www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Position
statement
of
the
Brazilian
Academy
of
Rhinology
on
the
use
of
antihistamines,
antileukotrienes,
and
oral
corticosteroids
in
the
treatment
of
inflammatory
sinonasal
diseases
夽
Olavo
de
Godoy
Mion
a,∗,
João
Ferreira
de
Mello
Jr
b,
Daniel
Lorena
Dutra
c,
Nilvano
Alves
de
Andrade
c,
Washington
Luiz
de
Cerqueira
Almeida
c,
Wilma
Teresinha
Anselmo-Lima
d,
Leonardo
Lopes
Balsalobre
Filho
e,
Jair
de
Carvalho
e
Castro
f,
Roberto
Eustáquio
dos
Santos
Guimarães
g,h,
Marcus
Miranda
Lessa
i,
Sérgio
Fabrício
Maniglia
j,
Roberto
Campos
Meireles
k,
Márcio
Nakanishi
a,l,
Shirley
Shizue
Nagata
Pignatari
m,
Renato
Roithmann
n,o,
Fabrizio
Ricci
Romano
p,
Rodrigo
de
Paula
Santos
f,
Marco
César
Jorge
dos
Santos
c,
Edwin
Tamashiro
qaUniversidadedeSãoPaulo(USP),DisciplinadeOtorrinolaringologia,SãoPaulo,SP,Brazil bUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,SãoPaulo,SP,Brazil
cUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,DepartamentodeOtorrinolaringologia,SãoPaulo,SP,Brazil dUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto,DepartamentodeOtorrinolaringologia,Ribeirão
Preto,SP,Brazil
eUniversidadeFederaldeSãoPaulo(UNIFESP),CiênciasdaSaúde,SãoPaulo,SP,Brazil fUniversidadeFederaldeSãoPaulo(UNIFESP),Otorrinolaringologia,SãoPaulo,SP,Brazil
gUniversidadeFederaldeMinasGerais(UFMG),FaculdadedeMedicina,BeloHorizonte,MG,Brazil hUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto,RibeirãoPreto,SP,Brazil
iUniversidadeFederaldaBahia(UFBA),FaculdadedeMedicina,DisciplinadeOtorrinolaringologia,Salvador,BA,Brazil jHospitalInstitutoParanaensedeOtorrinolaringologia,CentrodeRiniteeAlergia,Curitiba,PR,Brazil
kUniversidadedoEstadodoRiodeJaneiro(UERJ),RiodeJaneiro,RJ,Brazil lUniversidadedeBrasília(UnB),FaculdadedeMedicina,Brasília,DF,Brazil
mUniversidadeFederaldeSãoPaulo(UNIFESP),DepartamentodeOtorrinolaringologiaeCabec¸aePescoc¸o,SãoPaulo,SP,Brazil nUniversidadeLuteranadoBrasil(ULBRA),FaculdadedeMedicina,Otorrinolaringologia,Canoas,RS,Brazil
夽 Pleasecitethisarticleas:MionOG,MelloJF,DutraDL,AndradeNA,AlmeidaWL,Anselmo-LimaWT,etal.Positionstatementofthe BrazilianAcademyofRhinologyontheuseofantihistamines,antileukotrienes,andoralcorticosteroidsinthetreatmentofinflammatory sinonasaldiseases.BrazJOtorhinolaryngol.2017;83:215---27.
∗Correspondingauthor.
E-mail:[email protected](O.G.Mion).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2017.01.002
oMountSinaiHospital,DepartmentofOthorhinolaryngology,Toronto,Canada
pUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,Ciências,SãoPaulo,SP,Brazil
qUniversidadedeSãoPaulo(USP),FaculdadedeMedicinadeRibeirãoPreto,DepartamentodeOftalmologia,
OtorrinolaringologiaeCirurgiadeCabec¸aePescoc¸o,RibeirãoPreto,SP,Brazil
Received16December2016;accepted21December2016 Availableonline21January2017
KEYWORDS
Rhinitis; Rhinosinusitis; Antihistamines; Glucocorticoids; Leukotriene antagonists
Abstract
Introduction:Inflammatoryconditions ofthenoseandparanasalsinuses arevery prevalent
inthegeneralpopulation,resultinginmarkedlossofqualityoflifeinaffectedpatients,as wellassignificantwork,leisure,andsocialactivitylosses.Thesepatientsrequirespecificand specializedtreatment.Awiderangeoforalmedicationsareavailable.
Objective:Thepresentdocumentisaimedtoclarify,forprofessionalstreatingpatientswith
inflammatorysinonasaldiseases,bothspecialistsandgeneralpractitioners,specificoral ther-apiesinnoninfectiousnasalinflammatoryconditions.
Methods:Themethodologyusedtocreatethisarticleincludedthesearchforthekeywords:
oralcorticosteroids,antihistamines,antileukotrienes,rhinitis,rhinosinusitisintheMEDLINEand EMBASEdatabasesinthelast5years.Sincenorelevantarticlewasfoundforthetextonthe subjectofinterestinthelast5years,thesearchwasextendedforanother5years,andsoon, accordingtotheauthors’needs.
Results:Relevantliteraturewas foundregardingtheuseofantihistamines,antileukotrienes
andoralcorticosteroidsintheseconditions.TheBrazilianAcademyofRhinologyemphasizes, afterextensivediscussionbythecollegiate,keypointsinthetreatmentwiththesedrugs.
Conclusion:Thereissupportintheliteraturefortheuseofthesedrugs;however,final
consid-erationsabouttheroleofeachofthemhavebeenmade.
© 2017 Publishedby Elsevier EditoraLtda. on behalf ofAssociac¸˜ao Brasileira de Otorrino-laringologiaeCirurgiaC´ervico-Facial.ThisisanopenaccessarticleundertheCCBYlicense (http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Rinites; Rinossinusites; Anti-histamínicos; Glicocorticoides; Antagonistasde leucotrieno
PosicionamentodaAcademiaBrasileiradeRinologiasobreousodeanti-histamínicos, antileucotrienosecorticosteroidesoraisnotratamentodedoenc¸asinflamatórias nasossinusais
Resumo
Introduc¸ão:As afecc¸ões inflamatórias do narize seiosparanasaissão muitoprevalentesna
populac¸ãogeral,causamacentuadaperdadequalidadedevidadospacientesafetados,gerando perdassignificativasdasatividadesdetrabalho,lazeresociais.Estespacientesnecessitamde tratamentoespecíficoeespecializadoeumaamplagamademedicac¸õesoraisestãodisponíveis.
Objetivo:Opresentedocumentotemporobjetivoesclareceràquelesquetratamdasdoenc¸as
nasossinusaisinflamatórias,tantoespecialistasquantogeneralistas,sobreasterapêuticasorais nasafecc¸õesinflamatóriasnasaisnãoinfecciosas.
Método: A metodologia utilizada para elaborac¸ãodeste artigo incluiu abusca das palavras
chave:corticosteroidesorais,anti-histamínicos,antileucotrienos,rinite,rinossinusitenos ban-cosdedadosMEDLINEeEMBASE nosúltimos5anos.Nãosendoencontradoartigo relevante paraotextosobreoassuntodeinteressenosúltimos5anos,abuscapoiextendidapormais5 anos,eassimpordiante,deacordocomanecessidadedosautores.
Resultados: Literatura relevante foi encontrada comrelac¸ão ao uso dos anti-histamínicos,
antileucotrienosecorticosteroidesoraisnestasafecc¸ões.AAcademiaBrasileiradeRinologia resalta,apósamplodebatedocolegiado,pontos-chavenotratamentocomestesmedicamentos.
Conclusão:Há respaldo na literatura para o uso destes medicamentos, entretanto
considerac¸õesfinaisacercadopapeldecadadelesforamfeitas.
Introduction
Inflammatoryconditionsofthenose andparanasalsinuses arethemostprevalentgroupofdiseasesinthegeneral pop-ulation. These diseases, such as allergic and non-allergic rhinitis,acuteandchronicrhinosinusitis,withandwithout nasalpolyposis,resultinamarkeddecreaseinthequalityof lifeofaffectedpatients,generallycausingsignificantwork, leisure, and social activity losses. These patients require specificandspecializedtreatment.
Oral medicationsareextremelyimportantinthe treat-ment of inflammatory diseases of the nose and paranasal sinuses,aswell asinthetreatment of infectiousdiseases oftheupperairways.Althoughsomeclassesofdrugshave beenusedfor decades,newmolecules haverecentlybeen madeavailable.
