1 Universidade Federal de Santa Maria, Faculdade de Odontologia, Departamento de Estomatologia. Rua Floriano Peixoto, 1184, Santa Maria, RS,
Factors associated with Oral Health-Related Quality of Life of preschool
children in Southern Brazil
Fatores associados com a qualidade de vida relacionada à saúde bucal de pré-escolares no sul do Brasil
Fernanda Ruffo ORTIZ1
Yassmín Hêllwaht RAMADAN1
Rubén Alberto BAYARDO GONZÁLEZ2
Thiago Machado ARDENGHI1
ABSTRACT
Objective
The aim of this study was to assess the impact of socioeconomic factors and clinical conditions on the child oral health-related quality of life (COHRQoL) of preschool children.
Methods
A cross-sectional study was conducted with a representative sample of 547 children of 0-5-years-old from Santa Maria, RS, Brazil, in 2013. Data were collect in the National Children’s Vaccination Day Program by calibrated dentists. Clinical examinations assessed the prevalence of dental caries and dental trauma. Information about children's socioeconomic status was collected through a structured questionnaire answered by parents/caregivers. The COHRQoL was measured using the Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS). Multivariable Poisson regression models were performed to assess the association between clinical conditions, socioeconomic status and COHRQoL.
Results
The prevalence of dental caries and dental trauma were 16.42 % and 22.49%, respectively. Higher means of the ECOHIS were found in older children, those with toothache and those whose mother had lower level of formal education. The clinical conditions that have been associated with negative impact on oral health related quality of life were experience caries (RR 4.12; 95% CI 3.10-5.46) and dental trauma (RR 1.37; 95% CI 1.01-1.86).
Conclusion
Poor socioeconomic and clinical conditions had a negative impact on the COHRQoL, indicating the need of preventive strategies and policies aiming at improving the quality of life of this sample.
Indexing terms: Children. Dental caries. Quality of life. Oral health. Tooth injuries.
RESUMO
Objetivo
Avaliar a associação de fatores socioeconômicos e condições clínicas na qualidade de vida relacionada à saúde bucal (COHRQoL) de crianças pré-escolares.
Métodos
Um estudo transversal foi realizado com uma amostra representativa de 547 crianças de 0-5 anos de idade de Santa Maria, RS, Brasil, em 2013. Os dados foram coletados no Dia Nacional de Multivacinação Infantil por dentistas calibrados. Exames clínicos avaliaram a prevalência de cárie dentária e trauma dentário. Informações sobre as condições socioeconômicas das crianças foram coletados através de um questionário estruturado respondido pelos pais/cuidadores. A COHRQoL foi medida utilizando a versão brasileira da Early Childhood Oral Health Impact Scale (ECOHIS). Modelos de regressão multivariada de Poisson foram realizados para avaliar a associação entre as condições clínicas, condições socioeconômicas e COHRQoL.
Resultados
A prevalência de cárie dentária e trauma dentária foi 16,42% e 22,49%, respectivamente. As maiores médias dos ECOHIS foram encontradas em crianças mais velhas, aqueles com dor de dente e aqueles cuja mãe tiveram menor nível de educação formal. As condições clínicas que foram associadas com um impacto negativo na qualidade de vida relacionada à saúde bucal foram experiência de cárie (RR 4,12; IC 95% 3,10-5,46) e trauma dentário (RR 1,37; IC 95% 1,01-1,86).
Conclusão
Condições socioeconômicas e clínicas ruins tiveram um impacto negativo sobre a COHRQoL, indicando a necessidade de estratégias preventivas e políticas destinadas a melhorar a qualidade de vida da população estudada.
INTRODUCTION
The child oral health-related quality of life (COHQoL) is a subjective measured of oral health inluenced by environmental and clinical factors1. It is emphasized
three dimensions - physical, mental and social - in the context of disease and has been increasingly used in oral health research. The COHRQoL has been deined as ‘the impact of oral disease and disorders on aspects of everyday life that a patient or person values, that are of suficient magnitude, in terms of frequency, severity or duration to affect their experience and perception of their life overall’2.
