www.eerp.usp.br/rlae
Corresponding Author: Maritza Espinoza Venegas Victor Lamas, 1290 Concepción, Chile E-mail: [email protected]
Validation of Collett-Lester’s Fear of Death Scale in a sample
of nursing students
Maritza Espinoza Venegas
1Olivia Sanhueza Alvarado
2Omar Barriga
3This study aims to evaluate the psychometric properties of Collett-Lester’s Fear of Death
Scale. A sample of 349 nursing students answered Fear of Death and Attitude toward
death scales. Content validity was checked by expert review; reliability was proven using
Cronbach’s alpha; statistical analysis of the items, correlation between items and construct
validity were checked by the correlation of the Scale with the Attitude toward death Scale.
The multidimensionality of the scale was reviewed through factor analysis with varimax
rotation. The Fear of Death Scale possesses good internal consistency and construct
validity, confirmed by the significant correlation with the Attitude toward death Scale. Factor
analysis partially supports content validity of the subscale items, but presented a modified
multidimensional structure that points towards the reconceptualization of the subscales in
this sample.
Descriptors: Fear; Death; Scales; Reliability; Validity.
1 RN, Doctoral Student, Associate Professor, Departamento de Enfermería, Facultad de Medicina, Concepción, Chile. E-mail:
2 RN, Ph.D. in Nursing, Associate Professor, Departamento de Enfermería, Facultad de Medicina, Concepción, Chile. E-mail:
3 Sociologist, PhD. in Sociology, Associate Professor, Departamento de Sociología, Facultad de Ciencias Sociales, Universidad de
Validação de Escala de Medo da Morte de Collett-Lester em uma amostra de estudantes de enfermagem
O objetivo do presente trabalho foi avaliar as características psicométricas da Escala
de Medo da Morte de Collett-Lester. A amostra foi composta por 349 estudantes de
enfermagem que responderam às perguntas das Escalas de Medo da Morte e de
Atitude diante da Morte. A validade de conteúdo foi realizada por revisão de experts; a
coniabilidade foi veriicada pelo coeiciente alfa de Cronbach e averiguada pela análise
estatística dos elementos e correlação entre elementos e validade de construto, através
da correlação da escala com a Escala de Atitude diante da Morte. Através da análise
fatorial com rotação Varimax, revisou-se a multidimensionalidade da escala. A Escala
Medo da Morte tem boa consistência interna e validade de construto, conirmada pela correlação signiicativa com a Escala de Atitude diante da Morte. A análise fatorial apoia
parcialmente a validade do conteúdo dos itens das subescalas, apresentando, porém,
estrutura multidimensional adicional que orienta para a reconceituação das subescalas
na amostra estudada.
Descritores: Medo; Morte; Escalas; Coniabilidade; Validade.
Validación de la Escala de Miedo a la Muerte de Collett-Lester en una muestra de estudiantes de Enfermería
El presente trabajo tiene el objetivo de evaluar las características psicométricas de la
Escala del Miedo a la Muerte de Collett-Lester. Material y método: una muestra de 349
estudiantes respondieron las Escala de Miedo a la Muerte y Actitud ante la Muerte. La
validez de contenido fue revisada por expertos, la coniabilidad se comprobó mediante el Coeiciente alfa de Cronbach; se veriicó el análisis de los resultados estadísticos,
correlación entre elementos y la validez del constructo a través de la correlación con la
escala: Actitud ante la Muerte. Se revisó la multidimensionalidad de la escala a través
del análisis factorial con el método Rotación Varimax. La Escala Miedo a la Muerte tiene buena consistencia interna y una validez de constructo conirmada por la correlación signiicativa con la otra Escala de Actitud ante la muerte. El análisis factorial apoya
parcialmente la validez de contenido de los ítems de las subescalas, presentado una
estructura multidimensional adicional, que orienta hacia una reconceptualización de las
subescalas en la muestra estudiada.
Descriptores: Miedo; Muerte; Escalas; Fiabilidad; Validez.
Introduction
Fear of death cannot be directly observed, which
is why it should be inferred based on a subject’s
conduct or self-reported answers. Therefore, there is
no simple criterion with which an instrument can be
compared to establish its validity. On the opposite,
the construct validity of any measure of attitudes
towards death is gradually developed over time, as
the evolution of Collett-Lester’s Fear toward Death
Scale (CLFODS) demonstrates. The Scale was created
in 1969 to eliminite the content heterogeneity problem
of the items in the scales used to measure fear of
death. These authors suggested that fear of death
is a multidimensional concept with different possible
causes, which can make a person react differently
to the idea of death as a state and/or as a process.
