w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Paroxysmal
nocturnal
hemoglobinuria
clone
in
103
Brazilian
patients:
diagnosis
and
classification
Ana
Paula
de
Azambuja
∗,
Mariester
Malvezzi,
Marco
Antonio
Bitencourt,
Michel
Michels
Oliveira,
Larissa
Alessandra
Medeiros,
Ricardo
Pasquini
UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received14May2014 Accepted26November2014 Availableonline30January2015
Keywords: Hemoglobinuria Paroxysmal
Bonemarrowdiseases Flowcytometry
a
b
s
t
r
a
c
t
Background:Paroxysmalnocturnalhemoglobinuriaisanacquiredchronichemolytic ane-mia,whichoftenmanifestsasperipheralbloodcytopeniasandthrombosis.
Objective:TheaimofthisstudyistodescribeaBrazilianpopulationofparoxysmalnocturnal hemoglobinuriapatients.
Methods:Onehundredandthreeparoxysmalnocturnalhemoglobinuriacaseswere retro-spectivelyreviewedandtheclinicalpresentation,thrombosis,survival,andclonesizewere assessed.Diagnosiswasestablishedbyflowcytometry.
Results:Fifty-twomaleand51femalepatientswithamedianageof24.1years(5.5–62years) werestudied.Clinicalsymptomsincludedhemoglobinuria(18.4%),infection(46.6%)and thrombosis(16.5%),and80.6%hadpancytopenia.Patientswereclassifiedasclassic parox-ysmalnocturnalhemoglobinuria(10),paroxysmalnocturnalhemoglobinuriawithaplastic anemia(39),andparoxysmalnocturnalhemoglobinuriawithsubclinicalfeaturesand aplas-ticanemia(54).Thereweresignificantdifferencesintermsofmedianage,sizeofclone, clinicalsymptoms,andperipheralbloodcellcountsbetweenthethreesubcategories.The clonesizeinerythrocytesandgranulocyteswererespectively0.04%(range:0–18%)and7.3% (range:0.3–68.7%)inpatientswithsubclinicalfeaturesandaplasticanemia,15.8%(range: 0–99.7%)and63.0%(range:1.7–99.8%)inpatientswithaplasticanemiaalone,and82.2% (range:0–99.85%)and98.0%(81.3–100.0%)inClassicdisease.Statisticaldifferenceswere identifiedforplatelets(p-value=0.001),lactatedehydrogenase(p-value=0.002)andtheclone size(p-value<0.001)inpatientswhosufferedthromboticeventscomparedtothosewhodid not.Overallsurvivalwas81.7%,withpatientswithsubclinicalfeaturesandaplasticanemia havingloweroverallsurvival(76.5%).
Conclusion:Thisretrospectivereviewof103patientsoveran11-yearperiodrepresentsthe largestcollectionofparoxysmalnocturnalhemoglobinuriacasesfromasinglecenterin Brazil.Flowcytometryshowedthatalargerclonewasassociatedwithclassicalsymptoms andincreasedriskofthrombosis,eveninpatientswithbonemarrowfailure,whereasa smallerclonewasassociatedwithbonemarrowaplasia.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),RuaFlavioDallegrave,1580,apto31B,80045-315
AltodaXV,Curitiba,PR,Brazil.
E-mailaddress:[email protected](A.P.deAzambuja).
