed duringroutinescreening.
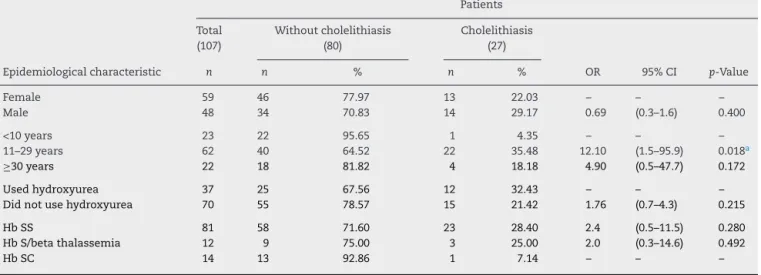
Thepercentageofcholelithiasiswashigherinthe11–29 agegroupthanintheagegroupsyoungerthan11yearsand over29years(p-value=0.018);thevastmajorityofthepatients werediagnosedbefore30yearsofage,withanaverageageat diagnosisof16years.Onlyfourcaseswerediagnosedafter30 yearsold.
There were no significant differences in frequency of cholelithiasisbetweenmalesandfemales(29.3%and22.0%, respectively; p-value=0.400), between the group that used hydroxyurea and thegroup thatdid notuse thismedicine (32.4%and21.4%,respectively;p-value=0.215)andbetween HbSS,HbS/beta-thalandHbSCgroups(28.4%,25.0%and7.1%, respectively,p-value>0.05;Table1).AllHbS/beta-thalpatients wereHbS/beta0.
Sixteenpatients(59%)underwentcholecystectomy, four-teenpatientsunderwentlaparoscopicsurgery,andtwocases underwent open surgery. Although laparoscopy had been startedinoneofthesetwocases,laparotomywithemergency splenectomywasperformedwithsatisfactoryresultsdueto excessivebleeding.Laparoscopyequipmentwasnotavailable atthetimeoftheprocedureoftheotherpatient.
Threecases(18.7%)ofthe16operatedpatientsdeveloped postoperative complications. One caserequired emergency splenectomyduetobleeding,andanotherpatientwasa chole-docholithiasis carrier submitted to endoscopic retrograde cholangiopancreatographyprogressingtoacutepancreatitis. Thepatientwastreatedwithagoodresponseandthen vide-olaparoscopiccholecystectomywasperformedwithoutmajor complications.Onepatientprogressedtodeath30daysafter surgeryduetosplenicsequestration.
Discussion
Cholelithiasiswassignificantlymoreprevalent inthe11–29 age group.These resultssuggestthat this groupshouldbe madeawareoftheriskofgallstones,relatedsymptoms, pos-siblecomplications,andtheneedforregularfollow-upswith routine preventive screenings.However, it should be high-lightedthatdespitehavingfoundahigheroccurrenceinthis group,thescreeningoflithiasissecondarytochronic hemol-ysisshouldbeprovidedtoallpatientswithsicklecelldisease regardless oftheir profileinaccordance withthe Brazilian HandbookofAcuteEventsinSickleCellDisease.9
30
revbrashematolhemoter.2 0 1 7;39(1):28–31Table1–Distributionofpatientswithandwithoutcholelithiasisregardinggender,age,useofhydroxyurea,andtypeof hemoglobinopathyintheHematologyandHemotherapyServiceoftheUniversidadeFederaldoTriânguloMineiro (UFTM).
Patients
Total Withoutcholelithiasis Cholelithiasis
(107) (80) (27)
Epidemiologicalcharacteristic n n % n % OR 95%CI p-Value
Female 59 46 77.97 13 22.03 – – –
Male 48 34 70.83 14 29.17 0.69 (0.3–1.6) 0.400
<10years 23 22 95.65 1 4.35 – – –
11–29years 62 40 64.52 22 35.48 12.10 (1.5–95.9) 0.018a
≥30years 22 18 81.82 4 18.18 4.90 (0.5–47.7) 0.172
Usedhydroxyurea 37 25 67.56 12 32.43 – – –
Didnotusehydroxyurea 70 55 78.57 15 21.42 1.76 (0.7–4.3) 0.215
HbSS 81 58 71.60 23 28.40 2.4 (0.5–11.5) 0.280
HbS/betathalassemia 12 9 75.00 3 25.00 2.0 (0.3–14.6) 0.492
HbSC 14 13 92.86 1 7.14 – – –
OR:OddsRatio;95%CI:95%confidenceinterval.
a Significantdifference.
(<15years).Sixty-three percentwere HbSS, witha statisti-callysignificantpredominance.Nonetheless,thisstudywas performed only inchildren and adolescents and this may havecontributedtothedifferingresults.Itisalsoimportant tonotethat sicklecell diseasehasgreatvariationsin clin-icalpresentation,naturalhistoryandseverityofhemolysis. Somepopulationsmayhavealowerfrequencyof cholelithi-asisbecauseofhaplotypevariations,environmentalfactors, anddifferentclinicalmanagements.6
Theuseofhydroxyureawasnotassociatedwithgallstones. Thiscontradictedourexpectationsasincreasedlevelsoffetal hemoglobincausedbythis medication promoteadecrease inhemolysisofpatientsanditwasexpectedthatthiswould decreasetheformationofgallstones.However,thefindings arenotconclusiveonthispointbecausethestudyhasthe limi-tationofnothavingbeenabletocheckthepatients’adherence totheuseofhydroxyurea.Itwasalsonotpossibletoidentify whetherpatientshadalreadyhadgallstonesbeforetheuseof thismedicine.