Likewise, attitudes and emotional reactions can differ
for oneself or for others. Thus, four sub-scales were
distinguished: fear of one’s own death, fear of other
persons’ death, fear of one’s own dying process and
The irst version of the CLFODS included 36
items, with a different number of items for each
sub-scale. Next, in 1994, a revised version was published
that included the same number of items in each
scale (32 items). In 2003, those items in each
sub-scale that did not contribute to the signiicance of Cronbach’s alpha were eliminted, resulting in a inal
28-item version(3).
Also, measuring this construct in the health
construct is relevant because the meaning of death
entails a certain denial and evasion in our society,
which includes health professionals(4-5). The availability
of valid instruments addressing fears of death permit
research that helps to visualize one construct and factor
at a time, which is considered determinant for people’s
end-of-life quality of care(6) and quality of life(7-8).
Although countless instruments have been used
to measure attitudes towards death, most of them
are one-dimensional. Their disadvantage is that they
do not permit the identiication and distinction of speciic elements involved in fears of death. For the
same reason, a trend exists to use well-validated
and multidimensional scales. In recent years,
Collett-Lester’s (2,9-11) multidimensional fear of death instrument
has been validated in several cultural contexts,
evidencing acceptable psychometric characteristics.
Recently, experts have translated the CLFODS
from the original to a Spanish version(12). The
psychometric characteristics exhibited based on a
sample of nursing students and health professionals
were as follows: satisfactory reliability, good internal
consistency and, moreover, the extracted component
offered considerable support for the factor validity
of the CLFODS, as opposed to the irst versions
of the instrument. Moreover, the Spanish version
demonstrated convergent and discriminant validity
through a positive correlation with anxiety towards
death and general anxiety(12-13).
In Chile, some instrument have been used, but
these do not display adequate reliability and do not
measure the death phenomenon as a state and, in
turn, as a process, in a multidimensional way(14).
Therefore, in view of positive psychometric
results of the CLFODS in other countries, this research
aims to assess the psychometric characteristics of
reliability and construct validity of the CLFODS –
Spanish version in Chilean nursing students, with a
view to the availability of a multidimensional measure
that permits valuing fear of death not only for use in
nursing, but also in other health professionals.
Method
This study was accomplished at two universities in
Concepción, involving 349 nursing students in the irst to ifth course year, mainly female (80% ), between
17 and 37 years of age (x=21.3 s=2.7). The Fear of
death Scale and the Attitude toward death Scale were
self-applied before the start of a class. Ethical aspects
of this research were guaranteed through review and
approval by the Institutional Review Board of the School
of Medicine and the Nursing Department Head. Next,
students were asked for their written informed consent,
which guaranteed conidentiality, privacy and anonymity
of answers and offered the possibility to withdraw at any
time and/or access to help if speciically asked to the
researcher. Finally, the researchers decided not to reveal
the name of the colleges the students belonged to, due
to the private nature of the research question.
To perform the psychometric assessment of the
CLFODS, irst, the Scale was submitted to expert review
to guarantee the understanding of the items, followed
by a pilot test of the instrument, in which 30 participants
showed good understanding of the scale.
Criterion and construct validity of the instrument
was analyzed involving the deinitive sample(15).
Moreover, the reliability of the original scale was
assessed, followed by exploratory factor analysis.
Reliability was studied through internal consistency,
using Cronbach’s alpha coeficient. It was considered
that the reagents optimally measured between 0.7 and
0.9(16-17).
The validity of the fear of death construct was
analyzed through element statistics, inter-element and
element-total scale correlation. Moreover, concurrent
criterion validity was reviewed through the correlation
between the CLFODS and the Attitude toward death
Scale(14). For the latter analysis, a sample of 133 students
from the total sample was used.
Finally, exploratory factor analysis was accomplished,
which permitted proving whether the factors and
variables that constitute the scale are in line with the
pre-established theory of multidimensionality(18). In this
study, principal component analysis (PCA) with varimax
rotation was used.
Instruments
The Spanish version of Collett-Lester’s Fear of
Death Scale comprises four sub-scales that provide
multidimensional information on the “Fear of one’s own
Rev. Latino-Am. Enfermagem 2011 Sep.-Oct.;19(5):1171-80.
other people’s Death” and the “Fear of other people’s
Dying Process”. In total, it contains 28 items, grouped in four sub-scales with seven items each. The answers
are given on a 1 (nothing) to 5 (much) Likert scale.
Scores are obtained for the total scale and for each sub-dimension, calculating the average of the respective
answers. The highest mean scores indicate greater fear of death or the dying process(18-20).
The Attitude Toward Death Scale (ATD) measures the favorable or unfavorable attitude towards death,
designed with 43 Likert-type items ranging from 1 to 5.
The highest score corresponds to the most unfavorable
attitude towards death(14).
