BrazJOtorhinolaryngol.2016;82(4):466---478
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Influence
of
the
breathing
pattern
on
the
learning
process:
a
systematic
review
of
literature
夽
Genef
Caroline
Andrade
Ribeiro
a,
Isadora
Diniz
dos
Santos
a,
Ana
Claudia
Nascimento
Santos
a,
Luiz
Renato
Paranhos
b,
Carla
Patrícia
Hernandez
Alves
Ribeiro
César
a,∗aDepartmentofSpeechTherapyandAudiology,UniversidadeFederaldeSergipe(UFS),CampusProf.AntônioGarciaFilho,
Lagarto,SE,Brazil
bDepartmentofOdontology,UniversidadeFederaldeSergipe(UFS),CampusProf.AntônioGarciaFilho,Lagarto,SE,Brazil
Received19June2015;accepted7August2015 Availableonline7January2016
KEYWORDS
Mouthbreathing; Learning; Reading; Writing; Mathematics
Abstract
Introduction:Mouthbreathingleadstonegativeconsequencesonqualityoflife,especiallyin school-agechildren.
Objective:Todeterminewhetherthebreathingpatterninfluenceschildren’slearningprocess.
Methods:ThissystematicreviewwascarriedoutaccordingtothePreferredReportingItemsfor SystematicReviewsandMeta-Analyses(PRISMA)instructions,withnorestrictionsregardingthe yearofpublicationandlanguage,createdbasedontheclinicalquestionformulationaccording totheProblem/Patient/Population,Intervention/Indicator,Comparison,Outcome(PICO) strat-egy:‘‘Isthemouth-breathingchildmorelikelytohavelearningdisabilitieswhencomparedto nasal breathers?’’intheSciELO, PubMed,LILACS, andScopus electronicdatabases. Google Scholarwas usedto searchthe grayliterature. The keywords ‘‘learning,’’ ‘‘mouth breath-ing,’’andtheirequivalenttermsinPortuguesewereusedinanintegratedmanner.Thestudies includedinthereview wereobservational,conducted withschoolchildrenaged 7---11years. Afterwards,thestudieswereevaluatedregardingtheirmethodologicalquality.Theresearch wasperformedbytwoeligiblereviewers.
Results:Atotalof357recordswereobtained,ofwhich43recordswereduplicate.After apply-ingtheeligibilitycriteria,tenarticleswereincludedintheresearchscope.Halfofthestudies usedacontrolgroupandotorhinolaryngologicalassessment,whereasaminorityusedvalidated (20%)andsamplecalculationprotocols(10%).Theevaluationprocedureswerevaried.Overall, 80%ofthearticlesshowedahigherincidenceoflearningdisabilitiesamongmouthbreathers.
夽 Pleasecitethisarticleas:RibeiroGCA,dosSantosID,SantosACN,ParanhosLR,CésarCPHAR.Influenceofthebreathingpatternonthe
learningprocess:asystematicreviewofliterature.BrazJOtorhinolaryngol.2016;82:466---78.
∗Correspondingauthor.
E-mail:[email protected](C.P.H.A.R.César).
http://dx.doi.org/10.1016/j.bjorl.2015.08.026
Oralbreathingandlearning:literaturereview 467
Conclusion: Thissystematicreviewhasshownthatmouthbreathersaremorelikelytohave learningdifficultiesthannasalbreathers.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Respirac¸ãobucal; Aprendizagem; Leitura; Escrita; Matemática
Ainfluênciadomodorespiratórionoprocessodeaprendizagem:umarevisão sistemáticadaliteratura
Resumo
Introduc¸ão: Arespirac¸ãooraltrazconsequênciasnegativasparaaqualidadedevidadas pes-soas,principalmenteparaescolares.
Objetivo: Verificarseomodorespiratórioinfluencianoprocessodeaprendizageminfantil.
Método: Esta revisão sistemática foi realizada seguindo as instruc¸ões PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses), sem restric¸ão quanto ao ano depublicac¸ãoeidioma,elaboradaapartirdaformulac¸ãodequestãoclínicaelaboradapela estratégiaP.I.C.O.:‘‘Acrianc¸arespiradoraoraltemmaischancesdeapresentardificuldades
de aprendizagemquandocomparada àrespiradoranasal?’’, nasbasesde dadoseletrônicas
SciELO, PubMed,LILACSeScopus.FoiutilizadooGoogleScholarparapesquisadaliteratura cinza.Aspalavras-chave‘‘aprendizagem’’,‘‘respirac¸ãobucal’’,‘‘learning’’e‘‘mouth breath-ing’’foramutilizadasdeformaintegrada.Osestudosincluídosforamobservacionais,realizados comescolaresentreseteeonzeanos.Emseguida,osestudosforamavaliadosquantoàsua qualidademetodológica.Todaapesquisafoirealizadapordoisrevisoresdeelegibilidade.
Resultados: Foramobtidos357registros,sendo314blindados(43registrosemduplicidade). Apósos critérios de elegibilidade,dez artigosintegraramo escopodesta pesquisa. Metade dos estudosusougrupo controlee fezusodeavaliac¸ãootorrinolaringológica,aminoria fez usodeprotocolosvalidados(20%)edecálculoamostral(10%).Osprocedimentosdeavaliac¸ão foramvariados.Deformageral,80%dosartigosevidenciarammaiorocorrênciadedistúrbiode aprendizagememrespiradoresorais.
Conclusão:Estarevisãosistemáticademonstrouqueindivíduoscomrespirac¸ãooralapresentam maiortendênciadedificuldadesnaaprendizagemdoqueosnasais.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Learning disorders may occur due to multifactorial rea-sons, among which are auditory information processing alterations,1,2 attention deficit, interpersonal relationship
difficulties, behavioral disorders, cognitive deficits, dis-advantaged socioeconomic background,3 family history of
learningdifficultiesanddisabilities,4aswellasothers,such
asmouthbreathing---whichcancompromiselearning.5
When breathingis performed only throughthe mouth, it can be considered a pathological adaptation resulting fromdifficultyofbreathingthroughthenose,6anditresults
in the inspiration of adrier, unfiltered air, at acolder or warmertemperature thantheexpected,which ultimately overwhelmsthetonsilsandthelarynxandcancausechronic inflammation.Ifsuchpathologicaladaptationoccursovera longperiod,itcanresultintonsillarhypertrophyand subse-quently,varyingdegreesofupperairwayobstruction.Thus, there will be resistance to gas flow, permanent increase inenergyexpenditure,andadaptationsthatarestructural
(high-archedpalateanddentalmalocclusion)andfunctional (orofacialmuscleflaccidity,dysphonia,andsleepapnea,for instance),thatcanimpairthequalityofsleep,mood, behav-ior,andschoolperformance,7althoughthereisnosignificant
scientificevidencetosupporttheassociationbetweenthe alteredbreathingpatternandlearningdifficulties.
Consideringthe high prevalence of mouth breathingin childhood8andthepossibilityofitsimpactonlearning,this
study was designed in order toverify, through a system-aticreviewoftheliterature,whetherthisbreathingpattern influenceschildren’slearningprocess.
