ORIGINAL
ARTICLE
O
R
IG
IN
A
L
A
R
T
IC
LE
Vancomycin: the need to suit serum concentrations in
hemodialysis patients
Authors
LíviaLuizeMarengo1 FernandodeSáDelFiol2 SaradeJesusOliveira2 CelsoNakagawa3 EduardoLeiteCroco3 SilvioBarberato-Filho2 MarcelaPellegrini Peçanha4
DouglasFelixdaSilva2 MariaInêsdeToledo2,5
1PharmacySchoolof UniversidadedeSorocaba PIBIC-CNPq
2Researcherofthe ReferenceCenteron InformationAbout Antibiotics(CRIA)of UniversidadedeSorocaba 3ConjuntoHospitalarde Sorocaba
4FaculdadedeCiências MédicasedaSaúde-PUC SãoPaulo
5FaculdadedeTecnologia deSorocaba
Submittedon:02/16/2009 Approvedon:10/15/2009
Correspondence to: Profa.Dra.MariaInêsde Toledo
RuaSilvérioE.Oliveira, 160–Jd.Saira Sorocaba–SãoPaulo– Brazil
CEP:18085-645 Phone:551532385266 E-mail:mitoledo@ yahoo.com
Thisstudyreceived financialsupportfrom theConselhoNacionalde DesenvolvimentoCientífico eTecnológico(CNPq) ABSTRACT
Thevancomycindoseforhemodialysis(HD)patientsshouldbeadjustedbymonitoringdrugserum concentrations. However, this procedure is not available in most health services in Brazil, which usuallyadoptsprotocolsbasedonpublishedstudies.Thetrialsavailablearecontroversial,andsev-eralhavenotbeenconductedwithcurrentdialyzers.Thisstudyaimedatassessingthesuitabilityof vancomycinserumconcentrationsinHDpatientsatapublichospital.BloodsamplesofHDpatients werecollectedfromNovember2006toMay2007,attimeintervalsof48,96,120,or168hoursafter vancomycinadministration.Drugmeasurementwasperformedwithpolarizedlightimmunofluo- rescence.Approximately86%oftroughvancomycinserumconcentrationswerebelowtherecom-mendedvalue,indicatingexposuretosubtherapeuticdosesandahigherriskforselectingresistant microorganisms.
Keywords:vancomycin,chronicrenalfailure,hemodialysis. [BrazJInfectDis2010;14(2):203-208]©ElsevierEditoraLtda.
INTRODUCTION
Vancomycin, an amphoteric and high-molec-ular-weight complex tricyclic glycopeptide an-tibiotic, available in the form of water-soluble hydrochloride, is often used for treating severe hospital infections.1 Vancomycin
concomitant-ly inhibits the cell wall synthesis of susceptible microorganismsorbacteria,alteringcytoplasm membrane permeability and interfering with RNAsynthesis.2 Itsmostsignificantadverseef-fectsareototoxicityandnephrotoxicity.Marinho (2005)hasreportedthatapproximately30%of patients have experienced some adverse reac-tiontovancomycin,suchasrenalfailure(18%), thrombocytopenia(7%),neutropenia(2%),red
mansyndrome(2%),andototoxicity(1%).3
Theincreaseduseofvancomycinhasbeen attributedtotheincreaseofnosocomialinfec-tionscausedbymethicillin-resistant
Staphylo-coccus aureus (MRSA), which increased from
2%in1974tomorethan50%in2000.4
Bacterialinfectionsmostoftenoccurinhe-modialysis (HD) patients. This is most prob-ably related to frequent violation of normal skin and mucosa barriers than to immune dysfunction. Bacterial infections in HD pa-tients progress more rapidly and resolve less promptly than those in non-uremic patients.5
Venousaccesssiteisthesourceof50%to80% ofthebacteremiaepisodesindialysispatients. Bacteremiacanleadtoendocarditis,meningi- tis,osteomyelitis,paraspinalabscess,orforma-tion of septic embolus.Arteriovenous fistulas donothaveanexitsite,thusbeingassociated withlowerinfectionrates.6