Results
Univariate analysis of the Fear of death variables
relects a trend near the normal curve. The mean fear of
death score among the nursing students was
moderate-high. What the students fear less is their own death. The
highest score per sub-scale corresponded to the fear of
other people’s death (Table 1).
Table 1 – Descriptive statistics of CLFODS
Sub-scale 1 death of self
Sub-scale 2 dying of self
Sub-scale 3 death of others
Sub-scale 4 dying of others
Total average fear of death
Mean 2.92 3.46 3.90 3.37 3.41
Standard deviation .93 .91 .76 .80 .70
Asymmetry .205 -.231 -.699 -.331 -.223
Reliability of the CLFODS
The total internal reliability of the CLFODS
corresponded to 0.91, which indicates that 91% of
the variability in the obtained scores represents actual
differences among people, while 9% relects random
oscillations. Also, for each sub-scale, the obtained
Cronbach’s alpha coeficients permit guaranteeing that
the items or elements are homogeneous and that the
scale consistently measures the characteristic for which
it was elaborated (Table 2).
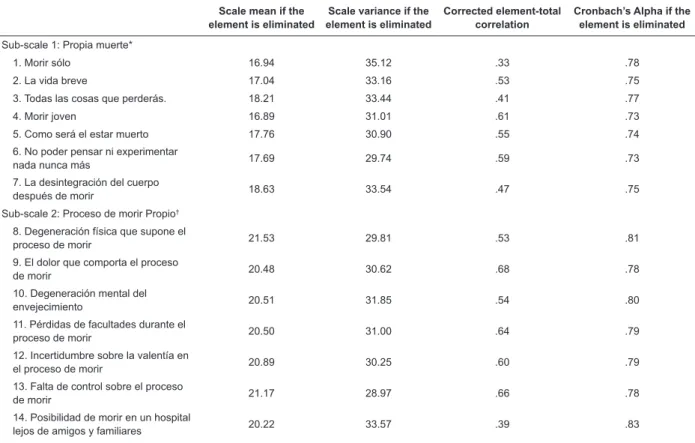
Table 2 – Total-element statistics of the 4 CLFODS sub-scales.
Scale mean if the element is eliminated
Scale variance if the element is eliminated
Corrected element-total correlation
Cronbach’s Alpha if the element is eliminated
Sub-scale 1: Propia muerte*
1. Morir sólo 16.94 35.12 .33 .78
2. La vida breve 17.04 33.16 .53 .75
3. Todas las cosas que perderás. 18.21 33.44 .41 .77
4. Morir joven 16.89 31.01 .61 .73
5. Como será el estar muerto 17.76 30.90 .55 .74
6. No poder pensar ni experimentar
nada nunca más 17.69 29.74 .59 .73
7. La desintegración del cuerpo
después de morir 18.63 33.54 .47 .75
Sub-scale 2: Proceso de morir Propio†
8. Degeneración física que supone el
proceso de morir 21.53 29.81 .53 .81
9. El dolor que comporta el proceso
de morir 20.48 30.62 .68 .78
10. Degeneración mental del
envejecimiento 20.51 31.85 .54 .80
11. Pérdidas de facultades durante el
proceso de morir 20.50 31.00 .64 .79
12. Incertidumbre sobre la valentía en
el proceso de morir 20.89 30.25 .60 .79
13. Falta de control sobre el proceso
de morir 21.17 28.97 .66 .78
14. Posibilidad de morir en un hospital
lejos de amigos y familiares 20.22 33.57 .39 .83
(continue...)