This study observed sixteen cases of symptomatic cholelithasis subjected to laparoscopy. The incidence of procedure-related complications was minimal and the vast majority of patients progressed satisfactorily after surgery.7,8Thesurgicalapproachesusedarelaparotomyand
laparoscopy,withmostauthorsconsideringthelattersaferfor patients,withlesscomplicationsrelatedtosurgery,shorter operativetimeandfasterpostoperativerecovery,aswell as a shorterhospital stay.10–14 However, astudy published in
theInternationalJournalofSurgeryin2009foundapositive relationshipbetweenacutechestsyndromeandlaparoscopic surgery.Thestudy stated thatthe pneumoperitoneumand respiratory acidosis secondary to the procedure are pre-dictors of the syndrome and that, in order to minimize the risk, surgery should be performed by an experienced teamwithlessintrabdominalpressureandshorteroperative time.8
Electiveremovalofasymptomaticgallstones,diagnosedby chance,isacontroversialmatter.7,8Mostexperts,similartoin
thehematologyserviceatUFTM,donotrecommendsurgery beforesymptomsappear.Thereisevidencethatthisprofile canbeclinicallymanagedforlongperiods,8,14sothemedical
teamusuallyprescribeantispasmodicagentsforminorpain andrecommendpreventativemeasuressuchasalow-fatdiet forthesepatients.
Episodesofacutecholecystitisoughttobetreated conser-vativelywithantibiotics,analgesia,andgeneralcareuntilthe crisisisover.Cholecystectomyshouldthenbeperformed.7,8
Recently, the National Heart, Lung, and Blood Institute of theUnitedStatesrecommended,fromevidence-based man-agementofsicklecelldisease,thatasymptomaticgallstones should be treated with watchful waiting in children and adults.Inthosewhodevelopsymptomsspecifictogallstones, cholecystectomy should be performed with the laparo-scopic approach being preferred if surgically feasible and available.15
Walker et al. observed a large number of asymp-tomatic patients over25 years offollow-up, andsuggested that research and surgery be indicated only for symp-tomatic patients.16 However, cholecystectomy in
asymp-tomatic patients with sickle cell disease prevents the risk of gallstone crisesin this patient group. Authors advocat-ing prophylacticcholecystectomyclaimthatthis procedure reducesthe riskofcomplicationssuchasacute chest syn-drome,painfulvaso-occlusivecrises,andhepaticandsplenic sequestration associated with cholecystitis crises in sickle cell patients. The authors also note that cholecystectomy in gallstone patients allows the exclusion of this differen-tialdiagnosisinindividualswithrecurrentabdominalpain, thusfacilitatingthediagnosisofabdominalvaso-occlusive cri-sis,which isquite frequentand hassimilarsymptoms.10,16
revbrashematolhemoter.2 0 1 7;39(1):28–31
31
exposespatientstoseveralfactorsthatprecipitatethe sick-lingofredbloodcells,thusfacilitatingtheonsetofasevere hemolyticcrisis.7
Patients with sickle cell disease who are to be submit-ted to anesthetic and surgical procedures require specific care. Conditions associated with these procedures, such as hypoxia, acidosis, hypothermia, infection, hematologic instability and hypovolemia may have particularly serious consequencesforthesepatients.Therefore,inorderto min-imize the risk of these complications, it is recommended that a multidisciplinary preoperative evaluation be per-formed, aswell asspecial attention be givento hydration and oxygenation, and less invasive surgical procedures be chosen, for example, laparoscopic surgery as well as spe-cial postoperative care. Even though patients with sickle cell disease are cared for, morbidity rates are as high as25%.7,8,10
Themajorpostoperativecomplications described are as follows:atelectasis,pneumonitis, pulmonaryinfarctionand infections.7,11–13,17,18 Three ofthe cases(18%)in this study
developed complications. The first case was due to organ damageduringtheprocedurethatrequiredlaparotomyand emergency splenectomy with the patient having a good evolution. In another case, the patient developed acute pancreatitis after endoscopic retrograde cholangiopancre-atography,butprogressedwellandsubsequentlyunderwent laparoscopiccholecystectomy.Finally,inthe thirdcase,the patientdevelopedsplenicsequestration30daysafterthe pro-cedure,wasunresponsivetoclinicalmeasures,andevolved to death. As the incident occurred days after the surgi-cal process, we discarded the association of death with cholecistectomy.