Duetotheprevalenceofthesediseases,therearevery high direct and indirect costs associated withtreatment, especiallyinthelongterm.Thecostassociatedwith treat-mentshould notbeignored,and thecorrectuseof these drugs can result in lower costs for both the patients and theirfamilies,aswellasforpublichealthandsociety.
The aimofthis documentis toclarifyfor professionals who treat inflammatory sinonasal diseases, both special-istsandgeneralpractitioners,nasaloraltherapiesforthese noninfectious diseases. Through a review of thescientific evidence, the Brazilian Academy of Rhinology provides a practicalandup-to-dateviewofthemostfrequentlyused nasal oral medications, except for medications that have antimicrobialagentsintheirformulation.
The methodology used to create this article included thesearchforthekeywords:oralcorticosteroids, antihis-tamines,antileukotrienes,rhinitis,andrhinosinusitisinthe MEDLINEandEMBASEdatabasesinthelast5years.Noarticle wasfoundrelevanttothetextonthesubjectofinterestin thelast5yearsand,therefore,thesearchwasextendedto another5years,andsoon,accordingtotheauthors’needs.
The
role
of
histamine
and
leukotrienes
in
nasal
inflammatory
diseases
Histamine
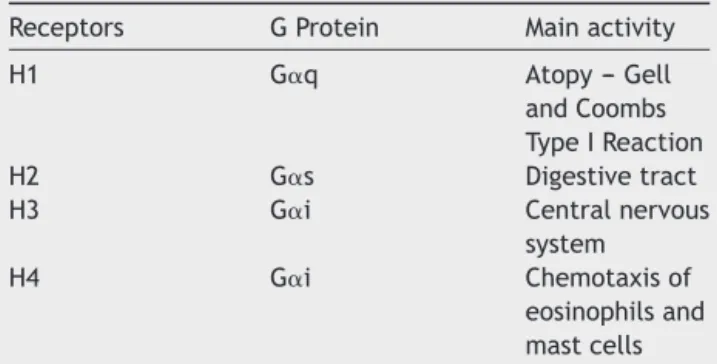
Histamine has an important physiological role and can bind to 4 different receptors1 (Table 1). Through these
Table1 Antihistaminesandhistaminereceptors.
Receptors GProtein Mainactivity
H1 G␣q Atopy---Gell
andCoombs TypeIReaction
H2 G␣s Digestivetract
H3 G␣i Centralnervous
system
H4 G␣i Chemotaxisof
eosinophilsand mastcells
AdaptedfromtheIIIConsensusonrhinitis.1
bindings,it acts onimmunoregulationand allergic inflam-mation.Inallergicrhinitis,thehistaminereleasedintothe nasalmucosabindsto H1receptors andtriggers vasodila-tion, increased vascular permeability, pruritus, increased glandularsecretion,andnerve-endingstimulation.
HistaminereceptorsareclassifiedasG-proteinreceptors in active or inactive form. Histamine stabilizes itsactive structuring,whileantihistamines,actingasinverseagonists, stabilizetheinactiveconformation.2
Leukotrienes
Evidenceoftheroleofleukotrienesindisease pathophysi-ologycomesfromstudiesoftheimmediateandlatephases in allergen-triggering. That did not happen after contact withmethacholine.3,4Analysisofthesecretionofpatients
withpersistentrhinitisshowedhighlevelsofC4andD4 cys-teineleukotrienes5andLTC4.6Duetotheintensecapacity
ofleukotrienestocauseinflammation,whichisthousandsof timesgreaterthanthatofhistamine,ithasbeenspeculated thatnasalobstructionandcongestionaredirectlyassociated withthisclassofmediators7(Fig.1).
Nasalpolyposisisachronicinflammatorydiseaseofthe upper respiratory tract that affects 2---4% of the popula-tionand 2/3ofpatients withacetylsalicylic acid-sensitive asthma.Thehistologyofpolypsissimilartothatofasthma, withabundant eosinophils, mast cells, and high levels of proinflammatorycystenylleukotrienes.8
It has been proposed that one of the potential causes ofchronic rhinosinusitiswithnasal polyps isthe presence ofdefectsintheeicosanoidpathway,morestrongly associ-atedwithacetylsalicylicacidintolerance.9Specifically,the
increased synthesis of pro-inflammatory leukotrienes and thedecreasedsynthesisofanti-inflammatoryprostaglandins havebeentheacceptedmechanism,notonlyforchronic rhi-nosinusitiswithnasalpolypsinacetylsalicylicacid-sensitive patientsbutalsointhosetoleranttothisdrug.10
Regardingleukotrienesandchronicrhinosinusitis,there aremanydataabouttheiractiononinflammationreduction, especiallyconcerningeosinophilsandeicosanoidpathway.11
Montelukastshoweda reductionin eosinophilic inflamma-tion,cytokineviabilityandproductioninnasalpolyps.12 It
hasbeendemonstratedthatcalcium(Ca+)influxintomast cellsthrough theactivation of Ca+ channels release stim-ulates the production of C4 leukotrienes, which in turn activatesahigherCa+influx.13
Antihistamines
Antihistaminesareconsideredthegoldstandardmedication forthetreatmentofallergicrhinitis.2
Theydecreasetheallergicinflammatoryreactionthrough their action on H1 receptors, by interfering with the action of histamine on sensory neurons and small ves-sels.Thekappa-betanucleartranscriptionfactorinhibition alsoreducestheantigenic presentation,theexpression of cytokines and cell adhesion molecules. They also reduce mastcellactivationinadose-dependentmanner.11
Arachidonic acid
FLAP
Hydrolase
Transmembrane transporter
Nucleus Zileuton
5-lipoxigenase
Leukotriene A4 Leukotriene C4
Leukotriene C4 Leukotriene B4
Leukotriene D4
BLT Receptor Chemotaxis
Extracellular
space
Leukotriene E4
CysLT1 Receptor Leukotriene C4
synthase
Montelukast pranlukaste zafirlukaste
Cell membranes Nuclear membrane
Airway Phospholipase A2
Figure1 Eicosanoidpathwayleadingtoleukotrieneformation.
membrane of histaminergic neurons. Most of these anti-histaminesweremarketedbeforepharmacologicalstudies wererequiredbyregulatoryagenciesthus,pharmacokinetic andpharmacodynamic data arenot available for most of them.11
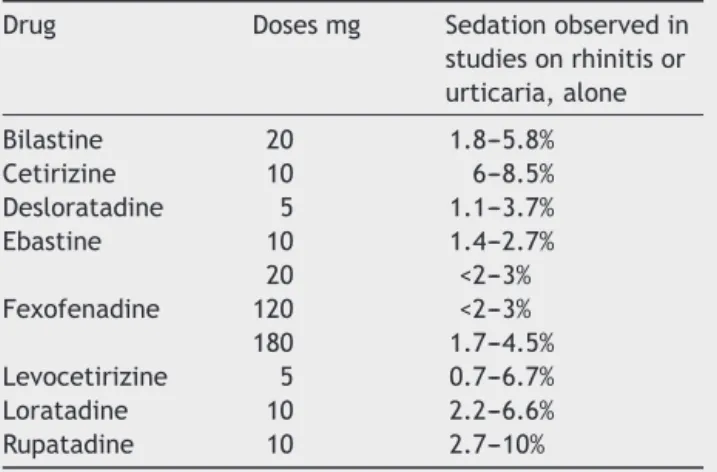
On the other hand, second-generation drugs create a lower potential for sedation (Table 2) and pharmacoki-neticand pharmacodynamicdatahave been publishedfor several groups, such as healthy adults, the elderly, chil-dren,patientswithrenalfailure,etc. (Table3).Similarly, theirinteractionwithfoodandother drugsis known.Itis emphasizedthatafterintakediscontinuation,thehistamine responsesuppressionintheallergictestslastsfrom1to5 days.11
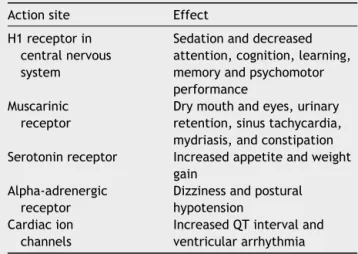
Thepotentialadverseeffectsoffirst-generation antihis-taminescan bedividedaccordingtotheiraction onother receptors,asshowninTable4.
There is strong scientific evidence for their action in improving allergic rhinitis and allergic rhinoconjunctivitis symptoms.2,11,14 Second-generationantihistamines prevent
Table2 Second-generationantihistaminesandeffectson thecentralnervoussystem.
