Research article
HPV knowledge and behavioral intention among health science undergraduate
students: Influence of future health care professionals
Kay Perrin*, Rajal Thaker**, Ellen Daley***, Cheryl Vamos ****, Pankaj Patel***** Associate Professor*, University Of South Florida College of Public Health, Associate Professor**, Obstetrics and Gynaecology, Smt N H L Municipal Medical College, Ahmedabad, India, Associate Professor***, Co-Director, Center for Transdisciplinary Research in
Women’s Health (CTR-WH), University of South Florida College of Public Health, Research Assistant Professor****, Associate
Director, Center for Transdisciplinary Research in Women’s Health (CTR-WH), University of South Florida College of Public Health, Dean*****, Smt N H L Municipal Medical College, Ahmedabad, India
ABSTRACT Objective:
The purpose of this study was to examine knowledge and preventive behaviors related to HPV and cervical cancer among undergraduate health science students in India.
Methods:
Six hundred and Thirty nine undergraduate health science students at a private Indian university completed a paper-and-pencil survey. Univariate and bivariate (chi-square and logistic regression) analyses were tabulated using SPSS 13.0.
Results:
Few (12%) respondents reported seeking preventive health care practices. HPV knowledge was very low (Mean=33.1%). Only half of responders were correct in knowing that the Pap smear tests for cervical cancer (53.6%). Whereas one in five responders (21.6%) reporting knowing a female diagnosed with cervical cancer, only 3.7% of females reporting having had a Pap test. Among those having heard of the HPV vaccine (9.3%), few reported having received the vaccine (5.2%) and most (83.1%) reported that is was Very Unlikely/Unlikely that they would vaccinate their daughters.
Conclusion:
Future efforts should address the low knowledge and rates of preventive behaviors regarding HPV and cervical cancer among Indian health science students as these emerging health professionals will play an important role in decreasing HPV-related morbidity and mortality in India.
Key Words:
Cervical Cancer, Human Papilloma Virus, Undergraduate Health Science Students, India, Prevention
INTRODUCTION
Globally, cervical cancer is the second most common cancer among women.1 In 2005, cervical cancer was responsible for approximately 260,000 deaths, with 95% of these deaths occurring in developing countries.1 Cervical cancer incidence rates remain the highest in Central and South America, eastern Africa, South and South-East Asia, and Melanesia. 1 India alone represents one-fifth of the world’s cervical cancer burden. 2
Scientific data have demonstrated genital human papillomavirus (HPV), the most common sexually transmitted virus, as the underlying cause of cervical cancer.1 Although most HPV infections are cleared naturally by the body’s immune system, persistent infection can manifest into cervical cancer.1 Because it takes approximately 10-20 years for a precursor lesion caused by HPV to develop into cervical cancer, screening and early detection are essential in preventing deaths.1 In developed countries where there is greater awareness and routine screening practices, cervical cancer burden has been significantly reduced. However, the majority of women (95%) in developing countries have never received a cervical cancer screening.1
including precancerous cells. Recent developments in cervical cancer prevention include a newly licensed quadrivalent HPV vaccine, consisting of virus-like particles (VLP), that has demonstrated to be 100% effective in protecting against two of the most common oncogenic types (HPV types 16 and 18) and two of the most common non-oncogenic types (HPV types 6 and 11).3 Because HPV is also attributable to other cancers such as penile, vulva, vagina, anus, mouth and oropharynx cancers, the potential impact of an HPV vaccine in preventing widespread burden is substantial.3
Cervical cancer serves as a significant public health problem as it remains one of the leading causes of death among women in India.4 This disease not only claims the lives of young women, but also disrupts families and communities and negatively affects social and economic well-being.1 The World Health Organization identifies several political, economic, organizational, technical, community, and individual barriers to cervical cancer screening.1 Among these barriers, lack of awareness, attitudes, misconceptions and beliefs surrounding HPV and cervical cancer remain hindrances to implementing a successful screening program in areas where health resources are present.1 In addition, social, cultural, religious and ethical issues can create difficulties when administering a vaccine that prevents a sexually transmitted infection to young women. 5,6
Efforts directed towards decreasing the morbidity and mortality associated with cervical cancer require both health providers and patients to practice preventive measures such as Pap smear screenings and HPV vaccination when
available. Emerging health professionals will lead the way in addressing such a paradigm of prevention for this deadly disease in developing and low-income countries.