InHDpatients,infectionscausedbyGram-positive bacteria can be treated with vanco-mycin,mainlyduetoitsactivityagainstmost Gram-positive pathogens, especially MRSA. Moreover, vancomycin has a long half life in renal failure, which allows using intermittent dosesregimes.7However,thepharmacokinetic characteristicsofthisantibioticshouldbere-spectedtomaintainadequatelevels,minimize the appearance of resistant strains, and avoid toxicity.8Changesinrenalfunctionassociated withnormalagingorwithdiseasescanhavea deepeffectonthepharmacologyofantibiotics, whichrequiretheirdosestobeadjusted.9,10,11
The amount of vancomycin removed by HD is negligible when conventional dialyzers areused;however,whenusinghigh-flowmem- branedialyzers,asignificantreductioninvan-comycinlevelscanoccur.5,11
Measurement of vancomycin serum levels
inpatientswithrenalfailureisrequiredtoas-BRIEF
sureadequatebactericidallevels.AccordingtoLentinoand Leehey(2001),vancomycinmaximumandminimumserum levelsare30-40µg/mLand5-10µg/mL,respectively.5
Due to the high variability of the minimum inhibi-tory concentrations (MIC) for vancomycin-susceptible staphylococcusstrains,arecentstudyhasrecommended thatvancomycinlevelsrangefrom5to10timestheMIC value.12
ThesuggesteddoseofvancomycinforHDpatientsis
15mg/kgevery7to10days.13However,whenhigh-flow
membranesareusedinHD,additionalvancomycindoses
arerecommendedateveryHDsession.14
LentinoandLee-hey(2001)haverecommendedthattheintervalbetween vancomycindosesinHDpatientsshouldbeenlarged,but treatmentshouldbeginwithanattackdoseof20mg/kg andcontinuedwithsubsequentdosesof15mg/kgevery sevendaysaftertheHDsession.5
Otherauthorshavesuggestedchangesindosingand intervalaccordingtotheadministrationregimenandthe typeofdialyzerused.However,reviewingstudiesonthe pharmacokineticsofvancomycininHDpatientsshowed severallimitations,differentconclusionsandsuggestions ofdoseadjustmentcouldbeidentifiedasshowninTable 1. The divergences and limitations of the studies pub-lished have motivated the conduction of this study that aimed at monitoring the serum levels of vancomycin in HDpatientsandcheckingiftheconcentrationsweread-equate.
METHOD
ThestudywasapprovedbytheResearchEthicsCommittee oftheUniversidadedeSorocaba(Protocol001/05)andby theTeachingandResearchCommitteeoftheConjuntoHos- pitalardeSorocaba(stateofSãoPaulo),astatepublichospi-talthatattendsapproximately120HDpatients.Allpatients includedinthisstudyusedvancomycinduringtheperiod studied(fromNovember2006toMay2007)andprovided writteninformedconsent.Theexclusioncriteriawereasfol- lows:reportofallergytovancomycin,liverdisease,orprevi- oususeofvancomycinupto15daysbeforesamplecollec-tion.
Datacollectionfrommedicalrecordsincludedthefol-lowing: gender, age, origin, and ethnicity. The results of culture and antibiogram were obtained from the Hospital InfectionControlServiceoftheConjuntoHospitalardeSo-rocaba.
Vancomycin(VancocinaCP–ABLAntibióticosdoBra- sil)wasgivenindoseof1gdilutedinto100mLof0.9%so-diumchloridesolutioninfusedduringthelasthourofHD, accordingtotheservice’sprotocol,whichrecommendsthe administrationof1geverysevendays.Bloodsampleswere collected by the nurse team in tubes containing ethylene diaminetetraaceticacid(EDTA)forhemogramandindry
tubesformeasuringvancomycinandalbumin.Then,they were centrifuged and frozen. The collections for measur-ingvancomycinwereobtainedinsinglesamplesatthetime points48,96,120or168hoursafteradministeringthefirst doseofthedrug.