http://dx.doi.org/10.1016/j.bjhh.2015.01.001
Introduction
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, acquired, stem cell disorder characterized by hemolytic anemia, bone marrow failure, and an acquired throm-bophilic state.1–4 Manifestations of the disease are related
tocomplement-mediatedintravascularhemolysisduetothe lackofglycosyl phosphatidylinositol-anchoredcomplement regulatory proteins (GPI-AP), CD55and CD59on red blood cells.5,6 Patients with PNH may present not only with a
wide range of clinical manifestations such as weakness, pallor,and asthenia dueto hemolysis, but also abdominal pain,dysphagia,orpulmonaryhypertension.2–4Thrombosis,
oftenoccurringatunusualsites,isamajorlife-threatening risk for patients with PNH.1–4 Ten-year risk of
thrombo-sis has been associated with the PNH clone, as patients withlargePNHclones(>50%)had44% of10-yearrisk com-paredwith5.8%inpatientswithsmall clones.7 Afrequent
association between PNH and aplastic anemia (AA) has been described, with two potential patterns of evolution: progressive marrow failure in patients without detectable PNH clones or AA in patients in whom a PNH clone is detected.8–10
DiagnosisofPNHhasimprovedover theyears withthe adoptionofmoderntechnologies.TwodecadesagotheHam test,whichisbasedonincreasedsensitivityofPNH-affected redbloodcellstocomplement-mediatedlysis,wasused.5,11
Today, the Ham test has usually been substituted by the moresensitive,informativeandlesscumbersomeflow cyto-metricassay (FCM),whichuses antibodies directedagainst theGPI-AP.11–14 PNHcells are characterizedbyGPI-AP
defi-ciency on the cell surface dueto an acquired mutationof the phosphatidylinositol glycan-class A (PIGA) gene inone or more hematopoietic stem cells.6,11,12 The development of
FCM-basedtesting hasallowedthe detectionofsmall PNH clones,whichwouldotherwisenotbeevident.13,15PNHclones
arealsodetectedinthesettingofbonemarrowfailure,and about40–50%ofAApatients haveaPNHclonedetectedat the time of diagnosis.8,15,16 The mechanism by which the
expansionofPNHcells occurs inAAremains unclear;one hypothesisisthatPNHcells haveaproliferativeadvantage overnon-PNHcellsbyanimmuneselectionmechanism.9,10
The presence of a PNH clone has been reported to be predictive of a response to immune suppression in AA15
but other authors did not observe this finding.16 For
opti-mummanagement,thecontributionofbothhemolysisand marrow failure to the complex anemia of PNH should be determined.1
Theobjectiveofthisstudywastoassesstheclinical pre-sentationofPNHpatients atthe timeofdiagnosis,aswell as report complications, such as thrombosis, survival, dif-ference between subcategories and clinical significance of the PNH clone size. Patients were assigned to one of the threesubcategories,namelyClassicPNH,PNH/AAsyndrome, andsubclinicalPNH(PNH-sc/AA)toexplorethedifferences betweenthesecategories.Furthermore,thesizeofPNHclone wasevaluatedintheentirecohortandineachsubcategory toassesswhetherthesizeofPNHcloneswasassociatedwith someoftheclinicalfeaturesofPNH.
Methods
Patientsandstudydesign
OnehundredandthreePNHclonecasesreferredtoatertiary medicalcenterinBrazilfromDecember1999through Decem-ber2011wereretrospectivelyreviewed.Atotalof398patients werescreenedforthePNHcloneusingaFCMassay.5,14The
diagnosisofPNHwasestablishedbydetectingaGPI-AP defi-cientclonegreaterthan0.1%,withatleasttwocelllineages showingGPI deficientpopulations. Thestudy included 103 patientswhohaddemonstratedthepresenceofaPNHclone and had available clinical data. The date of PNH diagno-sis was based on the first positive FCM analysis. Patients withco-morbidAAweresubclassifiedassevereornon-severe accordingtopublishedcriteria.17,18
Multiparameterflowcytometry
ThediagnosisofPNHwasestablishedbythedetectionofan unequivocalpositivePNHclonebymulticolorFCMassay5,11
using a FACSCalibur® cytometer (BD Biosciences, SanJose,
USA)and CellQuest Pro software(BD Biosciences,SanJose, USA).TheproteinsstudiedwereCD55andCD59onredcells, neutrophilsandmonocytes;CD16,CD24andCD66bon neu-trophilsandCD14onmonocytes.PNHclonesweredefinedby thepresenceofGPI-APdeficientcellsatafrequencygreater than 0.1%ofneutrophils,monocytesand redcells,and the proportionofGPI-APdeficientcells(clonesize)wasdefinedby thehighestlevelofthesecellslackingGPI-anchoredproteins. Debris was thresholded out, and at least 50,000 events inleukocytetubesand 20,000eventsinredcelltubeswere collectedand analyzedusingPaint-a-gate® (BDBiosciences,
San Jose, USA)or InfinicytTM (Cytognos, Salamanca,Spain)
software (for samplestested after January 2009). Red cells andgranulocyteswereidentifiedbasedonforwardandside scatter, and bystaining with CD41a FITC and CD45 PercP, respectively.ThegatesusedtodefineGPInegativepopulations wereestablishedbyusingnormalredcellsandgranulocytes ascontrols.
