BrazJOtorhinolaryngol.2017;83(4):416---419
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Rhinoseptoplasty
in
children
夽
Claudia
Pereira
Maniglia
∗,
José
Victor
Maniglia
FaculdadedeMedicinadeSãoJosédoRioPreto(FAMERP),SãoJosédoRioPreto,SP,Brazil
Received11March2016;accepted27April2016 Availableonline31May2016
KEYWORDS
Nasalseptum
deviation; Child; Rhinoplasty; Septoplasty
Abstract
Introduction:Untreatedseptaland/ornasalpyramiddeviationinchildrenshouldbecorrected assoonaspossible,becausetheycanresultinestheticorfunctionalproblemsyearslater.
Objective:Toreportthesurgicalexperienceintreatingchildrenwithnasalseptumand/ornasal pyramiddeviation.
Methods:Reviewofmedicalrecordsof202children,124(61.4%)malesand78(38.6%)females, between4and16yearsofage(M=11years)whounderwentrhinoplastyand/orseptoplastyin aPediatricOtolaryngologyServiceoftheDept.ofOtolaryngologyandHeadandNeckSurgery betweenJanuary1994andJanuary2010.
Results:Septoplastyperformedin157cases(77.7%);rhinoseptoplastyin23cases(11.4%),and rhinoplastyin22cases(10.9%).
Conclusion:Nasal changes shouldbe corrected inchildren, inorder toprovide harmonious growth,andpreventseveresequelaefoundinmouthbreathers.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Desviodeseptonasal;
Crianc¸a; Rinoplastia; Septoplastia
Rinosseptoplastiaemcrianc¸as
Resumo
Introduc¸ão:Desviodoseptoe/oudapirâmidenasalemcrianc¸as,senãotratado,pode apre-sentarproblemasestéticosoufuncionaisapósanos,devendosercorrigidooquantoantes.
Objetivo:Relatarexperiênciacirúrgicanotratamentodecrianc¸ascomdesviodeseptonasal e/oupirâmidenasal.
Método: Revisãodeprontuáriosde202crianc¸as,sendo124(61,4%)dogêneromasculinoe78 (38,6%)dofeminino,comidadeentre4e16anos(M =11anos);submetidasarinoe/ou sep-toplastianoperíododeJaneirode1994aJaneirode2010,emumServic¸odeOtorrinopediatria doDep.deORLeCirurgiadeCabec¸aePescoc¸o.
夽
Pleasecitethisarticleas:ManigliaCP,ManigliaJV.Rhinoseptoplastyinchildren.BrazJOtorhinolaryngol.2017;83:416---9.
∗Correspondingauthor.
E-mail:[email protected](C.P.Maniglia).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCervico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.019
1808-8694/©2017Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
Rhinoseptoplastyinchildren 417
Resultados: Septoplastiarealizadaem157casos(77,7%);rinosseptoplastiaem23casos(11,4%) erinoplastiaem22casos(10,9%).
Conclusão:Alterac¸õesnasaisdevemsercorrigidasemcrianc¸as,paraproporcionarcrescimento harmônicoeevitarasgravessequelasencontradasnorespiradorbucal.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Although septal and/or nasal pyramid deviation occursin
all age groups, it is most commonly diagnosed in young
adults. Its prevalence varies according to age groups.1,2
Only a minorityis diagnosed or treated in childhood,but untreatedindividualsmaylatermanifest estheticor func-tionalproblems.3
Children with nasal obstruction from any cause may develop serious sequelae and complications related to mouthbreathing.Thepatencyofthenasalpassagesallows propergrowthanddevelopmentofthenasomaxillary com-plex,and,bothcongenitalandacquireddeformities,should becorrectedasearlyaspossible.Conservativemodifications tothe nasal septum and the performance of osteotomies in children donot alter facialgrowth.4 The correctionof
other obstructions should be performed during the same operation.5
Objective
To report a surgical experience in treating children with nasalseptaland/ornasalpyramiddeviation,andto demys-tifytheconceptthatthesurgicalproceduresrecommended forseptalandnasalpyramidcorrectionsshouldonlybe indi-catedafter15yearsofageingirlsand18inboys.