Methods
468 RibeiroGCAetal.
Searchstrategyandeligibilitycriteria
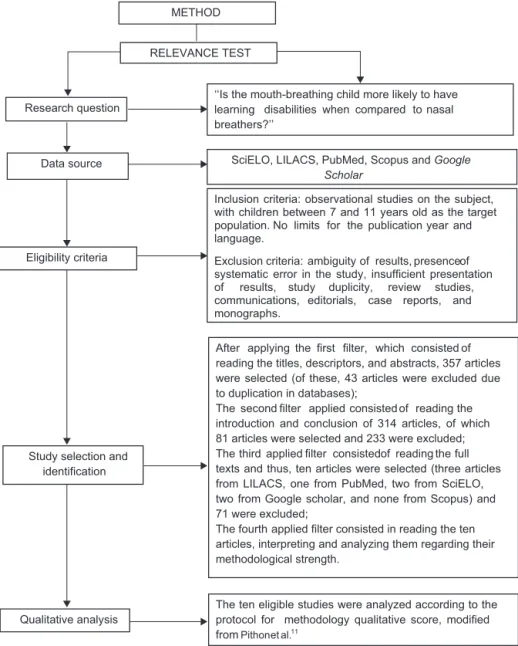
This systematic review study was conducted with no restrictions regarding the year and language of pub-lication. The P.I.C.O strategy was used, considering schoolchildrenwhoweremouthbreathersaged7---11years (P=patient), assessed regarding the aspects related to learning (I=intervention) and compared with schoolchil-drenwhowerenasalbreathers(C=interventioncomparison or control), aiming at verifying the possibility of learn-ing disability in those with altered breathing pattern (O=outcome),usingthefollowingguidingquestion:‘‘Isthe mouth-breathingchildmorelikelytohavelearning disabili-tieswhencomparedtonasalbreathers?’’.
The study designis explainedin Fig.1, withthestudy eligibilitycriteria.Forthestudiesconsideredpreliminarily eligible,thefulltextwasobtainedandassessedinorderto verifywhethertheymetalltheinclusioncriteria.The fol-lowing inclusion criteriawere used: observational studies (controlled, cross-sectional, prospective, or retrospective
longitudinal studies) on the subject, with schoolchildren agedbetween7and11years.
The exclusion criteria were: ambiguous results, poor presentation of results, study duplication based on the database search, review studies, communications, case reports, scientific meeting abstracts, monographs, com-ments,or editorials.Studies regardingsyndromic patients andthosewithintellectualdisabilitieswerealsoexcluded, aswellasregistriesnotdirectlyrelatedtothefinaloutcome ofthisstudy(Fig.1).
The keywords were selected in DeCS (VHL Health Sci-encesDescriptors)andMeSH(PubMed),inordertoidentify relevant studies in the PubMed,SciELO, LILACS, and Sco-pus electronicdatabases.The controlleddescriptorswere ‘‘learning’’and‘‘mouthbreathing,’’‘‘aprendizagem’’and ‘‘respirac¸ãobucal.’’Booleanoperators(ORandAND)were usedfordescriptorcombination.Thisresearchwascarried outonJuly15th,2015.Thegrayliteraturewasidentifiedby searchinginGoogleScholar,byconsultingthefirsthundred recordsofeachcombination.
Data source SciELO, LILACS, PubMed, Scopus and Google Scholar
Eligibility criteria
Inclusion criteria: observational studies on the subject, with children between 7 and 11 years old as the target
and year publication the
for limits No population. language.
of presence results, of ambiguity criteria:
Exclusion
systematic error inthe study, insufficient presentation studies, review
duplicity, study
results, of
and reports, case editorials, communications,
monographs.
Study selection and identification
of consisted which
filter, first the applying After
reading the titles, descriptors, and abstracts, 357 articles were selected (of these, 43 articles were excluded due to duplication in databases);
the reading of consisted applied filter second The
introduction and conclusion of314 articles,of which 81 articles were selected and 233 were excluded;
consisted filter
applied third
The full of reading the
texts and thus, ten articles were selected (three articles from LILACS, one from PubMed, two from SciELO, two from Google scholar, and none from Scopus) and 71 were excluded;
applied filter consisted in reading the ten The fourth
articles, interpreting and analyzing them regarding their methodological strength.
Qualitative analysis
The ten eligible studies were analyzed according to the protocol for methodology qualitative score, modified fromPithonetal.11
METHOD
RELEVANCE TEST
Research question
‘‘Is the mouth-breathing child more likely to have nasal to compared when
disabilities learning
breathers?’’
Oralbreathingandlearning:literaturereview 469
Assessmentprocessvalidityanddataextraction
Afterobtainingthelistofthestudies carriedoutwiththe chosendescriptors,therelevancetestwasappliedandeach studywascarefullyanalyzedbytwoeligibilityreviewers(not blindedtotheauthorsandjournals),whoperformedthe sur-veyindependentlyanddecided,byconsensus,whichstudies wouldbeselected.Incaseofdivergenceofresults,athird reviewer wasconsulted to resolve thequestion regarding whetherthestudyshouldbeincluded,assuggestedbythe literature.10
Initially, article titles, descriptors,and abstracts were identified; the first research filter was applied to select them.Subsequently,basedontheobtainedresults,the sec-ondfilterwasappliedbyreadingthestudyintroductionand conclusion.Ifthearticlewasconsideredeligible,thearticle wasreadinfulland,thus,thethirdfilterwasapplied.
Inthispreliminaryphase,theeligibletextswereassessed for theirmethodologicalstrength,representingthefourth andfinalrelevancetestfilterused.Themethodology quali-tativescoreprotocol,modifiedfromPithonetal.,wasused forthisevaluation11;itallowsamaximumscoreof13points
(Table1).Atthistime,thereviewwasblindedtotheauthors andjournals,toavoidanyselectionbiasandpossible con-flictsofinterest.
It should be noted that the adaptation occurred only whenestablishingthenumberofsubjectsthatshould par-ticipate in the studies (n), asa basis for the sample size calculation relatedtothe study subject, usingan ‘‘n’’of 147subjects basedonthestudyby Menezesetal.,12 who
usedthisnumberastheminimumoneforperformingastudy
withmouthbreathersbetweentheagesbetween8and10 yearsold,i.e.,withinthemeanageofthestudiesincluded inthisresearch.
Thestudiesweresynthesizedanddistributedinachart, containingthe following information: year of publication, typeofstudy,diagnosisandtoolsfordatacollection,sample characterization,mainfindings,andconclusionofthestudy, reportedintheresultssession.
Dataanalysis
Dataanalysiswasperformedqualitatively,asthemethods usedinthestudieswereheterogeneous.
Results
Researchstrategyandmethodologicalassessment
Using the keywords ‘‘respirac¸ão bucal’’ AND ‘‘aprendizagem,’’sevenarticlesfromtheLILACSdatabase were obtained, 2440 articles from the Google Scholar database (of these,the first hundredwere analyzed), six articlesfromScopus,andonefromSciELO.Usingthe key-words ‘‘mouthbreathing’’ AND‘‘learning,’’eightarticles fromLILACS, 147,000 from Google Scholar (of these, the first hundred were analyzed), five from SciELO, and 30 fromthePubMeddatabasewereobtained.Thus,theinitial samplecomprised357articles.
Afterapplyingthefiltersdesignedinthemethod,43 arti-cleswereexcludedafterthefirstfilterwasapplieddueto
Table1 Protocolfor themethodology qualitativescore,modifiedfrom Pithonetal.,11 withamaximum scoreofthirteen points.a
1.Studycharacterization(maximumscore:nine)
A.Adequatedescriptionofthepopulation(maximumscore:two)
Analyzeditems:age,gender,andpatientstatus: Twopointswhenallitemshavebeenachieved; Onepointwhentwoitemshavebeenachieved; Zeropointswhenoneornoitemhasbeenachieved.
B.Descriptionoftheselectioncriteria(maximumscore:one)b
C.Samplesize(maximumscore:two)
Analyzeditem:numberofparticipants:
Twopointswhenthesamplewasequaltoorhigherthan147participants; Onepointwhenthesamplewasbetween117and147participants; Zeropointswhentherewerelessthan117participants.