Subcategoriesofparoxysmalnocturnalhemoglobinuria patientsatdiagnosis
Patientswereassignedtooneofthethreesubcategoriesbased ontherecentlyproposedPNHworkingclinicalclassification1:
(I) TheClassicPNHsubcategoryincludedpatientswith clin-icalandlaboratoryevidenceofintravascularhemolysis (suchashemoglobinuria,hemoglobinemia,andelevated LDHandbilirubin)butnoevidenceofbonemarrow fail-ure;
(II) PatientsinthePNH/AAsubcategoryweredefinedbythe presenceorahistoryofbonemarrowfailurein conjunc-tionwithclinicalandlaboratoryevidenceofintravascular hemolysis;
Thecriteriaforbonemarrowfailureincludedbonemarrow hypoplasia(cellularity<50%)andatleasttwoofthe follow-ingthreelaboratoryabnormalities:hemoglobinlevel<12g/dL, absoluteneutrophil count <1.50×109/L, and platelet count (PLT) <100×109/L. Pancytopenia was considered when the threehematopoieticlineageswereaffected.Haptoglobin val-ueswerenotusedinthisstudy.
Statisticalanalysis
Overallsurvival(OS)wascalculatedfromthedateof diagno-sistothedateofdeathorthedateoflastfollow-up.Survival analysiswasperformedusingtheKaplan–Meiermethod.The distributionsofthepresentationofcharacteristicswere com-paredbetweenthethreesubcategoriesandbetweenClassic PNHandPNH-sc/AAbythechi-squaredorFisher’sexacttestas necessaryforcategoricalvariables,andbytheKruskal–Wallis (threesubcategories)orMann–Whitney(twogroups)testfor continuousvariables.ThepercentagesofGPI-APdeficientred bloodcellsandgranulocyteswerecomparedusingStudent’s t-test.Allstatisticalanalyseswereperformedusingthe Statis-ticav.8program.Ap-value<0.05wasconsideredstatistically significant.
Ethicalapproval
TheEthicsCommitteeoftheHospitaldeClinicas, Universi-dadeFederaldoParaná,Brazilapprovedthestudy.
Results
Patientcharacteristics
Ofthe398patientstested,125(31.4%)hadadetectablePNH population.Ofthese,103(51maleand52female),whohad clinicaldataavailable,werestudied.Themedianageat pre-sentationwas24.1years(range:5.5–62.0years).Therewere 24patientsbelowtheageof18years(range:5.5–17.9years; median:14.7).Alltheseyoungpatientswereintheaplastic groups(11HPNsc/AAand13HPN/AA).
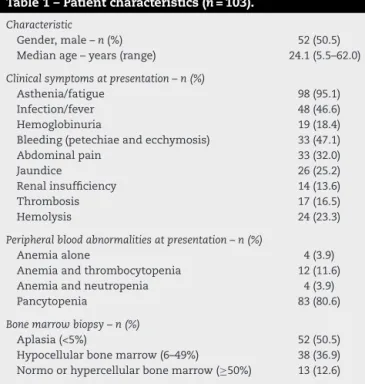
Hemoglobinuria was identified during monitoring in 43 (41.7%)patients, whileit wastheinitialsymptomatic man-ifestation in only 19 (18.4%) patients. The frequencies of infectionsand bleedingwere46.6%and 47.1%,respectively. Ninety-eight patients (95.1%) presented with asthenia, 33 (32.0%)withabdominalpain,and14(13.6%)withrenal insuf-ficiency;17(16.5%)developedthrombosisduringmonitoring and49patients(47.6%)haddocumentedhemolysis. Twenty-sixpatients(25.2%)withaplasiaatdiagnosis developedthe PNHcloneandhemolysisinamedianof2.35yearsafter diag-nosis.Ofthesepatients,eleven(10.7%)developedhemolysis fiveyearsafterthediagnosisofaplasia.
Peripheral blood abnormalities were present in 101 patients: 83 (80.6%) had pancytopenia, 12 (11.6%) anemia and thrombocytopenia, and four (3.9%) had anemia and leukopenia.Themedianhemoglobinlevelwas8.8g/dL(range: 3.8–14.5g/dL), the median absolute neutrophil count was 0.94× 109/L(range:0.26–1.45× 109/L)andthemedianplatelet countwas25× 109/L(range:2–294× 109/L).ThemedianLDH
Table1–Patientcharacteristics(n=103).
Characteristic
Gender,male–n(%) 52(50.5) Medianage–years(range) 24.1(5.5–62.0)
Clinicalsymptomsatpresentation–n(%)
Asthenia/fatigue 98(95.1) Infection/fever 48(46.6) Hemoglobinuria 19(18.4) Bleeding(petechiaeandecchymosis) 33(47.1) Abdominalpain 33(32.0)
Jaundice 26(25.2)
Renalinsufficiency 14(13.6)
Thrombosis 17(16.5)
Hemolysis 24(23.3)
Peripheralbloodabnormalitiesatpresentation–n(%)
Anemiaalone 4(3.9)
Anemiaandthrombocytopenia 12(11.6) Anemiaandneutropenia 4(3.9)
Pancytopenia 83(80.6)
Bonemarrowbiopsy–n(%)
Aplasia(<5%) 52(50.5) Hypocellularbonemarrow(6–49%) 38(36.9) Normoorhypercellularbonemarrow(≥50%) 13(12.6)
concentrationwas328U/L(range:30–7970U/L;normalrange 190–240U/L). Ninetypatients (87.4%)had hypocellularbone marrow.