Inpatientswithpainintherightupperabdominal quad-rantitisimportanttoperformdifferentialdiagnosesofviral hepatitis,vaso-occlusivecrisisoftheliver,commonbileduct obstruction,ordrug-inducedhepatotoxicity.Assessmentsof theliverandgallbladdermustbeperiodicallymadeby labo-ratoryandimagingexams(radiographyandultrasound),and thepatientmustbereferredtospecializedservices.14
Conclusion
Thisstudy showedthataprevalenceof25.2%ofgallstones wasobservedinpatientswithsicklecelldiseaseand11-to 29-year-old patientshave a higher incidenceof gallstones. So,patientswithsicklecelldiseaseshouldbemonitoredin specialized centers ona regular basis byundergoing regu-larscreening tests and bypreventing this complication of chronichemolysis.Nonetheless,earlydiagnosis,and preop-erative,intra-operativeandpostoperativecarearemandatory foragoodprogressionofsicklecelldiseaseandforlessriskof complications.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HerrickJB.Peculiarelongatedandsickle-shapedredblood
corpusclesinacaseofsevereanemia.ArchInternMed.
1910;6(5):517–21.
2.DeanJ,SchechterAN.Sicklecellanemia:molecularand
cellularbasesoftherapeuticapproaches.NEnglJMed.
1978;299(14):752–63.
3.KanYM,DozyAM.PolymorphismofDNAsequenceadjacent
tohuman-globinstructuralgene:relationshiptosickle
mutation.ProcNatlAcadSciUSA.1978;75(11):5631–5.
4.AntonarakisSE,KazazianHHJr,OrkinSH.DNA
polymorphismandmolecularpathologyofthehumanglobin
geneclusters.HumGenet.1985;69(1):1–14.
5.Brasil,MinistériodaSaúde.Doenc¸afalciformeeoutras
hemoglobinopatias.MinistériodaSaúde,Secretariade
Atenc¸ãoàSaúde,DepartamentodeAtenc¸ãoEspecializada.
Brasília:MinistériodaSaúde;2011.
6.GumieroAP,Bellomo-BrandãoMA,Costa-PintoEA.Gallstones
inchildrenwithsicklecelldiseasefollowedupataBrazilian
hematologycenter.ArqGastroenterol.2008;45(4):313–8.
7.TrainaF,SaadST.Complicac¸õeshepáticasnadoenc¸a
falciforme.RevBrasHematolHemoter.2007;29(3):299–303.
8.DanD,SeetahalS,HarnananD,SinghY,HariharanS,
NaraynsinghV.Laparoscopiccholecystectomyinsicklecell
diseasepatients:doesoperatingtimematter?IntJSurg.
2009;7(1):70–3.
9.ManualdeEventosAgudosemDoenc¸aFalciforme:SériaA. NormaseManuaisTécnicos.MinistérioSaúde2009.Available from:http://bvsms.saude.gov.br/bvs/publicacoes/manual
eventosagudosdoencafalciforme.pdf.
10.LeandrosE,KymionisGD,KonstadoulakisMM,Albanopoulos
K,DimitrakakisK,GomatosI,etal.Laparoscopicoropen
cholecystectomyinpatientswithsicklecelldisease:which
approachissuperior?EurJSurg.2000;166(11):859–61.
11.Al-SalemAH,NourallahH.Sequential
endoscopic/laparoscopicmanagementofcholelithiasisand
choledocholithiasisinchildrenwhohavesicklecelldisease.J
PediatrSurg.1997;32(10):1432–5.
12.TaggeEP,OthersenHBJr,JacksonSM,SmithCD,GayosoAJ,
AbboudMR,etal.Impactoflaparoscopiccholecystectomyon
themanagementofcholelithiasisinchildrenwithsicklecell
disease.JPediatrSurg.1994;29(2):209–12.
13.MeshikhesAN,al-DhuraisSA,al-JamaA,al-FarajAA,
al-KhatirNS,al-AbkarH.Laparoscopiccholecystectomyin
patientswithsicklecelldisease.JRCollSurgEdinb.
1995;40(6):383–5.
14.MuroniM,LoiV,LionnetF,GirotR,HouryS.Prophylactic
laparoscopiccholecystectomyinadultsicklecelldisease
patientswithcholelithiasis:aprospectivecohortstudy.IntJ
Surg.2015;22:62–6.
15.NationalHeart,Lung,andBloodInstitute.Evidence-Based ManagementofSickleCellDisease:ExpertPanelReport,2014. Bethesda,MD:NationalHeart,Lung,andBloodInstitute,US DepartmentofHealthandHumanServices;2014.Available from: http://www.nhlbi.nih.gov/health-pro/guidelines/sickle-cell-disease-guidelines/
16.WalkerTM,HambletonIR,SerjeantGR.Gallstonesinsickle
celldisease:observationsfromtheJamaicaCohortstudy.J
Pediatr.2000;136(1):80–5.
17.BuckJ,DaviesSC.Surgeryinsicklecelldisease.Hematol
OncolClinNorthAm.2005;19(5):897–902,vii.
18.FriedrichJR.CirugiaeAnestesianadoenc¸afalciforme.Rev