The measurement of COHRQoL outcomes has been gathered by means of questionnaires that were developed to assess physical and psychological symptoms, and life satisfaction3. In Brazil, the Early Childhood Oral
Health Impact Scale (ECOHIS) is the most commonly used questionnaire to measure the OHRQoL of preschoolers and their families4.
There are studies demonstrating that children with oral disease, as dental caries, have toothache or discomfort, dificulty to eat, loss of appetite, sleep disruption, change in behavior and poor school performance5-6.
The assessment of the relationship between dental caries and OHRQoL should not be based only on clinical indicators of disease and requires detailed understanding of the factors that can act as confounding or mediators such as personal, social and environmental. This knowledge can improve the relationship between patients, parents and dental professional6.
Therefore, the aim of this study was to assess the association of socioeconomic factors and clinical oral conditions on the oral health-related quality of life (OHRQoL) of preschool children.
METHODS
A cross-sectional study was conducted with a representative sample of 0-5-years-old children in August 2013, in Santa Maria, a southern city in Brazil. The city population was of approximately 261.031 including 18,420 children age 0-5 years-old, in the study period.
Sample size was calculated using the following parameters: mean score of the ECOHIS in children with dental caries of 2.8 (SD: 5.9). mean score of the ECOHIS of 1.0 (SD: 3.4) in children without dental caries7, 95%
conidence interval (CI), power of the statistical test of 80% and a design effect of 1.6. We added a 30% to possible
refuses. The minimum sample size required for the study was 245 children. As the present study was part of a survey in which other outcomes were considered, the inal sample size was greater than the minimum required to verify differences in ECOHIS scores.
Ethics approved through the Research Committee of the School of Dentistry Centro Universitário Franciscano, and prior written consent was obtained in all cases.
Data collection
Data were collected by calibrated dentists through structured interviews and oral examinations during the National Children’s Vaccination Day Program. The calibration process lasted a total of 36 hours containing theoretical and clinical exercises; it was performed prior by dental examiner with previous experience in oral health survey. For this purpose, a total of 10 children were examined twice by the same examiner, with an interval of two weeks each examination (kappa values 0.70-0.95 and 0.73-0.88, respectively).
The city is divided into ive regions, and each one has public health centers responsible for the vaccination of the children residing in their area. Children who attended in the National Children’s Vaccination Day Program were invited for participate this study. The vaccination program has had uptake rates consistently above 97%. The examiners were assigned one to each center, except for two centers which were the largest and had to locate two reviewers for each health center. The selected points were centers had dental chair and which represent each region. According to the number of children in each area, a quota sampling was selected from all children visiting the 15 health centers. Each ifth child in the queue for vaccination was invited to participate in the study. If their caregivers did not consent the participation, the next child was selected. Immediate relatives were excluded to avoid selection bias. The same selection procedure was used at all participating health centers.
Dental examination was performed on a dental chair, under conventional dental illumination, using periodontal probes (CPI; "ball point") and dental mirrors. Clinical examinations considered the dental caries experience measured by the dmf-t index and dental trauma8. Information
and "white" (children of European descent)9. Parent’s
educational level was compared those who had completed 8 years of formal instruction, which in Brazil corresponds to primary school, with those who did not. Household income was measured in terms of the Brazilian minimum wage which nearly corresponded to US$ 740 dollars, during the period of data gathering; the value was further dichotomized by the median. Household overcrowding was assessed by calculating the ratio between the number of household residents and the number of rooms in the home. Parents/guardians asked whether or not their children had toothache.
The Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS) was used to evaluate the COHRQoL10. It consists of 13 items, including a child impact
section (symptoms, function, psychological and self-image/ social interaction domains) and family impact section (parent distress and family function domains). Answers were recorded using a Likert scale with options coded 0–5 (0 = never; 1 = hardly ever; 2 = occasionally; 3 = often; 4 = very often; 5 = don’t know). Total score had a 0–52 range— higher score indicated greater impact of oral health problems and related treatment experiences on OHRQoL of preschoolers and their families. Mean ECOHIS scores were calculated for each domain and for the whole scale as a simple sum of the response codes, after recoding all ‘‘Don’t know’’ responses as missing. For those with up to two unanswered in the child section or one in the family section, were considered incomplete and excluded of analysis4.