Patientsincludedinthisstudyweredividedintothe sub-categoriesofClassicPNH(10patients),PNH/AA(39patients), andPNH-sc/AA(54patients)basedontheproposedPNH work-ing clinical classification.1 The initialcharacteristics ofthe
subgroupsaresummarizedinTable1.
The median ages of PNH-sc/AA, PNH/AA and Classic PNH patients were 25.1, 21.5 and 34.7 years, respec-tively(p-value=0.016).Theclinicalsymptomsofhemolysis, hemoglobinuriaandthrombosiswerehigherinthehemolytic formsofPNH(PNH/AAandClassicPNH)thaninPNH-sc/AA (p-value<0.001),whereasinfectionandfeverwerehigherin thePNH-sc/AAgroup(p-value<0.001).Themediannumbers ofneutrophils andplatelets were significantlylower inthe aplasticgroupsthanintheClassicPNHgroup(p-valueforboth <0.001).Ontheotherhand,theClassicPNHgrouphadhigher hemolyticmarkers,suchasLDH(p-value=0.001),reticulocyte count(p-value<0.001)and bilirubinlevels (p-value<0.001–
Table2).
Correlationofparoxysmalnocturnalhemoglobinuriaclone withclinicalcharacteristics
Table2–PNHsubgroupcharacteristics.
PNHcategory Total (n=103)
a–PNH-sc/AA (n=54)
b–PNH/AA (n=39)
c–Classic PNH(n=10)
p-Valuea
(a×b×c)
p-Value (a×b)
p-Value (a×c)
p-Value (b×c)
Age 24.1(5.5–62.0) 25.1(7.5–62.0) 21.5(5.5–49.4) 34.7(26.7–55.9) 0.016 0.322 0.017 0.004 Asthenia/fatigue 98(95.1%) 51(94.4%) 37(94.9%) 10(100%)
Infection/fever 48(46.6%) 23(42.6%) 25(64.1%) 0(0%) 0.001 Hemoglobinuria 43(41.7%) 4(7.4%) 30(76.9%) 9(90%) <0.001 Thrombosis 17(16.5%) 2(3.7%) 9(23.1%) 6(60%) <0.001 Hemolysis 49(47.6%) 0(0%) 39(100%) 10(100%) <0.001
Hemoglobin(g/L) 88(38–145) 80(38–132) 94(45–145) 89.5(51–117) 0.062a
Leucocytes (×103/L)
2970(1140–8800) 2675(1140–8800) 3110(1470–7780) 4490(1600–6680) 0.008a 0.05 0.005 0.106
ANC(×109/L) 0.94(0.26–4.95) 0.825(0.26–4.66) 1.06(0.59–4.95) 2.724(0.16–3.90) 0.000a 0.084 0.000 0.001
Platelets(×109/L) 25(2–294) 20(2–99) 27(3–137) 1815(6–294) <0.001a 0.041 0.00 0.00
ARC(×109/L) 53.8(2.4–437) 35.4(2.4–153) 70.8(3.2–214) 240(78–437) <0.001a 0.002 0.00 0.00
LDH(U/L) 328.5(30–7690) 234(30–783) 517(187–4550) 1608(328–7690) 0.001b 0.002 0.00 0.004
Bilirubin(mg/dL) 0.9(0.17–7.1) 0.7(0.17–4.93) 1.06(0.39–3.32) 2.54(0.39–7.1) <0.001a 0.004 0.00 0.00
Bonemarrow cellularity
5%(0–100%) 5% 10% 70% <0.001a 0.00 0.00 0.00
Flowcytometry
Neutrophil clonesize (median)
25.2(0.3–100) 7.3(0.3–68.7) 63(1.7–99.8) 98(81.3–100) <0.001a 0.00 0.00 0.001
Erythrocyte clonesize (median)
2.2(0–92.2) 0.04(0–18) 15.8(0–99.7) 82.2%(0–99.85) <0.001b 0.00 0.00 0.018
a:PNH-sc/AAgroup;b:PNH/AAgroup;c:ClassicPNHgroup.