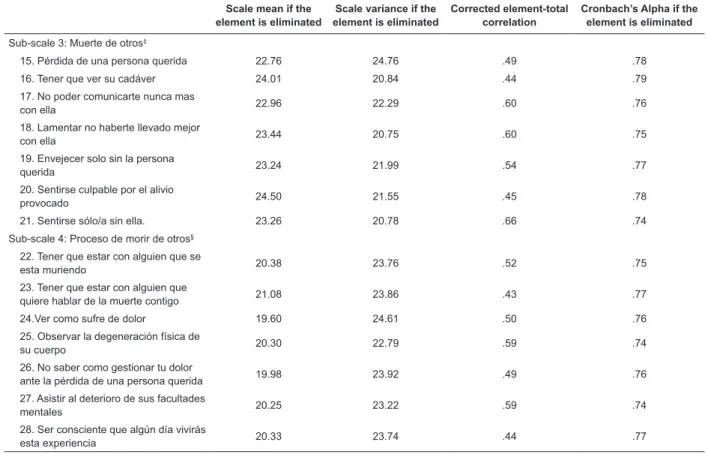
www.eerp.usp.br/rlae Table 2 – (continuation)
Scale mean if the element is eliminated
Scale variance if the element is eliminated
Corrected element-total correlation
Cronbach’s Alpha if the element is eliminated
Sub-scale 3: Muerte de otros‡
15. Pérdida de una persona querida 22.76 24.76 .49 .78
16. Tener que ver su cadáver 24.01 20.84 .44 .79
17. No poder comunicarte nunca mas
con ella 22.96 22.29 .60 .76
18. Lamentar no haberte llevado mejor
con ella 23.44 20.75 .60 .75
19. Envejecer solo sin la persona
querida 23.24 21.99 .54 .77
20. Sentirse culpable por el alivio
provocado 24.50 21.55 .45 .78
21. Sentirse sólo/a sin ella. 23.26 20.78 .66 .74
Sub-scale 4: Proceso de morir de otros§
22. Tener que estar con alguien que se
esta muriendo 20.38 23.76 .52 .75
23. Tener que estar con alguien que
quiere hablar de la muerte contigo 21.08 23.86 .43 .77
24.Ver como sufre de dolor 19.60 24.61 .50 .76
25. Observar la degeneración física de
su cuerpo 20.30 22.79 .59 .74
26. No saber como gestionar tu dolor
ante la pérdida de una persona querida 19.98 23.92 .49 .76
27. Asistir al deterioro de sus facultades
mentales 20.25 23.22 .59 .74
28. Ser consciente que algún día vivirás
esta experiencia 20.33 23.74 .44 .77
*Cronbach’s Alpha = .77; †Cronbach’s Alpha = .82; ‡Cronbach’s Alpha = .80; §Cronbach’s Alpha = .78.
Construct Validity of the CLFODS
Table 3 presents the summary statistics for the
elements of the four CLFODS sub-scales. The sub-scale
“fear of one’s own death”, with a lower average score,
shows greater oscillations (1.90 to 3.64). Moreover,
the average inter-element correlation demonstrates a
positive relation in each of the sub-scales.
Table 3 – Summary statistics of CLFODS sub-scale elements
Sub-scales Mean Minimum Maximum Range Maximum/
Minimum Variance Elements
Sub-scale 1 - Propia muerte
Element means 2.93 1.90 3.64 1.74 1.92 .46 7
Element variances 2.03 1.63 2.52 .88 1.54 .10 7
Inter-element correlations .33 .13 .58 .45 4.58 .01 7
Sub-scale 2 - Proceso de morir Propio
Element means 3.46 2.69 3.99 1.31 1.49 .21 7
Element variances 1.70 1.39 2.28 .89 1.64 .10 7
Inter-element correlations .41 .19 .67 .48 3.59 .02 7
Sub-scale 3 - Muerte de otros
Element means 3.91 2.86 4.60 1.74 1.61 .37 7
Element variances 1.30 .50 2.12 1.62 4.23 .27 7
Inter-element correlations .38 .18 .57 .39 3.13 .01 7
Sub-scale 4 - Proceso de morir de otros
Element means 3.38 2.57 4.06 1.49 1.58 .20 7
Element variances 1.46 1.17 1.75 .58 1.50 .04 7
Rev. Latino-Am. Enfermagem 2011 Sep.-Oct.;19(5):1171-80.
The correlation matrix, in turn, evidences that, in
sub-scale 1: Death of self, item 1 “morir sólo” presents
the lowest correlations with items 3, 6, 7. The other
correlations of element pairs range between 0.20 and
0.57. Sub-scale 2: Dying of self, shows correlations
higher than 0.3, except for item 7, “posibilidad de morir
sólo en un hospital lejos de amigos y familiares”, which
shows a low correlation level with item 1 “degeneración
física..”, while the rest of the correlations range between
0.20 and 0.67. Sub-scale 3 Death of others displays a low
correlation of 0.183 for item 1 “pérdida de una persona
querida” with item 6 “sentirse culpable…”, while the rest
of the correlations vary between 0.20 and 0.57. Sub-scale
4 dying of others shows correlations that vary between
more approximate levels, ranging from 0.24 to 0.52.
Going back to Table 2, for the four sub-scales, each
of the seven elements is positively correlated inside the
respective sub-scale. Element 1 “morir sólo” (0.33),
together with element 14 “posibilidad de morir en un
hospital…” (0.39), are the elements with the lowest
correlation within their respective sub-scales. In turn,
it is observed that the reliability coeficient decreases
when extracting most elements, except for elements
1, “morir sólo” and 14, “morir en un hospital…”, which
increase if the element is eliminated. The reliability
coeficients continue without signiicant variations when
eliminating these elements though, which is why none of
the elements can be eliminated to strengthen the scale.