The purpose of this study was to examine the knowledge and behaviors of undergraduate health science students associated with HPV, cervical cancer screening and the HPV vaccine at a private Indian university.
MATERIALS AND METHODS
A convenience sample of undergraduate health science (nursing, physical therapy and medicine) students attending a private English-speaking Indian university was recruited from designated courses. A paper-and-pencil questionnaire was developed based on the literature and validated instruments used in previous studies and was pilot-tested with a separate group of undergraduate health science students (n=12) who were not part of the final study sample to ensure cultural appropriateness. The Indian researcher contacted the course instructors to seek permission to administer the surveys. The researcher distributed the questionnaire during the specified class period; the survey took less than 10 minutes to complete. The cover letter explained the purpose of the study and advised students that completion of the survey constituted informed consent. All students attending class that day were invited to participate. Participation was voluntary and confidential and no incentives were provided. Univariate and bivariate (chi-square and logistic regression) analyses were tabulated using SPSS 13.0.
Table 1. Demographic Data (N=639) Author Disclosure Statement
Perrin, K.M.: No competing financial interests exist Thaker, R.: No competing financial interests exist Daley, E.M.: No competing financial interests exist Vamos, C.A.: No competing financial interests exist Patel, P.: No competing financial interests exist.
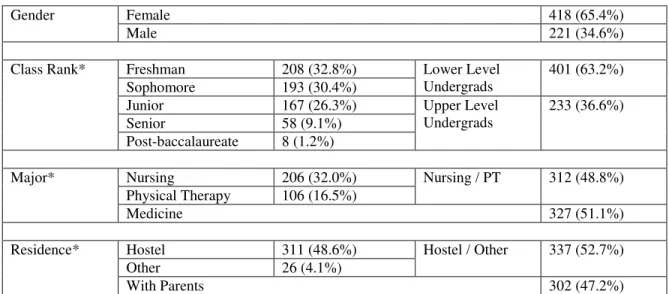
Table 1. Demographic Data (N=639)
*For the purposes of analysis, the following variables were recoded: a) Class Rank was changed from Freshman, Sophomore, Junior, Senior and Post-baccalaureate to Lower Level Undergraduates (Freshman/Sophomores) and Upper Level Undergraduates (Juniors/Seniors/Post-baccalaureate); and b) Major was changed from Nursing, Physical Therapy and Medicine to Nursing / Physical Therapy (PT) and Medicine; and c) Place of Residence was changed from Hostel, Parents and Others to Hostel / Others and Parents.
RESULTS
Demographic Data
Of the 639 responding students, there were 418 (65.4%) females and 221 (34.6%) males with a mean age of 19 years (Range [SD] = 16-24[1]). There were 206 (32.0%) nursing students, 327 (51.1%) medical students, and 106 (16.5%) physical therapy students. The majority (98%) of students were from India. The class rank of the students included 208 (32.8%) freshmen, 193 (30.4%) sophomores, 167 (26.3%) juniors, 58 (9.1%) seniors and 8 (1.2%) post-baccalaureate degrees. For place of residence, 311 (48.6%) of the students lived in the university hostel, 302 (47.2%) resided with their parents, and 26 (4.1%) lived with friends or other relatives as shown in Table 1.
Further analysis of the demographic data reveal that there was a statistically significance difference between the gender and major (OR=5.77, 95% CI=3.98, 8.36). Of the 316 nursing/physical therapy students, there were 265 (83.8%) females and 51 (16.2%) males. However, of the 323 medical students, there are nearly equal numbers of females (n=153; 47.3%) and males (n=170; 52.7%). In addition, there was a statistically significant difference between gender and place of residence (OR=4.70, 95%
CI=3.29, 6.70). Of the 418 responding females, 272 (65.1%) lived in the university hostel and 146 (35%) lived with their parents. Of the 221 responding males, 63 (28.5%) lived in the university hostel and 158 (71.5%) lived with their parents.