ANC:absoluteneutrophilcount;ARC:absolutereticulocytecount;LDH:lactatedehydrogenase.
a ANOVAp<0.05. b Kruskal–Wallis,p<0.05.
granulocytes were 7.3% (range: 0.3–68.7%), 63.0% (range: 1.7–99.8%) and 98.0% (range: 81.3–100.0%) in PNH-sc/AA, PNH/AA and Classic PNH, respectively (p-value <0.001 –
Figures1–3).
Thromboticevents
Seventeenpatientspresentedwiththromboticevents:sixin theClassicPNHgroup,nine inthe PNH/AAgroupandtwo
inthePNH-sc/AAgroup.Therewerefivecasesofdeepvein thrombosis (DVT), five abdominal thromboses,five arterial thromboseswithischemicstroke,onesinusvenous thrombo-sisandonerenalveinthrombosis.TwoPNHsc/AApatientshad DVTdespitetheabsenceofhemolyticsymptoms,anddied. FourofthePNH/AApatientsdiedduetothromboticevents. RegardingthePNHclone,cloneslargerthan 50%wereseen inneutrophilsof13(76.5%)patients(p-value<0.001),andin erythrocytesofsix(35.3%)patients(p-value=0.005–Table3).
100
90
80
70
60
50
40
30
20
10
0
% median clone
PNH clone percentages in flow cytometry
Total (n=103) PNHsc/AA (n=54) AA/PNH (n=39) Classic PNH (n=10)
25.2 7.3 63 98
2.2 Neutrophils %
Erytrocytes % 0.04 15.8 82.2
0 3 6 9 12 15 18 21 24 27 30
Erythrocytes
PNHsc/AA PNH/AA Clássic PNH ≥90
>80-90 >70-80 >60-70 >50-60 >40-50 >30-40 >20-30 >10-20 >5-10 >3-5 >1-3 >0-1 0
Figure2–Numberofpatientswithpredominantlysmallerythrocyteclonesinparoxysmalnocturnalhemoglobinuriawith
subclinicalfeaturesandaplasticanemia,intermediateclonesinparoxysmalnocturnalhemoglobinuriawithaplastic
anemiaandlargeclonesinclassicparoxysmalnocturnalhemoglobinuria.
0 3 6 9 12 15 18 21 24
27 Granulocytes
PNHsc/AA PNH/AA Clássic PNH
>70-80
>80-90
>90-100 >60-70 >50-60 >40-50 >30-40 >20-30 >15-20 >10-15 >5-10
≤5
Figure3–Numberofpatientswithpredominantlysmallgranulocyteclonesinparoxysmalnocturnalhemoglobinuriawith
subclinicalfeaturesandaplasticanemia,intermediateinparoxysmalnocturnalhemoglobinuriawithaplasticanemiaand
largeinclassicparoxysmalnocturnalhemoglobinuria.
Thedifferencesbetweenpatientswithorwithout throm-botic events are shown in Table 4. There were statis-tically significant differences in the number of platelets (p-value=0.001),LDH(p-value=0.002)andinmedian percent-ages of the PNH clonein neutrophils (p-value<0.001) and erythrocytes (p-value=0.008). The median neutrophil PNH clone in thrombotic patients was 92.7% (range: 3.4–100%) vs. 21.8% (range: 0.25–99.9%) in non-thrombotic patients.
The median erythrocyte PNH clone was 31.8% (range: 0.0–97.1%)vs.1.2%(range:0.0–92.2%)inthromboticand non-thromboticpatients,respectively.Thebonemarrow cellular-ity,hemoglobinconcentration,leukocytecountandabsolute reticulocyte count were similar between the two groups. There were six deaths among patients with thrombotic events (35.3%),and eight(9.3%)amongthe non-thrombotic group.
Table3–Paroxysmalnocturnalhemoglobinurianeutrophilanderythrocyteclonesinthromboticpatients.
PNHclone <10%
PNHclone 10–50%
PNHclone
≥50%
p-Value(2
test)
Table4–Characteristicsofpatientswithandwithoutthrombosis.
Thrombosis Yes No p-Value(2test)
Bonemarrowcellularity–% 10 5 0.166
Hemoglobin(g/L) 8.8 6.5 0.682
Leukocyte(×103/L) 3500 2600 0.663
ARC(×109/L) 78.2 48.6 0.046
Platelets(×109/L) 67.0 31.5 0.001
LDH(U/L) 607 299 0.002
Neutrophilclonesize(median)–% 92.7% 21.5% <0.001
Erythrocyteclonesize(median)–% 31.8% 1.2% 0.008
Death–n(%) 6/17(35.3%) 8/86(9.3%) <0.001
LDH:lactatedehydrogenase;ARC:absolutereticulocytecount.