Statistical analysis
Data analyses were performed using STATA, software 12.0 (Stata Corp., College Station, TX, USA). Descriptive and unadjusted analysis provided statistics summary assessing the association between the outcome (ECOHIS total scores mean) and dental caries. Multivariable Poisson regression models were performed to assess the association between clinical oral conditions, socioeconomic stats and COHRQoL. This strategy allowed estimating the rate ratios among the comparison groups and their respective 95% conidence interval. Explanatory variables were selected for the inal models only if they had a P value ≤ 0.05 after adjustment.
RESULTS
A total of 547 children of 0-5-years-old participated this is study. For all children invited, 90% agreed to participate.
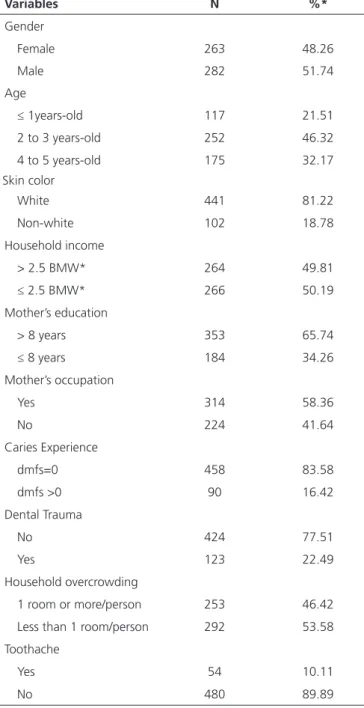
Table 1 show clinical and socioeconomic characteristics of the sample. A total sample, 51.7% was males, with mean
age of 2.67 (SD 1.23), their parents reported high educational level (65.74%) and subtly lower household income (50.19%). The prevalence of dental caries, dental trauma, and toothache was 16.42%, 22.49%, and 10.11%, respectively.
Table 1. Clinical and socioeconomic characteristics of participating children, Santa Maria, Brazil, 2013.
*BMW: Brazilian minimum wage (approximately U$ 740 during the data gathering).
Variables N %*
Gender
Female 263 48.26
Male 282 51.74
Age
≤ 1years-old 117 21.51
2 to 3 years-old 252 46.32
4 to 5 years-old 175 32.17
Skin color
White 441 81.22
Non-white 102 18.78
Household income
> 2.5 BMW* 264 49.81
≤ 2.5 BMW* 266 50.19
Mother’s education
> 8 years 353 65.74
≤ 8 years 184 34.26
Mother’s occupation
Yes 314 58.36
No 224 41.64
Caries Experience
dmfs=0 458 83.58
dmfs >0 90 16.42
Dental Trauma
No 424 77.51
Yes 123 22.49
Household overcrowding
1 room or more/person 253 46.42
Less than 1 room/person 292 53.58
Toothache
Yes 54 10.11
No 480 89.89
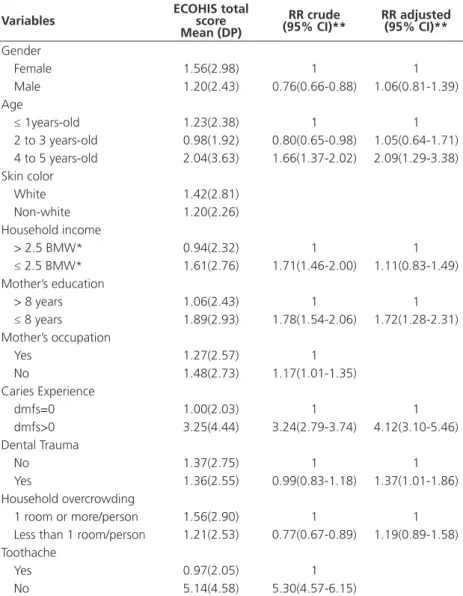
assessing the association of COHRQoL with clinical and sociodemographic variables was shown in Table 2. Children with toothache and dental caries presented the highest mean of ECOHIS. The oldest children (RR 2.09; 95% CI 1.29-3.38) and those whose mothers have less than 8 years of formal education (RR 1.72; 95% CI
1.28-2.31), had higher mean of ECOHIS when comparing to their counterparts. Clinical conditions that have been associated with negative impact on oral health related quality of life were the prevalence of dental caries (RR 4.12; 95% CI 3.10-5.46) and dental trauma (RR 1.37; 95% CI 1.01-1.86).