Preventive Health Care Practices
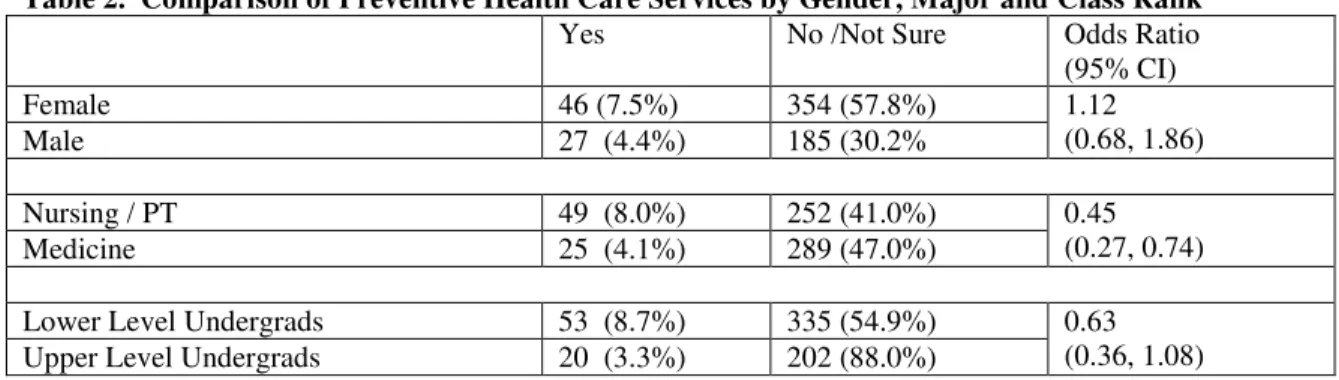
When asked, “Have you ever scheduled an appointment with a doctor when you were not sick and feeling just fine?” the responses were 73 (12%) Yes, 539 (88%) No/Not sure. Of the 73 positive responses, the most common response was “Getting regular check-up.” There were no statistically significance differences between seeking preventive health services and gender (OR=1.12, 95% CI=0.68, 1.86) and class rank (OR=0.63, 95% CI 0.35, 1.08), but there was a statistically significant difference between major and seeking preventive services (OR=0.45, 95% CI=0.27, 0.74). Nearly twice as many nursing/physical therapy students (n=49; 8.0%) reported seeking preventive health care than medical students (n=25; 4.1%) as shown in Table-2.
Gender Female 418 (65.4%)
Male 221 (34.6%)
Class Rank* Freshman 208 (32.8%) Lower Level
Undergrads
401 (63.2%)
Sophomore 193 (30.4%)
Junior 167 (26.3%) Upper Level
Undergrads
233 (36.6%)
Senior 58 (9.1%)
Post-baccalaureate 8 (1.2%)
Major* Nursing 206 (32.0%) Nursing / PT 312 (48.8%)
Physical Therapy 106 (16.5%)
Medicine 327 (51.1%)
Residence* Hostel 311 (48.6%) Hostel / Other 337 (52.7%)
Other 26 (4.1%)
Table 2. Comparison of Preventive Health Care Services by Gender, Major and Class Rank
Yes No /Not Sure Odds Ratio
(95% CI)
Female 46 (7.5%) 354 (57.8%) 1.12
(0.68, 1.86)
Male 27 (4.4%) 185 (30.2%
Nursing / PT 49 (8.0%) 252 (41.0%) 0.45
(0.27, 0.74)
Medicine 25 (4.1%) 289 (47.0%)
Lower Level Undergrads 53 (8.7%) 335 (54.9%) 0.63
(0.36, 1.08)
Upper Level Undergrads 20 (3.3%) 202 (88.0%)
Table 3. Purpose of Pap Test Responses
Knowledge about the HPV, the Pap Test, and Cervical Cancer:
HPV knowledge was assessed by having participants select True/False to a 23-item knowledge scale; theoretical range was 0-100%. Participants reported very poor knowledge with a mean knowledge score 33.1% (Range [SD] = 0-90% [29.2%]). Significant differences were found between gender (t=-8.10; df=544; p=.025), major (t=-12.77; df=547; p=.022) and class rank (t=-8.69; df=542; p=.024). Male (M=45.7%) and upper level undergrads (M=46.8%) demonstrated a mean knowledge score that was approximately two-times greater compared to females (M=24.9%) and lower level undergrads (M=25.7%), respectively. Medical students (M=46.4%) demonstrated a mean knowledge score that was approximately four-times greater than nursing/physical therapy students (M=18.5%).When asked, “Have you ever known any female that has been diagnosed with cervical cancer?” the responses were 137 (21.6%) Yes and 498 (78.5%) No/Not sure. When the females participants only were asked, “Have you ever had a Pap test?” the responses were 16 (3.7%) Yes and 390 (96.1%) No/Not sure. There were