D.Comparisonwithcontrolgroup(maximumscore:one)b
E.Statedrandomization(maximumscore:one)b
F.Descriptionoftheevaluationcriteriaofthereading,writing,andmathematicsassessment(maximumscore:one)b
G.Descriptionofbreathingassessment(maximumscore:one)b
2.Descriptionofthestudymeasurements(maximumscore:two)
H.Appropriatemethodinrelationtothearticleobjective(maximumscore:one)b
Blindstudyforexaminersandstatistics(maximumscore:one)b 3.Statisticalanalysis(maximumscore:two)
J.Appropriatestatisticaltest(maximumscore:one)b
K.p-Valuepresentation(maximumscore:one)b
470 RibeiroGCAetal.
duplicationinthe databasesand304 for addressing other subjects such as prevalence, behavioral assessment, pos-ture,hearingskills,malocclusion,adultstudies,andstudies inanimals andtreatment (233after thesecond filterand 71 afterthe third), as shown in Fig.1. Thus, the sample consistedoftenarticles.
As for the methodological strength, all (100%) of theincluded studies13---22 showedmoderatemethodological
strength(Table2).
Characteristicsoftheincludedstudies
Of the ten included studies, half (50%) used a control group.13,17,19,20,22Thestudieswerepublishedbetween2003
and2015, withpeakconcentrations in 2003 (two studies, 20%)13,14 and in 2013 (two studies, 20%).20,21 The use of
samplesizecalculationwasachievedinonestudy(10%).22 Table3showsthemaincharacteristicsoftheselected stud-ies.
Theageofthesamplesrangedbetween2and16years, withameanof9.28years.Regardinggender(fromthe stud-iesthatreportedit),mostsubjectsweremales(52.28%).
The proceduresusedforthe assessmentof the partici-pantswere:analysisofrecords/files:two(20%)16,20;
inter-view:four(40%)16,17,19,22;questionnaires:six(60%)13---16,18,21;
clinical evaluation or observation: six (60%)13,15---17,20,21;
otorhinolaryngologicalassessmentdisclosingmouth breath-ing:five(50%),15,17,19,20,22specifictests:six(60%)15,17---19,21,22;
andpuretoneaudiometry:two(20%).17,22
Regardingthedatacollectiontools,theuseofvalidated protocolswasattainedintwostudies17,22(20%ofthesample)
andUemaetal.17 used,amongseveraltests,a grapheme
recognitiontask,throughthelettercancelationtest,while Kuroishiet al.22 usedthe Academic Performance Test, in
partialform.
Mouth breathers showed greater difficulty in solving mathematical operations than nasal breathers.19,22
How-ever, some researchers21 found no difficulty regarding
mathematicaloperationsintheirstudy.
Reading comprehension was considered worse in the mouthbreathers,22aswellaswriting.21
Overall,eightstudies(80%)14---20,22reportedlearning
dis-abilities in mouth breathers, with three (30%) related to tonsillar or inferior turbinate hypertrophy,15,19,22 three
(30%) due to sleep-disordered breathing,14,17,18 two (20%)
tonasalobstruction20,22andallergicrhinitis(20%),15,19 one
(10%)associatedwithattentiondeficithyperactivity disor-der (ADHD),16 one (10%) due to asthma,18 and one (10%)
to septal deviation.22 Of the studies that found no
asso-ciation between mouth breathing and learning disability (n=2;20%),13,21 onewasrelatedtonasalobstruction13 and
another21didnotdividethegroupsbetweenmouthandnasal
breathers,classifyingtheparticipantsashavingrespiratory impairmentfeatures,withoutspecifyingthecause.
Discussion
School failures occur for different reasons; according to the last census,conducted by Instituto Nacional de Estu-dosePesquisasEducacionaisAnísioTeixeira23(INEP,BRASIL,
2013),in2013,6.1% ofstudentsfailtopass ontothe fol-lowing grade,withoneofthe reasonsbeingthe presence of learning disabilities. Literature has described several factors for its emergence, such as hearing,1,2 attention,
interpersonalrelationships,behaviorandcognition disabili-ties,socioeconomicstatus,3familyhistory,4aswellasmouth
breathing.5
This respiratory pattern is considered a pathological adaptation6,whichcan affectthe qualityofsleep,mood,
behavior,andschoolperformance7;however,therearefew
studiesthat showsuchinterrelation.Moreover,the preva-lenceof mouthbreathingis considered highin childhood8
and,thus,thepresentsystematicreviewwascarriedout. As shown by the sample composition, little has been investigatedonthesubject(2.8% of357 studies), demon-stratingtheneedforfurtherstudiesinthisarea.
Half of the studies in the sample used a control group,13,17,19,20,22 and it is noteworthy that Kajihara and
Nishimura19comparedtheirresultswiththecontrolgroupof
anotherstudy,althoughtheybelongedtothesameresearch group.Thus,itissuggestedthatstudiesonthesubjectwith controlgroupsbeperformedtoattaingreaterresult reliabil-ity.Additionally,forevidence-basedpractice,thatis,fora professionaldecisiontobemadebasedontheobtained sci-entificresults,accordingtoMuirGray24itisidealwhensuch
studiesshowhighevidencestrength,whichareusually con-trolledandrandomizedstudies;suchrandomizedcontrolled studieswerenotidentifiedinoursample.
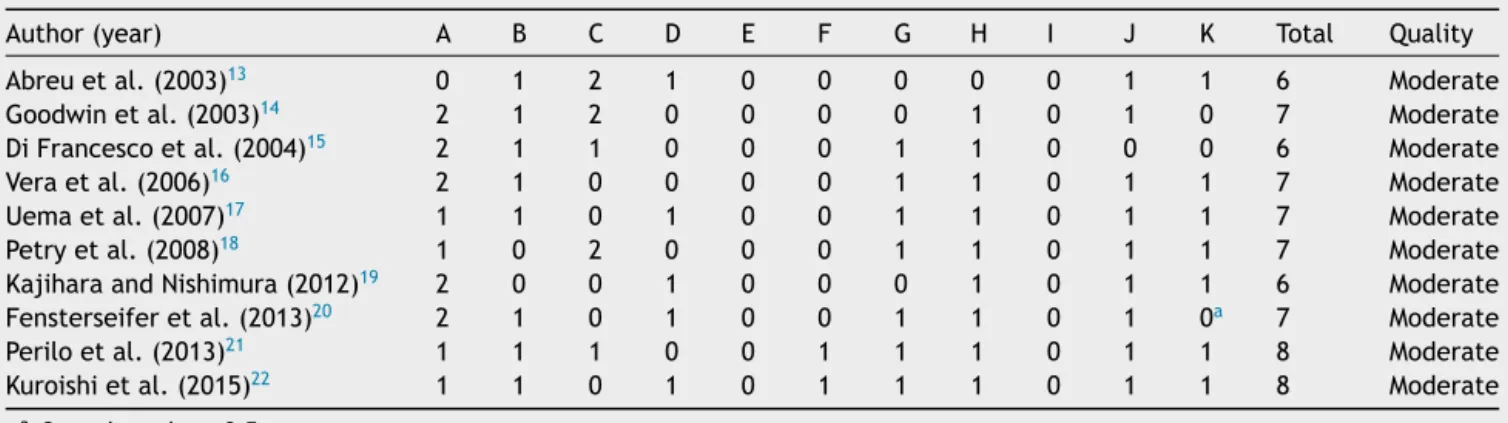
Table2 ScoresobtainedafterapplyingtheMethodologyQualitativeScoreProtocol,adaptedfromPithonetal.11
Author(year) A B C D E F G H I J K Total Quality
Abreuetal.(2003)13 0 1 2 1 0 0 0 0 0 1 1 6 Moderate
Goodwinetal.(2003)14 2 1 2 0 0 0 0 1 0 1 0 7 Moderate
DiFrancescoetal.(2004)15 2 1 1 0 0 0 1 1 0 0 0 6 Moderate
Veraetal.(2006)16 2 1 0 0 0 0 1 1 0 1 1 7 Moderate
Uemaetal.(2007)17 1 1 0 1 0 0 1 1 0 1 1 7 Moderate
Petryetal.(2008)18 1 0 2 0 0 0 1 1 0 1 1 7 Moderate
KajiharaandNishimura(2012)19 2 0 0 1 0 0 0 1 0 1 1 6 Moderate
Fensterseiferetal.(2013)20 2 1 0 1 0 0 1 1 0 1 0a 7 Moderate
Periloetal.(2013)21 1 1 1 0 0 1 1 1 0 1 1 8 Moderate
Kuroishietal.(2015)22 1 1 0 1 0 1 1 1 0 1 1 8 Moderate
Oral
breathing
and
learning:
literature
review
471
Table3 Summaryofthetenarticlesthatcomprisedthestudysampleonthesubject‘‘mouthbreathingandlearning’’.