Table 2. Mean (SD) distribution, simple and multiple analyses of the association between OHRQoL and clinical and socioeconomic in children. Santa Maria, Brazil, 2013.
*BMW: Brazilian minimum wage (approximately U$ 740 during the data gathering) ** Poisson Regression Analysis
RR: ratio rate
Variables ECOHIS total score
Mean (DP)
RR crude
(95% CI)** RR adjusted(95% CI)**
Gender
Female 1.56(2.98) 1 1
Male 1.20(2.43) 0.76(0.66-0.88) 1.06(0.81-1.39)
Age
≤ 1years-old 1.23(2.38) 1 1
2 to 3 years-old 0.98(1.92) 0.80(0.65-0.98) 1.05(0.64-1.71)
4 to 5 years-old 2.04(3.63) 1.66(1.37-2.02) 2.09(1.29-3.38)
Skin color
White 1.42(2.81)
Non-white 1.20(2.26)
Household income
> 2.5 BMW* 0.94(2.32) 1 1
≤ 2.5 BMW* 1.61(2.76) 1.71(1.46-2.00) 1.11(0.83-1.49)
Mother’s education
> 8 years 1.06(2.43) 1 1
≤ 8 years 1.89(2.93) 1.78(1.54-2.06) 1.72(1.28-2.31)
Mother’s occupation
Yes 1.27(2.57) 1
No 1.48(2.73) 1.17(1.01-1.35)
Caries Experience
dmfs=0 1.00(2.03) 1 1
dmfs>0 3.25(4.44) 3.24(2.79-3.74) 4.12(3.10-5.46)
Dental Trauma
No 1.37(2.75) 1 1
Yes 1.36(2.55) 0.99(0.83-1.18) 1.37(1.01-1.86)
Household overcrowding
1 room or more/person 1.56(2.90) 1 1
Less than 1 room/person 1.21(2.53) 0.77(0.67-0.89) 1.19(0.89-1.58) Toothache
Yes 0.97(2.05) 1
No 5.14(4.58) 5.30(4.57-6.15)
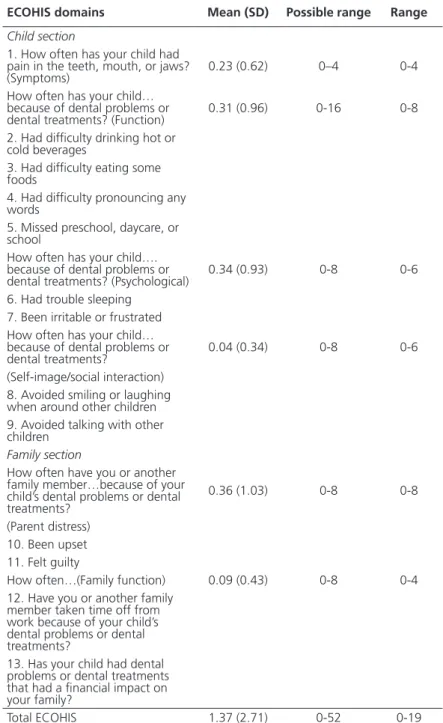
Table 3 indicates total ECOHIS and domain scores. Total scores ranged from 0 to 19 with a 1.37 mean (SD = 2.71). The highest mean was for the parent’s distress domain (0.36) and the lowest for the child’s
DISCUSSION
The present study evaluated the impact of clinical and socioeconomic characteristics on the OHRQoL of preschoolers. The most important ind was that children with dental caries and dental trauma and those with lower socioeconomic status presented poorer OHRQoL when comparing with their counterparts.
This study found a prevalence of dental caries of 16.42%, which is lower than other Brazilian studies with the same age group (ranging from 40.2%-64.8% 6,11-13). The overall mean of the ECOHIS for children with
dental caries was 3.25(SD: 4.44), a value similar to the study of Guedes et al.7. We found that dental caries and
dental trauma negatively impacts the quality of life of preschoolers and their parents, which is in agreement
Table 3. Descriptive distribution of total ECOHIS and domains scores. Santa Maria, Brazil, 2013.