no statistically significance differences between ever having a Pap test and major (OR=1.37, 95% CI=0.50, 3.76) or class rank (OR=1.42, 95% CI= 0.52, 3.90). As a follow-up question, 7 (1.7%) and 385 (98.2%) females responded Yes and No/No sure, respectively, to having ever had an abnormal Pap test. The same seven female responders reported “Yes” when asked if they had ever been diagnosed with HPV. All responders were asked the question, “What is the Pap smear a test for?” and eight items were given. For each item, responders could select “Agree,” “Disagree,” or “Not sure.” The response “Not sure” was later combined with either “Agree” or “Disagree” depending on which statement was correct for that particular item. Table 3 presents the proportion of responders who answered correctly vs. incorrectly for each item. Approximately 80% of the respondents answered correctly that the Pap smear was not a test for pregnancy, HIV/AIDS, herpes, gonorrhea, yeast infections, and vaginal infections. More than half of the respondents (53.6%) were correct in responding that the Pap smear does not test for HPV, but rather tests for cervical cancer.
Incorrect Correct
Pregnancy 163 (31.8%) 350 (68.2%)
HIV / AIDS 152 (29.4%) 366 (70.6%)
Herpes 115 (22.3%) 401 (77.7%)
Gonorrhea 104 (20.5%) 403 (79.5%)
HPV 501 (91.9%) 44 (8.1%)
Cervical Cancer 263 (16.4%) 301 (53.6%)
Yeast Infections 112 (21.9%) 399 (61.8%)
Table 4. Comparison of the Pap smear testing for HPV by Gender, Major and Class Rank
Correct Incorrect Odds Ratio(95% CI)
Female 25 (5%) 318 (59%)
OR=.75(0.40, 1.39)
Male 19 (3%) 179 (33%)
Nursing / PT 18 (3%) 247 (45%)
OR=.71(0.38, 1.33)
Medicine 26 (5%) 254 (47%)
Lower Undergrads 24 (4%) 319 (59%)
OR=.66(0.36, 1.23)
Upper Undergrads 20 (4%) 176 (33%)
Table 5. Comparison of Importance of Doctor’s Advice by Gender, Major and Class Rank Very Important Somewhat
Important
Not important at all Odds Ratio (95% CI)
Female 57 (11.0%) 84 (16.2%) 198 (38.1%) Х2=5.83; df=2;
p=.120
Male 39 (7.5%) 52 (10.0%) 89 (17.1%)
Nursing/Phys Therapy 54 (10.3%) 65 (12.4%) 138 (26.4%) Х2=2.95; df=2;
p=.399
Medicine 43 (8.2%) 72 (13.8%) 150 (28.7%)
Lower Undergrads 66 (12.7%) 95 (18.3%) 166 (32.0%) Х2=8.79; df=2;
p=.032
Upper Undergrads 29 (5.6%) 42 (8.1%) 120 (23.1%)
When looking specifically at the HPV item, there were statistically significant differences for the purpose of the Pap smear testing for HPV and gender (OR=0.75, 95% CI 0.40, 1.39), major (OR=0.71, 95% CI 0.38, 1.33) and class rank OR=0.66, 95% CI 0.36, 1.23) as seen in Table 4.