Author,year, andplaceof study
Diagnosisandinstrumentfordata collection
Samplecharacterization Mainresults Studyconclusion
Abreuetal. (2003),13Sao Paulo,Sao Paulo,Brazil
-Questionnairesaddressedat:teachers onschoolperformance(2ndhalfof 2001)andparents/guardians; -Medicalandclinicalassessment(the proceduresusedwerenotmentioned); -Statisticalanalysis:chi-squaredtest, withsignificancelevelof5%
-330students(ages,means,and genderdistributionwerenot mentioned);
-30mouthbreatherswithupper airwayobstruction;
-300nasalbreathers(control); -ElementarySchoolStudents(2nd to4thgraders)and
-Studentswererequiredtobe attendingtheappropriateschool yearforage
-Changesinacademicperformance werementionedin20%(n=6)of studentsinthestudygroupandin14% (n=42)ofthecontrolgroup,showinga p-value>5%
Mouthbreathingdid notinfluenceschool performanceofthe assessedchildren
Goodwinetal. (2003),14 Tucson, Arizona, UnitedStates ofAmerica
-Standardizedquestionnaire,not validated,addressedto
parents/guardiansonsleephabits (TuCASA);
-Polysomnographyathomeand -Statisticalanalysis:chi-squared(5%of significance),simplelogisticregression, andoddsratiocalculation(confidence intervalnotstated)
1494CaucasianandHispanic children;
-613malesand601females(280 formswithoutgender
identification);
-Groupsdividedbyagerange:1) Between4and7years(n=763, 53.9%)andbetween8and11 years(n=653;46.1%); -78formswithoutage
identification.Themeanageof thegroupswasnotmentioned
-Therewasnosignificantdifference betweengroupsforthepresenceof snoring,excessivedaytimesleepiness andwitnessedapnea,buttherewere significantdifferencesregardingthese characteristicswiththereported learningdisabilities;
-Significantprevalenceoflearning disabilitiesinthegroupofolder children;
-Therewerenosignificantresultswhen comparingthelearningdisabilitieswith thegendervariable
-Hispanicchildren hadahigher frequencyof symptomsof sleep-disordered breathing,snoring, excessivedaytime sleepiness,witnessed apneaandlearning disordersthanwhite children;
-Childrenwith learningdisorder complaintshadhigher chancesofhaving snoring(2.4×)
excessivedaytime sleepiness(2.5×)and
472
Ribeiro
GCA
et
al.
Table3(Continued)
Author,year, andplaceof study
Diagnosisandinstrumentfordata collection
Samplecharacterization Mainresults Studyconclusion
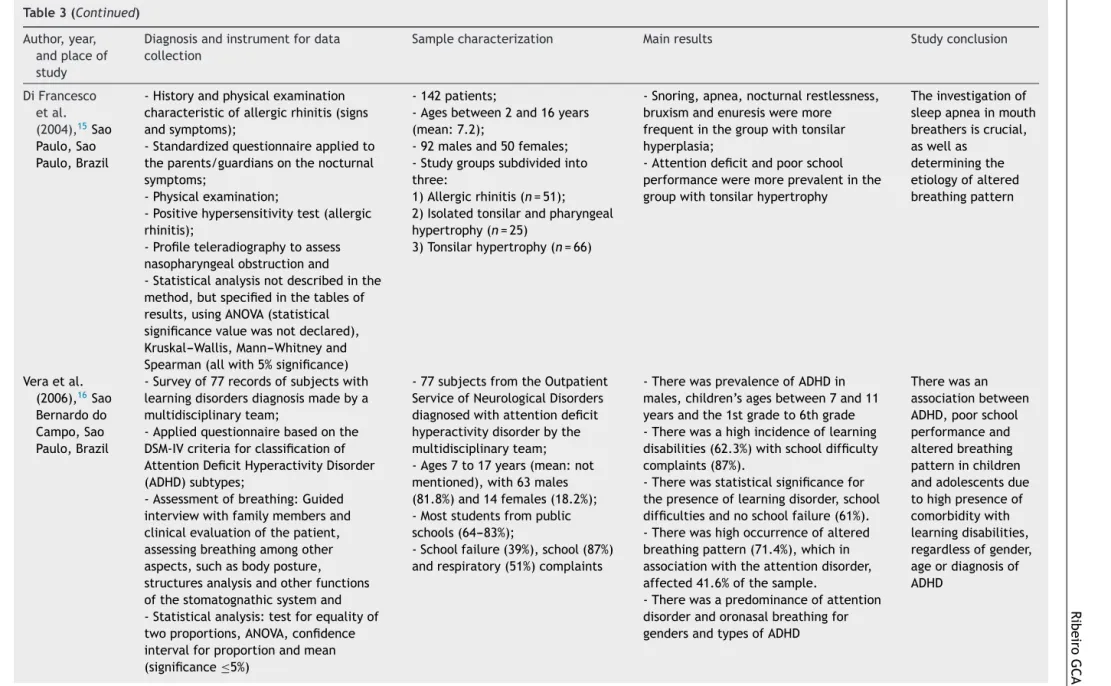
DiFrancesco etal. (2004),15Sao Paulo,Sao Paulo,Brazil
-Historyandphysicalexamination characteristicofallergicrhinitis(signs andsymptoms);
-Standardizedquestionnaireappliedto theparents/guardiansonthenocturnal symptoms;
-Physicalexamination;
-Positivehypersensitivitytest(allergic rhinitis);
-Profileteleradiographytoassess nasopharyngealobstructionand -Statisticalanalysisnotdescribedinthe method,butspecifiedinthetablesof results,usingANOVA(statistical significancevaluewasnotdeclared), Kruskal---Wallis,Mann---Whitneyand Spearman(allwith5%significance)
-142patients;
-Agesbetween2and16years (mean:7.2);
-92malesand50females; -Studygroupssubdividedinto three:
1)Allergicrhinitis(n=51); 2)Isolatedtonsilarandpharyngeal hypertrophy(n=25)
3)Tonsilarhypertrophy(n=66)
-Snoring,apnea,nocturnalrestlessness, bruxismandenuresisweremore frequentinthegroupwithtonsilar hyperplasia;
-Attentiondeficitandpoorschool performanceweremoreprevalentinthe groupwithtonsilarhypertrophy
Theinvestigationof sleepapneainmouth breathersiscrucial, aswellas
determiningthe etiologyofaltered breathingpattern
Veraetal. (2006),16Sao Bernardodo Campo,Sao Paulo,Brazil
-Surveyof77recordsofsubjectswith learningdisordersdiagnosismadebya multidisciplinaryteam;
-Appliedquestionnairebasedonthe DSM-IVcriteriaforclassificationof AttentionDeficitHyperactivityDisorder (ADHD)subtypes;
-Assessmentofbreathing:Guided interviewwithfamilymembersand clinicalevaluationofthepatient, assessingbreathingamongother aspects,suchasbodyposture, structuresanalysisandotherfunctions ofthestomatognathicsystemand -Statisticalanalysis:testforequalityof twoproportions,ANOVA,confidence intervalforproportionandmean (significance≤5%)
-77subjectsfromtheOutpatient ServiceofNeurologicalDisorders diagnosedwithattentiondeficit hyperactivitydisorderbythe multidisciplinaryteam; -Ages7to17years(mean:not mentioned),with63males (81.8%)and14females(18.2%); -Moststudentsfrompublic schools(64---83%);
-Schoolfailure(39%),school(87%) andrespiratory(51%)complaints
-TherewasprevalenceofADHDin males,children’sagesbetween7and11 yearsandthe1stgradeto6thgrade -Therewasahighincidenceoflearning disabilities(62.3%)withschooldifficulty complaints(87%).