HemogramwasperformedintheautomatedABXPen-tra60® device, at the Instituto Diagnóstico de Sorocaba. Theendpointcolorimetricmethodwasusedformeasuring albumin with a kit containing bromocresol green (BCG) of Laborlab, at the Universidade de Sorocaba.
Vancomy-cinserumlevelsweremeasuredbyusing150µLofserum
and polarized light immunofluorescence with monoclonal antibodies (ABBOTT Laboratories kits) in the automated AxSym®device(ABBOTT),inthesectorofserologyofthe HemonúcleooftheConjuntoHospitalardeSorocaba.
The results were reported regarding the percentage of patients with inadequate serum concentrations and need fordoseadjustment.Statisticalanalyses(ANOVA)wereper-formedinthecorrelationoftheresultsofvancomycinand albuminconcentrationsandhematocritlevels.Thesignifi-cancelevelof5%wasadopted.
RESULTS
The study comprised 17 patients, five of whom used van-comycin more than once during the period studied, at a meanintervalof72days,addinguptothecollectionof22 samples.Theirmeanagewas56.9±6.0years.Mostpatients (56%)werefemale,married(65%),white(65%),andcame fromthemunicipalitiesoftheSorocabaregion(59%).
ThefollowingclinicalconditionsrelatedtoHDproce-durestandout:double-lumencatheterasthemostcommon venous access (65%); dialysis capillary reuse time ranging from1-19days,medianofthreedays;associationofdiabe-tesmellitusandarterialhypertensionasthemostfrequent etiologyofchronicrenalfailure(41%);meanHDtimeof16 months.Allpatientsusedpolysulfonedialyzermembrane.
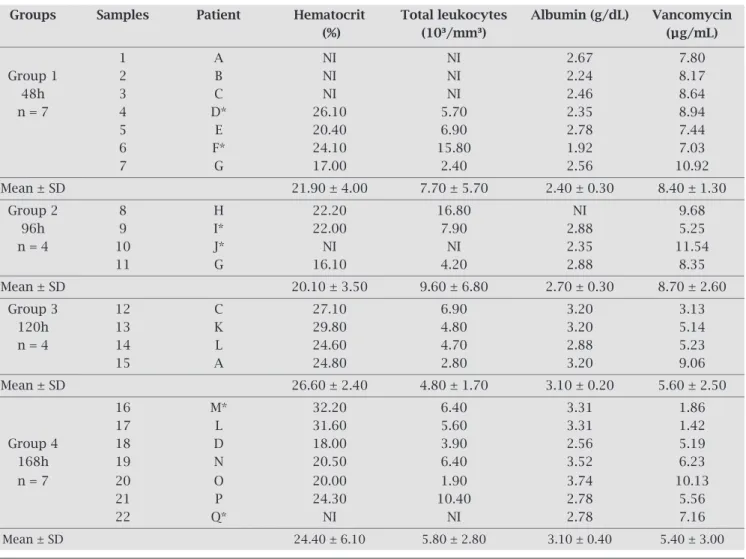
Patients’ laboratory data presented in Table 2 showed thatalbumin(referencevalues:3.4-4.8g/dL)21
andhemat-ocrit(referencevalues:women:39-49%andmen:35-45%)21
werebelownormalvalues,butcompatiblewiththesetting of chronic renal failure. Neither statistical difference be-tween groups (ANOVA), nor correlation bebe-tween the pa-tient’splasmalevelofalbuminandserumconcentrationof vancomycinwereobserved(p>0.05).
Regarding to vancomycin serum concentrations , no statistical difference (ANOVA, p > 0.05) between the val-uesofthefourgroupswasobserved(Table2).However,at least14%oftheresultswereinadequatewhenconsidering theminimumtroughconcentrationgreaterthan5µg/mL, and86%wereinadequatewhenconsideringtheminimum troughconcentrationgreaterthan10µg/mL(Figure1).
Table 1. Limitations, objectives and conclusions of the major studies on monitoring vancomycin in hemodialysis.