ECOHIS domains Mean (SD) Possible range Range
Child section
1. How often has your child had pain in the teeth, mouth, or jaws?
(Symptoms) 0.23 (0.62) 0–4 0-4
How often has your child… because of dental problems or
dental treatments? (Function) 0.31 (0.96) 0-16 0-8
2. Had dificulty drinking hot or cold beverages
3. Had dificulty eating some foods
4. Had dificulty pronouncing any words
5. Missed preschool, daycare, or school
How often has your child…. because of dental problems or
dental treatments? (Psychological) 0.34 (0.93) 0-8 0-6
6. Had trouble sleeping 7. Been irritable or frustrated How often has your child… because of dental problems or
dental treatments? 0.04 (0.34) 0-8 0-6
(Self-image/social interaction) 8. Avoided smiling or laughing when around other children 9. Avoided talking with other children
Family section
How often have you or another family member…because of your child’s dental problems or dental treatments?
0.36 (1.03) 0-8 0-8
(Parent distress) 10. Been upset 11. Felt guilty
How often…(Family function) 0.09 (0.43) 0-8 0-4
12. Have you or another family member taken time off from work because of your child’s dental problems or dental treatments?
13. Has your child had dental problems or dental treatments that had a inancial impact on your family?
with previous studies6,11-15. One of the reasons for dental
caries to affect the quality of life is painful sensition16-17.
Toothache leads to limitations in the oral functioning and emotional state of the child18, causing dificulty to
relax and problems in school performance19, as well as
dificulty sleeping16.
In our study, older children presented the higher means of ECOHIS, corroborating previous studies6,11.
This can be explained by the eruption period primary teeth in the oral cavity, which are more likely to develop oral diseases. Also, children whose mothers have a low educational level reported poorer oral health-related quality of life, conirming that the socioeconomic background of the children and their families inluences oral health14-15. Thus, non-awareness of the importance
of oral health care, lead to a neglect oral health of their children, and as consequence their quality of life will also be impaired. Another drawback are the inancial costs of dental treatment, because there is no government grant or third-party payment coverage of dental care for this children age group, a similar pattern found in other study15. Thereby, stands out the importance of assessing
socioeconomic conditions together with clinical and OHRQoL measures, even in preschool children2,11,14.
Children’s parents reported impact in the two sections of ECOHIS, showing that the oral health-related quality of life affect both the child as their family. The OHRQoL domains are relected in the deinition by Cella et al.20 as “the extent to which one’s usual or expected
physical, emotional, and social well-being is affected by a medical condition and/or treatment”. In the child section, a painful sensation in the teeth, dificulty chewing, irritation, dificulty drinking and trouble sleeping were also reported in previous studies11,14-15. For the parent’s
section, lost nights due to need of child care or spend time and money on dental care, cause suffering and inancial impact on the family11.
This study has some limitation. The data reported were cross sectional design, where associations not provide strong evidence for causation between predictors and outcome. However, cross-sectional studies are useful in order to identify risk indicators which can be included in further longitudinal assessments.
In the present study signiicant associations between lower maternal education level, dental caries and dental trauma in the COHRQoL, highlight the importance of assessing socioeconomic conditions together with clinical and OHRQoL measures. As preschoolers’ health depends on parental/caregiver knowledge about health care, these perceptions become important to improve child oral health outcome and oral health-related quality of life.
CONCLUSION
Poor socioeconomic and clinical conditions had a negative impact on the COHRQoL, indicating the need of preventive strategies and policies aiming at improving the quality of life of this population.