-Therewasstatisticalsignificancefor thepresenceoflearningdisorder,school difficultiesandnoschoolfailure(61%). -Therewashighoccurrenceofaltered breathingpattern(71.4%),whichin associationwiththeattentiondisorder, affected41.6%ofthesample.
-Therewasapredominanceofattention disorderandoronasalbreathingfor gendersandtypesofADHD
Oral
breathing
and
learning:
literature
review
473
Table3(Continued)
Author,year, andplaceof study
Diagnosisandinstrumentfordata collection
Samplecharacterization Mainresults Studyconclusion
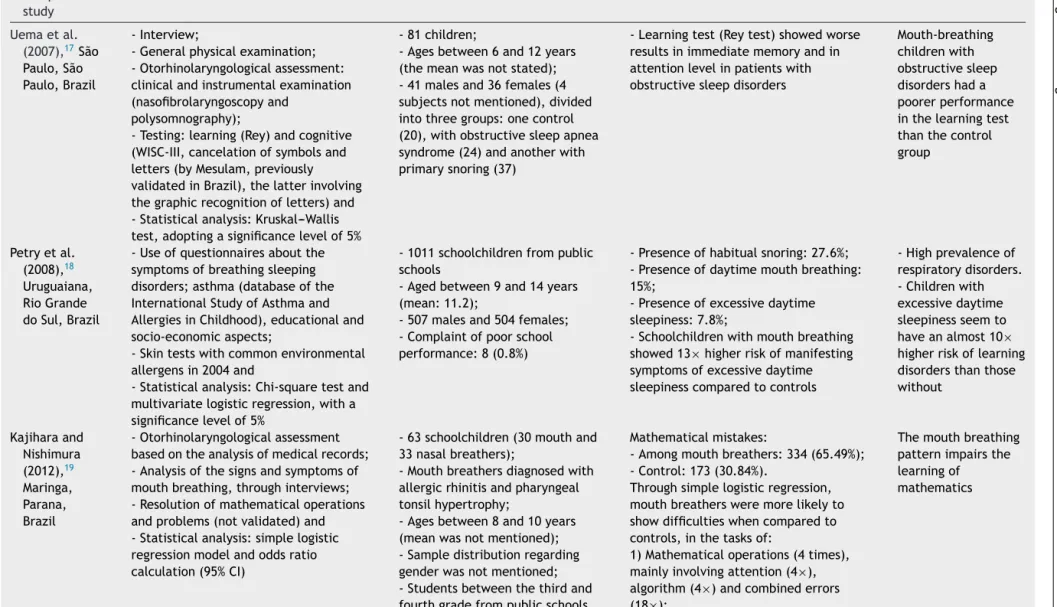
Uemaetal. (2007),17São Paulo,São Paulo,Brazil
-Interview;
-Generalphysicalexamination; -Otorhinolaryngologicalassessment: clinicalandinstrumentalexamination (nasofibrolaryngoscopyand
polysomnography);
-Testing:learning(Rey)andcognitive (WISC-III,cancelationofsymbolsand letters(byMesulam,previously validatedinBrazil),thelatterinvolving thegraphicrecognitionofletters)and -Statisticalanalysis:Kruskal---Wallis test,adoptingasignificancelevelof5%
-81children;
-Agesbetween6and12years (themeanwasnotstated); -41malesand36females(4 subjectsnotmentioned),divided intothreegroups:onecontrol (20),withobstructivesleepapnea syndrome(24)andanotherwith primarysnoring(37)
-Learningtest(Reytest)showedworse resultsinimmediatememoryandin attentionlevelinpatientswith obstructivesleepdisorders
Mouth-breathing childrenwith obstructivesleep disordershada poorerperformance inthelearningtest thanthecontrol group
Petryetal. (2008),18 Uruguaiana, RioGrande doSul,Brazil
-Useofquestionnairesaboutthe symptomsofbreathingsleeping disorders;asthma(databaseofthe InternationalStudyofAsthmaand AllergiesinChildhood),educationaland socio-economicaspects;
-Skintestswithcommonenvironmental allergensin2004and
-Statisticalanalysis:Chi-squaretestand multivariatelogisticregression,witha significancelevelof5%
-1011schoolchildrenfrompublic schools
-Agedbetween9and14years (mean:11.2);
-507malesand504females; -Complaintofpoorschool performance:8(0.8%)
-Presenceofhabitualsnoring:27.6%; -Presenceofdaytimemouthbreathing: 15%;
-Presenceofexcessivedaytime sleepiness:7.8%;
-Schoolchildrenwithmouthbreathing showed13×higherriskofmanifesting
symptomsofexcessivedaytime sleepinesscomparedtocontrols
-Highprevalenceof respiratorydisorders. -Childrenwith excessivedaytime sleepinessseemto haveanalmost10×
higherriskoflearning disordersthanthose without
Kajiharaand Nishimura (2012),19 Maringa, Parana, Brazil
-Otorhinolaryngologicalassessment basedontheanalysisofmedicalrecords; -Analysisofthesignsandsymptomsof mouthbreathing,throughinterviews; -Resolutionofmathematicaloperations andproblems(notvalidated)and -Statisticalanalysis:simplelogistic regressionmodelandoddsratio calculation(95%CI)
-63schoolchildren(30mouthand 33nasalbreathers);
-Mouthbreathersdiagnosedwith allergicrhinitisandpharyngeal tonsilhypertrophy;
-Agesbetween8and10years (meanwasnotmentioned); -Sampledistributionregarding genderwasnotmentioned; -Studentsbetweenthethirdand fourthgradefrompublicschools
Mathematicalmistakes:
-Amongmouthbreathers:334(65.49%); -Control:173(30.84%).
Throughsimplelogisticregression, mouthbreathersweremorelikelyto showdifficultieswhencomparedto controls,inthetasksof:
1)Mathematicaloperations(4times), mainlyinvolvingattention(4×),
algorithm(4×)andcombinederrors
(18×);
2)Resolutionofmathematicalproblems (8×),withchanceofattentionerrors
(10×)andproblemsinterpretation(9×)
474
Ribeiro
GCA
et
al.