These results permit guaranteeing that the items
or elements are homogeneous and that the four
sub-scales consistently measure the characteristic they
were elaborated for. Hence, they are reliable and show
construct validity.
Concurrent criterion validity
The concurrent criterion validity between the
CLFODS and its sub-scales and the Attitudes toward
death Scale, measured through Pearson’s correlation
coeficient, shows a positive mean correlation (p<0.001).
The correlation between the CLFODS sub-scales and the Attitude toward death Scale ranged between 0.369 and
0.315. A higher correlation coeficient was observed
between the total CLFODS and the Attitude toward death Scale (0.431).
Factor analysis
The initial Kaiser-Meyer-Olkin (KMO) test corresponded to 0.903 and the sphericity test showed
signiicance (p>0.000), which guarantees the pertinence
of factor analysis. Saturations higher than 0.40 were collected, following the criterion of eigenvalues higher
than one. The initial results before the rotation identiied ive factors, which summarize 54.9% of total data variability. The irst factor concentrated 31% of variability. This irst factor revealed ponderations ranging from 0.41
to 0.70 and all in a positive sense, mainly based on the
“death of others”.
However, to conirm the multidimensionality
hypothesis of the scale proposed in theory and to seek the best adjustment, the researchers decided to submit the PCA results to a varimax rotation.
The results produced a ive-factor structure. The irst factor (explained variance = 12.6%) can be
understood as “fear of other people’s death”, without item 20, “sentirse sólo por el alivio provocado”. The
second factor (explained variance = 10.8%) can be
understood as “fear of one’s own death”. The third factor
(explained variance = 10.7%) can be understood as
“fear of the physical dying process”. The fourth factor
(explained variance = 10.4%) can be understood as
“fear of death and dying according to the psychological
meaning”. The ifth factor (explained variance = 10,2%)
can be understood as “dying of others”.
The items that least explain the variability, in turn,
within their respective scales, are items 3 (34%) and 16 (32%). The variability of the remaining items ranged between 44% and 70% (Table 4).
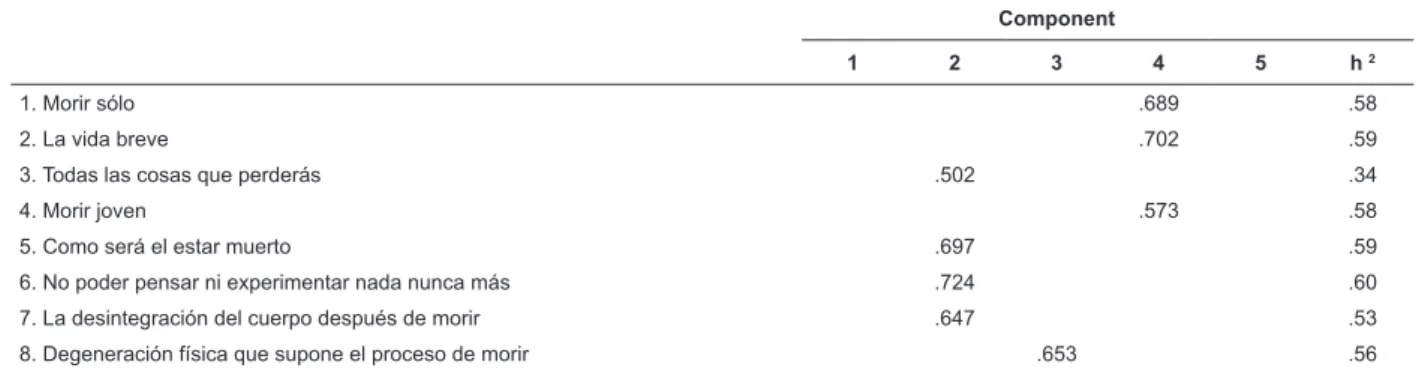
Table 4 – Rotated component matrix
Component
1 2 3 4 5 h 2
1. Morir sólo .689 .58
2. La vida breve .702 .59
3. Todas las cosas que perderás .502 .34
4. Morir joven .573 .58
5. Como será el estar muerto .697 .59
6. No poder pensar ni experimentar nada nunca más .724 .60
7. La desintegración del cuerpo después de morir .647 .53
8. Degeneración física que supone el proceso de morir .653 .56
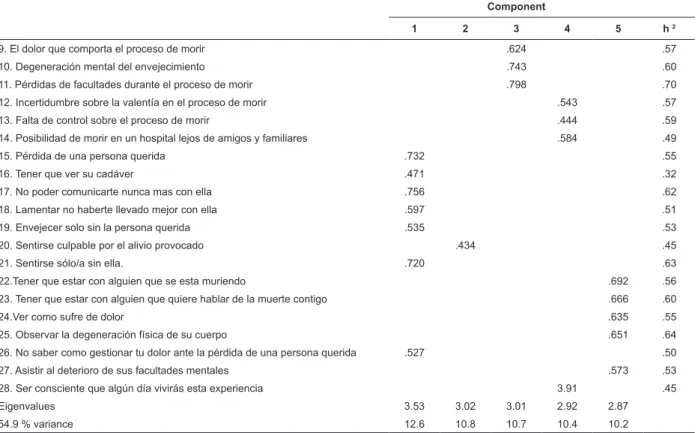
www.eerp.usp.br/rlae Table 4 – (continuation)
Component
1 2 3 4 5 h 2
9. El dolor que comporta el proceso de morir .624 .57
10. Degeneración mental del envejecimiento .743 .60
11. Pérdidas de facultades durante el proceso de morir .798 .70
12. Incertidumbre sobre la valentía en el proceso de morir .543 .57
13. Falta de control sobre el proceso de morir .444 .59
14. Posibilidad de morir en un hospital lejos de amigos y familiares .584 .49
15. Pérdida de una persona querida .732 .55
16. Tener que ver su cadáver .471 .32
17. No poder comunicarte nunca mas con ella .756 .62