Drug Dosesmg Sedationobservedin studiesonrhinitisor urticaria,alone
Bilastine 20 1.8---5.8% Cetirizine 10 6---8.5% Desloratadine 5 1.1---3.7% Ebastine 10 1.4---2.7% 20 <2---3% Fexofenadine 120 <2---3% 180 1.7---4.5% Levocetirizine 5 0.7---6.7% Loratadine 10 2.2---6.6% Rupatadine 10 2.7---10%
AdaptedfromSimonsandSimons.2
Table3 Pharmacokineticsandpharmacodynamicsofsomeantihistaminesinadults.11
Generation Tmax(h) Half-life(h) Startofaction(h) Durationofeffect(h)
Chlorpheniramine 1st 2.8 27.9 3 24
Diphenhydramine 1st 1.7 9.2 2 12
Hydroxyzine 1st 2.1 20.0 2 24
Bilastine 2nd 1.2 14.5 2 24
Cetirizine 2nd 1.0 6.5 0.7 ≥24
Desloratadine 2nd 1---3 27 2---2.6 ≥24
Fexofenadine 2nd 1---3 11 1---3 24
Levocetirizine 2nd 0.8 7 0.7 >24
Loratadine 2nd 1.2 7.8 2 24
Rupatadine 2nd 0.75 6 2 24
Table 4 Potential adverse effects of first-generation antihistamines.2
Actionsite Effect
H1receptorin centralnervous system
Sedationanddecreased attention,cognition,learning, memoryandpsychomotor performance
Muscarinic receptor
Drymouthandeyes,urinary retention,sinustachycardia, mydriasis,andconstipation Serotoninreceptor Increasedappetiteandweight
gain Alpha-adrenergic
receptor
Dizzinessandpostural hypotension
Cardiacion channels
IncreasedQTintervaland ventriculararrhythmia
AdaptedfromSimonsandSimons.2
andimprovesymptomssuchassneezing,nasalpruritus,and rhinorrhea,whichcharacterize theimmediateresponseof theGellandCoombsTypeIallergicreactionclassification. However,theyshowadiminishedeffectonnasalcongestion (latephase)(Table5). Theyalsocontrol ocular symptoms suchaserythema,tearing,pruritusandedema.2,11,14
AccordingtotheAmericanAcademyof Otorhinolaryngol-ogy and Head and Neck Surgery and the Allergic Rhinitis and Its Impact on Asthma consensus, it is recommended to use second-generation oral antihistamines for patients with allergic rhinitis. Although they are not as effective as intranasal corticosteroids, antihistamines possess the advantageofcost,rapidactiononset,andmaintenanceof efficiencywithregularuseinmildandmoderatecases.Their greatest benefit comes with regular use; however, their administration‘‘whennecessary’’isofgreatusefulnessas temporaryrescuemedication.2,14
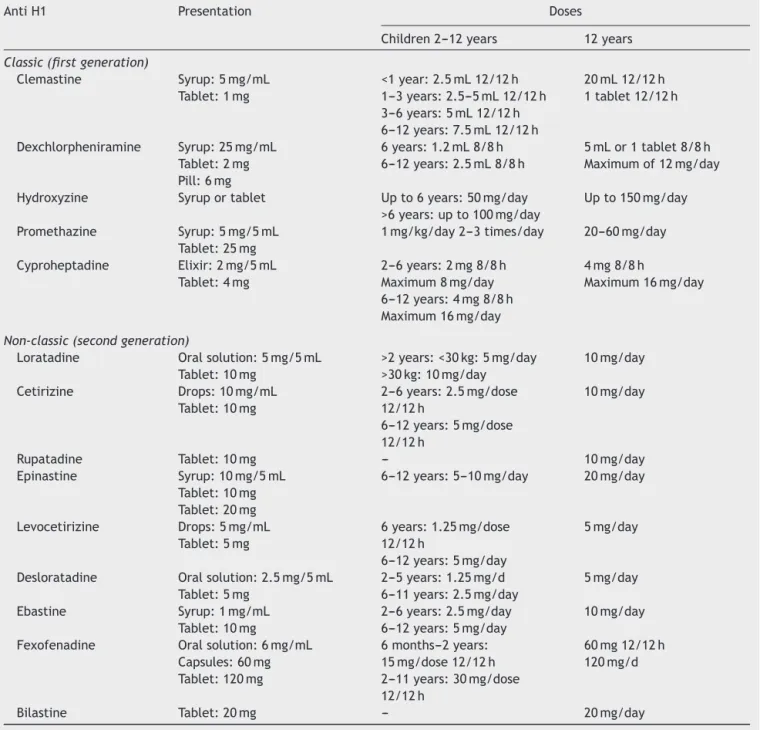
The firstandsecond-generationantihistaminedosesfor adultsandchildrenareshowninTable6.
Antihistamines arenotrecommended in thetreatment of acute bacterial rhinosinusitis,16 but they can be used
for relieving sneezing and rhinorrhea symptoms in viral cases.8Inpatientswithchronicrhinosinusitis,withor
with-out polyposis,thereis norecommendation for the useof oral antihistamines,exceptin allergicpatients.According toevidence-basedmedicalstudies,thereisimprovementin clinicalandendoscopicscoresinthesepatients.8
The intakeoffirst-generationantihistaminesmay occa-sionallycauseintensedizziness,confusion,delirium,coma, andrespiratorydepression.Inchildren,ontheotherhand,
theremaybeparadoxicaleffects,suchasexcitement, irri-tability,hyperactivity,insomnia,andhallucination.2
In contrast, the second-generation drugs, at the usual doses,arepracticallyfreeofadverseeffectsonthecentral nervoussystemandactiononthemuscarinic,serotoninand alpha-adrenergicreceptors.11Theirsafetyinspecial
popu-lationsisdescribedinTable7.
Decongestantsassociatedwithantihistamines
Nasal decongestants are subdivided into oral and topical formulations.As theyarealpha-adrenergic agonists, their main effect is vasoconstriction.1 Pseudoephedrine is the
most commonly used decongestant, in combination with antihistamines (Tables 8 and 9). This combination has a bettereffectthaneachdrugaloneincontrollingnasal symp-toms,butthechance ofadverseeffectssuchasinsomnia, headache,dry mouth, and irritabilityincreases.17,18 Their
usereduceshyperemia,edemaandnasalcongestion18 and
theirsafetyisknowninsingledailydosesofupto240mgfor thecontrolofnasalobstructioninseasonalallergicrhinitis, otherrespiratoryallergiesandrhinosinusitis.18
ArecentstudycarriedoutbytheFoodandDrug Admin-istration(FDA)toevaluatetheefficacyofphenylephrinein controllingnasalobstructionhasshownthatithasasimilar effecttoplacebowhengivenatadoseofupto40mgevery 4h.19
Thereisnoevidencefortheefficacyofdecongestantsin casesofacutebacterialrhinosinusitisinchildrenoradults, aswell as in patients with chronic rhinosinusitis (with or withoutpolyposis).20,21
Pseudoephedrine has minimal hepatic metabolism and is eliminated, unaltered, in the urine. Its half-life is 4---8h.21,22 Oral decongestants should be prescribed with
cautiontotheelderly, children,patientswithahistoryof cardiac arrhythmia, angina pectoris, cerebrovascular dis-ease,hypertension,urinaryretention,hyperthyroidismand shouldbeavoidedinpatientswithprostatichypertrophyand athletes,sinceitisconsidereddoping.23,24
Antihistaminesassociatedwithantileukotrienes
An antihistamine---antileukotriene association has been recentlylaunchedinthemarket.Itsobjectiveistoimprove the clinical effect of the drugs, either by association or potentiationof effect.Additionally, itcan improve adher-encetotreatmentbyofferingtwodifferentclassesofdrugs inasingletablet.
Some studies, mostly directed at rhinitis, have shown that montelukast has been associated with a variety of second-generation antihistamines, such as loratadine,25,26
Table5 Effectofmedicationsonallergicrhinitissymptoms.
Sneezing Rhinorrhea Nasalobstruction Nasalpruritus
Oralantihistamines ++ ++ + +++
Oraldecongestants +++
Antileukotrienes + + + +
Table6 Antihistaminepresentationanddoses.