Table3(Continued)
Author,year, andplaceof study
Diagnosisandinstrumentfordata collection
Samplecharacterization Mainresults Studyconclusion
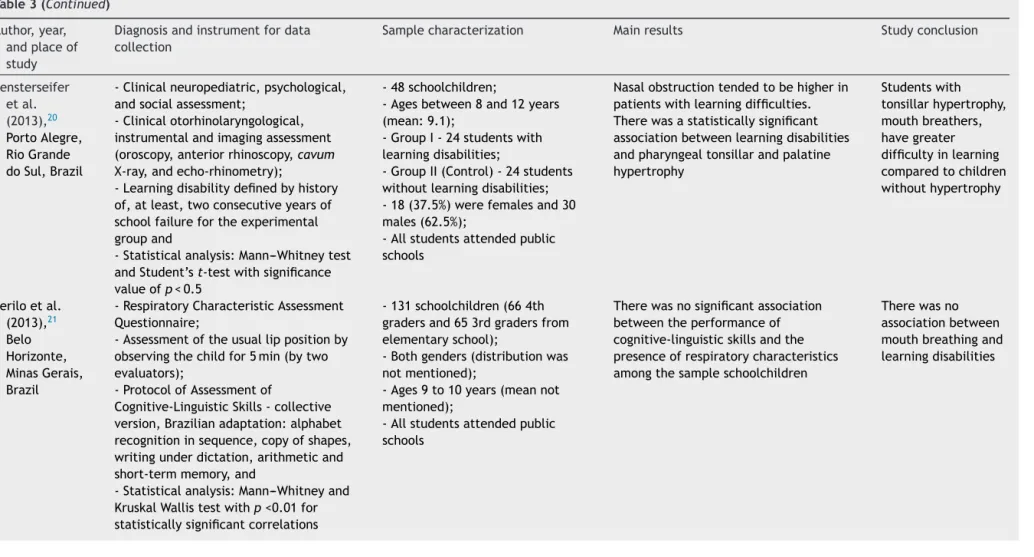
Fensterseifer etal. (2013),20 PortoAlegre, RioGrande doSul,Brazil
-Clinicalneuropediatric,psychological, andsocialassessment;
-Clinicalotorhinolaryngological, instrumentalandimagingassessment (oroscopy,anteriorrhinoscopy,cavum X-ray,andecho-rhinometry);
-Learningdisabilitydefinedbyhistory of,atleast,twoconsecutiveyearsof schoolfailurefortheexperimental groupand
-Statisticalanalysis:Mann---Whitneytest andStudent’st-testwithsignificance valueofp<0.5
-48schoolchildren;
-Agesbetween8and12years (mean:9.1);
-GroupI-24studentswith learningdisabilities;
-GroupII(Control)-24students withoutlearningdisabilities; -18(37.5%)werefemalesand30 males(62.5%);
-Allstudentsattendedpublic schools
Nasalobstructiontendedtobehigherin patientswithlearningdifficulties. Therewasastatisticallysignificant associationbetweenlearningdisabilities andpharyngealtonsillarandpalatine hypertrophy
Studentswith tonsillarhypertrophy, mouthbreathers, havegreater difficultyinlearning comparedtochildren withouthypertrophy
Periloetal. (2013),21 Belo Horizonte, MinasGerais, Brazil
-RespiratoryCharacteristicAssessment Questionnaire;
-Assessmentoftheusuallippositionby observingthechildfor5min(bytwo evaluators);
-ProtocolofAssessmentof
Cognitive-LinguisticSkills-collective version,Brazilianadaptation:alphabet recognitioninsequence,copyofshapes, writingunderdictation,arithmeticand short-termmemory,and
-Statisticalanalysis:Mann---Whitneyand KruskalWallistestwithp<0.01for statisticallysignificantcorrelations
-131schoolchildren(664th gradersand653rdgradersfrom elementaryschool);
-Bothgenders(distributionwas notmentioned);
-Ages9to10years(meannot mentioned);
-Allstudentsattendedpublic schools
Therewasnosignificantassociation betweentheperformanceof cognitive-linguisticskillsandthe presenceofrespiratorycharacteristics amongthesampleschoolchildren
Oral
breathing
and
learning:
literature
review
475
Table3(Continued)
Author,year, andplaceof study
Diagnosisandinstrumentfordata collection
Samplecharacterization Mainresults Studyconclusion
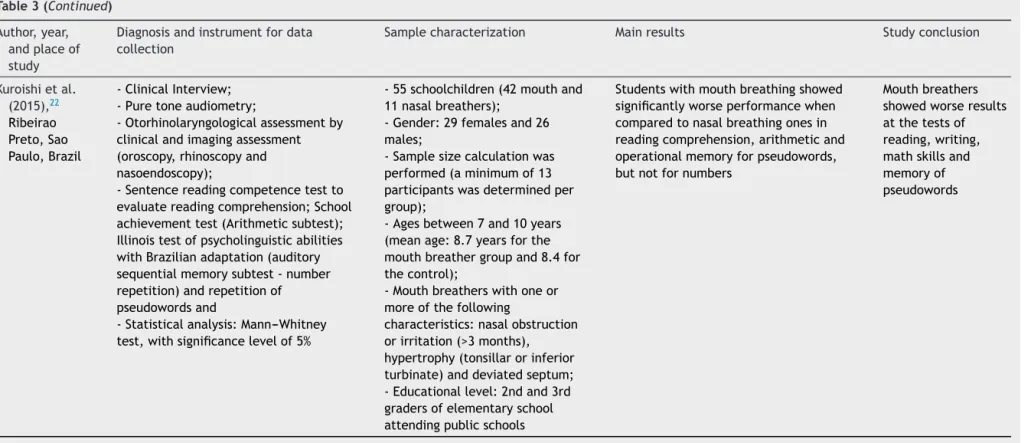
Kuroishietal. (2015),22 Ribeirao Preto,Sao Paulo,Brazil
-ClinicalInterview; -Puretoneaudiometry;
-Otorhinolaryngologicalassessmentby clinicalandimagingassessment (oroscopy,rhinoscopyand nasoendoscopy);
-Sentencereadingcompetencetestto evaluatereadingcomprehension;School achievementtest(Arithmeticsubtest); Illinoistestofpsycholinguisticabilities withBrazilianadaptation(auditory sequentialmemorysubtest-number repetition)andrepetitionof pseudowordsand
-Statisticalanalysis:Mann---Whitney test,withsignificancelevelof5%
-55schoolchildren(42mouthand 11nasalbreathers);
-Gender:29femalesand26 males;
-Samplesizecalculationwas performed(aminimumof13 participantswasdeterminedper group);
-Agesbetween7and10years (meanage:8.7yearsforthe mouthbreathergroupand8.4for thecontrol);
-Mouthbreatherswithoneor moreofthefollowing
characteristics:nasalobstruction orirritation(>3months), hypertrophy(tonsillarorinferior turbinate)anddeviatedseptum; -Educationallevel:2ndand3rd gradersofelementaryschool attendingpublicschools
Studentswithmouthbreathingshowed significantlyworseperformancewhen comparedtonasalbreathingonesin readingcomprehension,arithmeticand operationalmemoryforpseudowords, butnotfornumbers
476 RibeiroGCAetal.
As for the nosological diagnosis confirming the eti-ology of mouth breathing, half of the researchers we studied15,17,19,20,22submittedtheirsamplegroupsto
otorhi-nolaryngological assessment, demonstrating obstructive mouth breathing, although with different etiologies. It shouldalsobenotedthatAbreuetal.13statedthatthestudy
groupunderwentmedicalassessment,butdidnotmention whichspecialtyperformedsuchassessmentorwhat proce-dureswereperformed.
Perilo et al.21 sent a Questionnaire for Assessment
of Respiratory Characteristics, consisting of 22 closed questions with yes/no answers to the parents/guardians. However, the authors’ study, due to the absence of the otorhinolaryngologicalevaluationtoconfirmtheetiologyof thealteredbreathingpattern,didnotmentionthenumber ofaffirmative questionsthat shouldhave been marked in orderto consider the subject a possible mouth breather. Such bias was minimized by observing labial sealing for 5min,observedbytwoevaluatorsduringadistractortask. Thus,theydidnotdividethesampleintomouthandnasal breathers,analyzing therespiratory characteristics ofthe sample and comparing them with the cognitive-linguistic skills.