Survivalandtreatment
As a retrospective study, the cohort of patients received
differenttreatments depending on the physicianand time
criteria. Themajorityofpatients(81.9%)ofaplasticgroups
(PNH-sc/AA and PNH/AA) received cyclosporine A-based
immunosuppressivetherapywithorwithoutcorticosteroids
some time during the follow-up, and 12 patients (12.7%)
received anti-humanthymocyte immunoglobulin
immuno-suppressivetherapy.Hematopoieticstemcelltransplantation (HSCT)wasperformedin27patients(28.7%),themajorityof
whomwereinthePNH-sc/AAgroup.NinePNH/AAandtwo
ClassicPNHpatientsreceivedHSCTduetohemolytic
symp-toms.Eculizumabwasintroducedin2010,andfivepatients receivedthisdruguntiltheconclusionofthestudy.
The median follow-up period for all patients was 49.2
months(range:2.4–310months),withanOSof81.7%atten yearsafterdiagnosis.Therewasaslightdifferenceinsurvival betweenPNH-sc/AAandtheothertwogroups(76.5%vs.87.9%;
p-value=0.112). Intotal 14 patientsdied, nine inthe PNH-sc/AAgroupandfiveinthePNH/AAgroup.Thecausesofdeath weresepsis(sixpatients),pulmonarythromboembolism(four patients),mesentericthrombosis(twopatients),severe
graft-versus-host disease (GVHD) after HSCT (one patient) and
suddendeath(onepatient).Nodeathwasreportedinthe clas-sicalPNHgroupbytheendofthefollow-upperiod.
Discussion
PNH is a rare acquired disorder of hematopoietic stem
cells, which is characterized by a highly variable clinical course,includingintravascularhemolysis,bonemarrow fail-uresyndromesandthrombosis.1–3ThenaturalhistoryofPNH
hasbeenwidelydiscussedintheliteratureinretrospective series,3,4,8,9,16,19,20whichconfirmtheassociationbetweenPNH
andbonemarrowsyndromes.Theproportionofpatientswith bonemarrowhypoplasiawhodevelopclinicalorsubclinical PNHvariesfrom22%8to40%.16SomestudiesthatusedHam’s
testtodiagnosePNHshowedthat5–10%ofpatientswith Clas-sicPNHdeveloppancytopenia.2,4
Thecurrentstudyidentified103patientswithaPNHclone, 87.4%ofwhom hadhypoplasticmarrowatdiagnosis. PNH-associatedcytopeniaswerecommonandrecurrentinfections andbleedingwereseenin46.6%and47.1%ofpatients, respec-tively.Thehigh prevalenceofbonemarrowfailure may be
aresultofanascertainmentbiasexplainedbythefactthat theHospitaldeClinicasinCuritibareceivescasesofaplasia frommanyregionsofBrazil.Forthesamereasonthemajority ofpatients(81.9%)receivedimmunosuppressivetherapyand 28.7%receivedHSCT.
Patients included in this study were assigned to three subcategories based on the proposed PNHworking clinical classification,1namelyClassicPNH,PNH/AA,andPNH-sc/AA.
Asexpected,theclinicalsymptomsofhemolysis, hemoglobin-uria andthrombosiswere higherinthehemolyticformsof PNH(PNH/AAandClassicPNH)thaninPNH-sc/AA,whereas infection and fever were higher in the latter group. There weresignificantdifferencesintermsofperipheralbloodcell countsbetweenthethreesubcategories,especiallybetween the ClassicPNHandPNH-sc/AAsubcategories.Themedian PNHclonesizewasalsosignificantlydifferentbetweenthe threeclinicalsubcategoriesatdiagnosis.Ontheotherhand, eightpatientsinthe PNH/AAgrouppresentedwithintense hemolytic symptoms and PNH clones greater than 50%, despite the hypocellularbone marrow, suggestingan over-lapbetweenthesubgroups.Thisfactcouldbeexplainedby theheterogeneityofthesampleandthedisease,andbythe retrospectivebiasofthisstudy.