AntiH1 Presentation Doses
Children2---12years 12years
Classic(firstgeneration)
Clemastine Syrup:5mg/mL Tablet:1mg
<1year:2.5mL12/12h 1---3years:2.5---5mL12/12h 3---6years:5mL12/12h 6---12years:7.5mL12/12h
20mL12/12h 1tablet12/12h
Dexchlorpheniramine Syrup:25mg/mL Tablet:2mg Pill:6mg
6years:1.2mL8/8h 6---12years:2.5mL8/8h
5mLor1tablet8/8h Maximumof12mg/day
Hydroxyzine Syruportablet Upto6years:50mg/day >6years:upto100mg/day
Upto150mg/day
Promethazine Syrup:5mg/5mL Tablet:25mg
1mg/kg/day2---3times/day 20---60mg/day
Cyproheptadine Elixir:2mg/5mL Tablet:4mg
2---6years:2mg8/8h Maximum8mg/day 6---12years:4mg8/8h Maximum16mg/day
4mg8/8h
Maximum16mg/day
Non-classic(secondgeneration)
Loratadine Oralsolution:5mg/5mL Tablet:10mg
>2years:<30kg:5mg/day >30kg:10mg/day
10mg/day
Cetirizine Drops:10mg/mL Tablet:10mg
2---6years:2.5mg/dose 12/12h
6---12years:5mg/dose 12/12h
10mg/day
Rupatadine Tablet:10mg --- 10mg/day
Epinastine Syrup:10mg/5mL Tablet:10mg Tablet:20mg
6---12years:5---10mg/day 20mg/day
Levocetirizine Drops:5mg/mL Tablet:5mg
6years:1.25mg/dose 12/12h
6---12years:5mg/day
5mg/day
Desloratadine Oralsolution:2.5mg/5mL Tablet:5mg
2---5years:1.25mg/d 6---11years:2.5mg/day
5mg/day
Ebastine Syrup:1mg/mL Tablet:10mg
2---6years:2.5mg/day 6---12years:5mg/day
10mg/day
Fexofenadine Oralsolution:6mg/mL Capsules:60mg Tablet:120mg
6months---2years: 15mg/dose12/12h 2---11years:30mg/dose 12/12h
60mg12/12h 120mg/d
Bilastine Tablet:20mg --- 20mg/day
ModifiedfromMion.15
fexofenadine,27 desloratadine28 and cetirizine.29 A
meta-analysis has shown that their clinical effect is superior to that of placebo.30 Other studies have shown that
the combination is superior to that of antihistamines or antileukotrienes alone in controlling allergic rhinitis symptoms.29,31
Few studies have evaluated the combination of lev-ocetirizine and montelukast, but the results have been promising,superior totheassociationswithother antihis-tamines.Thecombinationoflevocetirizineandmontelukast showedsuperior results, with a beneficial additive effect in the treatment of persistent allergic rhinitis.32,33 There
arestudiesshowingthatsuchacombinationbringsbenefits
in preventingsymptomsin patientswithpoor responseto monotherapy andincontrollingsymptoms,especially noc-turnalones.34,35
Leukotriene
antagonists
The leukotrienereceptorantagonist,montelukast, isused in the control of allergic diseases, such as asthma and rhinitis, as it is a receptor blocker that binds with high affinity and selectivity to the cysteine receptors found in the airways.36,37 It has no bronchodilator effect, but
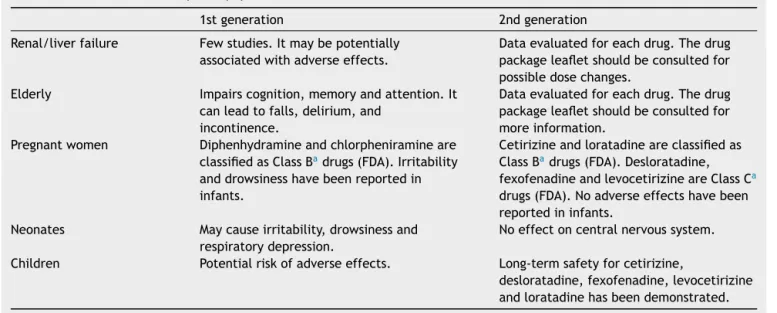
Table7 Adverseeffectsinspecialpopulations.11
1stgeneration 2ndgeneration
Renal/liverfailure Fewstudies.Itmaybepotentially associatedwithadverseeffects.
Dataevaluatedforeachdrug.Thedrug packageleafletshouldbeconsultedfor possibledosechanges.
Elderly Impairscognition,memoryandattention.It canleadtofalls,delirium,and
incontinence.
Dataevaluatedforeachdrug.Thedrug packageleafletshouldbeconsultedfor moreinformation.
Pregnantwomen Diphenhydramineandchlorpheniramineare classifiedasClassBadrugs(FDA).Irritability
anddrowsinesshavebeenreportedin infants.
Cetirizineandloratadineareclassifiedas ClassBadrugs(FDA).Desloratadine,
fexofenadineandlevocetirizineareClassCa
drugs(FDA).Noadverseeffectshavebeen reportedininfants.
Neonates Maycauseirritability,drowsinessand respiratorydepression.
Noeffectoncentralnervoussystem.
Children Potentialriskofadverseeffects. Long-termsafetyforcetirizine,
desloratadine,fexofenadine,levocetirizine andloratadinehasbeendemonstrated.
AdaptedfromSimonsandSimons.2
a Riskclassificationofdruguseinpregnancy,accordingtotheFoodandDrugAdministration(FDA).CategoryA---adequateand well-controlledstudieshavenotshownanyrisktothefetusinthefirsttrimesterofpregnancy(thereisnoevidenceofriskinothertrimesters); B---studiesonanimalreproductionhavenotshownarisktothefetusandtherearenoadequateandwell-controlledstudiesinpregnant women;C---animalreproductionstudieshavedemonstratedadverseeffectsonthefetusandtherearenoadequateandwell-controlled studiesinhumans;however,thepotentialbenefitsmayjustifythedruguseinpregnantwomendespitethepotentialrisks;D---thereis evidenceofrisktothefetusbasedonadversereactionsfrominvestigationalstudiesorpost-marketingstudies;however,thepotential benefitsmayjustify thedrug useinpregnantwomendespite thepotentialrisks;X---animalor humanstudieshave demonstrated fetalalterationsorevidenceofrisktothehumanfetusbasedonadversereactionsfrominvestigationalorpost-marketingstudiesand therisksinvolvedinthedruguseinpregnantwomendonotjustifythepotentialbenefits.FDAPregnancyCategories.Availableat: http://www.drugs.com/pregnancy-categories.html[accessed02.04.16].
severe asthma,38 In addition to improving the symptoms
of rhinitis,39 sleepapnea,40 andconjunctivitis,41 and may
be used asadjunctive therapy in chronic urticaria.42 The
GINA(GlobalInitiativeforAsthma),43PRACTALL(Practicing
Allergology)44 andARIA (Allergicrhinitisanditsimpacton
asthma)11 guidelinesrecommendtheuseofmontelukastas
atherapeuticagentforthecontrolofasthmaandrhinitis.