Methods
InaccordancewiththeRegulationsofResearchonHuman Subjects,Resolution 196/96of theMinistryof Health,the presentstudywasapprovedbytheResearchEthics Commit-teeoftheinstitutionunderReportNo.001/2012.
A cross-sectionalretrospective study wasconductedto evaluate the experience of Pediatric Otorhinolaryngology ServiceoftheDepartmentofOtolaryngologyandHeadand NeckSurgeryonthetreatmentofchildrenwithnasalseptal and/ornasalpyramiddeviation,regardlessofthecauseor etiology.Inthestudy,weevaluatedthemedicalrecordsof 202childrenofbothgenderswhowerereferredtothe Pedi-atricOtorhinolaryngologyServicebetweenJanuary1994and January2010.
Fortheselectionofpatientdata,wefollowedthe follow-inginclusioncriteria:pediatricagerange,specificsurgical procedureforseptalandnasalpyramiddeviationcorrection, either associated or not with other concomitant
proce-dures. Exclusion criteria were the presence of corrected orunrepairedcleft lip,congenital defectsof themidline, such as dermoid cyst, teratoma, encephalocele or nasal gliomas, andage older than 16 years.The following data wascollected:gender, ageat thetimeof surgery,typeof nasalsurgicalprocedure,associatedprocedures,outpatient revaluationsandpostoperativecomplications.
Among the 202 medicalrecords of patients evaluated, 124 (61.4%) are males and 78 (38.6%) are females, aged between4and16years,withtheaveragebeing11years.
Patients also underwent associated procedures, when specificallyindicated, inthesamesurgery, includingnasal turbinatesurgerythroughintraturbinalcauterization,adeno and/ortonsillectomy,endoscopicnasalsurgeryand otolog-icalmicrosurgerywithplacementofventilationtube.
Results
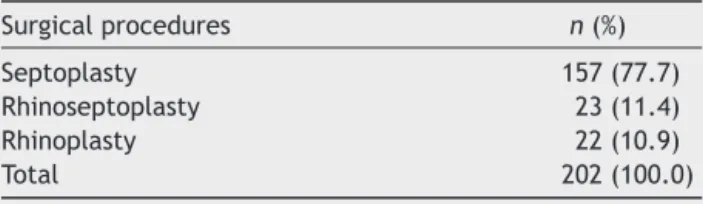
Table1shows therelationship ofsurgical procedures per-formedduringthestudyperiod.Septoplastywasthemost prevalent procedure, being carried out in about 78% of cases.
Among the associated procedures, nasal turbinate surgery was the most commonly performed, in approx-imately 34% of cases, and otological microsurgery with placementofventilationtubewastheoneoflowest preva-lence(0.5%)(Table2).
InaccordancewiththeroutineofthePediatrics Otorhi-nology Service, the method used in all patients for the correctionofseptaldeviationwasminimallyinvasive,with septalmucosahemitransfixionincisionontheconcaveside ofthedeviation,2mmposteriortothecaudaledge,and,on thecaudaldeviations,bilateraltransfixionincision.Careful elevationofmucoperichondriumandmucoperiosteum was performedovertheextentoftheseptum,includingthe high-estpartoftheseptumandthefloor,exposingthenasalspine maxillarycrest. Then,anteriorchondrotomyofthe septal deviation was performed, with subperiosteal detachment
Table1 Distributionofsurgicalproceduresperformed. Surgicalprocedures n(%) Septoplasty 157(77.7) Rhinoseptoplasty 23(11.4) Rhinoplasty 22(10.9)
418 ManigliaCP,ManigliaJV
onthe contralateral side. Posterior, superior and inferior
chondrotomiesallowedtheremovalofthecartilaginous
sep-tumdeviation.Inthepresenceofbonedeviation,thiswas
removedconservatively,withJansen-Middletonforcepsora
4-mmosteotome.Repositioning ofcartilage or bone parts
wasperformedwhenpossible.