PNHmainlypresentsasadiseaseofadults,butthemedian agefoundinthecurrentserieswaslowerthanintheliterature (24.1vs.34.2years).2,3,19Thisdifferencecanbeexplainedby
theproportionofaplasticpatientswhoevolvedwiththePNH clone(PNH-sc/AA)afteralongperiodoftimeinourseries. However,ifthemedianageoftheClassicPNHgroupis con-sidered,itissimilartootherstudies.4,16,20
Inthelastdecade,thedetectionofGPI-APdeficientcellsby flowcytometrygreatlyincreasedthesensitivityofdetectinga PNHcloneinbothredbloodcellsandleukocytes,minimizing theeffectsofredcelltransfusionsonestimatingclonesize.5,11
SincetheintroductionofFCM,quantitativeandkinetic differ-encesofGPI-APdeficientcloneshavebeenreportedbetween PNHpatients withand without marrow failure.The litera-turesuggeststhattheclinicalmanifestationsduetochronic hemolysis in PNHappearto be morecommon in patients withlargepopulationsofcellsdeficientinGPIproteins.1,19–21
Pu et al. showed adirect relationship between the sizeof PNHcloneand thedevelopmentofintravascularhemolysis inpatientswithaplasia.19Inthecurrentstudylarge
associatedwithincreasedrisksofhemoglobinuriaand throm-bosis,whereassmallPNHclones(<50%)areassociatedwith bonemarrowfailure.
In this study, life-threatening thrombotic complications were present in 16.5% of patients, with six deaths occur-ring in this group (35.3% vs. 9.3% in the non-thrombotic group).All three subcategories hadat leastoneepisode of thrombosis. Two PNHsc/AA patients had DVT despite the absenceofhemolyticsymptoms,anddied.FourofthePNH/AA patientsdiedduetothromboticevents.PNHcloneslargerthan 50%wereseeninthegranulocytesof13 (76.5%)thrombotic patients,whichisconsistentwiththeliteraturethatsaysthat aclonesizegreaterthan50%isassociatedwithincreasedrisk ofthrombosisand theneed ofprimaryanticoagulation.7,21
InthecurrentcohortthesizeofthePNHclonewasgreater inpatientswiththrombosisforbothneutrophils(92.7%vs. 21.5%)anderythrocytes(31.8%vs.1.2%).
TheOStenyearsafterdiagnosiswas81.7%inthisstudy, whichisslightlyhigherthanotherstudies,20whichreported
77.6%at10years.Infectionandthromboticeventswere iden-tified as the main causes of death. There were 14 deaths (13.5%),12ofwhichwere attributabletoPNHoraplasia;of thedeaths,six(42.8%)weresecondarytothrombosis.With regardtothediseasesubcategories,thelong-termoutcomes weresimilarbetweenpatientsinthehemolyticPNH subcate-gories,butslightlydifferentinPNH-sc/AAgroup,probablydue toahighriskofinfection.Furtherstudiesmayshedinsights intothehypothesisthatthePNH-sc/AAsubcategorymightbe aseparatediseaseentityfromClassicPNH.1,5,22
Conclusion
Thisretrospectivestudyof103PNHpatientsoveran11-year periodrepresentsthelargestcollectionofsuchpatientsfrom asinglecenterinBrazil.Theresultsconfirmedthesuggestion thatPNHisnotasimplebinarydiagnosisandbothflow cyto-metric characterizationofGPI-AP expressionon peripheral bloodcellsandmarrowanalysisarerequiredfor comprehen-sivediseaseclassification.FCMdatafromthis studyshows thatlargerPNHclonesareassociatedwithclassicalPNH symp-tomsandincreasedriskofthrombosis,eveninpatientswith bonemarrowfailure,whereassmallerPNHclonesare associ-atedwithbonemarrowaplasia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
TheauthorswishtothankRosanaInaraCattaneo,Miriam Per-lingeiroBeltrame,NoelySilvaandLeilaOliveirafortechnical assistancewithflowcytometricstudies.ThankstoDr.Adam CampbellSmith fortheEnglishrevisionand toDr.Alberto Orfaoforthescientificcomments.
r
e
f
e
r
e
n
c
e
s
1.ParkerC,OmineM,RichardsS,NishimuraJ,BesslerM,Ware R,etal.Diagnosisandmanagementofparoxysmalnocturnal hemoglobinuria.Blood.2005;106(12):3699–709.
2.SociéG,MaryJY,deGramontA,RioB,LeporrierM,RoseC, etal.Paroxysmalnocturnalhaemoglobinuria:long-term follow-upandprognosticfactors.FrenchSocietyof Haematology.Lancet.1996;348(9027):573–7.
3.deLatourRP,MaryJY,SalanoubatC,TerriouL,EtienneG, MohtyM,etal.Paroxysmalnocturnalhemoglobinuria. Naturalhistoryofdiseasessubcategories.Blood. 2008;112(8):3099–106.
4.HillmenP,LewisSM,BesslerM,LuzzattoL,DacieJV.Natural historyofparoxysmalnocturnalhemoglobinuria.NEnglJ Med.1995;333(19):1253–8.