Collaborators
REFERENCES
1. Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. 2011;90(11):1264-70. doi: 10.1177/0022034511399918
2. Locker D, Allen F. What do measures of “oral health related quality of life” meaure? Community Dent Oral Epidemiol. 2007;35(401):11. doi: 10.1111/j.1600-0528.2007.00418.x
3. Allen PF. Assessment of oral health related quality of life. Health Qual Life Outcomes. 2003;1:40. doi: 10.1186/1477-7525-1-40
4. Pahel BT, Rozier RG, Slade GD. Parental perceptions of children’s oral health: the Early Childhood Oral Health Impact Scale (ECOHIS). Health Qual Life Outcomes. 2007;5:6. doi: 10.1186/1477-7525-5-6
5. Ramos-Jorge J, Pordeus JA, Ramos-Jorge ML, Marques LS, Paiva SM. Impact of untreated dental caries on quality of life of preschool children: defferent stages and activity. Community Dent Oral Epidemiol. 2014;42(4):311-322. doi: 10.1111/ cdoe.12086
6. Gomes MC, Pinto-Sarmento TCDA, Costa EMMDB, Martins CC, Granville-Garcia AF, Paiva SM. Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study. Health Qual Life Outcomes. 2014;12:55. doi: 10.1186/1477-7525-12-55
7. Guedes RS, Piovesan C, Antunes JL, Mendes FM, Ardenghi TM. Assessing individual and neighborhood social factors in child oral health-related quality of life: a multilevel analysis. Qual Life Res. 2014;23(9):2521-30. doi: 10.1007/s11136-014-0690-z
8. WHO. The World Oral Health Report 2003: continuos improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Geneva: World Health Organization; 2003.
9. IBGE. Resultados da amostra: trabalho e rendimento 2010 [cited 2015 Dez 12]. Avaliable from: <http://biblioteca.ibge. gov.br/visualizacao/periodicos/1075/cd_2010_trabalho_ rendimento_amostra.pdf>.
10. Martins-júnior PA, Ramos-jorge J, Paiva SM, Ramos-jorge ML. Validations of the Brazilian version of the Early Childhood Oral Health Impact Scale (ECOHIS). 2012;28(2):367-74. doi: 10.1590/S0102-311X2012000200015
11. Martins-Júnior PA, Vieira-Andrade RG, Corrêa-Faria P, Oliveira-Ferreira F, Marques LS, Ramos-Jorge ML. Impact of early childhood caries on the oral health-related quality of life of preschool children and their parents. Caries Res.
2013;47(3):211-8. doi: 10.1159/000345534
12. Gradella CMF, Bernabé E, Bönecker M, Oliveira LB. Caries prevalence and severity, and quality of life in Brazilian 2- to 4-year-old children. Community Dent Oral Epidemiol. 2011;39(6):498-504. doi: 10.1111/j.1600-0528.2011.00625.x
13. Abanto J, Tsakos G, Paiva SM, Carvalho TS, Raggio DP, Bönecker M. Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: Perceptions of parents and children. Community Dent Oral Epidemiol. 2014;42(5):385-94. doi: 10.1111/cdoe.12099
14. Abanto J, Carvalho TS, Mendes FM, Wanderley MT, Bönecker M, Raggio DP. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent Oral Epidemiol. 2011;39(2):105-14. doi: 10.1111/j.1600-0528.2010.00580.x
15. Wong HM, McGrath CPJ, King NM, Lo ECM. Oral health-related quality of life in Hong Kong preschool children. Caries Res. 2011;45(4):370-6. doi: 10.1159/000330231
16. Slade GD. Epidemiology of dental pain and dental caries among children and adolescents. Community Dent Health. 2001;18(4):219-27.
17. Ortiz FR, Tomazoni F, Oliveira MDM, Piovesan C, Mendes F, Ardenghi TM. Toothache, associated factors, and its impact on oral health-related quality of life (OHRQoL) in preschool children. Braz Dent J. 2014;25(6):546-53. doi: 10.1590/0103-6440201302439
18. Krisdapong S, Prasertsom P, Rattanarangsima K, Sheiham A. Relationships between oral diseases and impacts on Thai schoolchildren’s quality of life: Evidence from a Thai national oral health survey of 12- and 15-year-olds. Community Dent Oral Epidemiol. 2012;40(6):550-9. doi: 10.1111/j.1600-0528.2012.00705.x
19. Blumenshine SL, Vann WF Jr, Gizlice Z, Lee JY. Children’s school performances: impacts of general and oral health. J Public Health Dent. 2008;68(2):82-7. doi: 10.1111/j.1752-7325.2007.00062.x
20. Cella DF. Measuring quality of life in palliative care. Semin Oncol. 1995;22(3):73-81.
Received on: 24/2/2016 Final version resubmitted on:13/4/2016