18. Lamentar no haberte llevado mejor con ella .597 .51
19. Envejecer solo sin la persona querida .535 .53
20. Sentirse culpable por el alivio provocado .434 .45
21. Sentirse sólo/a sin ella. .720 .63
22.Tener que estar con alguien que se esta muriendo .692 .56
23. Tener que estar con alguien que quiere hablar de la muerte contigo .666 .60
24.Ver como sufre de dolor .635 .55
25. Observar la degeneración física de su cuerpo .651 .64
26. No saber como gestionar tu dolor ante la pérdida de una persona querida .527 .50
27. Asistir al deterioro de sus facultades mentales .573 .53
28. Ser consciente que algún día vivirás esta experiencia 3.91 .45
Eigenvalues 3.53 3.02 3.01 2.92 2.87
54.9 % variance 12.6 10.8 10.7 10.4 10.2
Extraction method: Principal component analysis. Rotation method: Varimax normalization with Kaiser.
The reliability and item-element total correlation
analysis of these ive factors shows that the
total-item correlations exceeded 0.41, except for total-item 3
(0.37), but this correlation is nevertheless important.
Cronbach’s alpha coeficients for each of the ive factors
investigated all exceeded 0.70, which is considered the
minimum accepted reliability level (Table 5). Also, in the
ive factors, the alpha coeficient decreased if the item
was eliminated.
Table 5 – Item-total correlation and Cronbach’s alpha reliability of the 5 factors
Factor 1 Factor 2 Factor 3 Factor 4 Factor 5
Item Corr/Elem/total Item Corr/Elem/total Item Corr/Elem/total Item Corr/Elem/total Item Corr/Elem/total
15 0.53 3 0.37 8 0.56 1 0,59 22 0,53
16 0.43 5 0.60 9 0.60 2 0,51 23 0,43
17 0.62 6 0.60 10 0.59 4 0,59 24 0,49
18 0.59 7 0.52 11 0.59 12 0,65 25 0,41
19 0.52 20 0.40 13 0,72 27 0,52
21 0.67 14 0,47
26 0.53
Cronbach’s Alpha Cronbach’s Alpha Cronbach’s Alpha Cronbach’s Alpha Cronbach’s Alpha
0.82 0.73 0.80 0.82 0.75
Discussion
The present study indings demonstrate the
adequate psychometric characteristics of the CLFODS in
the Chilean population of Nursing students.
Regarding CLFODS reliability, its internal
consistency or homogeneity was demonstrated through
Rev. Latino-Am. Enfermagem 2011 Sep.-Oct.;19(5):1171-80.
as well as for each sub-scale of the original Scale,
similar to the results obtained in studies that used the
same instrument in a student population from Kuwait(21),
Nigeria(10) and Spain(12,22). Also, the obtained reliability of
the CLFODS is very similar to that found in the original
language(20).
The statistics to validate the fear of death construct,
evaluated through the four sub-scale that measure the
fear of one’s own death, fear of one’s own dying process,
fear of other people’s death and fear of other people’s
dying process relect relations that point towards the
same direction between element pairs, and show each
of the seven elements, its contribution to its respective
sub-scale, conirming this characteristic, which had
already been observed in other studies(3,20).
Likewise, the positive correlations between the Fear
of Death and the Attitudes toward Death Scales support
the construct validity in this study. The convergence
of the four sub-scales, in turn, offers a certain degree
of support to the validity of the CLFODS dimensions.
The magnitude of the relation relects that it measures
similar constructs. Hence, as the Fear of death increases,
so does the unfavorable Attitude toward death.