Regarding the cervical cancer item, there were statistically significant differences for the purpose of the Pap smear testing for cervical cancer and gender (OR=1.53, 95% CI 1.15, 2.32), major (OR=3.06, 95% CI 2.17, 4.32) and class rank (OR=4.47, 95% CI 3.04, 6.56). Approximately the same number of the lower level undergrads (n=148; 26.4%) and upper level undergrads (n=156; 27.8%) knew that the Pap smear tested for cervical cancer.
However, nearly twice as many medical students (n=194; 34.2%) as nursing/physical therapy students (n=110; 19.4%) agreed that the Pap smear tested for cervical cancer.
Knowledge and Behavioral Intention about HPV Vaccine
When asked, “Have you ever heard of a vaccine for HPV?” the response were 58 (9.3%) Yes and 568 (89.1%) No/Not sure. Of the 58 respondents who had heard of the HPV vaccine, 31 (53.4%) were females and 27 (46.6%) were males; 13 (22.4%) were nursing/physical therapy students and 45 (77.6%) were medical students; and 35 (60.3%) were lower level undergraduates and 23 (39.7%) were upper level undergraduates. Three of the 58 students stated that they had already received the HPV vaccine and 25 (44.6%) stated an intention to receive the HPV vaccine in the future. The most common reason for not intending to receive the HPV vaccine in the future was “I am not at risk.”
When asked, “If you are a parent or become a parent, how likely is it that you would have your adolescent daughter be vaccinated against HPV?” the responses were 36 (7.9%) Very Likely, 41 (9.0%) Likely, 171 (37.4%) Unlikely, and 209 (45.7%) Very Unlikely. There were no statistically significant differences between parental intention and gender (Х2
=3.73; df=2; p=.291) and class rank (Х2
but there was a statistically significance between parental intention and major (Х2
=13.57; df=2; p=.004). Among the respondents, 164 (35.9%) nursing/physical therapy students and 216 (47.3%) medical students stated that they would be Unlikely or Very Unlikely to have their adolescent daughters given the HPV vaccine. When asked, “How important is it to you that your doctor tells you to be vaccinated against HPV?” the overall responses were 96 (18.5%) Very Important, 136 (26.2%) Somewhat Important, and 287 (55.1%) Not Important at All. There were no statistically significance differences between doctor’s advice and gender (Х2=5.83; df=2; p=.120) and major (Х2
=2.95; df=2; p=.399), but there was a statistically significant difference between doctor’s advice and class level (Х2
=8.79; df=2; p=.032). However, about one-quarter of the nursing/physical therapy students (n=138; 26.4%) and medical students (n=150; 28.7%) stated that it is not important at all that their doctor tells them to be vaccinated against HPV as shown in Table 5.
DISCUSSION
These findings present implications for utilization of preventive health services, knowledge about the Pap smear related to association to HPV and cervical cancer, and intention to receive the HPV vaccination for the next generation of health care professionals in India. First, only 12% of the students reported scheduling an appointment with a doctor when they were not sick and felt just fine. In India, since most medical services are fee-for-service, health care may be delayed until the disease progresses to the point of being symptomatic or needing pain relief. Second, knowledge about the Pap smear was reported and the majority (80%) of students was able to correctly identify that a Pap smear did not test for pregnancy, HIV/AIDS, herpes, gonorrhea, yeast and vaginal infections; thus it is assumed that the Pap smear information is taught in the health science curricula. However, only a very small percentage of the students (8.1%) were correct in reporting that the Pap smear does not test for HPV, and only half of the students were correct in
reporting that the Pap smear is a test for cervical cancer (53.6%). In addition, less than 10% (n=58) of the students were familiar with the HPV vaccine. These data reveal that this sample of health science students lack adequate knowledge about how the Pap smear is used to diagnose HPV and cervical cancer; the link between HPV and cervical cancer; and the availability of the HPV vaccine.