5.BorowitzMJ,CraigFE,DigiuseppeJA,IllingworthAJ,RosseW, SutherlandDR,etal.Guidelinesforthediagnosisand monitoringofparoxysmalnocturnalhemoglobinuriaand relateddisordersbyflowcytometry.CytometryBClinCytom. 2010;78(4):211–30.
6.MortazaviY,MerkB,McIntoshJ,MarshJC,SchrezenmeierH, RutherfordTR,BIOMEDIIPathophysiologyandTreatmentof AplasticAnaemiaStudyGroup.ThespectrumofPIG-Agene mutationsinaplasticanemia/paroxysmalnocturnal hemoglobinuria(AA/PNH):ahighincidenceofmultiple mutationsandevidenceofamutationalhotspot.Blood. 2003;101(7):2833–41.
7.HallC,RichardsS,HillmenP.Primaryprophylaxiswith warfarinpreventsthrombosisinparoxysmalnocturnal hemoglobinuria(PNH).Blood.2003;102(10):3587–91.
8.DunnDE,TanawattanacharoenP,BoccuniP,NagakuraS, GreenSW,KirbyMR,etal.Paroxysmalnocturnal
hemoglobinuriacellsinpatientswithbonemarrowfailure syndromes.AnnInternMed.1999;131(6):401–8.
9.NakakumaH,NagakuraS,IwamotoN,KawaguchiT,Hidaka M,HorikawaK,etal.Paroxysmalnocturnalhemoglobinuria cloneinbonemarrowofpatientswithpancytopenia.Blood. 1995;85(5):1371–6.
10.Griscelli-BennaceurA,GluckmanE,ScrobohaciML,Jonveaux P,VuT,BazarbachiA,etal.Aplasticanemiaandparoxysmal nocturnalhemoglobinuria:searchforapathogeneticlink. Blood.1995;85(5):1354–63.
11.HallSE,RosseWF.Theuseofmonoclonalantibodiesandflow cytometryinthediagnosisofparoxysmalnocturnal
hemoglobinuria.Blood.1996;87(12):5332–40.
12.PiedrasJ,López-KarpovitchX.Flowcytometryanalysisof glycosylphosphatidyl-inositol-anchoredproteinstoassess paroxysmalnocturnalhemoglobinuriaclonesize.Cytometry. 2000;42(4):234–8.
13.Hernándes-CampoPM,AlmeidaJ,SanchezML,MalvezziM, OrfaoA.Normalpatternsofexpressionof
glycosylphosphatidylinositol-anchoredproteinsondifferent subsetsofperipheralbloodcells:aframeofreferenceforthe diagnosisofparoxysmalnocturnalhemoglobinuria. CytometryBClinCytom.2006;70(2):71–81.
14.RichardsSJ,RawstronAC,HillmenP.Applicationofflow cytometrytothediagnosisofparoxysmalnocturnal hemoglobinuria.Cytometry.2000;42(4):223–33.
15.SugimoriC,ChuhjoT,FengX,YamazakiH,TakamiA, TeramuraM,etal.MinorpopulationofCD55−CD59−blood
cellspredictsresponsetoimmunosuppressivetherapyand prognosisinpatientswithaplasticanemia.Blood. 2006;107(4):1308–14.
patientstreatedwithhorseanti-thymocyteglobulinplus cyclosporine.Haematologica.2010;95(7):1075–80.
17.CamittaBM,RappeportJM,ParkmanR,NathanDG.Selection ofpatientsforbonemarrowtransplantationinsevere aplasticanemia.Blood.1975;45(3):355–63.
18.SwerdlowSH,CampoE,HarrisNL,JaffeES,PileriAS,SteinH, etal.,editors.WHOclassificationoftumorsof
haematopoieticandlymphoidtissues.Lyon:IARC;2008.
19.PuJJ,MukhinaG,WangH,SavageWJ,BrodskyRA.Natural historyofparoxysmalnocturnalhemoglobinuriaclonesin patientspresentingasaplasticanemia.EurJHaematol. 2011;87(1):37–45.
20.GeM,LiX,ShiJ,ShaoY,ZhengY.Clinicalfeaturesand prognosticfactorsofAsianpatientswithnocturnal hemoglobinuria:resultsfromasinglecenterinChina.Ann Hematol.2012;91(7):1121–8.
21.KimJS,LeeJW,YoonS-S,LeeJH,JoDY,JangJH,etal. Associationbetweenelevatedhemolysisatdiagnosisand earlymortalityandriskofthrombosisinparoxysmal nocturnalhemoglobinuria(PNH)patientswithcytopenia. Blood.2010;116:4241[ASHAnnualMeetingAbstracts].