Reference Limitations of the study Goal Major conclusions
Number of patients (four) To check the renal excretion For anuric patients, 7% of Nielsen et al. undergoing hemodialysis rate in several degrees of the usual maintenance dose
(1975)15 with no infection renal failure per unit of time are
recommended
They do not specify To assess toxicity and Large variation in peak and Masur et al. the dialyzer used pharmacokinetics trough concentration (to
(1982)16 in prolonged treatment monitor). Negative cultures in
(accumulation) the initial 48 hours of therapy. Low toxicity
Small number of patients To correlate renal function For patients with creatinine Gonzáles-Martin with infection, several topographies and vancomycin clearance < 10 mL/min-1,
et al. (1996)17 and unstable patients (sepsis). concentration vancomycin doses of 1 g every
They also report peak concentration seven days are suitable above the limit of toxicity
Zoer; Schrander- To check vancomycin Vancomycin clearance does not Van der Meer; clearance with two types depend on HD flow. Van Dorp Patients with no infection of dialyzers Recommendation: one gram
(1997)18 initially + 500 mg during each
subsequent HD session
To assess the pharmacokinetics 25 mg/kg during HD of high doses of vancomycin determine adequate Foote et al. Five patients in F80-Fresenius polysulfone concentration for up to
(1998)19 with no infection membrane seven days and subsequent
doses should be adjusted according to serum
concentration
To determine the amount of Vancomycin administered Lucksiri et al. vancomycin removed by the during the last hour of HD
(2002)20 Patients with no infection CAHP-210 dialyzer results in a 24%-lower
concentration than when administered after HD
To compare three regimens Administration of 30 mg/kg Mason et al. Patients with no infection of vancomycin dosing during HD is equivalent to
(2003)7 administration of 15 mg/kg
after HD
Figure 1: Graphic representation of vancomycin measurement results in samples of patients with renal failure undergoing
hemodialysis (n = 22). MRC = minimum recommended concentration.
Concentration (µg/mL)
Patients’ vancomycin concentration Time (hours)
170
160
150
140
130
120
110
100
90
80
70
60
50
40
30
20
10
0
12
10
8
6
4
2
0
wereStaphylococcus aureus. Of those, 50% were oxacillin-resistant,and100%weresensitivetovancomycin.
DISCUSSION
Several studies used for establishing the current empirical protocolsofvancomycindosinginpatientswithrenalfailure undergoingHDareoutdatedwithregardstodialysisequip-ments.Themanufacturerofthereferencedrug(Vancocin®) reportsthatitisnotdialyzableanditshalflifeis7.5daysin patients with severe renal failure. However, the various tri-alshavedifferentcaseseriesandseverallimitations,suchas thesmallnumberofpatients,unstablepatients(withsepsis), patientswithnoinfection,andpatientsusingdifferenttypes ofdialyzers.Launay-Vaucheret al.(2002)havediscussedthe useofseveraldialysismembranesandsystemsaimingates-tablishingprotocolsformonitoringserumconcentration.In fact,thataspecthasbeenseldomexploredintheinternational literature,sincemosthospitalsindevelopedcountriesmoni-tor vancomycin concentration in patients at risk (neonates, patientswithlargeburns,patientswithrenalfailure,andthe
elderly).InBrazil,however,fewhospitalsdothisonaregular basis.Thecostofthatautomatedtestisconsideredalimiting factorandisequivalenttothemeanpriceofonedrugvial.10