Relations in the same sense are relected in a study
involving nursing students and nurses, in which the scale
correlation demonstrated discriminant validity through a
strong association with the anxiety toward death scale
than with general anxiety(12). Similar results were found
among medical students, correlating the Scale with the
anxiety toward death scale(10) and others(11-12), conirming
its convergent validity.
The multidimensionality is the most distinctive
characteristic of the CLFODS. Its analysis through
factor analysis, in this population, partially coincides
with the hypothesis based on the items’ content. This
study identiied ive factors with a reliable structure,
like the original scale. The results point towards a
reconceptualization, which considers fear of one’s own
death and fear of one’s own dying process as one
physical and another psychological dimension. The rest
of the items display signiicant loads in the structures
similar to the initial dimensions.
Various authors have tried to replicate its factor
structure using PCA and varimax rotation, inding
different results. This started with the Scale creator who,
after modifying it, studied its factor structure, a priori
deining four factors, so as to prove the replicability of
the theoretical structure. He concludes that consistent
loads are observed for two factors, corresponding to
“death of self” and “dying of self”. Regarding “death of
others” and “dying of others”, however, the main load
is found for factor 1(3). Another study that also used the
forced four-factor solution of PCA with varimax rotation
equally shows signiicant loads like the factors in the
previous study. The other two factors partially load
the sub-scales(21). Another factor analysis, however, involving psychology students, obtained ive factors,
with a structure very near the theoretical proposal. The
author justiies the range of results found regarding factor structure in this inal investigation, due to the
correlation that exists among the sub-scales, which in
turn would give rise to an inter-element correlation that
would create a bystander factor of factor loads(20).
It can be concluded that the CLFODS is a reliable
and valid instrument to measure the fear of death
construct. Multidimensionality is conirmed although,
in this population, the notion of fear of death entails
an additional perspective, which comprises two
sub-components that are interesting for research purposes,
which are the physical and psychological dimension of
fear of one’s own death and fear of one’s own dying
process. These dimensions could comprise new
conceptualizations of the construct, which would guide
the elaboration of an appropriate instrument for the
Chilean culture. Nevertheless, the study limitations
should be taken into account. The irst limitation is the
mainly female and young sample in a similar educational
situation, characteristics that are repeated in most
studies analised for this study. Therefore, the factor
solution found based on this scale does not exclude the
existence of other solutions in distinct samples. A better
adjustment of the models should be evaluated in the
future through new exploratory factor analyses.
References
1. Collett L, Lester D. The fear of death end the fear of
dying. J Psychol. 1969;72:179-81.
2. Niemeyer RA. Métodos de evaluación de la ansiedad
ante la muerte. Barcelona: Paidos Iberica; 1997.
3. Lester D, Abdel-Khalek A. The Collett-Lester
Fear of Death Scale: a correction. Death Stud.
2003;27(81):85.
4. Fonnegra DJI. El morir Humano. In: Fonnegra DJI,
editor. De cara a la muerte: como afrontar las penas
el dolor y la muerte y vivir más plenamente. Bogotá:
Editora Planeta; 2003.
5. Kübler-Ross E. On Death and Dying. New York:
6. Mohamed Ali W, Said N. Nurses´Attitudes Toward
Caring for Dying Patient in Mansoura University Hospitals.
J Med Biomed Sci. 2010;3(1):16-23.
7. Espinoza M Sanhueza O. Factores relacionados con la
calidad del proceso de morir en la persona con cáncer.
Rev. Latino-Am. Enfermagem. 2010;18(4):725-31.
8. Lange M, Thom B, Kline NE. Assessing nurses’
attitudes toward death and caring for dying patients
in a comprehensive cancer center. Oncol Nurs Forum.
2008;35(6):955-99.
9. Niemeyer RA. Constructions of death and loss:
Evolution of a research program. Personal Construc
Theory Prac. 2004;1:8-22.
10. Kolawole M, Olusegun A. The reliability and validity
of revised Collett-Lester Fear of Death Scale (version 3)
in Nigerian population. Omega. 2008;57(2):195-205.
11. Abdel-Khalek A, Lester D. Death ansiety as related
to somatic symptoms in two cultures. Psychol Rep.
2009;105(2):409-10.
12. Tomás-Sábado J, Limonero J, Abdel-Khalek AM.
Spanish Adaptation of the Collet-Lester fear of death
scale. Death Stud. 2007;31:246-60.
13. Abdel-Khalek A. Convergent validity of the Templer,
Collett-Lester, and Arabic Death Ansiety Scales: rejoinder.
Psychol Rep. 2004;94:1171-2.
14. Maza M, Zavala M, Merino JM. Actitud del profesional
de enfermeria ante la muerte de los pacientes. Cienc
Enferm. 2008;15(1):39-48.