Third, as for behavioral intention, less than 4% of the students stated an intention to receive the HPV vaccine in the future due to “not being at risk.” In addition, over 80% of the students stated that it would be Unlikely (37.4%) or Very Unlikely (45.7%) that they would vaccinate their daughters with the HPV vaccine. Lastly, 55% of the health science students stated that it is not important at all that the doctor tells you to be vaccinated against HPV. Thus, findings suggest that these health science students do not ascribe to the known research fact that among the strongest health behavior motivator is when doctors advise patients to perform a specific health behavior.7
These findings should be considered in light of the study’s limitations. First, a convenience sample was used and findings may not be generalizable to all health science students in India. More research is needed to examine health science students’ awareness, attitudes, and beliefs surrounding HPV and cervical cancer through a prevention lens. In addition, other barriers to screening due to the sexually transmissible nature of HPV and cervical cancer, and other cultural factors that play a role in primary and secondary prevention of this disease must be further explored.
It should be noted that India does not have a formal screening program for cervical cancer, as do many other countries. The World Health Organization (WHO) lists three successful criteria for successful screening programs, which are listed here from the WHO website:
Effective treatment, capable of reducing morbidity and mortality, should be available;
Test procedures should be acceptable, safe, and relatively inexpensive.8 Whereas cervical cancer is one of the leading causes of mortality for women in India, thereby meeting the first criteria of successful screening programs, India does not yet have a well-disseminated and functional screening program; treatment options are not readily available, and testing procedures (i.e. cervical cells obtained for cytological assessment) are not necessarily acceptable to the general population. Thus, results of this report should be viewed in the context that the students who answered the survey might have low knowledge and no intention to screen or treat for HPV-related cervical infection and early cancerous changes because they lack the awareness of the necessity of such a program. Nonetheless, identifying the awareness and attitudes of young professionals who will be health care providers is the first step in addressing this critical issue.
CONCLUSION
In conclusion, this study identified issues that may impact the success of primary and secondary prevention efforts in India, including future implementation HPV vaccine programs. Since the health science students in this study do not seek preventive health in their personal lives, it is less likely that they will encourage their future female patients to have regular Pap test when these patients are free of symptoms. Without adequate knowledge about HPV and without the intention to receive the HPV vaccine due to not perceiving themselves to be at risk, it is likely that the students will not recommend the HPV vaccine to patients or vaccinate their daughters thus leaving another generation at-risk for cervical cancer. Lastly, since students have limited assurance that advice given by health care professionals’ influences patient behavior, these future health care professionals may be less likely to recommend positive preventive health care practices to their future patients. Developing an effective prevention program that includes knowledge of HPV’s role in cervical cancer and
positive intentions by health care providers to educate patients, recommend the HPV vaccine and provide cytological screening for cervical cancer is an important public health effort.
REFERENCES
1.World Health Organization. Comprehensive cervical cancer control: A guide to essential practice. http://whqlibdoc.who.int/publications/2006/9241547006_e ng.pdf. Accessed July 27, 2009.
2.Sankaranarayanan R, Madhukar Budukh A, Rajkumar R. Effective screening progammes for cervical cancer in low- and middle-income developing countries. Bull World Health Organ 2001;79(10):954-62.
3.World Health Organization. Human papillomavirus and HPV vaccines: Technical information for policy-makers and health professionals. http://www.who.int/vaccines-documents/DocsPDF07/866.pdf. Accessed July 27, 2009. 4.Shanta V, Krishnamurthi S, Gajalakshmi CK, Swaminathan
R, Ravichandran K. Epidemiology of cancer of the cervix: Global and national perspective. J Indian Med Assoc 2000;98(2):49-52.
5.Sarin R. Inverse planning for the T1-T2 conudrum in translation research. J Cancer Res Ther2009;5(1):1-2. 6.Somasundaram K. HPV vaccine: End to women's major
health problem? Indian J Med Res 2008;127(6):511-513. 7.Whitlock EP, Orleans T, Pender N, Allan J. Evaluating
primary care behavioral counseling interventions: An evidence-based approach. Am J Prev Med 2002;22(4):267-84.