The assessed studies that comprised the sample used non-probabilisticsamples,chosen intentionallyor by con-venience, that can result in bias in data interpretation as it depends on the researcher’s appraisal. Despite the abovementionedfact,Kuroishietal.22carriedoutasample
calculationstudytodeterminethesample sizethatwould providea morerepresentativepopulation andmore accu-rateresults.25
Although school failure is a complex analysis variable since other aspects can influence its occurrence, it is inferredthatstudentswithlearningdisordershaveagreater chance for failure.Therefore,it wouldbe worthwhilefor studiestoshowwhetherthe sampleconsisted ofstudents thatdidordidnotfailschool.TheresearchbyFensterseifer etal.20establishedaminimumoftwoyears,andthestudy
byVeraetal.16reportedcomplaints(bymostofthefamily
membersofmouthbreathers)oflearningdifficulties,while 39%hadfailed(fromonetothreetimes),moreoftenin ele-mentaryschool.Otherstudies14,15,17---19,21,22didnotmention
schoolfailure,andinthestudybyAbreu etal.,13 the
stu-dentswererequiredtobeattheappropriateschoolyearfor age,i.e.,thosestudentswhofailedwerenotincludedinthe study,whichmaybeconsideredaweakness.
Anotherimportantfactorforanalysisistheplacewhere theselectedstudioes occurredandthetimeperiodduring which the studies were performed, since climate change must be taken into account.26 Most studies in our
sam-plewerecarriedoutbyBrazilianresearchers,13,15---22which
justifies our interest in the subject. Only four studies (40%)13,15,17,20indicatedtheperiod(inmonthsoryears)
dur-ingwhichthesampleselectionwasobtained.
Researchers27 have emphasized the impact of climate
changeonupperairway(UA)disordersinchildrenyounger than 13 years in the metropolitan region of São Paulo, in the months that correspond to the start of winter. Theyaddedthatthepeakofrespiratorydiseasemorbidity occursin May,possiblydue tothermoregulation problems insubjectsadaptedtothemilderclimate/weatherofApril, explainingthatpeoplewiththermoregulationproblemsare
more sensitive torespiratory andcardiovasculardiseases, especiallythepediatricpopulation.
There is an increase in hospital consultations27
dur-ing this period and,consequently, a higher probability of school absenteeism, which can impair academic perfor-mance,dependingonthechronicityofthecondition.
In Brazil, respiratory diseases accounted for 5% of the years of life lost due to premature death,28 emphasizing
the importance of public health measures to reduce this percentage.
Anotheranalysisvariableconcernstheimpactof urban-izationontheliving conditionsandhealthof theBrazilian population. It can be observed that of the ten selected studies,halfwereperformedincapitalcities13,15,17,20,21and
the other half14,16,18,19,22 in well-developed cities. Inlarge
Brazilian cities, according to Maricato,29 there has been
an increase in ecological social inequality, a situation in whichthereisanuncontrolledgrowthofcities,with popula-tionincreaseintheoutskirtregions.Usually,theindividuals livingintheoutskirtsofBraziliancitieshavealow socioeco-nomicstatus(asdemonstratedbyresearch)30and,thus,are
morevulnerabletofactorsthatcancompromisequalityof lifeandhealth.
In addition to the aforementioned facts, it can be observedthatschoolfailureishigherinboysthaningirls, predominantly among African-descendants and/or those fromlow-incomefamilies.30 Thisstudy samplewasmostly
comprised of boys,confirming whatliterature has shown, bothwithrespecttoschoolfailureandthepossibilityofthe presenceofacomorbidityfactor,suchasADHD.16
Thus,itispossibletoconcludethattheunderstandingof thedeterminantsoflearninganditsfailureare multifacto-rialandcomplex;moreover,therearefewvalidated tools toinvestigatelearningdisorders,andthatcreatesdifficulty when comparing the procedures. Only two studies22 used
validated tools, another21 used a published protocol that
was adapted to Brazilian students, and another19 applied
anevaluationtestthatwasusedinadifferentnon-validated study;theremainingstudies13---16,18,20didnotuseassessment
protocols withthe students, butinstead usedschool fail-urerecordsorquestionnairesappliedtofamilymembersor teachers,increasingtheanalysisbiasinsuchstudies.
The School Achievement Test (Teste de Desempenho Escolar --- TDE), developed by Lilian Stein,31 waspartially
usedinonestudy(10%).22 The studycomparedthe
exper-imentalgroupwithacontrolgroup andthesubjectswere matched for age and educational level, with part of the sampleshowingmouthbreathing.Itwasverifiedthatsuch students had lower school performance than the control group in reading comprehension, arithmetic, and working memorytasks(exceptfornumbers).
Regardingtheassessmentofmathematicalskills,two19,22
ofthestudiesthatappliedtestsfoundresultsindicating dif-ficultiesinmouthbreathers,whiletheotheronedidnot.21
Reading comprehension was considered worse in mouth breathers,22 aswellaswritingskillsinsubjectswith
respi-ratorydisordercharacteristics,whencomparedwiththose withoutsuchdisorders.21
Oralbreathingandlearning:literaturereview 477
for analysis was small and showed diverse evaluation procedures.Controlled, interdisciplinarystudies, withthe inclusionofstandardizedassessments,usingvalidatedtools and uniform sample groups must be performed sothat a systematic meta-analysisreview study canbe carried out and,thus,morescientificevidencewillbecomeavailable, both for clinical practice and for the implementation of publichealthandeducationpolicies.
Conclusions
Thereisevidencethatthebreathingpatterncaninfluence the learning process.This systematic review showed that mouthbreathersaremorelikelytohavelearningdifficulties thannasalbreathers.Furtherstudiesareneededinorderto increasethescientificevidenceforclinicalpractice,andfor theimplementationofpublichealthandeducationpolicies.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Pinheiro FH, Capellini SA. Desenvolvimento das habilidades auditivasdeescolarescomdistúrbiodeaprendizagem,antese apóstreinamento auditivo, esuas implicac¸ões educacionais. Rev Psicopedag. 2009;26:231---41. Available from: http:// pepsic.bvsalud.org/scielo.php?pid=S0103-4862009000200008& script=sciarttext[cited10.06.15].
2.WiemesGRM,KozlowskiL,MocellinM,HamerschmidtR,Schuch LH. Potencial evocado cognitivo e desordem de processa-mentoauditivoemcrianc¸ascomdistúrbiosdeleituraeescrita. Braz J Otorhinolaryngol. 2012;78:91---7, http://dx.doi.org/ 10.1590/S1808-86942012000300016[cited10.06.15].
3.FigueiredoVLM,QuevedoL,GomesG,PappenL. Habilidades cognitivasdecrianc¸aseadolescentescomdistúrbiode apren-dizagem.Psico-USF.2007;12:281---90. Available from:http:// pepsic.bvsalud.org/scielo.php?pid=S1413-82712007000200016& script=sciarttext[cited10.06.15].
4.Tabaquim MLM. Avaliac¸ãoneuropsicológica nosdistúrbios de aprendizagem.In:CiascaSM,editor.Distúrbiosde aprendiza-gem:propostadeavaliac¸ãointerdisciplinar.SãoPaulo:Casado Psicólogo;2003.p.91---111.
5.ChedidKAK, DiFrancesco RC,JunqueiraPAS.Ainfluência da respirac¸ãooralnoprocessodeaprendizagemdaleituraeescrita em crianc¸as pré-escolares. Rev Psicopedag.2004;21:157---63. Available from: http://pepsic.bvsalud.org/pdf/psicoped/ v21n65/v21n65a08.pdf[cited10.06.15].
6.DiFrancescoRC.Consequênciasdarespirac¸ãooral.In:Krakauer LH,DiFrancescoRC,MarchesanIQ,editors.Conhecimentopara atenderbemarespirac¸ãooral. SãoJosé dosCampos:Pulso; 2003.p.19---25.