Affinityandselectivityforthecysteinereceptor
When montelukast binds withhigh affinity andselectivity to cysteine receptors (CysLT), it promotes the physiolog-ical blocking of leukotrienes C1 to C4, D and E. This binding does not occur with other respiratory receptors (cholinergic,prostanoid,beta-adrenergic).Montelukast,as wellasanotherleukotrieneantagonist,zafirlukast,arealso potent ligands of the CysLT receptor, more strongly than pranlukasteandotherequivalentcompounds(LM-1507and LM-1484).45
Safetyandsideeffects
Montelukasthasshowntobeadrugwithahighsafety pro-fileandis recommendedforthetreatment ofasthma and rhinitisbyconsensusandglobalguidelines.11,44,45The
over-allincidenceofadverseeventsisconsideredlow(Table10). TheCochraneFoundationratedthedrugasbeingsaferthan long-actingbeta-2agonists.46
Efficacyofmontelukastinallergicrhinitis
Severalstudiessincethe1990shaveinvestigatedthe possi-bleefficacyofleukotrieneantagonistsinthetreatmentof allergicrhinitis.58,59
The antagonist zafirlukast was evaluated in allergic rhinitis, which showed some protection,59 as well as
pranlukaste.60 The useof montelukast resulted in greater
efficacy, includinggood cost---benefit,61 although it is less
effectivethannasalcorticosteroids.35
Severalauthorshaveevaluatedtheactionofmontelukast instudies withmorethan1000 patients withseasonal62,63
andpersistentrhinitis,64confirmingtheimprovementofall
cardinalsymptomsofallergicrhinitis,witheffectonsleep andquality of sleep, ocular symptoms, allergic rhinocon-junctivitisandqualityoflifeingeneral.60,62---64
The efficacy of antileukotrienes in allergicrhinitis and asthma,aftermorethan15yearsofuse,hasbeen widely demonstrated.Montelukast has been very well evaluated forthetreatment ofseasonalandperennialallergic rhini-tis.Itresultsinsignificantimprovementsinnasalandocular symptomsbetween 1 and 3 days,as well asin nocturnal symptoms,sleepqualityandqualityoflife.60
Antileukotrienesandchronicrhinosinusitiswith andwithoutnasalpolyps
Table8 Associationoffirst-generationantihistamineswithdecongestants.1
Association Presentation Dosesforchildren Dosesforadultsand
childrenolderthan 12years
Azatadine+pseudoephedrine Pill1mgazatadine+120mg pseudoephedrine
Syrup0.5mgazatadine+30mg pseudoephedrine/mL
>6years:5mLevery 12h
1---6years:2.5mL every12h
1tabletevery12h 10---20mLevery12h
Brompheniramine+phenylephrinea Syrup5mLwith2mg
brompheniramine+5mg phenylephrine
Drops1mLwith2mg brompheniramine+2.5mg phenylephrine
Tablet:12mg
brompheniramine+15mg phenylephrine
>2years:2.5---5mL every6h
>2years:2dropsper kgdividedevery8h
15---30mLevery6h 1tabletevery12h
Brompheniramine+pseudoephedrine Syrup1mLwith0.2mg brompheniramine+3mg pseudoephedrine Capsuleswith4mg brompheniramine+60mg pseudoephedrine
>6months:
0.25---0.30mL/kg/dose every6h
20mLevery6h 1capsuleevery6h
Triprolidine+pseudoephedrine Syrup:every5mL 1.25triprolidine+30mg pseudoephedrine
Tablet:2.5mgtriprolidine+60mg pseudoephedrine
2---5years:2.5mL every6h 6---12years:5mL every6h
10mLevery6h 1tabletevery6h
AdaptedfromIIIConsensusonrhinitis.1
aNoevidenceofclinicaleffectonnasalobstruction.
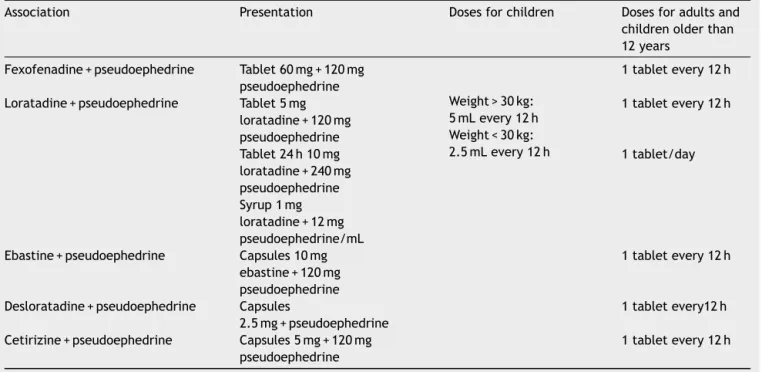
Table9 Associationofsecond-generationantihistamineswithoraldecongestants.1
Association Presentation Dosesforchildren Dosesforadultsand
childrenolderthan 12years
Fexofenadine+pseudoephedrine Tablet60mg+120mg pseudoephedrine
1tabletevery12h
Loratadine+pseudoephedrine Tablet5mg loratadine+120mg pseudoephedrine
Weight>30kg: 5mLevery12h Weight<30kg: 2.5mLevery12h
1tabletevery12h
Tablet24h10mg loratadine+240mg pseudoephedrine Syrup1mg loratadine+12mg pseudoephedrine/mL
1tablet/day
Ebastine+pseudoephedrine Capsules10mg ebastine+120mg pseudoephedrine
1tabletevery12h
Desloratadine+pseudoephedrine Capsules
2.5mg+pseudoephedrine
1tabletevery12h
Cetirizine+pseudoephedrine Capsules5mg+120mg pseudoephedrine
Table10 Sideeffectsofantileukotrienes.48---59
Adverseeffectsofmontelukast
Overalleffects Pharyngitis,fever, infection
Comparableto placebo47
Effectsonlower airways
Worseningof asthma
Comparableto placebo47
Effectsoncentral nervoussystem
Irritability, aggressiveness, hallucinations Suicide?
Relatedto otherdrugs usedtogether? Symptom improvement aftertreatment discontinuation48---52
Vascularsystem Churg-Strauss Syndrome? (Vasculitis) Angioedema
Notfully clarified53,54
Skin Urticaria 53
Hepatic Hepatitis 53,55
Highdosesofup to1000g
Malaise,vomiting, abdominalpain andhyperactivity
Noserious accountsin relationto overdose56,57
and 2/3 of asthmatic patients with acetylsalicylic acid sensitivity.8
Although the pathophysiology of chronic rhinosinusitis suggests the use of antileukotrienes, double-blind ran-domized clinical trials do not support theoretical studies regardingtheefficacyofleukotrieneinhibitorssoclearly.65
Leukotrieneantagonists,suchasmontelukast,zafirlukast and zileuton were evaluatedin studies involving patients withchronicrhinosinusitiswithnasalpolyposisand Aspirin-Exacerbated Respiratory Disease (AERD).66,67 The results
werenot clear. Manyuncontrolled open studieshave sug-gestedthebenefitsofantileukotrienesinsymptomatology, nasal polyp size and tomographic scores.68 Other results
includesignificantimprovementinheadache,painandfacial pressure,auditorydiscomfort,dentalpain,purulent nasal discharge,post-nasaldrip,nasalcongestionandobstruction, as well as olfactory symptoms.69 These studies conclude
thatleukotriene-modifyingdrugs,ifaddedtostandard med-ications,includingcorticosteroids,resultinimprovednasal symptoms in patientswith chronic rhinosinusitiswith and withoutpolyposis.70---72
However, data from double-blind, randomized con-trolled studies do not consistently support the benefit of antileukotriene therapy in patients with chronic rhinosinusitis.66,73 Although antileukotrienes are effective
inpatients withAERD,theyarenomoreeffectivethanin acetylsalicylicacid-tolerantpatients.74,75
Regardingtheassociationofmontelukastwithintranasal corticosteroids, there are studies that demonstrate the efficacy of their combined use in chronic rhinosinusitis. Montelukast added to intranasal corticosteroids improves symptoms in patients withchronic rhinosinusitis, withan excellentsafetyprofile.76
Forthesereasons,theactionofantileukotrienes,when analyzedfromthepointofviewofevidence-basedMedicine,
disclosesalimitedlevelofefficacyandhasalowdegreeof recommendationinpatientswithchronicrhinosinusitiswith nasalpolyposis.77
Montelukast was, to date, the most commonly used antileukotriene. Its anti-inflammatory action, especially thoserelatedtotheeosinophilanditscytokineshasbeen demonstratedbyseveralstudies.Anotherimportantfactor whenconsidering montelukastis itshigh safetyand toler-ability,eveninchildren.11 Whatisclearlyunderstoodisits
usefulnessinallergicpatientswithasthmaandpatientswith acetylsalicylicacidintolerance.Thesearethepatientswith chronic rhinosinusitis whoshould receive antileukotrienes therapy,eitherasanadjunctivetherapyornot,inthe post-operativeandmaintenanceperiods.
Oral
corticosteroids
Glucocorticosteroids(GCs)areaclassofdrugswitheffects onseveralcellfunctions,andtheirimportanteffectonthe mechanismsinvolvedininflammationmakethemoneofthe mainmodalitiesoftreatmentinautoimmuneand inflamma-torydiseases,suchasasthma,allergy,rheumatoidarthritis, multiplesclerosis,andinflammatoryboweldiseases.78 This
characteristicalsoprovidesarelevantroleinnasal inflam-matory diseases. However, their therapeutic benefits are limitedbythesideeffectsassociatedwiththeirprolonged useandhighdoses.
These effects include osteoporosis, skin atrophy, dia-betes,glaucoma,cataracts,hypertension,avascular necro-sis,infectionandincreasedabdominalfat.79Table11shows
themainsystemic GCsusedin clinicalpracticewiththeir equivalencetableandanti-inflammatorypotency.80 Weuse
theterminology‘‘corticosteroid’’(CS)assynonymouswith GC.