Currently, approximately 80% of the hospital sta-phylococcal infections are treated with glycopeptides, suchasvancomycinandteicoplanin.Thisisstillthean-timicrobialclassofchoicefortreatinginfectionscaused by MRSA, although strains with reduced sensitivity to
vancomycinhavealreadybeenisolatedinBrazil.22
Theaccessorygeneregulator(agr)ofStaphylococcus
aureusmodulatestheexpressionofnumerousvirulence
factors in the phase-dependent growth. According to Roseet al. (2007), all agr groups develop intermediate resistance to vancomycin with subtherapeutic expo-sures.23
The study by Sakoulaset al. (2006) has shown that theexposuretosubtherapeuticvancomycinconcentra-tions is associated with the development of clinically
hetero-GISA(glycopeptideintermediate-resistant
S.au-reus)isolates.Theseauthorsconsiderthattheconstant
Table 2. Laboratory data and vancomycin measurement in samples (n = 22) of HD patients
Groups Samples Patient Hematocrit Total leukocytes Albumin (g/dL) Vancomycin
(%) (10³/mm³) (µg/mL)
1 A NI NI 2.67 7.80
Group 1 2 B NI NI 2.24 8.17
48h 3 C NI NI 2.46 8.64
n = 7 4 D* 26.10 5.70 2.35 8.94
5 E 20.40 6.90 2.78 7.44
6 F* 24.10 15.80 1.92 7.03
7 G 17.00 2.40 2.56 10.92
Mean ± SD 21.90 ± 4.00 7.70 ± 5.70 2.40 ± 0.30 8.40 ± 1.30
Group 2 8 H 22.20 16.80 NI 9.68
96h 9 I* 22.00 7.90 2.88 5.25
n = 4 10 J* NI NI 2.35 11.54
11 G 16.10 4.20 2.88 8.35
Mean ± SD 20.10 ± 3.50 9.60 ± 6.80 2.70 ± 0.30 8.70 ± 2.60
Group 3 12 C 27.10 6.90 3.20 3.13
120h 13 K 29.80 4.80 3.20 5.14
n = 4 14 L 24.60 4.70 2.88 5.23
15 A 24.80 2.80 3.20 9.06
Mean ± SD 26.60 ± 2.40 4.80 ± 1.70 3.10 ± 0.20 5.60 ± 2.50
16 M* 32.20 6.40 3.31 1.86
17 L 31.60 5.60 3.31 1.42
Group 4 18 D 18.00 3.90 2.56 5.19
168h 19 N 20.50 6.40 3.52 6.23
n = 7 20 O 20.00 1.90 3.74 10.13
21 P 24.30 10.40 2.78 5.56
22 Q* NI NI 2.78 7.16
Mean ± SD 24.40 ± 6.10 5.80 ± 2.80 3.10 ± 0.40 5.40 ± 3.00
exposure of microorganisms to a vancomycin concen-
tration>10mg/Lisimportantinpreventingtheappear-anceofintermediateresistancetoglycopeptides.24
Johnson and Woodford (2002), studying glycopeptide resistantS.aureus (GRSA),havereportedthatGRSAisolat-edinMichiganwithonevanAgene,alongwithothergenes, encodeahighlevelofresistancetoglycopeptides.25
Due to the increasing use of vancomycin, worrisome vancomycin-resistant strains ofE. faeciumandE. faecalis
haveemerged.Thedeterminantofthisresistanceislocated inatransposonthatispartofaplasmid;thus,thevancomy-cin-resistantenterococcuscantransferitsresistancetoother Gram-positive bacteria, such as staphylococci, worsening evenmoretheoccurrenceofmulti-resistantbacteria.3
TheGISAandGRSAresistances,althoughstillrare,should beunderconstantmultidisciplinarysurveillance.Thefollow-ingpatientsareatriskforGISA:patientsreceivingprolonged vancomycintherapy;patientspreviouslycolonizedbyMRSA orvancomycin-resistantenterococci(VRE),particularlythose withperitonealcatheters;patientswithdocumentedMRSA infection;andHDpatients,whofrequentlyhaveMRSAand undergotherapywithglycopeptides.26
Because VRE are usually resistant to other antibiotics commonlyusedinhospitals,severeexposuretootherdrugs isassociatedwithahighriskofacquiringVRE.27
Similarly to beta-lactam antibiotics, vancomycin has negligible post-antibiotic effects and requires the mainte-nanceofconcentrationsequivalenttofourtofivetimesMIC duringprolongedperiodstoobtainanefficientantibacterial effect.8