Inpatientswithalterationsofthenasalpyramid,withor
without septaldeviation,intercartilaginous incisionswere
madewithdetachmentoftheskintissue,toaccessthenasal
dorsum,remove aboney hump, when present, using
dor-sal scissorsandshaver or double-guarded osteotome.The
surgerywascompletedwithlateralandmedialosteotomies.
No nasal tip surgery with reduction of alar cartilages or
placementofcartilagegraftswasperformed.
The incisionsweresuturedwithVicryl 4-0,with
place-mentof‘‘splint’’mold,whichwasremovedontheseventh
dayaftersurgery,buttherewasnonasalpacking.Currently,
‘‘splint’’moldsareavoided, andmattresssutureare
per-formed.
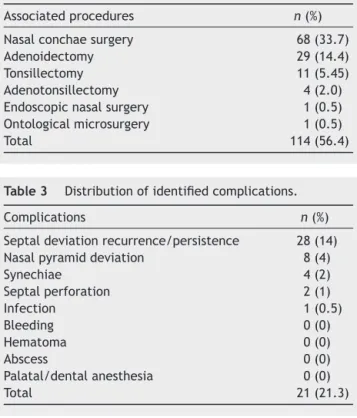
Patientswerereassessedatdays7,30,90and180
post-operatively. Relapse and/or persistence of the deviated
septum was the most frequent complication (14%); there
were no recorded cases of bleeding in the early or late
postoperativeperiod(Table3).
Of the cases that had complications, nine were reop-erated (4.45%), with seven cases being reoperated due todeviated septum (3.5%), onedue to septalperforation (0.5%),andoneduetosynechiae(0.5%).
Discussion
During pregnancy and childhood, several traumas occur affectingtheface,andtheirconsequencesoftengo unde-tected.Thus,thediagnosisofchangesinseptumandnasal
Table2 Distributionofassociatedsurgicalprocedures. Associatedprocedures n(%) Nasalconchaesurgery 68(33.7) Adenoidectomy 29(14.4) Tonsillectomy 11(5.45) Adenotonsillectomy 4(2.0) Endoscopicnasalsurgery 1(0.5) Ontologicalmicrosurgery 1(0.5)
Total 114(56.4)
Table3 Distributionofidentifiedcomplications. Complications n(%) Septaldeviationrecurrence/persistence 28(14) Nasalpyramiddeviation 8(4)
Synechiae 4(2)
Septalperforation 2(1)
Infection 1(0.5)
Bleeding 0(0)
Hematoma 0(0)
Abscess 0(0)
Palatal/dentalanesthesia 0(0)
Total 21(21.3)
bone positionis notoften made, andthe child usually is
takentoaspecialist onlywhenlateestheticand/or
func-tionalproblemsappear.1---3
Congenitalnasalabnormalitiesmustundergosurgeryto improvethespatialrelationshipbetweentheboneandthe softtissue,tomakethenosemorefunctional,andto facil-itatethenormalgrowthstimulus.Acquiredchangesshould alsobecorrectedinordertoavoidaccommodationofsoft tissuestobonemalpositioning,andviciousremodelings.4---6
Electiverhinosurgery(septoplasty,rhinoplasty, rhinosep-toplasty) shouldbeperformed inchildren tocorrectnasal functionandesthetics,aimingtorestoretheanatomyand promotenormaldevelopment.7---10Theresultsof
reconstruc-tiverhinoplastyperformed earlyin lifearecomparableto thoseobtained after theend of growth.The mobilization ofthenasalbonesandnasalseptalreconstructioncanand shouldbeperformedatthesametime.11---16
Possiblesurgicalcomplicationsdescribedinclude persis-tence or recurrence of deviation, deviation of the nasal pyramid,withcosmeticdeformity,bleeding,infection, sep-talhematoma,septalabscess,synechia,septalperforation, palatal and dental anesthesia.17 Changes in cartilaginous
structure, which are more vulnerable in the phases of growth, can lead to a loss of the good results achieved afterinitialsurgery,duetopubertygrowthspurt,leadingto postsurgicaldistortion.Thus,thepossibilityofinappropriate growth ofthe septumwithseptal deviationafter surgery, andnecessityof asecondarysurgeryinthefuture, should alwaysbeclarified.5
Nasalairflowiscrucialforfacialbalanceandgoodnasal physiologicalfunction.Facialdeformityisnotdependenton theobstructioncauseandageatonset.However,the sever-ity, duration and age for correction are essential for the settlementofpossibleimpactoncraniofacialgrowth.18,19
Conclusions
Oursurgical experienceofthe correctionofnasal septum and/ornasalpyramiddeviationinchildrenleadsusto con-clude that, based on clinical improvement and physical examination,thesechangesshouldbecorrectedassoonas possibletoprovideharmoniousgrowthandpreventserious sequelaefoundinmouthbreathers.