Corticosteroids act on protein synthesis. When they penetratethecells,theybindtoreceptorscalled glucocor-ticosteroidreceptors andgo into the cell nucleus, where theytriggergenomiceffects.Theyhavetwoaction mecha-nisms:thefirstiscalledtransactivation,whenitinducesthe synthesisof proteinssuchaslipocortin-1, beta-adrenergic receptors,secretoryleukoproteaseinhibitor.Theyalsohave atransrepression action, wherethereis inhibition of syn-thesisof inflammatory cytokinesand adhesion molecules, amongothers.Suchmechanismseemstobethemost rele-vantininflammatorydiseases,andalsotheleastrelatedto theadverseeffectsofthisclassofdrugs.1,81
Acutebacterialrhinosinusitis
A Cochrane review has reported that there is no robust currentevidencefortheuseofsystemiccorticosteroidsas monotherapyforthetreatmentofacuterhinosinusitis.82
Inpatientswhoreceivedanassociationofcorticosteroids andsystemic antibiotics, thereseems tobe some benefit suchassymptomaticrelief,althoughcurrentdataare lim-ited.The short-term benefitoccurswith thereduction in painscores,andthereseemstobeimprovementinthemore acute symptoms of facial pain and headache.82,83 There
Table11 Equivalence,anti-inflammatorypotencyandhalf-lifeofcorticosteroids.
Approximate
equivalencedoseinmg
Relativeanti-inflammatory potencya
Biological half-life(h)
Hydrocortisone 20 1 8---12
Prednisone 5 3.5---4.0 12---36
Prednisolone 5 4.0 12---36
Methylprednisolone 4 5.0 12---36
Dexamethasone 0.75 30 36---72
Betamethasone 0.6 30 36---72
Deflazacort 7.5 2.5---3.5 24---36
Adaptedfromhormonalanti-inflammatorydrugs:glucocorticoids.80
aIncomparisontohydrocortisone(cortisol).
antibiotics resembles those observed in the placebo groups.83,84 Therefore,itappearscorticosteroids canbring
symptomaticreliefintheshorttermasadjunctivetherapy.
Chronicrhinosinusitis
Arecentsystematic reviewsuggestsan importantrolefor systemiccorticosteroidsintreatingexacerbationsofchronic rhinosinusitis(CRS)withpolyps,beingindicatedforashort, intermittent treatment (1---3 weeks).85 This study cites 3
previous systematic reviews for use in CRS,86---88
demon-stratinganassociationwithsymptomimprovement,quality oflife questionnaires,andpolypscorewhen comparedto placebo,inatotalof5randomizedcontrolledtrials. How-ever,thetrialsshowedimprovementonlyintheshort-term, forapproximately2---3weeks,withlimitedfollow-upof2---6 months.
In CRS without polyps, the evidence in the literature ismorelimited,thestudies areheterogeneousand lacka controlgroup,withoutrandomizedcontrolledtrials, demon-strating a lower level of evidence. The use of systemic corticosteroidsinpatientswithCRSwithoutpolypsrequires studieswithamorerobustmethodology.
Ameta-analysisandasystematic review evaluatedthe roleofcorticosteroids in endoscopicfunctional surgeryof theparanasalsinuses.89Eighteenstudieswereincluded,for
a total of 1309 patients. Studies with mixed populations of CRS with and without polyps and the use of systemic and/ortopicalcorticosteroids wereevaluated. Theresults indicated a significant intraoperative benefit: significant reductionofblood loss,reducedsurgical timeand quality ofthesurgicalfieldimprovement.Therewasnosignificant differenceregardingpostoperativepainandpostoperative symptom scores. However, the postoperative endoscopic evaluationscoresweresignificantlybetterinthe corticos-teroidgroup.ThesubgroupofpatientswithCRSwithpolyps hadalowerrateofrecurrencewhencomparedtocontrols.
Allergicrhinitis
The useof corticosteroids for a shortperiodof timemay beatherapeuticoptioninallergicrhinitispatientswhoare notresponsivetoothertreatments.90Theexistenceofother
veryeffectivetreatmentoptions,togetherwithsteroiduse potentialadverseeffects,especiallyforaprolongedperiod
of time,does notjustify their systematicand routineuse inallergicrhinitis.Therefore,theyarenotconsideredasa first-linetreatment.91
Final
considerations
The use of second-generation antihistamines is recom-mended over the first-generation ones due to improved safetyprofile. Regardingdrowsiness orsedation, thedose ofsecond-generationdrugsshouldbeconsidered,aswellas timeofuseandindividualsensitivityofeachpatient.
Theuseoforaldecongestantsisusefulinrelieving symp-tomsofacutenasalobstruction.Cautionisadvisedregarding theiruseduetotheirpotentialsideeffects.
The use of antihistamines associated with antileukotrienes becomes important in the presence ofmonotherapyfailure.
Leukotrienereceptorantagonistscan beusedinadults andchildrenwithseasonalallergicrhinitisandinpreschool childrenwithpersistentallergicrhinitisduetotheirefficacy, highsafety,andtolerability.16 Thislineofmedicationscan
stillbeusedasanadjuvanttreatmentinthetreatment of chronicrhinosinusitis.
Oralcorticosteroidsareusefulasrescuemedicationfor chronicrhinosinusitiswithpolyps,andareusuallyprescribed for a short period of 1---3 weeks. In chronic rhinosinusi-tis without polyps, the evidence for corticosteroid use is very limited. Therefore, the analysis of a possible bene-fit againstthe potential risksof usingoral corticosteroids shouldguidetheclinicaldecision-making.Similarly,inacute bacterial rhinosinusitis, the physician should individually evaluateeachpatient,determinesymptomseverityandthe risksoforalcorticosteroiduseandconsidertheiruseasan optionforsymptomaticrelief.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
2.SimonsFE, SimonsKJ.Histamine andH1-antihistamines: cel-ebrating a century of progress. J Allergy Clin Immunol. 2011;128:1139---50.
3.Creticos PS, Peters SP, Adkinson NF Jr, Naclerio RM, Hayes EC,NormanPS,etal.Peptideleukotrienereleaseafter anti-genchallengeinpatientssensitivetoragweed.NEnglJMed. 1984;310:1626---30.
4.Miadonna A, Tedeschi A, Leggieri E. Behaviour and clinical relevance of histamine and leukotrienes C4 and B4 in grass pollen-inducedrhinitis.AmRevRespirDis.1987;136:357---62. 5.Knani J, Campbell A, Enander I. Indirect evidence of nasal
inflammationassessedbytitrationofinflammatorymediators andenumerationofcellsinnasalsecretions ofpatientswith chronicrhinitis.JAllergyClinImmunol.1992;90:880.
6.SkonerDP,Lee L,DoyleWJ. Nasalphysiologyand inflamma-torymediators during natural pollen exposure. Ann Allergy. 1990;65:206---10.
7.OkudaM,WataseT,MezawaA,LiuCM.Theroleof leukotriene-D4inallergicrhinitis.AnnAllergy.1988;60:537---40.
8.FokkensWJ,LundVJ,MullolJ,BachertC,AlobidI,BaroodyF, etal.Europeanpositionpaperonrhinosinusitisandnasalpolyps 2012.RhinolSuppl.2012;23Suppl.:1---298.
9.VanCrombruggenK,ZhangN,GevaertP,TomassenP,BachertC. Pathogenesisofchronicrhinosinusitis:inflammation.JAllergy ClinImmunol.2011.
10.Roca-FerrerJ,Garcia-GarciaFJ,PeredaJ,Perez-GonzalezM, PujolsL,AlobidI,etal.ReducedexpressionofCOXsand pro-ductionofprostaglandinE(2)inpatientswithnasalpolypswith orwithout aspirin-intolerantasthma.JAllergy ClinImmunol. 2011;128:66---72.
11.BousquetJ,theARIAWorkshopGroup.Allergicrhinitisandits impactonasthma(ARIA)2008.Allergy.2008;63:8---160. 12.MullolJ,CallejasFB, Méndez-ArancibiaE,FuentesM,Alobid
I,Martínez-Antón A, et al. Montelukast reduceseosinophilic inflammationbyinhibitingbothepithelialcellcytokine secre-tion(GM-CSF,IL-6,IL-8) andeosinophil survival.JBiol Regul HomeostAgents.2010;24:403---11.
13.Di Capite J, Nelson C, Bates G, Parekh AB. Targeting Ca2+
release-activatedCa2+channelchannelsandleukotriene
recep-torsprovidesa novelcombinationstrategyfortreatingnasal polyposis.JAllergyClinImmunol.2009;124:1014---210. 14.Seidman MD, Gurgel RK, Lin SY, Schwartz SR, Baroody
FM, Bonner JR, et al. Clinical practice guideline: aller-gicrhinitisexecutive summary.Otolaryngol Head NeckSurg. 2015;152:197---206.
15.MionO.Rinite.RevBrasMed.2013;70:154---63.