InclinicalpracticeinBrazilianhospitals,dosingformost patients with chronic renal failure is 1 g every seven days. However, in a study by González-Martinet al. (1996), the vancomycinlevelsevendaysafteradministrationwaslow-er than expected and a subtherapeutic level was probably achieveddaysbefore.17
Zoeret al .(1997)haverecommendedaninitialvanco- mycindoseof1g,towhich500mgshouldbeaddeddur-ingeachsubsequentHDsessioninpatientswithapositive cultureforS.aureus.Theidealtimeforplasmamonitoring
wouldoccur48h,and96hor120haftervancomycininfu-sion.18Otherauthorshaverecommendedthedetermination
ofvancomycinserumconcentrationbeforethefirstHDses-sionsubsequenttotheadministrationandbefore72-hour of HD session. If the results are below the recommended
values(between5and10µg/mL),acomplementary500-mg
doseofvancomycincanbeused.5,28
It is worth noting that, in this study, 86% of the
pa-tientshadconcentrationsbelow10µg/mLand14%ofthe
patientshadconcentrationsbelow5µ
g/mL.Whenthecol-lectiontimesareconsidered,onecaninferthatthenumber
ofpatientsreachingtroughconcentrationsbelow5µg/mL
would be greater. It is also worth noting that vancomycin
hasbeenadministeredduringtheHDsession,butsupple-
mentarydosesarenotadministeredaccordingtotherecom-mendationofMasonet al.(2003)whohavecomparedthree
regimensofvancomycindosing.7
In conclusion, the patients included in this study were exposedtoantibioticsubtherapeuticdoses.Consideringthe increasedriskofselectingresistantmicroorganisms,moni-toringofvancomycinserumconcentrationinHDpatients isrecommended.
ACKNOWLEDGEMENTS
TheauthorsthankthesupportoftheNephrologyService, the nurse Yuriko Miyamoto, Edênia M. C. Fronteira, and IvanildaS.AquinooftheServiceofHospitalInfectionCon-trolandBloodCenterofConjuntoHospitalardeSorocaba. They also thank the Instituto de Diagnóstico de Sorocaba andtheUnimedHospitaldeSorocaba.
TheauthorsalsothanktheCNPqforfinancialsupport (references402722/2005-1and117276/2006-5).
REFERENCES
1. KlascoRKeditor.Martindale:theextrapharmacopoeia.Base dedadosnaInternet.GreenwoodVillage:ThomsonMICRO-MEDEX;1974-2006.Disponível:http://www.periodicos.capes. gov.br.Acessoem20demaiode2008.
2. GeM,ChenZ,OnishiHR,KohlerJ,SilverLLet al
.Vancomy-cinderivativesthatinhibitpeptidoglycanbiosynthesiswithout bindingD-ala-D-ala.Science1999;284:507-10.
3. Marinho, DS Vancomicina, estudo de utilização com ênfase emsuasreaçõesadversas.2005.120f.Dissertação(Mestrado) –FundaçãoOswaldoCruz,RiodeJaneiro,2005.
4. Bartlett JG Antibiotic selection for infections involving me-thicillin-resistantStaphylococcusaureus.2004.Disponívelem: http://www.medscape.com/viewprogram/3124.Acessoem03 dedezembro2007.
5. LentinoJR,LeeheyDJ.Infecções.In:DaugirdasJT,BlakePG, Ing TS. Manual de diálise. 3. ed. Rio de Janeiro: Guanabara Koogan,2001.
6. Marcondes CRR, Biojone CR, Cherri JM, Takachi P, Carlos E. Complicações precoces e tardias em acesso venoso cen-tral: análise de 66 implantes. Acta Cirúrgica Brasileira 2007; 15:73-5.
7. MasonNA,NeudeckBL,WelageLS,PatelJA,SwartzRD.Com- parisonof3vancomycindosageregimensduringhemodialy-siswithcellulosetriacetatedialyzers:post-dialysisversus intra-dialyticadministration.ClinicalNephrology2003;60:96-104. 8. SilvaLAM,PansardHM,RosaDB,BottonSR,MezzomoNF
et al.Níveissanguíneosdevancomicinaeadequaçãodeseu
usoempacientescominsuficiênciarenalemtratamentodi-alítico.JornalBrasileirodeNefrologia1998;20:411-8. 9. Tavares W. Glicopeptídeos e Lipopeptídeos. In:
Antibióti-cos e quimioterápiAntibióti-cos para o clínico. São Paulo: Atheneu, 2007.