Thenasalsurgerythatisperformed earlyinchildren is asafeprocedure,providedthatitis carriedoutcarefully, withappropriateconservationofcartilage,andrespectfor facialgrowthcenters.Thefearofinterruptingfacialgrowth canperpetuatethefunctionalandestheticproblems.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GrayLP.Thedeviatednasalseptum.II.Preventionand treat-ment.JLaryngolOtol.1965;79:806---16.
2.VerwoerdCD,Verwoerd-VerhoefHL.Rhinosurgeryinchildren: basicconcepts.FacialPlastSurg.2007;23:219---30.
Rhinoseptoplastyinchildren 419
4.CardimVLN.Crescimentocraniofacial.In:PsillakisJM,Zanini AS,MélegaJM,CostaEA,CruzRL,editors.Cirurgia Craniomax-ilofacial:osteotomiasestéticasdaface.RiodeJaneiro:Medsi; 1987.p.25---41.
5.ShandilyaM,DenHerderC,DennisSC,NolstTrenitéG. Pedi-atric rhinoplasty in an academic setting. Facial Plast Surg. 2007;23:245---57.
6.EnlowDH.Crescimentofacial.3rded.PortoAlegre:Artes Médi-cas;1993.
7.Zielnik-JurkiewiczB,Olszewska-Sosi´nskaO.Thenasalseptum deformitiesinchildrenandadolescentsfromWarsaw,Poland. IntJPediatrOtorhinolaryngol.2006;70:731---6.
8.D’AscanioL,ManziniM.Safeandrapidapproachtothedeviated nasalseptuminchildren.Laryngoscope.2009;119:2000---3.
9.VerucchiF,Caropreso CA.Indicac¸ões econtra-indicac¸ões da septoplastiaemcrianc¸as.In:VIManualdeOtorrinolaringologia PediátricadaIAPO.Barueri:RRDonnelleyLtda;2007.
10.WillemotJ,PirsigW.Indications,technicandlong-termresults ofsurgeryofthenasalpyramidandseptuminchildren.Acta OtorhinolaryngolBelg.1984;38:427---32.
11.Ortiz-Monasterio F,Olmedo A. Corrective rhinoplasty before puberty:along-termfollow-up.PlastReconstrSurg.1981;68: 381---91.
12.FreerOT.Thewindowresectionoperationforthecorrectionof deflectionsofthenasalseptum.JAMA.1903;XLI:1391---8.
13.KillianG.Thesubmucouswindowresectionofthenasalseptum. AnnOtol.1905;14:363.
14.MurakamiWT,WongLW,DavidsonTM.Applicationsofthe biome-chanical behavior of cartilage to nasal septoplastic surgery. Laryngoscope.1982;92:300---9.
15.DennisSC,denHerderC,ShandilyaM,NolstTrenitéGJ.Open rhinoplastyinchildren.FacialPlastSurg.2007;23:259---66.
16.Costa DB, Anselmo-Lima WT, Tamashiro E, Enoki C, Valera FC. The impact of Metzembaum septoplasty on nasal and facial growth in children. Braz J Otorhinolaryngol. 2013;79: 454---9.
17.TurkJB,CrysdaleWS.Nasalandseptaldeformities.In: Blue-stone CD, Rosenfeld RM, editors. Surgical atlas of pediatric otolaryngology.BCDecker:Ontario;2002.
18.DispenzaF,SaranitiC,Sciandra D,KulamarvaG,Dispenza C. Managementofnaso-septaldeformityinchildhood:long-term results.AurisNasusLarynx.2009;36:665---70.