7.Lee JH. O respirador bucal na visão da pediatria. In: Coelho-FerrazMJP,editor.Respiradorbuccal:umavisão mul-tidisciplinar.SãoPaulo:Lovise;2005.p.79---83.
8.De PaulaMVQ, Leite ICG, Werneck RR. Prevalência de por-tadoresda síndromedarespirac¸ãobucal narede escolar do municípiodeJuizdeFora---MG.HURev.2008;34:33---8. Avail-able from: http://http://hurevista.ufjf.emnuvens.com.br/ hurevista/article/view/46/56[cited10.06.15].
9.MoherD,LiberatiA,TetzlaffJ,AltmanDG.Preferredreporting itemsfor systematic reviewsand meta-analyses:thePRISMA
statement. Int J Surg. 2010;8:336---41, http://dx.doi.org/ 10.1371/journal.pmed.1000097[cited15.07.15].
10.McDonald S, Crumley E, Eisinga A, Villanueva E. Search strategiestoidentifyreportsofrandomizedtrialsinMedline: protocolforaCochranereview.Oxford:TheCochraneLibrary; 2006. Available from: http://www.researchgate.net/profile/ ElmerVillanueva/publication/230285759Searchstrategiesto identifyreportsofrandomizedtrialsinMEDLINE/links/ 02bfe50eb83296203c000000.pdf[cited10.06.15].
11.Pithon MM, Sant’Anna LIDA, Baião FCS, SantosRL, Coqueiro RC,MaiaLC.Assessmentoftheeffectivenessofmouthwashes inreducing cariogenicbiofilmin orthodonticpatients: a sys-tematicreview.JDent. 2015;43:297---308,http://dx.doi.org/ 10.1016/j.jdent.2014.12.010[cited01.07.15].
12.Menezes VA, Leal RB, Pessoa RS, Pontes RMES. Prevalência e fatores associados à respirac¸ão oral em escolares par-ticipantes do projeto Santo Amaro-Recife, 2005. Rev Bras Otorrinolaringol. 2006;72:394---9, http://dx.doi.org/10.1590/ S0034-72992006000300017[cited01.07.15].
13.AbreuACB,MoralesDA,BalloMBJF.Arespirac¸ãooral influen-ciao rendimentoescolar.RevCefac.2003;5:69---73.Available from:http://www.cefac.br/revista/revista51/Artigo%2011.pdf [cited15.07.15].
14.Goodwin JL, BabarSI, Kaemingk KL, RosenGM, Morgan WJ, SherrillDL,etal.Symptomsrelatedtosleep-disordered breath-ing in white and Hispanic children: the Tucson Children’s AssessmentofSleepApneaStudy.ChestJ.2003;124:196---203, http://dx.doi.org/10.1378/chest.124.1.196[cited15.07.15]. 15.DiFrancescoRC,PasserotiiG,PaulucciB,MinitiA.Respirac¸ão
oralnacrianc¸a:repercussõesdiferentesdeacordocomo diag-nóstico.RevBrasOtorrinolaringol.2004;70:665---70,http://dx. doi.org/10.1590/S0034-72992004000500014[cited15.07.15]. 16.VeraCFD,CondeGES,WajnsztejnR,NemrK.Transtornosde
aprendizagemepresenc¸aderespirac¸ãooralemindivíduoscom diagnósticodetranstornosdedéficitdeatenc¸ão/hiperatividade (TDAH).RevCefac.2006;8:441---55,http://dx.doi.org/10.1590/ S1516-18462006000400005[cited15.07.15].
17.Uema SFH, Pignatari SSN, Fujita RR, Moreira GA, Pradella-Hallinan M, Weckx L. Avaliac¸ão da func¸ão cognitiva da aprendizagememcrianc¸ascomdistúrbiosobstrutivosdosono. RevBrasOtorrinolaringol.2007;73:315---20,http://dx.doi.org/ 10.1590/S0034-72992007000300005[cited15.07.15].
18.PetryC,PereiraMU,PitrezP,JonesMH,SteinRT.Prevalência de sintomas de distúrbios respiratórios do sono em esco-laresbrasileiros.JPediatr.2008;84:123---9,http://dx.doi.org/ 10.1590/S0021[cited15.07.15].
19.KajiharaOT,NishimuraCM.Respirac¸ãooral:umfatorquepode prejudicaraaprendizagemdamatemática.RevSérie-Estudos. 2012;33:101---18. Available from: http://www.serie-estudos. ucdb.br/index.php/serie-estudos/article/viewFile/78/173 [cited15.07.15].
20.FensterseiferGS,CarpesO,WeckxLLM,MarthaVF.Respirac¸ão bucal em crianc¸as com dificuldade de aprendizado. Braz J Otorhinolaryngol. 2013;79:620---4,http://dx.doi.org/10.5935/ 1808-8694.20130111[cited15.07.15].
21.PeriloTVC,FreitasCS,CardosoNC,MottaAR,AlvesLM. Habil-idadescognitivo-linguísticasesuarelac¸ãocomcaracterísticas respiratórias.Rev Cefac.2013;15:579---91,http://dx.doi.org/ 10.1590/S1516-18462012005000065[cited15.07.15].
22.KuroishiRCS,GarciaRB,ValraFCP,Anselmo-LimaWT,Fukuda MTH. Déficits de memória operacional, compreensão de leitura ehabilidades aritméticas em crianc¸as com síndrome da respirac¸ão oral: estudo transversal analítico. São Paulo MedJ.2015;133:78---83,http://dx.doi.org/10.1590/1516-3180. 2013.7630011[cited15.07.15].
478 RibeiroGCAetal.
24.MuirGrayJA.Evidence-basedhealthcare:howtomakehealth policyandmanagementdecision.Edinburgh:Churchill Living-stone;1997.
25.Normando D, Almeida MADO, Quintão CCA. Análise do empregodocálculoamostraledoerrodométodoempesquisas científicaspublicadasnaliteraturaortodônticanacionale inter-nacional. Dental Press J Orthod. 2011;16:33e1---9. Available from: http://www.scielo.br/pdf/dpjo/v16n6/a06v16n6.pdf [cited10.06.15].
26.Ribeiro WC, Impactos das mudanc¸as climáticas em cidades no brasil. Parcerias Estratégicas. 2008;27:297---321. Avail-able from: http://www.cetesb.sp.gov.br/userfiles/file/ mudancasclimaticas/proclima/file/publicacoes/metropoles/ ribeiroimpactos.pdf[cited10.06.15].
27.Goncalves FLT, Coelho MDSZS. Variac¸ão da morbidade de doenc¸asrespiratórias emfunc¸ãodavariac¸ãodatemperatura entre os meses de abril e maio em São Paulo. Ciênc Nat. 2010;32:103---18. Available from: http://cascavel.ufsm.br/
revistas/ojs2.2.2/index.php/cienciaenatura/article/viewFile/ 9500/5649[cited10.06.15].
28.Schramm JMA, Oliveira AF, Costa Leite I, Valente JG, Gadelha ÂMJ, Portela MC, et al. Transic¸ão epidemiológica e o estudo de carga de doenc¸a no Brasil. Ciênc Saúde Coletiva. 2004;9:897---908, http://dx.doi.org/10.1590/S1413-81232004000400011[cited10.06.15].
29.Maricato E. Urbanismo na periferia do mundo globalizado: metrópoles brasileiras. São Paulo Perspect. 2000;14:21---33, http://dx.doi.org/10.1590/S0102-88392000000400004
[cited10.06.15].
30.Carvalho MP. Quem são os meninos que fracassam na escola? Cad Pesqui. 2004;34:11---40. Available from: http://www.scielo.br/pdf/cp/v34n121/a02n121.pdf [cited 10.06.15].