10. Launay-VacherV,IzzedineH,MercadalL,DerayG.Clinical review:useofvancomycininhaemodialysispatients.Criti-calCare2002;6(4):313-6.
12. BingenE,Mariani-KurkdjianP,NebbadB.Optimalvanco-mycinserumlevelinStaphylococcusaureus infections?Me-decineetMaladiesInfectieuses2006;36(9):439-42. 13. Mandell GL, Bennett JE, Dolin R. Mandell, Douglas, and
Bennett´s: principles and pratice of infectious diseases. 6 ed. Philadelfia:Elsevier,2005.
14. StryjewskiME,SzczechLA,BenjaminDK,InrigJK,Kanafani
ZAet al.Useofvancomycinorfirst-generationcephalosporins
for the treatment of hemodialisys-dependent patients with methicillin-susceptibleStaphylococcus aureus bacteremia. ClinicalInfectiousDiseases2007;20:190-6.
15. NielsenHE,HansenHE,KorsagerB,SkovPE.Renalexcretion of vancomycin in kidney disease. Acta Medica Scandinavica 1975;197(4):261-4.
16. MasurH,FrancioliP,RuddyM,MurrayHW.Vancomycinse-rumlevelsandtoxicityinchronichemodialysispatientswith
Staphylococcus aureus bacteremia. Clinical Nephrology 1993;
2:85-8.
17. Gonzalez-MartinG,AcunaV,PerezC,LabarcaJ,GuevaraA, TagleR.Pharmacokineticsofvancomycininpatientswithse- verelyimpairedrenalfunction.InternationalJournalofClini-calPharmacologyandTherapeutics1996;34(2):71-5. 18. ZoerJ,Schrander-VanDerMeerAM,VanDorpWT.Dosage
recommendationsofvancomycinduringhaemodialysiswith highly permeable membranes. Pharmacy World & Science 1997;19(4):191-6.
19. Foote EF, Dreitlein WB, Steward CA, Kapoian T, Walker JA, Sherman RA. Pharmacokinetics of vancomycin when ad-ministeredhighfluxhemodialysis.ClinicalNephrology1998; 50(1):51-5.
20. Lucksiri A, Scott MK, Mueller BA, Hamburger RJ, Sowinski KM. CAHP-210 dialyzer influence on intra-dialytic
vanco-mycin removal. Nephrology Dialysis Transplantation 2002; 17(9):1649-54.
21. GoldmanL,AusielloD.Cecil:tratadodemedicinainterna.22. ed.RiodeJaneiro:Elsevier,2005.
22. BernardesRC,JorgeAOC,LeãoMVP.Sensibilidadeàoxacili- na,vancomicinaeteicoplaninadeStaphylococcuscoagulase-positivoisoladosdepacienteshospitalizadosdeSãoJosédos Campos.RevistaBiociências2004;10(1-2):73-8.
23. RoseWE,RybakMJ,TsujiBT,KaatzGW,SakoulasG.Correla-tionofvancomycinanddaptomycinsusceptibilityin
Staphy-lococcus aureus infererence to accessory gene regulator(agr)
polymorphismandfunction.JournalofAntimicrobialChem-otherapy2007;59:1190-3.
24. SakoulasG,HowardSG,CohenRA,VenkataramanL,Moel-lering RC, Eliopoulos GM. Effects of prolonged vancomycin administrationonmethicillin-resistantStaphylococcusaureus (MRSA) in a patient with recurrent bacteraemia. Journal of AntimicrobialChemotherapy2006;57(4):699-704.
25. Johnson AP, Woodford N. Glycopeptide-resistant
Staphylo-coccus aureus.JournalofAntimicrobialChemotherapy2002;
50:621-23.
26. CenterforDiseaseControlandPrevention.Laboratorycapac-itytodetectantimicrobialresistance.1998;48:1167-71. 27. Finch RG, Eliopoulos GM. Safety and efficacy glicopeptide
antibiotics. Journal of Antimicrobial Chemotherapy 2005; 55(S2):ii5-ii13.