16.DesrosiersM,EvansGA,KeithPK,WrightED,KaplanA,Bouchard J,et al. Canadian clinicalpractice guidelinesfor acute and chronicrhinosinusitis.AllergyAsthmaClinImmunol.2011;7:2. 17.OrlandiRR,KingdomTT,HwangPH,SmithTL,AltJA,Baroody
FM,etal.Internationalconsensusstatementonallergyand rhi-nology:rhinosinusitis.IntForumAllergyRhinol.2016;6Suppl. 1:S22---09.
18.ShaikhN,WaldER.Decongestants,antihistaminesandnasal irri-gationforacutesinusitisinchildren.CochraneDatabaseSyst Rev.2014;10:CD007909.
19.MeltzerEO,RatnerPH,McGrawT.OralphenylephrineHClfor nasal congestion in seasonal allergic rhinitis: a randomized, open-label,placebo-controlled study.J AllergyClinImmunol Pract.2015;3:702---8.
20.FokkensWJ, LundVJ,MullolJ,Bachert C,AlobidI,Baroody F,etal. European position paperonrhinosinusitis and nasal polyps.Rhinology.2012;23:1---298.
21.WallaceDV,DykewiczMS,BernsteinDI,Blessing-MooreJ,Cox L,KhanDA,etal.Thediagnosisandmanagementofrhinitis:an updatedpracticeparameter.JAllergyClinImmunol.2008;122 Suppl.:S1---84.
22.MansfieldLE.Once-dailyimmediate-releasefexofenadineand sustained-releasepseudoephedrinecombination:anew treat-ment option for allergic rhinitis.Expert Opin Pharmacother. 2006;7:941---51.
23.CastellanoF,MautoneG.Decongestantactivityofanew formu-lationofxylometazolinenasalspray:adoubleblind,randomized versus placebo and reference drugs controlled, dose---effect study.DrugsExpClinRes.2002;28:27---35.
24.SussmanGL,MasonJ, ComptonD,StewartJ,Ricard N.The efficacyandsafetyoffexofenadineHClandpseudoephedrine, aloneandincombination,inseasonalallergicrhinitis.JAllergy ClinImmunol.1999;104:100---6.
25.Meltzer EO,Malmstrom K, LuS, Prenner BM, WeiLX, Wein-stein SF, et al. Concomitant montelukast and loratadine as treatmentforseasonalallergicrhinitis:arandomized, placebo-controlled clinical trial. J Allergy Clin Immunol. 2000;105: 917---22.
26.Watanasomsiri A,Poachanukoon O, VichyanondP.Efficacyof montelukastandloratadineastreatmentforallergicrhinitisin children.AsianPacJAllergyImmunol.2008;26:89---95. 27.SimonsFE, JohnstonL, GuX,Simons KJ.Suppressionofthe
earlyandlatecutaneousallergicresponsesusingfexofenadine andmontelukast.AnnAllergyAsthmaImmunol.2001;86:44---50. 28.CiebiadaM,Gorska-CiebiadaM,BarylskiM,KmiecikT,GorskiP. Useofmontelukastaloneorincombinationwithdesloratadine orlevocetirizineinpatientswithpersistentallergicrhinitis.Am JRhinolAllergy.2011;25:e1---6.
29.KurowskiM,KunaP,GórskiP.Montelukastpluscetirizineinthe prophylactictreatmentofseasonalallergicrhinitis:influence onclinicalsymptomsandnasalallergicinflammation.Allergy. 2004;59:280---8.
30.Grainger J, Drake-Lee A. Montelukast in allergic rhinitis: a systematic review and meta-analysis. Clin Otolaryngol. 2006;31:360---7.
31.CiebiadaM,CiebiadaMG,KmiecikT,DuBuskeLM,GorskiP. Qual-ityoflifeinpatientswithpersistentallergicrhinitistreated withmontelukastaloneorincombinationwithlevocetirizineor desloratadine.JInvestigAllergolClinImmunol.2008;18:343---9. 32.GuptaV,MatrejaPS.Efficacyofmontelukastandlevocetirizine astreatmentforallergicrhinitis.JAllergyTher.2010;1:103. 33.CingiC,GunhanK,Gage-WhiteL,UnluH.Efficacyofleukotriene
antagonistsasconcomitanttherapyinallergicrhinitis. Laryn-goscope.2010;120:1718---23.
34.YamamotoH,YamadaT,SakashitaM,KuboS,SusukiD,Tokunaga T,etal.Efficacyofprophylactictreatmentwithmontelukast and montelukastplusadd-on loratadinefor seasonalallergic rhinitis.AllergyAsthmaProc.2012;33:e17---22.
35.Nayak AS, Philip G, Lu S, Malice MP, Reiss TF, Montelukast Fall Rhinitis Investigator Group. Efficacy and tolerability of montelukast aloneor incombination withloratadine in sea-sonalallergicrhinitis:amulticenter,randomized,double-blind, placebo-controlled trial performed in the fall. Ann Allergy AsthmaImmunol.2002;88:592---600.
36.Lipworth BJ. Leukotriene-receptor antagonists. Lancet. 1999;353:57---62.
37.SheardP.Selectiveinhibitorofslowreactingsubstanceof ana-phylaxis.NatNewBiol.1973;245:215---7.
38.AsherMI,KeilU,AndersonHR,BeasleyR,CraneJ,MartinezF, etal.Internationalstudyofasthmaandallergiesinchildhood (ISAAC):rationaleandmethods.EurRespirJ.1995;8:483---91. 39.Drazen JM,Israel E,O’Byrne PM.Treatmentofasthma with
drugs modifying the leukotriene pathway. N Engl J Med. 1999;340:197---206.
41.GaneJ,BuckleyR.Leukotrienereceptorantagonistsinallergic eyedisease:asystematicreviewandmeta-analysis.JAllergy ClinImmunolPract.2013;1:65---74.
42.deSilvaNL,DamayanthiH,RajapakseAC,RodrigoC,Rajapakse S.Leukotrienereceptorantagonistsforchronicurticaria:a sys-tematicreview.AllergyAsthmaClinImmunol.2014;10:24. 43.GINA. Global Initiative for Asthma. Global Strategy for
Asthma management and prevention. Revised 2014; 2016 www.ginasthma.org[accessed30March].
44.BacharierLB,BonerA,CarlsenKH,EigenmannPA,FrischerT, Götz M, et al.,European PediatricAsthma Group.Diagnosis andtreatmentofasthmainchildhood:aPRACTALLconsensus report.Allergy.2008;1:5---34.
45.RavasiS, CapraV,Panigalli T,Rovati GE,Nicosia S. Pharma-cologicaldifferencesamongCysLT1receptorantagonistswith respecttoLTC4andLTD4inhumanlungparenchyma.Biochem Pharmacol.2002;63:1537---46.
46.ChauhanBF,DucharmeFM.Anti-leukotrieneagentscomparedto inhaledcorticosteroidsinthemanagementofrecurrentand/or chronicasthmainadultsandchildren.CochraneDatabaseSyst Rev.2012;5:CD002314.
47.BisgaardH, SkonerD,Boza ML,TozziCA,Newcomb K,Reiss TF, et al. Safetyand tolerabilityof montelukastin placebo-controlled pediatricstudies and theiropen-label extensions. PediatrPulmonol.2009;44:568---79.
48.ActisGC,BugianesiE,OttobrelliA,RizzettoM.Fatalliver fail-urefollowingfoodsupplementsduringchronictreatmentwith montelukast.DigLiverDis.2007;39:953---5.
49.Kocyigit A, GulcanOksuz B,Yarar F,UzunF,Igde M, Islek I. Hallucination development withmontelukast in a child with asthma: casepresentation. Iran J Allergy Asthma Immunol. 2013;12:397---9.
50.Ibarra-Barrueta O, Palacios-Zabalza I, Mora-Atorrasagasti O, Mayo-SuarezJ.Effectofconcomitantuseofmontelukastand efavirenz on neuropsychiatric adverse events. Ann Pharma-cother.2014;48:145---8.
51.Callero-Viera A, Infante S, Fuentes-Aparicio V, Zapatero L, Alonso-LebreroE.Neuropsychiatricreactions tomontelukast. JInvestigAllergolClinImmunol.2012;22:452---3.
52.SchumockGT,StaynerLT,ValuckRJ,JooMJ,GibbonsRD,LeeTA. Riskofsuicideattemptinasthmaticchildrenandyoungadults prescribedleukotriene-modifyingagents:anestedcase---control study.JAllergyClinImmunol.2012;130:368---75.