15. Hernández R, Fernández C, Batista P. Recolección de datos. In: Hernández R, Fernández C, Batista P, editors.
Metodología de la investigación. México: Mac Graw Hill;
2010. p. 342-482.
16. Campo-Arias A. Usos del Coeficiente alfa de Cronbach.
Rev Colombiana Psiquiatr. 2006;26(4):585-8.
17. Pérez C. Reducción de la dimensión: fiabilidad de
escalas y escalamiento multidimensional. In: Perez
C, editor. Métodos estadísticos avanzados con SSPS.
Madrid: Ediciones Paraninfo; 2005. p. 689-758.
18. Lester D. Escala de miedo a la muerte de
Collett-Lester. In: Niemeyer RA, editor. Métodos de evaluación
de la ansiedad ante la muerte. Barcelona: Paidos; 1996.
p. 57-72.
19. Tomás-Sábado J, Gómez-Benito J. Variables
relacionadas con la ansiedad ante la muerte. Rev Psicol
Gral Aplic. 2003;56(3):257-79.
20. Lester D. The factorial structure of revised
Collett-Lester Fear of Death Scale. Death Stud.
2004;28(8):795-8.
21. Abdel-Khalek AM, Lester D. The Factorial Structure
of the Arabic Versión of the Revised Collett-Lester Fear
of Death Scale. Death Stud. 2004;28(8):787-93.
22. Colell R, Limonero G. Análisis de las actitudes
ante la muerte y el enfermo al final de la vida en
estudiantes de enfermería de Andalucía y Cataluña
Universidad Autónoma de Barcelona. Facultad de
Psicología; 2005.
ATTACHMENT
Escala de Miedo a la Muerte de Collett-Lester
Lee cada frase y contéstala rápidamente. No utilices demasiado tiempo pensando en tu respuesta. Se trata de expresar
la primera impresión de cómo piensas ahora mismo. Marca el número que mejor representa tu sentimiento
¿Qué grado de preocupación o ansiedad tienes en relación a TU PROPIA MUERTE en …….? Mucho Moderado Nada
1. El morir sólo. 5 4 3 2 1
2. La vida breve. 5 4 3 2 1
3. Todas las cosas que perderás al morir 5 4 3 2 1
4. Morir joven 5 4 3 2 1
5. Cómo será el estar muerto/a 5 4 3 2 1
6. No poder pensar ni experimentar nada nunca más 5 4 3 2 1
7. La desintegración del cuerpo después de morir 5 4 3 2 1
¿Qué grado de preocupación o ansiedad tienes en relación a TU PROPIO PROCESO DE MORIR en …. Mucho Moderado Nada
1. La degeneración física que supone el proceso de morir 5 4 3 2 1
2. El dolor que comporta el proceso de morir 5 4 3 2 1
3. La degeneración mental del envejecimiento 5 4 3 2 1
4. La pérdida de facultades durante el proceso de morir 5 4 3 2 1
5. La incertidumbre sobre la valentía con que afrontarás el proceso de morir 5 4 3 2 1
6. Tu falta de control sobre el proceso de morir 5 4 3 2 1
Rev. Latino-Am. Enfermagem 2011 Sep.-Oct.;19(5):1171-80.
(continuation)
¿Qué grado de preocupación o ansiedad tienes en relación A LA MUERTE DE OTROS en ….. Mucho Moderado Nada
1. La pérdida de una persona querida 5 4 3 2 1
2. Tener que ver su cadáver 5 4 3 2 1
3. No poder comunicarte nunca más con ella 5 4 3 2 1
4. Lamentar no haberte llevado mejor con ella cuando aún estaba viva 5 4 3 2 1
5. Envejecer solo/a, sin la persona querida 5 4 3 2 1
6. Sentirse culpable por el alivio provocado por su muerte 5 4 3 2 1
7. Sentirse solo/a sin ella 5 4 3 2 1
¿Qué grado de preocupación o ansiedad tienes en relación al PROCESO DE MORIR DE OTROS en….. Mucho Moderado Nada
1. Tener que estar con alguien que se está muriendo 5 4 3 2 1
2. Tener que estar con alguien que quiere hablar de la muerte contigo 5 4 3 2 1
3. Ver cómo sufre dolor 5 4 3 2 1
4. Observar la degeneración física de su cuerpo 5 4 3 2 1
5. No saber cómo gestionar tu dolor ante la pérdida de una persona querida 5 4 3 2 1
6. Asistir al deterioro de sus facultades mentales 5 4 3 2 1
7. Ser consciente de que algún día también vivirás esta experiencia 5 4 3 2 1
Received: Mar. 8th 2011