53.Sabbagh R, Sheikh-Taha M. Possible montelukast-induced angioedema.AmJHealthSystPharm.2009;66:1705---6. 54.Spertini F. Le syndrome de Churg-Strauss. Rev Med Suisse
Romande.1995;115:147---51.
55.Minciullo PL, Saija A, Bonanno D, Ferlazzo E, Gangemi S. Montelukast-inducedgeneralizedurticaria.AnnPharmacother. 2004;38:999---1001.
56.IncecikF,OnlenY,SangunO,AkogluS.Probable montelukast-inducedhepatotoxicityinapediatricpatient:casereport.Ann SaudiMed.2007;27:462---3.
57.ChengH,LeffJA,AminR,GertzBJ,DeSmetM,NoonanN,etal. Pharmacokinetics, bioavailability, and safety of montelukast sodium(MK-0476)inhealthymalesandfemales. Pharmaceut Res.1996;13:445---8.
58.Lichtenstein LM. The effect of leukotriene antagonist on the early responseto antigen. Otolaryngol Head Neck Surg. 1990;102:219---24.
59.DonnellyAL,GlassM,MinkwitzMC,CasaleTB.Theleukotriene D4 receptor antagonist, ICI2 204,219, relieves symptoms of acute seasonals rhinitis. Am J Respir Crit Care Med. 1995;151:1734---9.
60.UedaT,TakenoS,FurukidoK,HirakawaK,YajinK.Leukotriene receptor antagonist pranlukast suppresses eosinophil infil-tration and cytokine production in human nasal mucosa
of perennial allergic rhinitis. Ann Otol Rhinol Laryngol. 2003;112:955---61.
61.Goodman MJ, Jhaveri M, Saverno K, Meyer K, Nightengale B.Cost-effectivenessofsecond-generationantihistaminesand montelukastinrelievingallergicrhinitisnasalsymptoms.Am HealthDrugBenefits.2008;1:26---34.
62.ChervinskyP,PhilipG,MaliceMP,BardelasJ,NayakA,Marchal JL,etal.Montelukastfortreatingfallallergicrhinitis:effect ofpollenexposurein3studies.AnnAllergyAsthmaImmunol. 2004;92:367---73.
63.vanAdelsbergJ,PhilipG,LaForceCF,WeinsteinSF,MentenJ, MaliceMP,etal.Randomizedcontrolledtrialevaluatingthe clin-icalbenefitofmontelukastfortreatingspringseasonalallergic rhinitis.AnnAllergyAsthmaImmunol.2003;90:214---22. 64.PatelP,Philip G,YangW, Call R, Horak F,LaForce C,et al.
Randomized, double-blind,placebo-controlled studyof mon-telukast for treating perennial allergic rhinitis. Ann Allergy AsthmaImmunol.2005;95:551---7.
65.GuilemanyJM,AlobidI,MullolJ.Controversiesinthetreatment ofchronicrhinosinusitis.ExpertRevRespirMed.2010;4:463---77. 66.RagabS,ParikhA,DarbyYC,ScaddingGK.Anopenauditof mon-telukast,aleukotrienereceptorantagonist,innasalpolyposis associatedwithasthma.ClinExpAllergy.2001;31:1385---91. 67.KieffDA,BusabaNY.Efficacyofmontelukastinthetreatment
ofnasalpolyposis.AnnOtolRhinolLaryngol.2005;114:941---5. 68.DahlénB,NizankowskaE,SzczeklikA,ZetterströmO,Bochenek
G, Kumlin M,et al.Benefitsfrom addingthe 5-lipoxygenase inhibitorzileutontoconventionaltherapyinaspirin-intolerant asthmatics.AmJRespirCritCareMed.1998;157:1187---94. 69.Parnes SM, Chuma AV. Acute effects of antileukotrienes
on sinonasal polyposis and sinusitis. Ear Nose Throat J. 2000;79:18---20,24---25.
70.NonakaM,SakanushiA,KusamaK,OgiharaN,YagiT.One-year evaluation of combined treatment with an intranasal corti-costeroidandmontelukastforchronicrhinosinusitisassociated withasthma.JNipponMedSch.2010;77:21---8.
71.Pauli C, Fintelmann R, Klemens C, Hilgert E, Jund F, Rasp G, et al. Polyposis nasi-improvement in quality of life by theinfluenceofleukotrienereceptorantagonists. Laryngorhi-nootologie.2007;86:282---6.
72.StewartRA,RamB,HamiltonG,WeinerJ,KaneKJ.Montelukast asanadjuncttooralandinhaledsteroidtherapyinchronicnasal polyposis.Otolaryngology.2008;139:682---7.
73.Mostafa BE, Abdel H, Mohammed HE, Yamani M. Role of leukotrieneinhibitorsinthepostoperativemanagementofnasal polyps.ORLJOtorhinolaryngolRelatSpec.2005;67:148---53. 74.StewartRA,RamB,HamiltonG,WeinerJ,KaneKJ.Montelukast
asanadjuncttooralandinhaledsteroidtherapyinchronicnasal polyposis.OtolaryngolHeadNeckSurg.2008;139:682---7. 75.Dahlen B. The Swedish-Polish treatment study with the
5-lipoxygenaseinhibitorZileutoninaspirin-intolerantasthmatics. JRespirCritCareMed.1995;151:376---80.
76.FergusonBJ,BradleyA,OttoHP.Whensurgery,antibiotics,and steroidsfailtoresolvechronicrhinosinusitis.ImmunolAllergy ClinNAm.2009;29:719---32.
77.AlobidI,MullolJ.Roleofmedicaltherapyinthemanagement ofnasalpolyps.CurrAllergyAsthmaRep.2012;12:144---53. 78.Ramamoorthy S, Cidlowski JA. Corticosteroids: mechanisms
of action in health and disease. Rheum Dis Clin N Am. 2016;42:15---31,vii.
79.SchackeH,DockeWD,AsadullahK.Mechanismsinvolvedinthe sideeffectsofglucocorticoids.PharmacolTher.2002;96:23---4. 80.AntiSMA,GiorgiRDN,ChahadeWB.Antiinflamatórios
hormon-ais:glicocorticoides.Einstein.2008;6Suppl.1:S159---65. 81.BarnesPJ.Corticosteroidresistanceinpatientswithasthmaand
82.VenekampRP,ThompsonMJ,HaywardG,HeneghanCJ,DelMar CB,PereraR,etal.Systemiccorticosteroidsforacutesinusitis. CochraneDatabaseSystRev.2014;25:CD008115.
83.GehannoP, BeauvillainC, BobinS, Chobaut JC, DesaultyA, DubreuilC,etal. Shorttherapy withamoxicillin-clavulanate andcorticosteroidsinacutesinusitis:resultsofamulticentre studyinadults.ScandJInfectDis.2000;32:679---84.
84.Klossek JM,Desmonts-Gohler C,Deslandes B, Coriat F, Bor-dure P, Dubreuil C, et al. Treatment of functional signs of acutemaxillaryrhinosinusitisinadults.Efficacyandtolerance of administrationof oral prednisonefor 3 days [Traitement des signes fonctionnels des rhinosinusites maxillaires aiguës del’adulte. Efficacitéet tolérance dela prednisone admin-istrée par voie orale pendant 3jours]. Presse Méd. 2004; 33:303---9.
85.RudmikL,SolerZM.Medicaltherapiesforadultchronicsinusitis: asystematicreview.JAMA.2015;314:926---39.
86.Martinez-Devesa P, Patiar S. Oral steroids for nasal polyps. CochraneDatabaseSystRev.2011:CD005232.
87.PoetkerDM,JakubowskiLA,LalD,HwangPH,WrightED,Smith TL. Oralcorticosteroidsinthemanagement ofadultchronic rhinosinusitis with and without nasal polyps: an evidence-basedreviewwithrecommendations.IntForumAllergyRhinol. 2013;3:104---20.
88.LalD,HwangPH.Oralcorticosteroidtherapyinchronic rhinosi-nusitiswithoutpolyposis:asystematicreview.IntForumAllergy Rhinol.2011;1:136---43.
89.Pundir V,Pundir J, LancasterG, Baer S,KirklandP, Fokkens WJ,etal.Roleofcorticosteroidsinfunctionalendoscopicsinus surgery - a systematic review and meta-analysis. Rhinology. 2016;54:3---19.
90.Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canon-icaGW,Casale TB,et al. Allergicrhinitisand its impacton asthma(ARIA)guidelines:2010revision.JAllergyClinImmunol. 2010;126:466---76.